
Abstract
The review describes the syndrome of endogenous intoxication in patients with mental disorders. Oxidative stress, middle-mass endotoxic molecules, impaired functional properties of serum albumin and albumin thiol groups, neurotrophic factors, and enzymes, including monoamine oxidase and semicarbazide-sensitive amine oxidase contribute to the development of endogenous intoxication. Possible pathogenetic mechanisms of the endogenous intoxication development in mental disorders and approaches to its treatment are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Intoxication is characteristic of diseases associated with heightened catabolism, hypoxia, altered microcirculation, elevated tissue decomposition, and accumulation of excessive amounts of substances, metabolites, and components untypical for healthy metabolism in tissues and body fluids [1]. The symptoms of intoxication share common features and clinical manifestations and develop via similar mechanisms [2]. In any pathology, endogenous intoxication (endotoxicosis) aggravates the course of the disease.
We hypothesized that endogenous intoxication is an integral component in the pathogenesis of mental disorders [1, 3, 4].
The mechanisms of develo** endogenous intoxication can be classified into several groups [1, 4], some of which are described below:
(i) degradation processes resulting in the accumulation of excessive amounts of intermediate and terminal metabolites;
(ii) impairment and damage of body systems functioning to bind, inactivate, and excrete the products of metabolism;
(iii) damage to the barrier systems normally regulating substance exchange between the cell and extracellular space and preventing the entrance of toxic agents to the cell.
Alterations in the endocrine, immune, and other systems also contribute to develo** endotoxicosis.
However, all attempts to identify a toxin (or toxins) specific to particular pathologies have been unsuccessful so far. Pathological conditions are characterized by accumulation of large amounts of intermediate and final metabolites that can damage organs and tissues.
It is impossible to identify all toxic substances of endogenous origin. Moreover, a great variety of their targets underlies both specific and general clinical manifestations of endotoxicosis. Therefore, non-specific endogenous intoxication syndrome per se can be considered as an important component of pathogenesis in all diseases.
Endogenous intoxication can be manifested at two levels – metabolic and clinical.
Metabolic endotoxicosis is characterized by excessive accumulation of normal and pathological metabolites that can be detected by biochemical and other laboratory assays. Clinical manifestations of endotoxicosis include both alterations of metabolism and various clinical symptoms, such as disease complications and side effects of therapy.
Endogenous intoxication syndrome can be identified using integrative biological tests that simultaneously evaluate several processes (partially or fully) instead of a single biochemical or pathophysiological parameter, which allows to draw conclusions on the status of a biological system or a complex of biological and biochemical systems.
However, despite the importance of this topic, the mechanisms and metabolic hallmarks of develo** endogenous intoxication syndrome in patients with mental disorders (as well as with other pathological conditions) have been poorly investigated.
The processes contributing to the development of endogenous intoxication and corresponding alterations in homeostasis will be discussed below.
OXIDATIVE STRESS
Oxidative stress is one of the factors contributing to the development of endogenous intoxication.
Oxidative stress is characterized by the excessive production of prooxidant compounds in the cells and altered balance between the prooxidant and antioxidant molecules. Oxidative stress develops when the cell antioxidant defense mechanisms fail to control the level of reactive oxygen species (ROS) and reactive nitrogen species (RNS) generated in routine oxidative metabolism or in the prooxidant environment [5]. The link between oxidative stress and pathophysiological mechanisms of diseases may be accounted for by a physiological phenomenon called the oxidative paradox [6]. According to this concept, oxygen plays two opposite roles: oxygen is vital for supporting life; on the other hand, oxygen is toxic for the cell [5, 6].
ROS are extremely reactive molecules, and, therefore, all evolutionary attempts to develop adaptation mechanisms capable to fully neutralize negative oxygen-related effects have failed. Excessive ROS generation produces multiple harmful effects, including the damage of membrane structures, lipid oxidation, disturbance of the protein structure and function, and damage of nucleic acids. These effects are especially prominent in the brain because of the low antioxidant defense of neurons [7].
Stress is a host’s response to potentially damaging insults. Moderate acute stress can be beneficial, as it activates memory-related processes and stimulates proliferation and neurogenesis of hippocampal cell. However, chronic stress can elicit brain damage [8]. Long-term stress plays an important role in pathogenetic mechanisms of mental disorders by suppressing cell proliferation and neurogenesis [9].
Environmental stress factors cause damage by altering immune and hormonal responses, which results in impaired neurogenesis and neurotransmission and eventually leads to the development of neurodegenerative disorders [10].
It was confirmed that chronic stress contributes to the oxidative stress in the brain areas involved in the development of mental pathologies [11]. In the process of metabolism, biological systems generate the products, whose excessive amounts may have a harmful effect on the entire human body. Under physiological conditions, the levels of free radicals and antioxidant molecules are balanced. Oxidative stress disrupts redox reactions and mechanisms controlling them, thus resulting in the damage of biological molecules [12-14].
Free radicals are generated in multiple metabolic pathways involving a broad range of compounds. The four major sources of free radicals are the (i) electron transfer in the mitochondrial electron transport chain, (ii) fatty acid peroxidation, (iii) reactions catalyzed by cytochrome P450, and (iv) phagocytic cells [15].
Unsaturated carbon bonds in cholesterol and fatty acids of membrane lipids react with free radicals in a process called lipid peroxidation (LPO) that generates free peroxide radicals. Polyunsaturated fatty acids are especially sensitive to peroxidation [16]. After initiation, LPO becomes autocatalytic, resulting in the emergence of highly reactive compounds, such as lipid peroxides, lipid alcohols, and various aldehydes.
The three major classes of biological macromolecules – lipids, nucleic acids, and proteins – are also susceptible to the attack of free radicals. For example, the main effect of peroxidation is reduced membrane fluidity, which impairs the properties of the membrane and can significantly damage membrane-bound proteins. Free radical attack leads to the oxidation of sulfhydryl (thiol) groups, reduction of disulfide bonds, formation of bonds (crosslinks) between proteins, lipids, or between proteins and lipids, fragmentation of polypeptide chains, damage and inactivation of enzyme active sites, etc. Ionizing radiation-induced mutations and cell death are mainly due to the reactions between free radicals and DNA [16].
LPO causes structural damage of membranes and results in the generation of specific epitopes via membrane oxidation. These epitopes represent cytotoxic secondary products of polyunsaturated fatty acid peroxidation, e.g., 4-hydroxy-2-nonenal (4-HNE) and malonic dialdehyde (MDA) that have the proinflammatory properties. Such epitopes are extremely toxic and exert a destructive effect on biological membranes [17].
Elevated levels of these molecules (in particular, MDA, which causes protein damage and generation of LPO terminal products with proinflammatory properties) serve as indirect markers of oxidative stress in patients with depression. These compounds were also found in the serum and plasma of patients with depression [18, 19].
The serum of individuals with depression also contains elevated concentrations of other LPO markers, e.g., compounds reacting with thiobarbituric acid and 8-iso-prostaglandin F2α, that serve as DAMPs (damage-associated molecular patterns). The level of these compounds was found to correlate with the severity of depression [20].
ROS can damage nuclear and mitochondrial DNA through modification of nucleotide bases, induction of damage or breaks in the DNA helix and loss of purine bases, damage to sugar moieties in the sugar-phosphate backbone, interference with the DNA–protein interactions, and impairments in the activity of DNA repair system [5]. All these effects of ROS disturb the regulation of genetic processes and can induce programmed cell death. Neurons are able to respond to DNA damage by inhibiting expression of affected genomic region playing a vital role in the cell survival. Oxidation of deoxyguanosine leads to the formation of 8-hydroxy-2′-deoxyguanosine (8-OH-dG) that is used as a marker of DNA damage in clinical studies. The level of 8-OH-dG is increased in patients with depression [21].
Various mental disorders, e.g., depression and schizophrenia, are characterized by excessive telomere shortening and decreased telomerase activity [22]. The study conducted in a large cohort of patients with affective disorders revealed accelerated telomere shortening, thus supporting a hypothesis on the accelerated cell aging in depression [22, 23]. The extent of telomere shortening was found to correlate with the oxidative stress level, suggesting a significant impact of oxidative stress on the telomere damage, a hallmark of cell aging, in patients with depression [24]. Importantly, the length of telomeres in untreated patients with depression negatively correlated with the interleukin-6 (IL-6) level. However, the exact mechanism behind telomere shortening and its role in premature cell senescence in depression remain unclear [22].
Proteins can be directly or indirectly affected by oxidative stress including peroxidation, damage of amino acids, degradation or fragmentation, and disturbance of the protein spatial structure. As a result, proteins can lose their functional or enzymatic activity, resulting in the loss or impairment of their physiological functions [5]. An interesting example is neural cell adhesion molecules (NCAMs), which are membrane-bound glycoproteins expressed on the surface of neurons and glial cells. NCAMs mediate interactions between different types of neurons and play an important role in the neurogenesis of fetal and adult brain by regulating cell proliferation, differentiation, and survival. Importantly, many proteins serve as secondary messengers and functional modifications can disrupt the physiological activity of neurons [25].
MDA, a product of polyunsaturated fatty acid oxidation, contributes to the weakening of the cell antioxidant defense. Compared to the healthy controls, patients with depression demonstrate increased serum MDA levels [26], as well as increased serum concentration of the markers of oxidative stress F2-isoprostane and 8-OHdG. 8-OHdG is a derivative of deoxyguanosine, and its presence in the cells indicates oxidative stress. Isoprostanes are generated in vivo by the free-radical oxidation of arachidonic acid and can be used as markers of LPO [21].
Activation of free radical production and LPO in individuals with mental disorders have been reported in numerous studies [9]. It was found that patients with schizophrenia display increased levels of lipid hydroperoxides and fluorescent Schiff bases. Elevated amounts of diene conjugates and MDA were observed in various psychoorganic diseases, while increased levels of Schiff bases, MDA, and superoxide dismutase activity were found in patients with Alzheimer’s disease and tardive dyskinesia. The activity of superoxide dismutase is also increased in patients with schizophrenia and manic-depressive psychosis [5, 27].
We examined patients with endogenous psychoses (attack-like schizophrenia and manic-depressive psychosis) in combination with various psychopathological syndromes resistant to psychopharmacotherapy. All subjects had significantly increased serum MDA levels compared to the healthy controls, whereas 1 to 3 sessions of plasmapheresis (therapeutic plasma exchange) produced clear activating and psycho-stimulating effects in these patients, resulting in the disappearance of existing symptoms of productive psychopathological disorders (depressions, obsessions, cenesthopathy, delirium, hallucinations) accompanied by the decrease in the level of serum MDA almost to the control range [28].
Hence, experimental results and published data suggest a significant activation of free radical- and peroxide-mediated processes in patients with endogenous mental disorders, resulting in the formation of substances exerting a toxic effect on metabolism. An adequate therapy normalizes the LPO processes and decreases the level of oxidative stress, as well as reduces endogenous intoxication.
MIDDLE-MASS ENDOTOXIC MOLECULES
Middle-mass endotoxic molecules (MMEMs) represent a fraction of serum components with molecular weights of 300 to 5000-6000 Da [29].
MMEMs (more than 30 biologically active substances) include various peptides, glycoproteins, degradation products of albumin, fibrinogen, thrombin, and other blood proteins, hormones, and other compounds [30-32]. A close attention to MMEMs is due to the high biological activity of some of their representatives capable of inhibiting metabolism of various compounds, impairing tissue respiration, membrane transport, erythropoiesis, and microcirculation, and exerting immunosuppressive, cytotoxic, neurotropic, and psychotropic properties [30, 33]. It was shown that MMEMs display the toxic effect at much lower concentrations than urea, uric acid, aromatic amines, and other substances [33]. It should be emphasized that the plasma content of MMEMs reflects the intensity of catabolic processes, as well as destructive cellular processes in the case of pathologies.
Despite that MMEMs exhibit the psychotropic activity, there are very few publications investigating their role in mental disorders. Thus, it was found that patients with progressive paranoid schizophrenia display significantly elevated MMEM levels compared to the healthy subjects [34].
We analyzed the clinical data with regard to MMEM levels in order to assess the extent of endotoxicosis more objectively and to follow up the therapeutic dynamics in patients with different pharmacotherapy-resistant forms of paranoid schizophrenia after plasmapheresis. The baseline (prior to the treatment) plasma concentration of MMEMs in the patients was more than 3-fold higher compared to the normal values. After plasmapheresis, all patients demonstrated improved clinical state and significantly decreased plasma MMEM content (p < 0.05) which, however, was still more than 2 times higher than in the control subjects (0.45 g/liter). We believe that aggravation of the patient’s condition and development of psychopharmacological resistance activate catabolic processes in the brain, in particular, proteolysis resulting in the elevated content of peptides of varying molecular weight. It should be remembered that all the aforementioned events occurred in parallel with the activation of oxidative stress and free-radical processes [28].
It is possible that the brain of individuals with endogenous psychoses accumulates pathological fractions of MMEMs, which eventually initiates endotoxicosis development. The latter was corroborated in our study. High-performance liquid chromatography of serum samples from the patients with pharmacotherapy-resistant paranoid schizophrenia revealed that prior to plasmapheresis, MMEMs included two components that disappeared after the treatment. Plasmapheresis improved the patients’ mental status and lowered the total MMEM level [35].
We also found that the content of MMEMs was increased more than 2-fold in the first-episode schizophrenia (FES) [36] and anxious depression [29]. The antipsychotic and antidepressant therapy improved the patients’ condition in parallel with lowering the MMEM level [29, 36].
Hence, the decline in the plasma MMEM concentration after the therapy together with markedly improved clinical and mental status may reflect an amelioration of endotoxicosis and a tendency toward the overall normalization of homeostasis. The content of MMEMs correlates with the severity of endotoxicosis and can serve as a prognostic biomarker. It should be emphasized that measuring the MMEM level is a relatively easy procedure that can be performed in any clinical or diagnostic laboratory.
Analysis of our experimental results and data published elsewhere allowed to suggest that the serum MMEM level in patients is an integral parameter that can be used to assess the extent of endogenous intoxication.
FUNCTIONAL PROPERTIES OF ALBUMIN
Many diseases are accompanied by excessive accumulation of toxic metabolites. Formation of complexes between these compounds and plasma proteins is one of the universal mechanisms used by the organism to respond to the elevated levels of metabolites [37, 38]. Serum albumin has a unique capacity to form such complexes. To determine the binding capacity of albumin, we used the stationary fluorescence spectroscopy with the K-35 fluorescent probe, because serum albumin is the only serum protein that binds this probe [39, 40].
We demonstrated that schizophrenia and various types of stress are accompanied by the conformational changes in the serum albumin molecule [39, 41]. However, stationary fluorescence spectroscopy provided no information on the nature of these conformational changes. Moreover, while investigating albumin in the FES patients, we found no changes in its conformation, although some other neurochemical parameters were altered similar to those in chronic schizophrenia [36], leading to the suggestion that the albumin molecule was indeed altered in the FES patients, but the sensitivity of stationary fluorimetry was insufficient to detect such fine changes. Scientists from the Moscow Research Institute of Psychiatry, Research Institute of Physical and Chemical Medicine, Lebedev Physical Institute (Moscow), and Russian Federal Nuclear Center of the All-Russian Research Institute of Experimental Physics (Sarov) have focused their efforts on creating novel technological approaches to investigate human serum albumin [42, 43]. As a result, a new technique was developed based on the analysis of kinetics of the subnanosecond fluorescence decay for the albumin-bound probe in subjects suffering from mental disorders. The use of time-resolved fluorescence spectroscopy allowed to selectively monitor the status of major binding sites in albumin.
Fine changes in the albumin molecule could be detected with nanotechnology-based techniques, including those using fluorescent molecular probes and analysis of fluorescence decay within a 10–11-10–9 second time range at a 33-picosecond resolution (nano- and picosecond fluorescence spectroscopy). The fluorescent probe K-35, which selectively binds to albumin in the plasma or serum, is 1.5 nm in size and easily integrates into specific molecular sites on the protein molecule [44].
At least three types of fluorescent molecules emerge after laser excitation of serum albumin with the bound molecular probe. In particular, K-35 binds to three sites in albumin with the fluorescence decay amplitude of 9, 3, and 1 ns (denoted as 9-, 3-, and 1-ns sites, respectively). Compared to stationary fluorimetry, fluorescence decay spectroscopy provides more detailed characterization of the binding sites in albumin. Instead of a single total averaged parameter – effective albumin concentration – it allows to observe the state of all three major binding sites and their changes in pathological processes [44].
For instance, patients with the FES vs. control subjects were found to have significant changes in the K-35-binding 3-ns site. To reveal the differences between the properties of albumin binding sites in the two groups, we subjected albumin molecules to other stress factors, e.g., changes in the medium ionic strength. The albumin globule in the FES patients vs. healthy subjects responded differently to the elevated ionic strength; in particular, the fluorescence decay amplitude characteristic of the 3-ns site was significantly lower in schizophrenia patients compared to the control [42].
Analysis of the K-35 fluorescence decay in the serum samples demonstrated that before the antidepressant therapy, the average decay amplitudes for all three sites in the serum of patients with melancholic depression were significantly (p = 0.025) elevated vs. control subjects.
Therefore, it may be assumed that alterations in the conformational and physicochemical properties of albumin disturb one of its crucial functions, namely, binding and transport of metabolites, which is accompanied by the emergence of excessively increased levels of metabolites in the blood [45], which might profoundly contribute to endogenous intoxication.
ALBUMIN THIOLS
Of particular interest is the state of the body systems providing defense against emerging intoxication and oxidative stress in patients with mental pathologies.
Plasma albumin has a single reduced thiol (SH-) group in Cys34 residue. Under physiological conditions, albumin thiols comprise up to 80% total plasma high-molecular weight thiol species [46].
It is believed that albumin non-specifically reacts with free radicals due to its high concentration in the extracellular space and relatively rapid turnover (~20 days) [47]. Irreversible oxidation of thiol group terminates the chain reaction of free-radical oxidation.
The antioxidant function of albumin depends not only on the reduced state of its thiol group, but also on the protein conformation [48]. The thiol status of albumin can serve as a marker of relevant conformational changes eventually affecting albumin potential to execute its antioxidant functions.
In connection with this, the concentration of thiol groups in albumin and their reactivity in different pathological conditions are of significant interest not only as factors of the antioxidant defense, but also as crucial parameters of the organism metabolism.
The significance of concentration and reactivity of albumin thiol groups in the oxidative events in the serum of individuals with mental disorders have never been evaluated before. The disturbance in this arm of the redox processes in mentally ill subjects might play a role in the development of metabolic disorders earlier defined as endogenous intoxication syndrome.
No significant differences in the content of reduced albumin thiol group were found between healthy individuals and patients with the FES.
The reactivity of SH-group (KV) characterizes the rate at which reduced (native) albumin thiol groups enters the thiol-disulfide exchange (i.e., reaction occurring in vivo during free radical oxidation).
The studies on the reactivity of albumin SH-groups remaining in the reduced state in the serum revealed that the reaction rate constant (KV) was significantly decreased in the FES patients, indicating reduced antioxidant activity of albumin thiol groups. Hence, FES is accompanied by changes in the serum albumin reactivity, which may affect the free-radical processes in the patient’s organism [49].
Albumin constitutes more than a half of total serum protein; it participates in the transport of multiple compounds and ensures defense against free-radical oxidation. However, the antioxidant function of albumin depends not only on the presence of reduced thiol groups, but also on the conformational state of albumin molecule. In albumin, the SH-group is positioned within a cleft (pocket) on the protein surface [50]. If this pocket is inaccessible for other molecules (e.g., free radicals) due to the protein conformation, albumin will be unable to participate in the redox reactions despite the presence of reduced SH-group. However, if the albumin molecule is unfolded to the extent when the SH-group becomes accessible for the interaction with any low concentration of free radicals, then almost entire albumin thiol pool will be capable of oxidation. Moreover, the properties of albumin thiol group may serve as a marker of protein conformational changes [49].
Earlier, we demonstrated significant metabolic changes in patients with FES that also affected the properties of binding sites and molecule conformation in serum albumin.
Impaired albumin function can profoundly impact the redox processes in vivo and increase the extent of endogenous intoxication [2].
NEUROTROPHIC FACTORS
Neurotrophic factors (neurotrophins) belong to a large protein group that includes brain-derived neurotrophic factor (BDNF), glial fibrillary acidic protein (GFAP), nerve growth factor (NGF), ciliary neurotrophic factor (CNTF), etc. The hallmark feature of these proteins is their ability to control the development of nervous system, as well as migration and differentiation of nerve cells. To a great extent, the functions of neurotrophic factors and related signaling pathways overlap.
CNTF (22 kDa) is a cytokine of the interleukin-6 (IL-6) family that is expressed mainly by glial cells in the central and peripheral nervous systems [51]. CNTF is a neurotrophin that acts as a neuroprotective agent [52] and plays an essential role in neurogenesis, neuroprotection, and cognitive processes. However, physiological importance of circulating CNTF remains unclear.
As demonstrated by the studies conducted at the Brain Pathology Laboratory, Moscow Research Institute of Psychiatry, the levels of CNTF in patients with melancholic depression are significantly higher than in healthy volunteers [53]. It has been demonstrated that depression is accompanied by the alterations in the blood–brain barrier (BBB) permeability [54]. We believe that in melancholic depression, CNTF is produced and released in the cerebral tissue at higher levels than in healthy subjects, but fails to exert its neuroprotective properties because of immediate removal to the circulation via the impaired BBB [53].
This hypothesis was confirmed in the studies on the therapy with the antidepressant venlafaxine, which had no effect on the serum CNTF level. The content of CNTF in the serum of treated patients was almost the same as upon their admission to the clinic, suggesting that the venlafaxine had no effect on the recovery of the BBB function.
The fate of CNTF released into the bloodstream remains unknown. We suggest that circulating CNTF undergoes degradation resulting in the emergence of large amounts of toxic peptide fragments contributing to the endogenous intoxication.
ENZYMES AND THEIR CONTRIBUTION TO THE OXIDATIVE STRESS AND ENDOGENOUS INTOXICATION
Monoamine oxidase (MAO) plays a special role in endotoxicosis. MAO is involved in deamination of monoamine neurotransmitters (catecholamines and indolamines), thereby reflecting the state of monoaminergic neurotransmitter system [55].
In particular, we showed that in patients with chronic schizophrenia [56], FES [36], and anxious depression [29], the level of platelet MAO is elevated by at least 100% (platelet MAO activity reflects MAO activity in the brain [55, 57]).
Events associated with the elevated MAO activity can be considered from several viewpoints. First, MAO is an integral constituent of the outer mitochondrial membrane. Impaired MAO activity observed in various endogenous disorders indicates that these pathologies are accompanied by the damage of membrane structures and emergence of toxic products in the circulation [27], accumulation of which in the blood contributes to the elevation of MMEM concentration and exacerbates endotoxicosis.
Second, increased MAO activity is accompanied by an increase in the content of hydrogen peroxide, which is generated in the MAO-catalyzed deamination reactions (via the Fenton reaction) and is the major source of free radicals in the brain [15]. Hence, increased MAO activity in mental pathologies promotes free-radical reactions and LPO. Moreover, high MAO activity facilitates increase in the level of toxic compounds (aldehydes and ammonia) produced in the deamination reaction in the blood and tissues.
Taken together, the aforementioned data suggest that impaired MAO activity significantly contributes to endotoxicosis.
Xanthine oxidase catalyzes xanthine oxidation with the formation of superoxide radical anion and hydrogen peroxide. The activity of xanthine oxidase was found to be significantly increased in the blood serum of patients with depression vs. control subjects [58, 59]. These results were confirmed by the reports on increased xanthine oxidase activity in various areas of the postmortem brain of patients with depression [60].
NADPH oxidase-catalyzes reactions with the generation of superoxide anion radical. The activity of neuronal NADPH oxidase positively correlates with the inflammation processes, inducing activation of microglial NADPH oxidase and nitric oxide synthase that act synergistically. This results in the formation of peroxynitrite eliciting the death of neurons. Peroxynitrite is a powerful oxidant, whose biological activity is similar to that of hydroxyl radical. Altered NADPH oxidase activity was found in patients with depression and schizophrenia [59].
The amino acid tryptophan, a precursor in the synthesis of serotonin, is metabolized to kynurenine by indoleamine 2,3-dioxygenase. Kynurenine metabolic pathways result in the emergence of 3-hydroxykynurenine and quinoline acid. Along with the elevated activity of indoleamine 2,3-dioxygenase, increased levels of 3-hydroxykynurenine and quinoline acid are typical of depression. Kynurenine, kynurenic acid, and xanthurenic acid (tryptophan metabolites) exert depressogenic, anxiogenic, and neurotoxic properties [61, 62].
SEMICARBAZIDE-SENSITIVE AMINOXIDASE
Serum semicarbazide-sensitive amine oxidase (SSAO) is an enzyme that differs from monoamine oxidase in a number properties [63]. It was suggested that SSAO takes part in the oxidation of some xenobiotics, e.g., pharmaceutical agents. SSAO substrates include endogenous metabolites, e.g., polyamines (spermine and spermidine) and aminoacetone synthesized from L-threonine. The products of polyamine and aminoacetone deamination, acrolein and methylglyoxal, respectively, are carcinogenic and cytotoxic compounds [64]. SSAO activity is impaired in a number of human diseases, such as cancer, diabetes, heart disorders, and burn disease [65]. However, the activity SSAO in mental disorders has not been assessed.
We found that anxious depression [29] and FES [36, 41] are accompanied by a significant decrease (approximately 30-40%) in the SSAO activity compared to the healthy controls. We believe that significant accumulation of endometabolites in the blood can profoundly contribute to the development of endogenous intoxication.
PATHOGENETIC MECHANISMS BEHIND ENDOGENOUS INTOXICATION AND TREATMENT APPROACHES
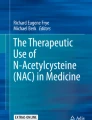
Based on the published reports and our own data, we propose a scheme of pathogenetic mechanisms underlying the development of endogenous intoxication in mental disorder (figure). It represents a closed circuit of transformations, so that alteration in any of its parts results in a cascade of further pathological impairments. The pathological mechanisms of endogenous intoxication are linked via monoamines and MAO to the general pathogenetic pathways involved in the development of endogenous psychoses (schizophrenia and depression). Thus, impaired metabolism of biogenic monoamines (particularly, dopamine) and altered MAO activity result in the excessive generation of free radicals. Catecholamines and, especially, dopamine, participate in the regulation of protein metabolism. Activation of catabolic processes causes a rise in the content of MMEMs because of the elevated proteolysis of cytoplasmic and membrane-bound proteins resulting in a significantly increased concentration of peptides of varying molecular weight [30] and emergence of pathological MMEM species [35].

Model of endogenous intoxication development
We discovered significantly elevated CNTF levels in patients with melancholic depression. The antidepressant therapy used to treat these patients had no effect on the serum CNTF concentration, which did not differ from the baseline level (before the treatment). It was assumed that patients with depression have an impaired BBB function that was not affected by the antidepressant therapy [53]. Our hypothesis on the BBB dysfunction and its increased permeability in melancholic depression was indirectly confirmed by the fact that addition of citicoline (cytidine-5′-diphosphocholine, nootropic drug) to the therapeutic protocol in patients with epilepsy helped to significantly decrease the elevated serum levels of CNTF and improved the clinical status of the patients [66]. This indicates that citicoline promoted some recovery of the damaged membrane structure, thus reducing the leakage of CNTF from the brain parenchyma.
The damage of membrane proteins and metabolic hypoxia observed in patients with mental diseases contribute to the impaired mitochondrial oxidative phosphorylation. It is known that hypoxia promotes reduction of some electron carriers within the mitochondrial electron transport chain, resulting in excessive free radical generation [67], which in turn, initiates LPO and its detrimental consequences [68], including dysfunction of proteins, enzymes, and receptors. Lipid hydroperoxides affect the properties of albumin by changing its conformation, thus impairing its detoxification and antioxidant functions, as well as exacerbating endotoxicosis. Elevated MMEM levels and emergence of “pathological” MMEM species can negatively impact the activity of enzymes (MAO) and albumin. The progression of the underlying disease further promotes the “vicious cycle” and aggravates endotoxicosis.
We believe that the proposed scheme not only allows us to interpret the mechanisms of endotoxicosis development, but also to suggest the approaches to break the “vicious cycle” and to ameliorate intoxication. Theoretically, the following arms can be targeted by pharmacological agents: MAO (monoamines) – by MAO inhibitors; free radicals (lipid peroxides) – by various antioxidants; MMEMs – by inhibitors of proteolysis; respiratory chain – by compounds correcting energy metabolism; recovery of the cell membrane functional state (including BBB) – by membrane-protecting compounds (citicoline).
Abbreviations
- BBB:
-
blood-brain barrier
- CNTF:
-
ciliary neurotrophic factor
- FES:
-
first-episode schizophrenia
- LPO:
-
lipid peroxidation
- MAO:
-
monoamine oxidase
- MDA:
-
malonic dialdehyde
- MMEM:
-
middle-mass endotoxic molecule
- ROS:
-
reactive oxygen species
References
Uzbekov, M. G., and Missionzhnik, E. Yu. (2000) Nonspecific endogenous intoxication syndrome as an integral component of mental disorders pathogenesis [in Russian], Ross. Psychiatrist. Zhurn., 4, 56-65.
Uzbekov, M. G., Gurovich, I. Ya., and Ivanova, S. A. (2016) Potential biomarkers of mental illness in systems approach [in Russian], Sots. Klin. Psikhiatr., 26, 98-109.
Stober, G., Ben-Shachar, D., Cardon, M., Falkai, P., Fonteh, A. N., Gawlik, M., Glenthoj, B., Grunblatt, E., Jablensky, A., Kim, Y-K., Kornhuber, J., McNeil, T., Muller, N., Oranje, B., Saito, T., Saoud, M., Schmitt, A., Schwartz, M., Thome, J., Uzbekov, M., Durany, N., and Riederer, P. (2009) Schizophrenia: from the brain to peripheral markers – a consensus paper of the WFSBP Task Force on biological markers, World J. Biol. Psychiatry, 10, 127-155, https://doi.org/10.1080/15622970902898980.
Uzbekov, M. G. (2019) Endogenous intoxication and its role in the pathogenetic mechanisms of mental disorders [in Russian], Sots. Klin. Psikhiatr., 29, 14-20.
Kohen, R., and Nyska, A. (2002) Invited review: oxidation of biological systems: oxidative stress phenomena, antioxidants, redox reactions, and methods for their quantification, Toxicol. Pathol., 30, 620-650, https://doi.org/10.1080/01926230290166724.
Davies, K. J. (1995) Oxidative stress: the paradox of aerobic life, Biochem. Soc. Symp., 61, 1-31, https://doi.org/10.1042/bss0610001.
Mehta, S. L., Kumari, S., Mendelev, N., and Li, P. A. (2012) Selenium preserves mitochondrial function, stimulates mitochondrial biogenesis, and reduces infarct volume after focal cerebral ischemia, BMC Neurosci., 13, 79, https://doi.org/10.1186/1471-2202-13-79.
Wong, E. Y. H., and Herbert, J. (2004) The corticoid environment: a determining factor for neural progenitors’ survival in the adult hippocampus, Eur. J. Neurosci., 20, 2491-2498, https://doi.org/10.1111/j.1460-9568.2004.03717.x.
Juszczyk, G., Mikulska, J., Kasperek, K., Pietrzak, D., Mrozek, W., and Herbet, M. (2021) Chronic stress and oxidative stress as common factors of the pathogenesis of depression and Alzheimer’s disease: the role of antioxidants in prevention and treatment, Antioxidants, 10, 1439-1470, https://doi.org/10.3390/antiox10091439.
Jesulola, E., Micalos, P., and Baguley, I. (2017) Understanding the pathophysiologyof depression: from monoamines to the neurogenesis hypothesis model – are we there yet?, Behav. Brain Res., 341, 25-38, https://doi.org/10.1016/j.bbr.2017.12.025.
Sies, H., Berndt, C., and Jones, D. P. (2017) Oxidative stress, Ann. Rev. Biochem., 86, 715-748, https://doi.org/10.1146/annurev-biochem-061516-045037.
Pizzino, G., Irrera, N., Cucinotta, M., Pallio, G., Mannino, F., Arcoraci, V., Squadrito, F., Altavilla, D., and Bitto, A. (2017) Oxidative stress: harms and benefits for human health, Oxid. Med. Cell. Longev., 2017, e8416763, https://doi.org/10.1155/2017/8416763.
Wojsiat, J., Zoltowska, K. M., Laskowska-Kaszub, K., and Wojda, U. (2018) Oxidant/antioxidant imbalance in Alzheimer’s disease: the therapeutic and diagnostic prospects, Oxid. Med. Cell. Longev., 2018, 6435861, https://doi.org/10.1155/2018/6435861.
Uzbekov, M. G. (2022) Oxidative stress and depression: issues of pathogenesis [in Russian], Sots. Klin. Psikhiatr., 32, 73-81.
Halliwell, B. H., and Gutteridge, J. M. (2007) Free Radicals in Biology and Medicine, Fourth Edition, Oxford, Oxford Univ. Press.
Uzbekov, M. G. (2015) Lipid peroxidation and antioxidant systems in mental illness [in Russian], Report II, Sots. Klin. Psikhiatr., 25, 92-101.
Ayala, A., Munoz, M. F., and Argeuelles, S. (2014) Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal, Oxid. Med. Cell. Longev, 2014, 360438, https://doi.org/10.1155/2014/360438.
Gałecki, P., Szemraj, J., Bienkiewicz, M., Zboralski, K., and Gałecka, E. (2009) Oxidative stress parameters after combined fluoxetine and acetylsalicylic acid therapy in depressive patients, Hum. Psychopharmacol., 24, 277-286, https://doi.org/10.1002/hup.1014.
Maes, M., Mihaylova, I., Kubera, M., Uytterhoeven, M., Vrydags, N., and Bosmans, E. (2011) Lower whole blood glutathione peroxidase (GPX) activity in depression, but not in myalgic encephalomyelitis/chronic fatigue syndrome: another pathway that may be associated with coronary artery disease and neuroprogression in depression, Neuroendocrinol. Lett., 32, 133-140.
Yager, S., Forlenza, M. J., and Miller, G. E. (2010) Depression and oxidative damage to lipids, Psychoneuroendocrinology, 35, 1356-1362, https://doi.org/10.1016/j.psyneuen.2010.03.010.
Forlenza, M. J., and Miller, G. E. (2006) Increased serum levels of 8-hydroxy-2’-deoxyguanosine in clinical depression, Psychosom. Med., 68, 1-7, https://doi.org/10.3109/15622971003797241.
Verhoeven, J. E., Revesz, D., Epel, E. S., Lin, J., Wolkowitz, O. M., and Penninx, B. W. (2014) Major depressive disorder and accelerated cellular aging: results from a large psychiatric cohort study, Mol. Psychiatry, 19, 895-901, https://doi.org/10.1038/mp.2013.151.
Simon, N. M., Smoller, J. W., McNamara, K. L., Maser, R. S., Zalta, A. K., Pollack, M. H., Nierenberg, A. A., Fava, M., and Wong, K. K. (2006) Telomere shortening and mood disorders: preliminary support for a chronic stress model of accelerated aging, Biol. Psychiatry, 60, 432-435, https://doi.org/10.1016/j.biopsych.2006.02.004.
Kawanishi, S., and Oikawa, S. (2004) Mechanism of telomere shortening by oxidative stress, Ann. NY Acad. Sci., 1019, 278-284, https://doi.org/10.1196/annals.1297.047.
Bakunina, N., Pariante, C. M., and Zunszain, P. A. (2015) Immune mechanisms linked to depression via oxidative stress and neuroprogression, Immunology, 144, 365-373, https://doi.org/10.1111/imm.12443.
Gałecki, P., Szemraj, J., Bienkiewicz, M., Florkowski, A., and Gałecka, E. (2009) Lipid peroxidation and antioxidant protection in patients during acute depressive episodes and in remission after fluoxetine treatment, Pharmacol. Rep., 61, 436-447, https://doi.org/10.1016/s1734-1140(09)70084-2.
Prilipko, L. L., Erin, A. N., Belyaev, B. S., Pyatnitsky, A. N., Syunyakov, S. A., Panteleeva, G. P., Panteleeva, G. P., Tsutsulkovskaya, M. Ya., and Lideman, R. R. (1987) Activation of lipid peroxidation in patients with schizophrenia and manic-depressive psychosis [in Russian], Zhurn. Nevrol. Psikhiatr. im. S.S. Korsakova, 1, 100-103.
Uzbekov, M. G., Missionzhnik, E. Yu., Malin, D. I., and Neduva, A. A. (1997) Altered level of medium molecules and some other biochemical parameters in patients with endogenous psychoses during plasmapheresis [in Russian], Sots. Klin. Psikhiatr., 7, 93-99.
Uzbekov, M., Misionzhnik, E., Maximova, N., and Vertogradova, O. (2006) Biochemical profile in patients with anxious depression under the treatment with serotonergic antidepressants with different mechanisms of action, Hum. Psychopharmacol. Clin. Exp., 21, 109-115, https://doi.org/10.1002/hup.749.
Ringoir, S., Vanholder, R., and Massry, S. G. (1987) Uremic Toxins, New York–London, Academic Press.
Nikolaychik, V. V., Moin, V. M., Kirkovsky, V. V., Mazur, L. I., Lobacheva, G. A., Bychko, G. N., and Baratashvili, G. G. (1991) Method for “medium molecules” detection [in Russian], Lab. Delo, 10, 13-18.
Chalenko, V. V. (1991) Potential cause for increased concentration of medium molecules in pathology [in Russian], Patol. Fiziol. Eksp. Ter., 4, 13-14.
Tupikova, Z. A. (1983) Medium-molecule uremic toxins (literature review) [in Russian], Vopr. Med. Khim., 1, 2-10.
Turyanitsa, I. M., Mishanich, I. I., and Rostoka, L. M. (1988) Treatment-related medium molecule spectrum in the blood serum of patients with continuous paranoid schizophrenia [in Russian], Zhurn. Nevrol. Psikhiatr. im. S.S. Korsakova, 88, 109-111.
Shikhov, S. N., Uzbekov, M. G., and Malin, D. I. (2000) Altered “middle molecules” spectrum in patients with depressive disorders during plasmapheresis [in Russian], Materialy 13 S’ezda Psikhiatrov Rossii, pp. 373-374.
Uzbekov, M. G., Misionzhnik, E. Yu., Shmukler, A. B., Gurovich, I. Ya., Gryzunov, Yu. A., Smolina, N. V., Kalinina, V. V., Sokolova, T. N., Moskvitina, T. A., and Shevchenko, V. A. (2009) Altered monoamine oxidase activity and indicators of endogenous intoxication in patients with first-episode schizophrenia [in Russian], Zhurn. Nevrol. Psikhiatr. im. S.S. Korsakova, 109, 48-52.
Gryzunov, Yu. A., and Dobretsov, G. E. (1994) Serum Albumin in Clinical Medicine. Book 1 [in Russian], Irius, Moskva.
Gryzunov, Yu. A., and Dobretsov, G. E. (1998) Serum Albumin in Clinical Medicine. Book 2 [in Russian], GEOTAR, Moskva.
Gryzunov, Yu. A., Misionzhnik, E. Yu., Uzbekov, M. G., and Molodetskikh, A. V. (1994) The effect of haloperidol therapy on the dynamics of serum albumin binding capacity in patients with schizophrenia [in Russian], Klin. Lab. Diagn., 5, 31-33.
Moin, V. M., Misionzhnik, E. Yu., Kuznetsova, Z. I., Gryzunov, Yu. A., Kirkovskiy, V. V., Uzbekov, M. G., and Zubovskiy, D. I. (1994) Some characteristics of the method and reagents for the fluorescent determination of the effective and total serum albumin concentration [in Russian], Klin. Lab. Diagn., 5, 33-35.
Uzbekov, M. G., Misionzhnik, E. Yu., Gurovich, I. Y., and Shmukler, A. B. (2013) Aspects of metabolic changes in first-episode drug-naïve schizophrenic patients, Acta Neuropsychiatr., 25, 268-274, https://doi.org/10.1017/neu.2013.1.
Uzbekov, M. G., Syreyshchikova, T. I., Babushkina, T. A., Smolina, N. V., Kalinina, V. V., Dobretsov, G. E., Klimova, T. P., Peregudov, A. S., Misionzhnie, E. Yu., and Tokarev, V. A. (2013) High-technology approaches allowing to detect conformational changes in the albumin molecule in first-episode schizophrenia patients [in Russian], Sib. Vestnik Psikhiatr. Narkol., 1, 26-30.
Smolina, N., Gryzunov, Yu., Syrejshchikova, T., Uzbekov, M., Dobretsov, G., Misionzhnik, E., Komar, A., and Tokarev, V. (2009) Albumin binding sites in first- episode drug-naive patients with paranoid schizophrenia studied by subnanosecond fluorescence spectroscopy, Eur. Arch. Psychiatry Clin. Neurosci., 259, 98.
Smolina, N. V., Syreyshchikova, T. I., Uzbekov, M. G., and Dobretsov, G. E. (2015) Fluorescent Probes as a Source of Clinically Relevant Information [in Russian], in Fundam. Sci. Med. Biophys. Med. Technol. (Grigor’ev, A. I., Vladimirov, Yu. A., eds) MAKSPRESS, Moscow, pp. 293-327.
Babushkina, T. A., Klimova, T. P., Peregudov, A. S., Gryzunov, Yu. A., Smolina, N. V., Dobretsov, G. E., and Uzbekov, M. G. (2012) Study of high-resolution H1 nuclear magnetic resonance spectra of the serum and its albumin fraction in patients with the first schizophrenia episode, Bull. Exp. Biol. Med., 152, 748-751, https://doi.org/10.1007/s10517-012-1622-y.
Jocelyn, P.C. (1972) Biochemistry of the SH Group, London–New York, Academic Press.
Pikkering, U. F. (1977) Modern Analytical Chemistry [in Russian], Khimiya, Moscow.
Gryzunov, Y. A., Aarroyo, A., and Vigne, J. L. (2003) Binding of fatty acids facilitates oxidation of cysteine-34 and converts copper-albumin complexes from antioxidants to prooxidants, Arch. Biochem. Biophys., 413, 53-66, https://doi.org/10.1016/s0003-9861(03)00091-2.
Brilliantova, V. V, Smolina, N. V., Syreyshchikova, T. I., Uzbekov, M. G., and Dobretsov, G. E. (2018) The state of albumin thiol groups in patients with the first episode of schizophrenia, Neurochem. J., 12, 107-110, https://doi.org/10.7868/S102781331801003X.
Peters, T. J. (1995) All about Albumin: Biochemistry, Genetics and Medical Applications, San Diego, Academic Press.
Akahori, Y., Takumoto, N., Inoue, S., Nakatsukasa, H., Masuyama, H., and Hiramatsu, Y. (2010) Circulating levels of ciliary neurotrophic factor in normal pregnancy and preeclampcia, Acta Med. Okayama, 64, 129-136, https://doi.org/10.18926/AMO/32847.
Brondino, N., Rocchetti, M., and Fusar-Poli, L. (2018) Increased CNTF levels in adults with autism spectrum disorders, World J. Biol. Psych., 19, 1-5, https://doi.org/10.1080/15622975.2018.1481999.
Uzbekov, M., and Shikhov, S. (2019) Ciliary neurotrophic factor disturbances in patients with melancholic depression, Biomed. J. Sci. Tech. Res., 13, 1-2, https://doi.org/10.26717/BJSTR.2019.13.002408.
Najjar, S., Pearlman, D., Devinsky, O., Najjar, A., and Zagzag, D. (2013) Neurovascular unit dysfunction with blood-brain barrier hyperpermeability contributes to major depressive disorder: a review of clinical and experimental evidence, J. Neuroinflamm., 10, 142-158, https://doi.org/10.1186/1742-2094-10-142.
Uzbekov, M. (2021) Monoamine oxidase as a potential biomarker of the efficacy of treatment of mental disorders, Biochemistry (Moscow), 86, 773-783, https://doi.org/10.1134/S0006297921060146.
Mosolov, S. N., Uzbekov, M. G., Saykin, M. A., Misionzhnik, E. Yu., Tsukarzi, E. E., and Molodetskikh, A. V. (1999) Intravenous low-intensity helium-neon laser therapy and change in number of biochemical parameters in patients with schizophrenia resistant to psychopharmacotherapy [in Russian], Sots. Klin. Psikhiatr., 9, 57-62.
Chen, K., Wu, H. F., and Shih, J. C. (1993) Thededuced amino acid sequences of human platelet and frontal cortex monoamine oxidase are identical, J. Neurochem., 61, 187-190, https://doi.org/10.1111/j.1471-4159.1993.tb03554.x.
Herken, H., Gurel, A., Selek, S., Armutcu, F., Ozen, M. E., Bulut, M., Kap, O., Yumru, M., Savas, H. A., and Akyol, O. (2007) Adenosine deaminase, nitric oxide, superoxide dismutase and xanthine oxidase in patients with major depression: impact of antidepressant treatment, Arch. Med. Res., 38, 247-252, https://doi.org/10.1016/j.arcmed.2006.10.005.
Martorell, M., Lucas, X., Alarcon-Zapata, P., Capó, X., Quetglas-Llabrés, M. M., Tejada, S., and Sureda, A. (2021) Targeting xanthine oxidase by natural products as a therapeutic approach for mental disorders, Curr. Pharm. Des., 27, 367-382, https://doi.org/10.2174/138161282666600621165839.
Michel, T.M., Camara, S., and Tatschner, T. (2010) Increased xanthine oxidase in the thalamus and putamen in depression, World J. Biol. Psychiatry, 11, 314-320, https://doi.org/10.3109/15622970802123695.
Halliwell, B. (2014) Systems Biology of Free Radicals and Antioxidants, Berlin, Springer.
Vavakova, M., Durackova, Z., and Trebaticka, J. (2015) Markers of oxidative stress and neuroprogression in depression disorder, Oxid. Med. Cell. Longev., 2015, 898393, https://doi.org/10.1155/2015/898393.
Strolin Benedetti, M., Whomsley, R., and Baltes, E. (2006) Involvement of enzymes other than CYPs in the oxidative metabolism of xenobiotics, Expert Opin. Drug Metab. Toxicol., 2, 895-921, https://doi.org/10.1517/17425255.2.6.895.
Callingham, B. A., Crosbie, A. E., and Rous, B. A. (1995) Some aspects of the pathophysiology of semicarbazide-sensitive amine oxidase enzymes, Prog. Brain Res., 106, 305-321, https://doi.org/10.1016/s0079-6123(08)61227-3.
Toninello, A., Pietrangeli, P., De Marchi, U., Salvi, M., and Mondovi, B. (2006) Amine oxidases in apoptosis and cancer, Biochim. Biophys. Acta, 1765, 1-13, https://doi.org/10.1016/j.bbcan.2005.09.001.
Uzbekov, M., and Musina, L. (2018) Serum ciliary neurotrophic factor concentration as a potential biomarker of efficacy of citicoline pharmacotherapy of temporal-lobe epilepsy in women, Theranost. Brain Spine Neural Disord., 3, 555619, https://doi.org/10.19080/JOJS.2019.03.555619.
Feher, J., Csomos, G., and Vereckei, A. (1985) Free Radical Reactions in Medicine, Heidelberg, Springer-Verlag, https://doi.org/10.1007/978-3-642-83104-1.
Uzbekov, M. G. (2014) Lipid peroxidationand antioxidant systems in mental illness [in Russian], Report I, Sots. Klin. Psikhiatr., 4, 97-103.
Acknowledgments
I am cordially grateful to my colleagues, who were involved in the studies described in the review: Yu.A. Gryzunov, I.Ya. Gurovich, G.E. Dobretsov, S.A. Ivanova, V.N. Krasnov, A.B. Shmukler, N.M. Maksimova, E.Yu. Missionzhnik, N.V. Smolina, S.N. Shikhov, V.V. Brilliantova, and E.B. Skokina.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The author declares no conflict of interest. All studies involving human subjects were carried out in accordance with the Declaration of Helsinki on Ethical Principles for Medical Research, ethical standards of the National Committee on Research Ethics and were approved by the Ethics Committee of the Moscow Research Institute of Psychiatry. All participants provided a written informed consent to participate in the study.
Rights and permissions
Open access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Uzbekov, M.G. Pathogenetic Mechanisms of Mental Disorders: Endogenous Intoxication. Biochemistry Moscow 88, 491–501 (2023). https://doi.org/10.1134/S0006297923040053
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S0006297923040053