
Abstract
Background
The incidence of cognitive impairment is increasing with an aging population. Develo** effective strategies is essential to prevent dementia. Higher education level is associated with better baseline cognitive performance, and reading activities can slow down cognitive decline. However, it is unclear whether education and reading activities are synergistic or independent contributors to cognitive performance.
Methods
This was a sub-study of an ongoing prospective community cohort of China National Clinical Research Center Alzheimer’s Disease and Neurodegenerative Disorder Research (CANDOR). Demographic and clinical information, educational levels, and reading activities were collected. All participants finished neuropsychological testing batteries and brain MRIs. We analyzed cognitive performance and brain structures with education and reading activities.
Results
Four hundred fifty-nine subjectively cognitively normal participants were enrolled in the study. One hundred sixty-nine (36.82%) of them had regular reading activities. Participants in the reading group had better performance in all cognitive tests compared with those in the non-reading group, but no difference in brain MRI variables. Participants with higher education levels (more than 13 years) had better cognitive performance and higher hippocampal volumes. In low education groups (less than 12 years), more reading activities were associated with better cognitive test scores.
Conclusions
Both education and reading activities are important and synergistic for baseline cognitive function. Higher education level is associated with larger hippocampal volumes. Education may stimulate the growth and development of the hippocampus. Reading activities help to maintain and improve cognitive function in people with low levels of education.
Trial registration
NCT04320368.
Similar content being viewed by others

Introduction
Aging is the most important risk factor for dementia. With an aging population, dementia has cast an enormous social and economic burden around the world [1, 2]. Develo** effective strategies is essential to prevent dementia [3]. It has been reported there are modifiable risk factors for dementia and modifying 12 of them may prevent or delay up to 40% of dementia [4]. The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), a multicenter randomized controlled trial, reported beneficial effects on cognition through multimodal intervention including cognitive training [5]. Reading activities and other mental stimulation help to slow down cognitive decline [6, 7].
High education level is associated with better cognitive performance and lower likelihood to have Alzheimer’s disease (AD) [8, 9]. High education level may delay cognitive decline in individuals with subjective cognitive decline [10, 11]. However, although education is associated with baseline cognitive performance, it doesn’t affect the rate of cognitive decline [12], nor does it affect the neuropathological changes related to dementia, such as amyloid plaques and tangles [13].
Previous research compared the influence of reading activities and education on cognition and found that reading activities were associated with a lower risk of dementia even in late life, independent of education and other related factors [6, 7], while another study demonstrated that reading activities have a stronger relationship than education with executive function tests [14].
It is inconclusive whether reading activities and education are synergistic or independent contributors to cognitive performance. In this prospective community-based cohort study, we try to answer the following questions. First, what are the relationships of education and reading activities with cognitive performance on domain-specific tests? Second, are education and/or reading activities associated with brain structure? Third, can reading activities compensate for lower levels of education?
Methods
Study design and participants
This study was a sub-study of an ongoing prospective community-based cohort study of the China National Clinical Research Center Alzheimer's Disease and Neurodegenerative Disorder Research (CANDOR). CANDOR was started in July 2019 and planned to enroll one thousand and five hundred participants, including individuals with normal cognition (NC), mild cognitive impairment (MCI), and dementia. Demographic information and past medical history were collected. All participants were required to have a study partner to provide an independent evaluation of daily and social functions. They underwent detailed assessments for cognition and functional abilities, a comprehensive neuropsychological battery (described below in “Neuropsychological assessment”) including the Mini-Mental State Examination (MMSE), Clinical Dementia Rating (CDR), and brain MRIs. All enrolled participants for this study (1) were subjectively cognitively normal; (2) aged 40–100 years old; (3) had at least 3 years of education; (4) had no condition known to affect cognitive function, such as Alzheimer’s Disease, vascular dementia, Lewy body dementia, frontotemportal dementia, Parkinson’s disease, epilepsy, stroke, hydrocephalus, multiple sclerosis, traumatic brain injuries, genetic disorders affecting cognition, alcoholism, uncontrolled depression, or other psychiatric disorders; (5) had no uncontrolled neoplasia, or severe pulmonary, cardiovascular, metabolic, infectious, inflammatory, or endocrine diseases. We excluded individuals with less than 3 years of education because people started to learn how to read and write in the third year of elementary school in China. Therefore, people who have less than three years of education will have difficulties in reading.
To assess the relationship between education and leisure reading activities, we defined regular reading activities as reading at least one book per month on average for at least one year. We divided the participants as follows. First, participants were divided into 2 groups based on their reading activities. Reading activities were detailed, including (1) reading materials, such as paper books, e-books, and audio-books; (2) reading content, such as literature books, and non-literature books; (3) the total number of books, which was calculated as the average number of books read per month ×12 months × years of reading. In participants with reading habits, we divided them further into several groups based on reading years, reading content and reading materials. Second, participants were divided based on their education. Previous studies analyzed education by ≤9, 10–12, and ≥13 years [15, 16]. In our study, the average education years of all participants were 12.12 years. Therefore, we used a 12-year cut-off to divide participants into two groups: low education (≤12 years, high school education or below, under the average education level) and high education (≥13 years, college education or above, over the average education level). Third, participants were divided into four groups based on education years and reading activities: low education (educational years ≤12) with and without reading activities (groups 1 and 2), and high education (educational years ≥13) with and without reading activities (groups 3 and 4).
Standard protocol approvals, registrations, and patient consents
This protocol was approved by the Institutional Review Board of Bei**g Tiantan Hospital (approval number: KY 2019-004-007) and was in accordance with relevant guidelines and regulations. Written informed consent was obtained from each participant.
Neuropsychological assessment
Thirteen neuropsychological tests were completed at the visit, including (1) tests for overall cognitive performance: Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), and Clinical Dementia Rating (CDR) with global scores; (2) Tests for specific cognitive domain: Rey Auditory Verbal Learning Test (RAVLT) [17], Rey-Osterrieth Complex Figure Test (ROCF) [18], Stroop Color-Word Test-Victoria version [19], Trail Making Test-A (TMT- A) and Trail Making Test B (TMT -B) [20], clock drawing test (CDT), Boston Naming Test (BNT), Digit Span Test (DST), and Symbol Digit Modalities Test (SDMT); and (3) Neuropsychiatry Inventory (NPI). These tests were administered by experienced neuropsychologists who were blinded to group assignment.
MRI assessment
All participants completed the brain MRI to exclude other demonstrable neurological diseases. Quantitative measures of signal-to-noise ratio, uniformity, and geometric distortion were conducted in each research center. 3.0 T-MRI was used with the scanning thickness not exceeding 1.5mm. The three-dimensional T1 weighted images were corrected for intensity non-uniformity with the N4 algorithm. Brain surface was reconstructed using FreeSurfer (version 7.2.0, http://surfer.nmr.mgh.harvard.edu/) recon-all pipeline. The cortical thickness and volume of the total brain, nuclei, gray matter white matter, and white matter lesion were all obtained with this pipeline. Regional cortical thickness was obtained and statistical analysis was performed.
Statistical analysis
The analysis was conducted with SPSS 24.0. Continuous variables were characterized as mean plus and/or minus standard deviations (SD). T-test or nonparametric test was used by the characteristic of the distribution. Categorical variables were analyzed by Pearson’s χ2 tests. We performed logistic regression analysis to evaluate the association between reading and CDR (CDR=0 or >0), linear regression analysis for the association of reading and neuropsychological assessment, and linear regression analysis for education and brain structure. The regression analyses were independent of age and sex in Table 2 model 1 and Table 5. The regression analyses were independent of age, sex, and education in Table 2 model 2. We also performed the collinearity analysis in every linear regression analysis, and all the results showed no collinearity between every included independent variable.
Results
From July 31, 2019, to August 1, 2021, 694 individuals were screened from communities in Bei**g, Shijiazhuang, and Langfang, all in northern China. They completed standard baseline assessments. 459 were enrolled in the study who had both valid brain MRI examination and cognitive evaluation (Fig. 1). Among them, 169 (36.82%) had regular reading activities. There was no significant difference in age, sex, medical history, and mood assessment (NPI) between the two groups (Table 1). The reading group had more years of education and better cognitive performance than the non-reading group, including CDR, MMSE, MoCA, DST, RAVLT, ROCF, Stroop D and W time, TMT-A and B, BNT, SDMT, and CDT. However, there was no difference in cortical thickness and hippocampal volume in either hemisphere between the two groups.

Study flowchart. Shown is the flowchart of the study enrollment
Logistic and linear regression were used to assess confounding factors (Table 2). Reading activities were associated with better cognitive performance, such as MMSE (beta 2.193, 95%CI: 1.463–2.923, P<0.001), independent of age and sex in model 1. In model 2, when education was taken into account, reading activities showed similar effects in MoCA and Boston Naming; significant but less effects in MMSE, DST, ROCF delayed recall, Stroop D and W time, TMT-A and SDMT, but no effects in CDR, RAVLT, ROCF copy, TMT-B, and CDT.
Education had a remarkable effect on cognitive performance (Table 3). Participants with high education scored higher in all cognitive tests than those with low education. They also have higher hippocampal volumes on both sides (Fig. 2).

Hippocampal volumes at different education levels. Shown is the right (open box) and left (closed dot) hippocampal volume associated with different education levels
Reading years and reading content had little impact on cognitive performance and brain structure (Supplemental Tables 1 and 2). Reading e-books showed no obvious cognitive benefits than paper books, and listening to audio-books performed better in MoCA, BNT, and SDMT (Supplemental Table 3).
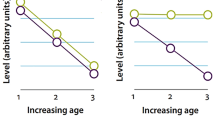
To assess if reading activities have a compensatory effect for low education, we divided participants into four groups: low education (educational years ≤12) with and without reading activities (groups 1 and 2), and high education (educational years ≥13) with and without reading activities (groups 3 and 4). Reading activities improved most cognitive tests (except RAVLT, ROCF copy, and TMT-B) in the low education group (group 1 better than group 2, Table 4). By reading more books, participants with low education could achieve similar or even better cognitive scores than those with high education in MMSE, MoCA, DST, and BNT (Fig. 3). In the high education groups, reading activities showed few effects probably due to ceiling effects (group 3 similar to group 4, Table 4).

Cognitive performance associated with reading activities at different education levels. Shown is that by reading more books, participants with low education (blue line) could achieve similar or even better cognitive scores than those with high education (red line) in a MMSE, b MoCA, c DST, and d BNT. a MMSE (education ≤12: beta, 95% CI 0.1035 [0.0009, 0.0198], P=0.0316; education ≥13: beta, 95% CI 0.0012 [−0.0035, 0.0059], P=0.6113); b MoCA (education ≤12: beta, 95% CI 0.0136 [0.0031, 0.0241], P=0.0112; education ≥13: beta, 95% CI 0.0040 [−0.0020, 0.0100], P=0. 1856); c DST (education ≤12: beta, 95% CI 0.0086 [0.0035, 0.0136], P=0.0009; education ≥13: beta, 95% CI 0.0008 [−0.0037, 0.0053], P=0.7199); d BNT (education ≤12: beta, 95% CI 0.0166 [0.0076, 0.0256], P=0.0003; education ≥13: beta, 95% CI 0.0012 [0.0012, 0.0100], P=0.0371)
The linear regression related to hippocampal volume on either side showed that years of education influenced hippocampal volume with beta1 14.999 [4.906, 25.092], P=0.004 and beta2 15.816 [4.949, 26.683], P=0.004 (Table 5), regardless of age and sex.
Discussion
In this community-based subjectively cognitively normal population, participants with regular reading activities showed better cognitive performance in overall cognitive abilities, attention, memory, language, visuospatial and executive function. This effect is independent of brain volume, especially hippocampal volume. A prospective cohort study showed that increased participation in cognitive activities (including reading) was associated with better memory [21]. Although reading activities involve multiple brain areas, subgroup analysis of the FINGER study has shown that the multi-domain intervention has no effects on brain volume, cortical thickness, and white matter lesion [22].
Education was related to cognition across all tested domains. Reading is associated with all tested domains controlled with age and sex. However, when education was included in the analysis, the effect of reading on cognitive assessment weakened, indicating a stronger correlation between education level and cognition. Reading is a complex task that involves various brain areas, including the insular and frontal opercular cortex, lateral temporal cortex, and early auditory cortex with the positive reaction and inferior temporal and motor cortex with the negative reaction [23]. However, we did not see a difference in the cortical thickness and the hippocampus between reading and non-reading groups. This suggests that reading activities may help to improve cognitive function in participants with low education level (≤12 years) independent of brain volume. In some cognitive domains, the cognitive performance gap caused by education level is decreased with the increase in reading activities. Reading is a good way to fill the cognitive gap brought about by lack of education, especially in language, non-verbal memory, and executive function.
In this study, participants with high education level had higher hippocampal volume. Larger hippocampal volumes may be associated with higher intelligence quotient (IQ), practice in hippocampus-related function (e.g., learning and memory), lifestyle, and medial/historical factors (neurotoxic effects of obesity, diabetes mellitus, hypertension, hypoxic brain injury, obstructive sleep apnea, bipolar disorder, clinical depression, and head trauma) [24]. Higher education level is favorable to the neurological task performance [10, 12, 25,26,27], but not to AD-related pathology [28].
MMSE and MoCA are screening tests for cognition. Their cut-off scores are based on education levels. In this study, participants with low education but reading more books showed no difference in MMSE and MoCA compared with participants with high education level. It suggests that people with low education but who read a lot probably should be screened at the same level as those who are more educated.
Audio devices are a new form of reading activities and have become popular. It is suggested that audiobooks are probably better than non-audio books at improving cognitive function. Young children learned more words from the e-book and from the audio narrator than print books [29]. Different types of books may influence the ability to retrieve information. Listening to audiobooks may stimulate more brain areas to have positive effects on cognition, especially memory and executive function. Since poor vision is not uncommon in the elderly, audiobooks are a better tool for old people to enjoy reading activities.
The strength of this study is a large community-based cohort with detailed neuropsychological testing batteries and brain MRI analysis. But the study has several limitations. First, this is an observational, cross-sectional study. Correlation does not imply causation. To study the causative effect of reading activities on cognitive function, a randomized clinical trial is warranted. Participants with certain education levels would be assigned with different reading activities. Other intellectual activities besides leisure reading would also be taken into account. Second, we enrolled participants with subjectively normal cognitive function to represent community-based cohorts. The average CDR was 0.18 although a few participants with a CDR more than 0.5. Ongoing longitudinal follow-ups will allow us to assess the relationship between risk/protective factors and the conversion to dementia. Third, all participants were enrolled from northern China. There is likely a difference in culture, education, and environmental factors among different regions in China. To expand population sampling is needed in future studies. Fourth, higher education level is associated with larger hippocampal volumes. One explanation is that education may stimulate the growth and development of the hippocampus. Alternatively, people with larger hippocampal volume may have a better chance to acquire higher education. Fifth, the study may have a recall bias since reading activities were recorded by self-reported questionnaires. People might under- or overestimate the books they read. Objective measures (e.g., a shop** receipt of purchased books) may help to validate the finding. Finally, reading activities as measured by reading books are mainly leisure reading. It does not take into account of all activities related to intellectual activities. Individuals who do a lot of reading or research at work but have little time in reading books outside of work may be underestimated in reading activities.
Conclusions
Participants in reading groups with less education (educational years ≤12) had better cognitive performance than the ones in non-reading groups. Education affects more than reading habits in every cognitive domain and in hippocampal volume.
Availability of data and materials
SL and JS had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Abbreviations
- CANDOR:
-
China National Clinical Research Center Alzheimer's Disease and Neurodegenerative Disorder Research
- FINGER:
-
Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability
- AD:
-
Alzheimer’s disease
- MRI:
-
Magnetic resonance imaging
- NC:
-
Normal cognition
- MCI:
-
Mild cognitive impairment
- MMSE:
-
Mini-Mental State Examination
- CDR:
-
Clinical Dementia Rating
- MoCA:
-
Montreal Cognitive Assessment
- RAVLT:
-
Rey Auditory Verbal Learning Test
- ROCF:
-
Rey-Osterrieth Complex Figure Test
- TMT:
-
Trail Making Test
- CDT:
-
Clock drawing test
- BNT:
-
Boston Naming Test
- DST:
-
Digit Span Test
- SDMT:
-
Symbol Digit Modalities Test
- NPI:
-
Neuropsychiatry Inventory
- SD:
-
Standard deviations
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- WM:
-
White matter
- eTIV:
-
Estimated total intracranial volume
References
Patnode CD, Perdue LA, Rossom RC, Rushkin MC, Redmond N, Thomas RG, et al. Screening for Cognitive Impairment in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2020;323(8):764–85. https://doi.org/10.1001/jama.2019.22258.
Chan KY, Wang W, Wu JJ, Liu L, Theodoratou E, Car J, et al. Epidemiology of Alzheimer's disease and other forms of dementia in China, 1990–2010: a systematic review and analysis. Lancet. 2013;381(9882):2016–23. https://doi.org/10.1016/s0140-6736(13)60221-4.
Lisko I, Kulmala J, Annetorp M, Ngandu T, Mangialasche F, Kivipelto M. How can dementia and disability be prevented in older adults: where are we today and where are we going? J Intern Med. 2021;289(6):807–30. https://doi.org/10.1111/joim.13227.
Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–46. https://doi.org/10.1016/S0140-6736(20)30367-6.
Ngandu T, Lehtisalo J, Solomon A, Levälahti E, Ahtiluoto S, Antikainen R, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015;385(9984):2255–63. https://doi.org/10.1016/S0140-6736(15)60461-5.
Lee ATC, Richards M, Chan WC, Chiu HFK, Lee RSY, Lam LCW. Association of Daily Intellectual Activities With Lower Risk of Incident Dementia Among Older Chinese Adults. JAMA Psychiatry. 2018;75(7):697. https://doi.org/10.1001/jamapsychiatry.2018.0657.
Wilson RS, Boyle PA, Yu L, Barnes LL, Schneider JA, Bennett DA. Life-span cognitive activity, neuropathologic burden, and cognitive aging. Neurology. 2013;81(4):314–21. https://doi.org/10.1212/WNL.0b013e31829c5e8a.
Hall K, Gao S, Unverzagt F, Hendrie H. Low education and childhood rural residence: risk for Alzheimer's disease in African Americans. Neurology. 2000;54(1):95–9. https://doi.org/10.1212/wnl.54.1.95.
Valenzuela M, Sachdev P. Brain reserve and cognitive decline: a non-parametric systematic review. Psychol Med. 2006;36(8):1065–73. https://doi.org/10.1017/s0033291706007744.
Chen G, Zhao M, Yang K, Lin H, Han C, Wang X, et al. Education Exerts Different Effects on Cognition in Individuals with Subjective Cognitive Decline and Cognitive Impairment: A Population-Based Study. J Alzheimers Dis. 2021;79(2):653–61. https://doi.org/10.3233/JAD-201170.
Bento-Torres NV, Bento-Torres J, Tomas AM, Costa VO, Correa PG, Costa CN, et al. Influence of schooling and age on cognitive performance in healthy older adults. Braz J Med Biol Res. 2017;50(4):e5892. https://doi.org/10.1590/1414-431X20165892.
Schneider AL, Sharrett AR, Patel MD, Alonso A, Coresh J, Mosley T, et al. Education and cognitive change over 15 years: the atherosclerosis risk in communities study. J Am Geriatr Soc. 2012;60(10):1847–53. https://doi.org/10.1111/j.1532-5415.2012.04164.x.
Wilson RS, Yu L, Lamar M, Schneider JA, Boyle PA, Bennett DA. Education and cognitive reserve in old age. Neurology. 2019;92(10):e1041–e50. https://doi.org/10.1212/WNL.0000000000007036.
Johnson AS, Flicker LJ, Lichtenberg PA. Reading ability mediates the relationship between education and executive function tasks. J Int Neuropsychol Soc. 2006;12(1):64–71.
O'Carroll R, Ebmeier K. Education and prevalence of Alzheimer's disease and vascular dementia. Premorbid ability influences measures used to identify dementia. BMJ. 1995;311(6997):125–6. https://doi.org/10.1136/bmj.311.6997.125b.
Mougias A, Christidi F, Kaldi M, Kerossi MI, Athanasouli P, Politis A. Mini-Mental State Examination: Greek Normative Data Stratified by Age and Education in a Large Sample of 925 Community-Dwelling Healthy Participants. Adv Exp Med Biol. 2020;1196:93–102. https://doi.org/10.1007/978-3-030-32637-1_9.
Lezak MD. Neuropsychological Assessment, (2nd ed). New York: Oxford University Press; 1983.
Zhang X, Lv L, Min G, Wang Q, Zhao Y, Li Y. Overview of the Complex Figure Test and Its Clinical Application in Neuropsychiatric Disorders, Including Copying and Recall. Front Neurol. 2021;12:680474. https://doi.org/10.3389/fneur.2021.680474.
Spreen O, Strauss E. A compendium of neuropsychological tests: administration, norms, and commentary. 2nd ed. New York: Oxford University Press; 1998
Lezak MDHD, Loring DW, Hannay HJ, Fischer JS. Neuropsychological Assessment. 4th ed. New York: Oxford University Press; 2004.
Verghese J, Lipton RB, Katz MJ, Hall CB, Derby CA, Kuslansky G, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med. 2003;348(25):2508–16.
Stephen R, Liu Y, Ngandu T, Antikainen R, Hulkkonen J, Koikkalainen J, et al. Brain volumes and cortical thickness on MRI in the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER). Alzheimers Res Ther. 2019;11(1):53. https://doi.org/10.1186/s13195-019-0506-z.
Kristanto D, Liu M, Liu X, Sommer W, Zhou C. Predicting reading ability from brain anatomy and function: From areas to connections. Neuroimage. 2020;218:116966. https://doi.org/10.1016/j.neuroimage.2020.116966.
Fotuhi M, Do D, Jack C. Modifiable factors that alter the size of the hippocampus with ageing. Nat Rev Neurol. 2012;8(4):189–202. https://doi.org/10.1038/nrneurol.2012.27.
Bruandet A, Richard F, Bombois S, Maurage CA, Masse I, Amouyel P, et al. Cognitive decline and survival in Alzheimer's disease according to education level. Dement Geriatr Cogn Disord. 2008;25(1):74–80. https://doi.org/10.1159/000111693.
Cabeza R, Albert M, Belleville S, Craik F, Duarte A, Grady C, et al. Maintenance, reserve and compensation: the cognitive neuroscience of healthy ageing. Nat Rev Neurosci. 2018;19(11):701–10. https://doi.org/10.1038/s41583-018-0068-2.
Stern Y, Arenaza-Urquijo E, Bartrés-Faz D, Belleville S, Cantilon M, Chetelat G, et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dementia. 2020;16(9):1305–11. https://doi.org/10.1016/j.jalz.2018.07.219.
Richards M, Deary IJ. A life course approach to cognitive reserve: a model for cognitive aging and development? Ann Neurol. 2005;58(4):617–22. https://doi.org/10.1002/ana.20637.
O'Toole KJ, Kannass KN. Emergent literacy in print and electronic contexts: The influence of book type, narration source, and attention. J Exp Child Psychol. 2018;173:100–15. https://doi.org/10.1016/j.jecp.2018.03.013.
Acknowledgements
We would like to thank the participants and their caregivers who participated in the study.
Funding
This study is supported by the Bei**g Municipal Science & Technology Commission (Grant No. Z181100001518005) and the Strategic Priority Research Program of the Chinese Academy of Sciences (XDB39000000).
Author information
Authors and Affiliations
Contributions
SL and JS designed the study. YW, SL, and JS did the scientific literature search. YW, SW, SL, NL, CZ, YP, and QW collected data. YW, WZ, SL, and JS analyzed data. YW and SL created the tables. YW, SL, and JS wrote and all authors edited the report. All authors read and approve the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This protocol was approved by the Institutional Review Board of Bei**g Tiantan Hospital (approval number: KY 2019-004-007) and was in accordance with relevant guidelines and regulations. Written informed consent was obtained from each participant.
Consent for publication
Not involving any person’s data in any form.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental Table 1.
Cognitive performance of participants having different reading years.
Additional file 2: Supplemental Table 2.
Cognitive performance of participants reading different content.
Additional file 3: Supplemental Table 3.
Cognitive performance of participants using different reading materials.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, Y., Wang, S., Zhu, W. et al. Reading activities compensate for low education-related cognitive deficits. Alz Res Therapy 14, 156 (2022). https://doi.org/10.1186/s13195-022-01098-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13195-022-01098-1