
Abstract
We have used second differential near infrared spectroscopy of water to determine the mean optical path length of the neonatal brain. By obtaining the ratio of the second differential features of deoxyhemoglobin to those of water, the absolute cerebral concentration of deoxyhemoglobin can be monitored continuously and noninvasively. Nineteen neonates were studied; the gestational age at birth varied from 23 to 38 wk, and the postconceptual age, when the spectra were recorded, ranged from 35 to 48 wk. The calculated mean deoxyhemoglobin concentration was 14.6 ± 4.0 μM; the differential path length factor (mean optical path length/optode separation) calculated from the water peak at 730 nm was 4.66 ± 1.01, and that calculated at the 830-nm peak was 3.91 ± 0.75. These values are consistent with path length measurements using laser time-of-flight spectroscopy on postmorten neonates and phase-resolved spectroscopy on live neonates. Induced arterial oxygen saturation decreases from 98 to 93% showed no significant change in the mean optical path length, despite significant cerebral desaturation. Changes in the deoxyhemoglobin concentration after this procedure were identical, whether measured by second differential analysis at 760 nm or by multilinear regression over the wavelength range 740-900 nm. When combined with existing methods of measuring total cerebral hemoglobin concentration, second differential near infrared spectroscopy can be used to derive the mean cerebral oxygen saturation. A preliminary experiment outlined the feasibility of this approach and yielded a saturation value of 63%, consistent with near infrared sampling of a predominantly venous pool in the brain.
Similar content being viewed by others


Main
NIRS is a noninvasive technique for measuring changes in oxygenation and hemodynamics in the neonatal brain(1, 2). The technique has been used to detect abnormalities in CBV, CBF, and their response to CO2, in the first day after intrapartum perinatal asphyxia(3, 4). The altered hemodynamics, observed by NIRS, precede the decrease in the cerebral concentration of phosphocreatine/inorganic phosphate detected by NMR spectroscopy, and which is predictive of neurodevelopmental outcome(5).
Current commercially available NIR spectrometers can detect onlychanges in cerebral Hbo2 and Hb. Quantification of these changes in chromophore concentrations requires a knowledge of the path length of light through the tissue of interest in the NIR region. Due to scattering of light by tissue this path length is significantly larger than the source:detector distance. Previous measurements(6, 7) show that the average path length of light in the neonatal head is approximately 4 cm per cm of tissue. The DFP (mean optical path length/cm) is therefore 4. These measurements have utilized time-of-flight techniques which, because of the size and complexity of the equipment involved, have been possible only on postmortem neonates (which may not have normal scattering and absorption properties in the NIR). However, it is possible to measure the path length of light in live neonates relatively simply if the NIR spectrum of a chromophore of known concentration can be determined. We have previously shown that the absorbance of water can be used as such a standard(8, 9), as the concentration of water is known to a few percent accuracy in the brain(10, 11). The method utilizes second differential spectroscopy, a technique that largely eliminates the baseline offset and wavelength dependent spectral features due to tissue scattering. By measuring the second differential of the spectral features in tissue at 730 and 830 nm and comparing them to those of pure water, it is possible to calculate the mean optical path length and DPF at these wavelengths, continuously and noninvasively.
However, even with a continuous measure of optical path length, the use of NIRS in the assessment of neonatal cerebral hemodynamics is limited, unless some other manipulation is performed. For example, it is necessary to change the Sao2(12, 13) and/or Paco2(1) to measure CBF, CBV, and the response of CBV to changes in Paco2; CSvo2 can be measured by tilting infants(14). Furthermore, although continuous monitoring of changes in cerebral Hb and Hbo2 concentrations can yield useful information, measuring changes alone can also provide ambiguous results; for example decreases in CBV have been shown in the first 24 h after birth asphyxia in neonates(4); however, it is possible that this is a return to normal perfusion after the initial hyperperfusion detected by absolute measures of CBF and CBV(3).
For these reasons several groups are currently attempting to develop NIR spectrometers that can measure absolute concentrations of Hb and Hbo2. Techniques for absolute quantification utilizing time(15) or frequency domain(16) spectrometers require a detailed knowledge of the theory of light diffusion through the brain and assume that there are no significant absorbers other than hemoglobin and water in the NIR region. Fewer assumptions are required for multiwavelength techniques using first(17) or second differential(9) spectroscopy. We have shown that Hb has a unique feature in its second differential spectrum around 760 nm; by obtaining the ratio of the Hb signal to that of water it is therefore possible to calculate the absolute Hb concentration of the neonatal brain(18). This method is completely noninvasive and requires no experimental manipulation of the subject. Coupling this technique with the manipulation of Sao2 used to obtain absolute CHC, allows an estimate of absolute [Hbo2] to be derived and hence Smco2.
The purpose of this study was twofold: 1) to measure the mean optical path length in live neonates to allow accurate quantitation of CHCchanges with NIRS and 2) to measure noninvasively theabsolute cerebral concentration of Hb in neonates.
METHODS
Subjects. Measurements were performed on a total of 19 babies who were admitted to the Obstetric Hospital, University College, London. The studies were approved by the Local Hospital Committee on the Ethics of Human Research, and informed written consent was obtained from all the parents of the infants studied. The median gestational age of the infants (at birth) was 34 wk (range 23-38), and the babies were studied at a median age of 3 wk(range 0.2-23), equivalent to a median postconceptual age of 37 wk (range 35-48). Seventeen of the babies had normal cranial ultrasound scans at the time of study and in two infants mild ventricular dilatation was detected. Two infants had chronic lung disease.
NIRS. The CCD spectrometer system has been described previously(8). Briefly, the system uses a quartz halogen light source, a commercial grating spectrograph, and a liquid nitrogen-cooled CCD detector to obtain continuous NIR spectra over the wavelength range 650-1000 nm, at 1.1-nm resolution. For all the experiments performed here, the monochromator entrance slit width was set at 110 μm, resulting in an effective bandwidth of 5 nm. Fiber-optic probes (“optodes”) were placed a median distance of 4.9 cm apart on the temporalfrontal aspect of the infant's head. Optical coupling gel was applied, and the optodes were secured in place and covered with an opaque cloth to prevent stray light reaching the detector. Before each study, a spectrum was recorded in the absence of the light source; in all cases this was indistinguishable from the dark count of the CCD. The quartz halogen light source was filtered with a 1 000-nm short pass filter to reduce any risk of tissue heating, and as a further safety precaution, skin temperature beneath the emitting optode was continuously recorded via a thermistor placed over the optode prism. Skin temperature did not exceed 40°C in any study. An iris between the light source and the input fiber was varied so that the peak detected photon flux/s/nm was approximately 8 000. Although information can be obtained at 1-5-s time resolution, the data were integrated until a minimum of 2 million photons were detected at the peak position to improve the signal:noise ratio; in all cases adequate spectra were collected within 10 min. The predicted photon noise for acquisitions of different length was calculated by Monte Carlo simulations as described previously(9). The infants were all asleep throughout the procedure. On each day of the study, a reference spectrum of the light source was taken by placing the source and detector optodes approximately 20 cm apart in the dark, a black cloth being used to shield out external sources of light. A spectrum of a low pressure neon discharge lamp was also taken to confirm the wavelength calibration of the spectrograph.
Determination of CHC. In one infant CHC was determined directly using the technique described previously(13). Fio2 was varied to produce small changes in Sao2, which was measured via a pulse oximeter (Nellcor N200, Hayward, CA) probe on the infant's hand or foot. The program controlling the CCD spectrometer acquisition was modified to record the average Sao2 during the 2-s integration time used in this study; this allowed the direct regression of Sao2 against Δ[Hbo2]. necessary for measuring the CHC.
Reference chromophore spectra used. Due to the temperature dependence of the water spectrum(19) it was measured at different temperatures on a commercial Cary UV/VIS/NIR spectrophotometer with a thermostatically controlled sample compartment; the spectrum was then differentiated twice by standard methods(18). The Hb second differential spectrum used was determined from the attenuation spectrum of Cope(20). A smoothing over 11 nm was applied to both spectra before the differentiation. A digital copy of the second differential spectra used in this study is available from the authors (send either MS-DOS or Macintosh disk). The Hbo2, Hb, and cytochrome oxidase spectra used to fit the changes in OD as Fio2 was varied were those used to generate the algorithm used by the commercial Hamamatsu NIRO500 spectrometer; this uses the optical spectra published previously(21) and applies a spectral correction factor to account for the wavelength dependence of the DPF(22). The use of a multiwavelength spectrometer allowed the attenuation change to be fitted over the wavelength range 740-900 nm (1 point every 1.1 nm), rather than just the 4 wavelengths used in the commercial spectrometer. Rather than applying a fixed DPF, each time point was individually corrected for DPF by the use of the water peak second differential (fit from 710-840 nm).
Data analysis. Absolute Hb(18) and mean optical path length(9) were calculated from the in vivo spectra as shown in Figure 1. Each spectrum of detected broadband light was averaged over the period of interest(a) and then converted into a tissue attenuation spectrum, utilizing the lamp reference spectrum (b). The spectral intensity values recorded at the CCD detector were divided at each wavelength and the logarithm of the ratio taken thus: Equation

NIR attenuation spectrum of neonatal brain. Shape of NIR spectrum calculated as described in “Methods”: (a) detected light, (b) lamp reference spectrum, (c) attenuation spectrum, and (d) smoothed attenuation spectrum. Spectra(a) and (b) have units of flux, and spectra (c) and (d) have units of OD. No attempt is made to determine the absolute OD. The baseline in spectra (c) and (d) is therefore arbitrary; however, the shape of the spectrum with respect to wavelength will determine the relative size of the hemoglobin and water second differential features (shown in Fig. 2). The infant studied was no. 9 (Table 1).
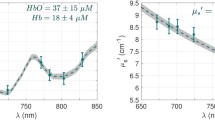
This attenuation spectrum (c), whose absolute values are arbitrary, was then smoothed (d) over 11 nm (10 points); the same smoothing was applied to the chromophore reference spectra.Figure 2 illustrates how the mean optical path length and absolute [Hb] were calculated from the tissue attenuation spectrum. First the second differential was calculated (Fig. 2a)-note the clear features at 730 and 830 nm (water) and 760 nm (Hb). Then the water(Fig. 2b) and Hb (Fig. 2c) second differential reference spectra were fitted to the tissue second differential spectra via a multilinear least squares regression. As described previously(18) the optimum method for calculating the absolute [Hb] is to fit over the wavelength range 710-840 nm. Figure 2d shows the residuals for a fit over the complete wavelength range 710-840 nm(smaller residuals were observed when the water peaks at 730 and 830 nm were fit separately). If the reference Hb spectrum is in units of OD mM -1 cm-1 nm-2 and that of pure water is in units of OD cm-1 nm-2, then, assuming a neonatal cerebral water content of 85%(10), the absolute [Hb] is calculated as:Equation where “H2O signal” and“Hb signal” represent the amount of the pure second differential chromophore spectrum required to fit the second differential tissue spectrumi.e. spectra b and c in Figure 2.

Second differential spectrum of neonatal brain.(a) Second differential spectrum calculated from the smoothed attenuation spectrum of Figure 1. The dotted line is the multilinear regression fit of standard water and Hb spectra to(a); offset are the fitted second differential spectra of water(b) and Hb (c) and the residuals for the fit(d).
The mean optical path length was calculated for the region of each water peak separately. The 730-nm differential path length factor (DPF) was calculated by fitting both Hb and water spectra over the wavelength region 710-780 nm; the 830-nm DPF was calculated by fitting the in vivo data with only the water spectrum over the wavelength region 815-840 nm, using the fixed contribution from Hb as previously calculated at 710-780 nm (there is only a very small contribution from Hb at 815-840 nm, so fitting to Hb here is impractical, but assuming a fixed contribution is likely to marginally improve the accuracy of the calculation). The differential path length factor(DPF) is then calculated as follows: Equation
The relationships between age and measured parameters were tested by linear least squares regression; the significance of a nonzero slope was measured with a t test (p values for these tests are quoted in the text).
RESULTS
Temperature-dependent studies showed that the absorbance of the water NIR peak at 970 nm increased by 0.5%/°C; the observed temperature effect varied with wavelength, and some-what larger dependent changes were seen in the water second differential spectrum at 730 and 830 nm used in this study. Therefore a spectrum recorded at 37°C was used to generate a second differential reference spectrum for water.
Table 1 shows the absolute Hb concentrations [Hb] and mean optical path lengths for the 19 neonates studied. As might be expected,[Hb] has a larger variation (SD 28% of mean) than the differential path length factor (SD 20% of mean). Regression analysis (Fig. 3) showed that there was a positive correlation between gestational age at birth and DPF at 730 nm (p = 0.02) and a slight positive correlation between gestational age and DPF at 830 nm (p = 0.07). Surprisingly there was no significant correlation between postconceptual age and DPF (at either wavelength). This appeared to be due to the fact that for technical reasons the very low gestational age babies (with low DPF values) were studied at high postconceptual age. This suggests that there is an abnormally low DPF in very preterm babies (>30 wk) that is not rectified by 50 wk postconception.

Variation of the differential path length factor with gestational age at birth. DPF was measured at 730 (•) or 830 nm (□). Linear least squares regressions for 730 (solid line) and 830 nm(dotted line) were as follows: 730 nm: y = 0.12x+ 0.73; r = 0.52 (p = 0.02); 830 nm: y = 0.07x + 1.64; r = 0.42 (p = 0.07).
There is a significant increase (p < 0.02) in the DPF measured at 730 nm, when compared with that at 830 nm. In agreement with our previous study on a single infant(9) the DPF at the 970-nm region(using second differential spectroscopy of the large water peak feature there) is lower than the DPF at 830 nm. However, due to the large absorbance of light at the optode spacing used in this study, and the low input light levels, it was not possible to obtain usable data in the 930-970-nm region for over half of the neonates studied. If the optical path length in this region was required, the inter optode spacing would need to be reduced, or the data collection time significantly increased, to get consistent results.
No correlations were observed between Hb concentration and the DPF at 730 or 830 nm, showing that small changes in chromophore concentrations are insignificant in determining the mean DPF. There was, however, a significant increase in [Hb] with postconceptual (p = 0.0005), but not gestational (p = 0.58), age. This correlation must be viewed with caution, however, as any decrease in the water content with postconceptual age will be observed as an artifactual apparent increase in [Hb]. An average water content of 85% was assumed for all the babies studied-the maximum variation for this value(10) is from 90% (preterm neonate) to 80%(adult).
To calculate Smco2 it is necessary to measure the total hemoglobin concentration and Hb concentration in the same infant.Figure 4 shows the variation in [Hbo2] with arterial saturation after changes in Fio2. CHC remained essentially constant throughout the changes in Sao2, as judged by (Δ[Hb] +Δ[Hbo2]). The differential path length also remained constant despite the changes in hemoglobin oxygenation, again showing that small variations in chromophore concentration do not have a large effect on the mean optical path length. This is consistent with simulations using the diffusion equation for light transport through tissue(18); the predicted increase in the DPF at 830 nm for the observed saturation change seen in Figure 4 is only 1%, undetectable at the level of noise shown.

Variation of DPF, [Hbo2] and Sao2 with changes in Fio2. Fio2 was varied and the parameters calculated as described in the methods section. DPF was monitored at 830 nm. The infant studied was no. 13 (Table 1). The variations in the DPF seen with time are within the 12% error predicted from simulations of the noise at this sampling rate (see “Methods”).
From the relationship between Δ[Hbo2] and Sao2(13) it is possible to calculate a value for the absolute CHC, [Hb] + [Hbo2], of 33.5 μM. Before the swings (Sao2 = 99%) the absolute Hb in this neonate was 12.6 μM; therefore Smco2, in this neonate started at 63% and dropped to a minimum of 56% as Sao2 dropped to 93%. Studies to determine this value in a larger group of infants are currently in progress.
DISCUSSION
Validity of the method. The distinct Hb and water features in the second differential spectra allow good fits to be calculated relatively easily. The main pitfall in interpreting these data lies in the temperature dependence of the reference spectra. Although, not surprisingly, there are many publications reporting the NIR spectrum of water(19, 23), none of them have been obtained at 37°C. A new reference water spectrum was therefore recorded at 37°C. The OD we found at 970 nm (0.22 cm-1) agreed with that in recent publications(19), once the temperature effect was accounted for. A failure to correct adequately for these temperature effects may be responsible for some of the discrepancy previously seen between water peak differential path lengths and those measured by time-of-flight systems(9). There is a much smaller, but still significant, temperature effect on the Hb spectrum(24, 25); the maximum change at 760 nm is + 0.1%/°C increase(25). The systematic errors that occur due to our incomplete knowledge of the scattering properties of the neonatal brain(18) are of a similar order of magnitude to this; the small differences between neonatal and adult hemoglobin NIR spectra(26) may also have a similar small effect on their second differential spectra. Therefore we have chosen to ignore the hemogolbin temperature effect for the purposes of this study.
One of the problems with develo** novel NIRS methodology is the difficulty in comparing data with a “gold standard.” This is impossible in this case as there are no other noninvasive measurements of absolute Hb concentration. However, it is possible to compare changes in the absolute [Hb] obtained by second differential spectroscopy with those measured by conventional NIRS techniques(18).Figure 5 shows this comparison when Fio2 is varied(for the same infant studied in Figure 4). Linear regression shows a strong correlation between the two methods (r = 0.94), with a slope that is not significantly different from 1. Thus measuring a narrow feature of the Hb spectrum gives results identical with those obtained by measuring it over a wider spectral range. This demonstrates that there are no other significant chromophores contributing to the 760-nm second differential Hb feature and improves our confidence in the reliability of both methods for measuring quantified changes in [Hb]. Furthermore, the few assumptions utilized in the calculation of absolute [Hb] by this method makes it of value as a standard to compare with other, possibly less robust, methodologies for determining absolute chromophore concentrations.

Comparison of absolute and relative Hb changes. Comparison of Hb concentration changes derived from the second differential(absolute, -) and conventional (relative, •) algorithm as Fio2 is varied. The relative [Hb] was calculated using a current commercial algorithm (as described in “Methods”). This was offset by a fixed concentration of Hb to facilitate the comparison with the absolute [Hb] method (the value of the offset was calculated by linear least squares regression, minimizing the difference between the relative and absolute traces).
Mean optical path length. The variation in DPF between subjects in this study is larger than can be accounted for by known uncertainties,e.g. the interoptode spacing is known to ±1 mm, a 2% error, and the predicted photon noise for a 10-min acquisition is 0.7%. The variation is similar to that measured by direct time-of-flight spectroscopy on postmortem neonates(7). There is apparently a significant intrinsic (physiologic/anatomical) variation in DPF in neonates that is not a measurement artifact. Measurements of DPF using phase resolved spectroscopy in 35 neonates(27) also show a SD/mean of 10-15%. Some, but not all, of the variation in these studies can be ascribed to the differences in gestational age of the neonates.
There have been two previous studies of the neonatal head DPF, calculated in postmortem neonates by direct time-of-flight spectroscopy at 783 nm, one(6) yielding a DPF of 4.39 ± 0.28 (n = 6) and the other(15) of 3.85 ± 0.57 (n = 10). The mean gestational age in the larger study was 31 wk, very similar to the group in this study (32 wk). t tests, assuming unequal variances(28), show no significant differences between the means of either of the postmortem DPF values (measured at 783 nm) and that from live babies in this study, calculated by fitting the water peak between 710 and 840 nm.
Measurements of DPF on a group of 35 infants using phase resolved spectroscopy(27) have yielded a DPF of 4.67 ± 0.65 at 832 nm and 5.11 ± 0.48 at 744 nm. These are significantly higher than those measured by the water peak method at 830 and 730 nm, respectively. However, the mean gestational age in the phase study was higher than those studied in this report (mean of 40 wk as compared with 32 wk). Using the regression curve in Figure 3 to modify the water peak DPF values, to correct for this, resulted in there being no significant difference between the values for the DPF obtained at either 830 nm or 730/740 nm as measured by the two methods.
In both the current study and the phase-resolved data discussed above, the DPF is seen to increase as the wavelength is decreased from 830 to 730 nm. This is due to a combination of an increase in scattering and a decrease in absorbance at the shorter wavelength(22). This relationship is in agreement with time-of-flight measurements on normally oxygenated adult brain, but in disagreement with that on postmortem neonatal brain. In the latter case the wavelength dependence of the optical path length is distorted by the presence of a large concentration of Hb, which increases the path length at 830 nm, relative to that at 730 nm(22).
The DPF is necessary to convert NIR chromophore (water, hemoglobin, cytochrome oxidase) changes from OD changes to μM. The fact that three separate methods (phase resolved spectroscopy, time-of-flight spectroscopy, and second derivative spectroscopy) all yield very similar values for the mean optical path length in the neonate, increases our confidence in the use of this number to quantify NIR spectra. However, the significant variation of DPF within subjects and its correlation with gestational age suggest that the simultaneous measurement of DPF is essential for further improving the accuracy of quantitative NIR techniques.
The DPF may be of biologic interest in its own right. The results suggest that very preterm infants have a lower DPF than term infants, and that this does not rapidly return to normal after birth. Although the cerebral water content changes (decreases) during brain development, this cannot account for the observed difference as a decreased water content of the brain would lead to an increased apparent DPF using the second differential method described here (see “Methods”). As no significant changes in DPF were observed with changes in chromophore concentrations, it seems most likely that it is the lack of scattering material in the brain that is causing this low DPF. One possible explanation is that DPF rises as myelination increases; thus abnormalities in DPFmay be an indicator of abnormalities in cerebral maturation in the neonate. However, it is important to note that the changes in DPF observed in this study are relatively small compared with the individual variation in DPF; they require further characterization by a longitudinal study, monitoring changes in DPF with age in individual infants.
Absolute Hb measurements. Although DPF measurements are important in improving the quantification of NIR data, the real advantage of second differential spectroscopy is in the measurement of absolute Hb concentrations. When coupled to a measurement of CBV, this allows a noninvasive determination of mean cerebral oxygen saturation(Smco2). The mean CHC in the neonate can be calculated using NIRS(13) or positron emission tomography(29). For 12 neonates of a mean gestational age of 29 wk(range 25-40 wk), the NIRS-calculated CHC was in the range of 11.4-50.1 μM(13). The range of Hb concentrations (6.8-27 μM) in this study is significantly lower than CHC, consistent with values of Smco2 in the likely physiologic range (50-70%). The value for mean cerebral saturation determined for the single neonate in this study (63%) is closer to that previously reported(14) for venous saturation (53%) than the arterial saturation of 98%. This is consistent with the larger cerebral venous blood volume in the brain. Independent measurements of cerebral venous saturation(14), Sao2 and Smco2 (this study) on the same infant would enable the venous/arterial ratio in the volume of the brain probed by NIRS to be determined.
Clinical utility. The use of multiwavelength spectrometers takes advantage of the unique shape of chromophore spectra in the NIR to reduce the problems associated with the effects of light scattering. This opens new possibilities in the measurement of cerebral hemodynamics in children. A system with a broad band light source and a sensitive CCD detector can be constructed at a similar size and portability compared with current commercial NIR spectrometers. Alternatively expanding the number of laser diodes on a “conventional” NIR spectrometer (e.g. from 4 to 16) would also allow a multiwave-length second differential analysis of the type described here.
We have shown that second differential spectroscopy is a reliable method of measuring absolute Hb concentration and mean optical path length in the neonatal brain. From these parameters it is possible to derive mean cerebral oxygen saturation if CHC is known. Given that NIRS can also measure CBF, it is possible to distinguish whether altered cerebral Hb concentrations are due to variations in CBF or in oxygen consumption. However, even in the absence of other information, the absolute cerebral Hb concentration is likely to be a useful clinical parameter. It is currently impractical to monitor every neonate with a NIR spectrometer, but because the technique described here does not require any experimental manipulations, it could be used as an initial screening technique to detect altered cerebral hemodynamics. It is more straightforward than obtaining the response to an induced change in Paco2 and may be less variable than absolute CHC measurements. An abnormally high Hb concentration may be the result of either an abnormally low Sao2, a high CHC or a high rate of cerebral oxygen consumption; an abnormally low Hb concentration may be the result of either a low CHC or a decrease in oxygen consumption. Direct CHC and Sao2 measurements will then reveal which of these possibilities is more likely. It should be noted that methods that measure Smco2 alone will not necessarily detect abnormalities due to decreased CBF if they are accompanied by decreases in the oxygen consumption rate.



Abbreviations
- NIRS:
-
near infrared spectroscopy
- NIR:
-
near infrared
- CBF:
-
cerebral blood flow
- CBV:
-
cerebral blood volume
- CHC:
-
cerebral hemoglobin concentration (μmol/L of brain tissue)
- Hb:
-
deoxyhemoglobin
- Hbo2:
-
oxyhemoglobin
- Δ[Hbo2]:
-
change in [oxyhemoglobin]
- Sao2:
-
arterial oxygen saturation
- Paco2:
-
arterial carbon dioxide tension
- Fio2:
-
inspired oxygen fraction
- CSvo2:
-
cerebral mixed venous oxygen saturation
- Smco2:
-
mean cerebral oxygen saturation
- CCD:
-
charge-coupled device
- DPF:
-
differential path length factor
References
Wyatt JS 1992 Near infrared spectroscopy. Biol Neonate 62: 290–294
von Siebenthal K, Bernert G, Casaer P 1992 Near-infrared spectroscopy in newborn infants. Brain Dev 14: 135–143
Wyatt JS 1993 Near-infrared spectroscopy in asphyxial brain injury. Clin Perinatol 20: 369–378
van Bel F, Dorrepaal CA, Benders MJ, Zeeuwe PE, van de Bor M, Berger HM 1993 Changes in cerebral hemodynamics and oxygenation in the first 24 hours after birth asphyxia. Pediatrics 92: 365–372
Wyatt JS, Edwards AD, Azzopardi D, Reynolds EOR 1989 Magnetic resonance and near infrared spectroscopy for investigation of perinatal hypoxic-ischaemic brain injury. Arch Dis Child 64: 953–963
Wyatt JS, Cope M, Delpy DT, van der Zee P, Arridge SR, Edwards AD, Reynolds EOR 1990 Measurement of optical pathlength for cerebral near infrared spectroscopy in newborn infants. Dev Neurosci 12: 140–144
van der Zee P, Cope M, Arridge SR, Essenpreis M, Potter LA, Edwards AD, Wyatt JS, McCormick DC, Roth SC, Reynolds EOR, Delpy DT 1992 Experimentally measured optical pathlengths for the adult head, calf and forearm and the head of the newborn infant as a function of inter optode spacing. Adv Exp Med Biol 316: 143–155
Cope M, Delpy DT, Wyatt JS, Wray SC, Reynolds EOR 1989 A CCD spectrometer to quantitate the concentration of chromophores in living tissue utilising the water absorption peak of water at 975 nm. Adv Exp Med Biol 247: 33–41
Matcher SJ, Cope M, Delpy DT 1994 Use of the water absorption spectrum to quantify tissue chromophore concentration changes in near-infrared spectroscopy. Phys Med Biol 39: 177–196
Holland BA, Haas DK, Norman D, Brant-Zawadzki M, Hans-Newton T 1986 MRI of normal brain maturation. AJNR 7: 201–208
Woodward HQ, White DR 1986 The composition of body fluids. Br J Radiol 59: 1209–1219
Edwards AD, Wyatt JS, Richardson C, Delpy DT, Cope M, Reynolds EOR 1988 Cotside measurements of cerebral blood flow in ill preterm infants by near infrared. Lancet 2: 770–771
Wyatt JS, Cope M, Delpy DT, Richardson CE, Edwards AD, Wray S, Reynolds EOR 1990 Quantitation of cerebral blood volume in newborn human infants by near infrared spectroscopy. J Appl Physiol 68: 1086–1091
Skov L, Pryds O, Greisen G, Lou H 1993 Estimation of cerebral venous saturation in newborn infants by near infrared spectroscopy. Pediatr Res 33: 52–55
Patterson MS, Chance B, Wilson B 1989 Time Resolved Reflectance and Transmittance for the Non-Invasive Measurement of Optical Properties. Appl Optics 289: 2331–2336
Gratton E, Fantini S, Franceschini M, Fishkin JB 1994 Near infrared optical spectroscopy of tissues using an LED frequency domain spectrometer. In: Advances in Optical Imaging and Photon Migration, Technical Digest. Optical Society of America, Washington, DC, pp 212–215
Ferrari M, Wilson DA, Hanley DF, Hartman JF, Traystman RJ, Rogers MC 1989 Non invasive determination of haemoglobin saturation in dogs by derivative near-infrared spectroscopy. Am J Physiol 256:H1493–H1499
Matcher SJ, Cooper CE 1994 Absolute quantification of deoxyhaemoglobin concentration in tissue near infrared spectroscopy. Phys Med Biol 39: 1295–1312
Kou L, Labrie D, Chylek P 1993 Refractive indices of water and ice in the 0.65 to 2.5 μM spectral range. Appl Optics 32: 3531–3540
Cope M 1991 The application of near infrared spectroscopy to non-invasive monitoring of cerebral oxygenation in the newborn infant. PhD thesis, University of London
Wray S, Cope M, Delpy DT, Wyatt JS, Reynolds EOR 1988 Characterisation of the near infrared absorption spectra of cytochromeaa 3 and haemoglobin for the non-invasive monitoring of cerebral oxygenation. Biochim Biophys Acta 933: 184–192
Essenpreis M, Elwell CE, van der Zee P, Arridge SR, Delpy DT 1993 Spectral dependance of temporal point spread functions in human tissues. Appl Optics 32: 418–425
Hale GM, Querry MR 1973 Optical Constants of Water in the 200-nm to 200-μM wavelength region. Appl Optics 12: 555–563
Cordone L, Cupane A, Leone M, Vitrano E 1986 Optical absorption spectra of deoxy-and oxyhaemoglobin in the temperature range 300-20K. Biophys Chem 24: 259–275
Biagio PLS, Vitrano E, Cupane A, Madonia F, Palma MU 1977 Temperature induced difference spectra of oxy and deoxy hemoglobin in the near IR, visible and Soret regions. Biochem Biophys Res Commun 77: 1158–1165
Zijlstra WG, Buursma A, Meeuwsen-van der Roest WP 1991 Absorption spectra of human fetal and adult oxyhaemoglobin, de-oxyhaemoglobin, carboxyhaemoglobin, and methaemoglobin. Clin Chem 37: 1633–1638
Duncan A, Meek JH, Clemence M, Elwell CE, Tyszczuk L, Cope M, Delpy DT 1995 Optical pathlength measurements on adult head, calf and forearm and the head of the newborn infant using phase resolved spectroscopy. Phys Med Biol 40: 295–304
Parker RE. 1991 Introductory Statistics for Biology. Cambridge University Press, Cambridge, p 21
Altman DI, Perlman JM, Volpe JJ, Powers WJ 1993 Cerebral oxygen metabolism in newborns. Pediatrics 92: 99–104
Acknowledgements
The authors thank Dr. Kaveh Nahid (University College, London) for technical assistance and Prof. Mike Wilson (University of Essex) for the use of the Cary NIR spectrophotometer.
Author information
Authors and Affiliations
Additional information
Supported by the Medical Research Council (UK), the Wellcome Trust, and Hamamatsu Photonics KK.
Rights and permissions
About this article
Cite this article
Cooper, C., Elwell, C., Meek, J. et al. The Noninvasive Measurement of Absolute Cerebral Deoxyhemoglobin Concentration and Mean Optical Path Length in the Neonatal Brain by Second Derivative Near Infrared Spectroscopy. Pediatr Res 39, 32–38 (1996). https://doi.org/10.1203/00006450-199601000-00005
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199601000-00005
- Springer Nature America, Inc.
This article is cited by
-
Noninvasive monitoring of cerebral oxygenation in traumatic brain injury: a mix of doubts and hope
Intensive Care Medicine (2010)
-
Tissue hemoglobin index: a non-invasive optical measure of total tissue hemoglobin
Critical Care (2009)
-
Schwellungsänderungen in der Nase
HNO (2007)
-
Measurement of Cerebral Oxidative Metabolism with Near-Infrared Spectroscopy: A Validation Study
Journal of Cerebral Blood Flow & Metabolism (2006)
-
Measurement of Cerebral Optical Pathlength as a Function of Oxygenation Using Near-infrared Time-resolved Spectroscopy in a Piglet Model of Hypoxia
Optical Review (2003)