
Abstract
Background
Lipomas are ubiquitous tumors. They are mostly present in the trunk as well as the proximal portion of the limbs. However, 15–20% are located in the head and neck regions, and only 4.4% are found in the oral cavity. They normally present as a bulge with signs of compression, without signs of infiltration.
Case presentation
This is the rare case of a 36-year-old man, who was admitted to ENT consultation for a bulge in the left inferior vestibule of the oral cavity. The bulging was not painful, with no inflammatory signs, no dental mobility, or abnormalities in the vestibular mucosa. No other masses were found in the general clinical exam. The patient underwent a dental panoramic X-ray, which showed a low opacity lesion next to the left inferior vestibular space, without signs of bone invasion. There was no hypoesthesia in the territory of the alveolar nerve was found. The patient underwent a craniofacial MRI which showed a mass which was hypointense on T1 and hyperintense on T2. Fine needle aspiration was not performed. The patient’s pre-operative blood work showed no abnormalities. He underwent surgical excision under general anesthesia. The incision was carried out in the left inferior vestibular space, 1 cm away from the alveolar gingiva; careful dissection of the mucosa allowed the discovery of a large fatty mass, encapsulated, with a nourishing pedicle, without signs of invasion or ulceration in the adjacent structures. Careful dissection and hemostasis were performed, followed with the closure of the mucosa with Vicryl 4.0. The histopathological exam showed mature adipose tissue. The fat contains few small capillaries within thin fibrous strands. A thin fibrous capsule was seen. Clinical follow-up of 2 months showed no complications. The surgical incision healed perfectly, and no bulging was noticed upon palpation.
Conclusions
This is the rare case of a vestibular lipoma of the oral cavity; the clinical and radiological aspect allowed consideration of several differential diagnoses. The most important take away lesson is related to the very rich variety of differential diagnosis in oral cavity masses. Clinical and radiological aspects allow the clinician to have diagnostic theories. Only histological results allow to establish a definitive diagnosis.
Similar content being viewed by others


Background
Lipomas are ubiquitous benign mesenchymal tumors composed of mature adipocytes [1,2,3,4,5,6,7,8]. They are mostly present in the trunk as well as the proximal portion of the limbs [3]. However, only 15–20% are located in the head and neck regions [4, 5], and only 4.4% are found in the oral cavity [2,3,4,5, 8]. It appears as a bulge covered by normal oral mucosa [5, 8]. They are generally presented as a bulge without signs of extension to adjacent structures; in the oral cavity, they can be responsible for problems in swallowing and speech [2,3,4,5].
Case presentation
This is a rare case of a vestibular lipoma in the oral cavity, in a 36-year-old man, who was admitted in ENT consultation for a bulge in the left inferior vestibule of the oral cavity. The bulge was not painful, no inflammatory signs, no dental mobility, or abnormalities in the vestibular mucosa. No hypoesthesia in the territory of the alveolar nerve was found. No other masses were found in the general clinical exam. The patient underwent a dental panoramic X-ray, which showed a low opacity lesion next to the left inferior vestibular space.
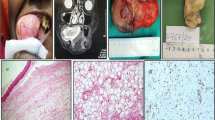
The patient underwent a craniofacial MRI which showed a mass which was hyperintense on T2 and hypointense on T1. Fine needle aspiration was not performed.
The patient’s pre-operative blood work showed no abnormalities (Figs. 1, 2, and 3). He underwent surgical excision under general anesthesia.

MRI sections showing T2 hyper-intense lesions, in the left vestibular region

Per-operative image showing the extirpation of a lipoma of the inferior oral vestibule

Post-operative specimen
The incision was carried out in the left inferior vestibular space, 1 cm away from the alveolar gingiva; careful dissection of the mucosa allowed the discovery of a large fatty mass, encapsulated, with a nourishing pedicle, without signs of invasion or ulceration in the adjacent structures. Careful dissection and hemostasis were performed, followed by closure of the mucosa with Vicryl 4.0.
The histopathological exam showed mature adipose tissue. The fat contains few small capillaries within thin fibrous strands. A thin fibrous capsule was seen.
A clinical follow-up of 2 months showed no complications. The surgical incision healed perfectly, and no bulging was noticed upon palpation.
Discussion
The first case of lipoma was described in 1848 by Roux [2, 8]; the age of onset is between 40 and 60 years old [1,2,3, 5, 7, 8]. They are very rare in children [4, 7]
Studies have suggested that there is no gender predilection. However, some series suggested that lipomas are generally predominant in males [1, 5, 7, 8]. Oral localizations are favorably found in female patients [4, 7].
The most frequent mode of presentation is a slow-growing mass, covered by healthy mucosa, without any signs of invasion [1, 3, 5].
Lipomas of the oral cavity are most frequently localized in the buccal mucosa, especially in the cheek (50%) [1, 4] (Table 2). followed by other localizations such as the tongue, lip, floor of the mouth, buccal vestibule, palate, and retro-molar area [1, 2, 4, 5, 7].
The size usually fluctuates between 0.8 and 2.6 cm [3, 5, 7, 8]. Lipomas are rarely superior to 25 mm [1, 7]. Superficial presentations are generally yellowish well circumscribed, with a smooth nodular surface, that could be either peduncular or sessile. While profound forms are infiltrating, rarely typically yellowish and could present diagnostic challenge [4, 5].
Lipomas are generally clinically asymptomatic and slowly grows, until it manifests with signs of compression [1, 8]. Could present as solitary or multiple lesions [1, 8]. Multiple lesions could be associated with syndromes like Gardner’s syndrome, Decrum’s disease, multiple familial lipomatosis, encephalo-cranio-cutaneous lipomatosis, Pai syndrome, and neurofibromatosis [5].
Etiopathogenesis
While a definitive etiology of lipoma formation remains unclear [2, 5, 6, 8], two theories have been associated with the formation of lipomas [2, 5, 6, 8].
The hypertrophy theory stipulates that lipomas are advertent growths of adipose tissue; it explains the formation of lipomas by the onset of obesity and the adipose tissue associated with it [2, 5, 6, 8].
The metaplasia theory stipulates that lipomas are due to aberrant differentiation of mesenchymal cells into lipoblasts [2, 5, 6, 8].
Besides, a congenital origin has been suspected where embryogenic cells differentiate into lipomas under hormonal influence [6].
Several factors have been associated with the onset of oral cavity lipomas: obesity, hereditary, injuries, infection, muscle cell metaplasia, residual embryonic fat cells, chronic irritation, fatty degeneration, and hormonal abnormalities [2,3,4, 6, 8].
Several differentials could be lymphoepithelial cysts, epidermoid cysts, dermoid cysts, and granular cell tumors, neurofibroma, traumatic fibroma, and salivary gland lesions such as mucocele and mixed tumors [1,2,3,4,5, 8].
Clinical aspect of lipomas generally allows diagnosis. However, association with X-ray and sonography is necessary for unusual localizations, sometimes even CT scan and MRI are necessary to rule out more frequent lesions [4]. Histological aspect remains the gold standard to establish a definitive diagnosis [4, 5].
Several histological patterns depend on the histological subtype [1,2,3,4,5] Table 2.
Macroscopically, lipomas are generally made of benign mesenchymal neoplasms composed of fatty cells, generally surrounded by a thin fibrous capsule. The following are the different histological sub-types: simple lipoma, spindle cell lipoma, fibro-lipoma, angiolipoma, polymorphic myxoid lipoma, and atypical lipomas [1, 2, 4, 6, 8]. Sialo-lipoma and chondro-lipomas are very rarely reported in the literature [4,5,6, 8].
Liposarcomas are rare in the oral cavity [1].
Proliferating cell nuclear antigen (PCNA) and ki67 are found in lipomas [5]. PCNA could suggest faster-growing lipomas [5]. Microscopical aspect is a circumscribed but not encapsulated aggregate of mature adipocytes with large and clear cytoplasm, without vascularity [1].
Spindle cell lipomas are related to 13q or 16q chromosome abnormalities [6, 8].
Treatment
Surgical excision is the treatment of choice, as a complete excision allows to bring recurrence rate to very low values. Infiltrating lipomas are very hard to extirpate [1, 8]. Recurrence after complete excision is rare; infiltrative lipomas have more recurrence rates as they are not encapsulated [8].
Secondary atrophy can be spotted and should not be confused with malignant degeneration [5]. No incidence of malignant transformation has been cited [5, 8].
Medical treatment based on steroid injection could be recommended for spindle cell lipomas inferior to 2.5 cm [8].
Conclusions
Differential diagnosis of oral cavity benign masses is diverse; lipomas are very rare in this localization. However, their management is very simple, and the outcome is generally very good.
Availability of data and materials
Not applicable.
References
Hoseini AT, Razavi SM, Khabazian A (2010) Lipoma in oral mucosa: two case reports. Dent Res J (Isfahan). 7(1):41–43
Egido-Moreno S, Lozano-Porras AB, Mishra S, Allegue-Allegue M, Marí-Roig A, López-López J (2016) Intraoral lipomas: review of literature and report of two clinical cases. J Clin Exp Dent 8(5):e597–e603. Published 2016 Dec 1. https://doi.org/10.4317/jced.52926
Naruse T, Yanamoto S, Yamada S et al (2015) Lipomas of the oral cavity: clinicopathological and immunohistochemical study of 24 cases and review of the literature. Indian J Otolaryngol Head Neck Surg. 67(Suppl 1):67–73. https://doi.org/10.1007/s12070-014-0765-8
Kumar LK, Kurien NM, Raghavan VB, Menon PV, Khalam SA (2014) Intraoral lipoma: a case report. Case Rep Med 2014:480130. https://doi.org/10.1155/2014/480130 Epub 2014 Jan 30. PMID: 24592278; PMCID: PMC3926394
Fregnani ER, Pires FR, Falzoni R, Lopes MA, Vargas PA (2003) Lipomas of the oral cavity: clinical findings, histological classification and proliferative activity of 46 cases. Int J Oral Maxillofac Surg 32:49–53. [PubMed] [Google Scholar]. https://doi.org/10.1054/ijom.2002.0317
Mehendirratta M, Jain K, Kumra M, Manjunatha BS (2016) Lipoma of mandibular buccal vestibule: a case with histopathological literature review. BMJ Case Rep 2016:bcr2016215586. Published 2016 Aug 3. https://doi.org/10.1136/bcr-2016-215586
Morais AL, Mendonça EF, de Alencar AH, Estrela C (2011) Intraosseous lipoma in the periapical region of a maxillary third molar. J Endod. 37(4):554–557. https://doi.org/10.1016/j.joen.2010.12.006 Epub 2011 Feb 25. PMID: 21419308
Molano-Valencia PE, Betancourt-Rivera VA, Ruiz-Mazuera LM (2017) Gingival lipoma: a case report. Rev Fac Odontol Univ Antioq. 29(1):211–221. https://doi.org/10.17533/udea.rfo.v29n1a11
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
O.B performed the surgery. K.C contributed to the clinical management and investigation and analyzed and interpreted the patient data. NO contributed to the clinical and surgical management of the patient. SB contributed to the clinical management of the patient. All authors have read and agreed to its content. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics and consent to participate
Not applicable.
Consent for publication
The subject provided written consent for participation and publication of the case report.
Competing interests
All authors have participated in the (a) conception and design or analysis and interpretation of the data, (b) drafting of the article or revising it critically for important intellectual content, and (c) approval of the final version.
This manuscript has not been submitted to, nor is under review at, another journal or other publishing venue.
The authors have no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the manuscript. The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Benhoummad, O., Cherrabi, K., El Orfi, N. et al. A rare case of oral cavity lipoma in the inferior vestibule: a case report and literature review. Egypt J Otolaryngol 38, 87 (2022). https://doi.org/10.1186/s43163-022-00257-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-022-00257-3