
Abstract
Background
In malaria-endemic countries, repeated intake of artemisinin-based combination therapies (ACTs) is rampant and driven by drug resistance, improper usage, and easy accessibility. Stress effects and potential liver toxicity due to the frequent therapeutic use of ACTs have not been extensively studied. Here, we investigated the effects of repeated treatment with standard doses of the commonly used ACTs artemether/lumefantrine (A/L) and artesunate-amodiaquine (A/A) on oxidative stress and liver function markers in male mice (BALB/c).
Methods
Forty Five mice were divided into three groups: control, A/L, and A/A. The drugs were administered three days in a row per week, and the regimen was repeated every two weeks for a total of six cycles. The levels of oxidative stress and liver function markers were measured in both plasma and liver tissue after initial (baseline) and repeated exposures for the second, third, and sixth cycles.
Results
Exposure to A/L or A/A caused a significant (p < 0.001) increase in plasma malondialdehyde (MDA) levels after the first and repeated exposure periods. However, Hepatic MDA levels increased significantly (p < 0.01) only after the sixth exposure to A/A. Following either single or repeated exposure to A/L or A/A, plasma and liver glutathione peroxidase (GPx) and catalase (CAT) activities, plasma aspartate and alanine transaminase, alkaline phosphatase activity, and bilirubin levels increased, whereas total plasma protein levels decreased significantly (p < 0.001). Varying degrees of hepatocyte degeneration and blood vessel congestion were observed in liver tissues after a single or repeated treatment period.
Conclusion
Irrespective of single or repeated exposure to therapeutic doses of A/L or A/A, plasma oxidative stress and liver damage were observed. However, long-term repeated A/A exposure can led to hepatic stress. Compensatory processes involving GPx and CAT activities may help reduce the observed stress.
Similar content being viewed by others


Background
Malaria is a serious infectious disease caused by the Plasmodium parasite and transmitted by infected female Anopheles mosquitos. There are an estimated 247 million malaria cases in 84 endemic countries in 2021, with almost all malaria cases recorded in 29 countries, including Nigeria (27%), the Democratic Republic of the Congo (12%), Uganda (5%), and Mozambique (4%), accounting for nearly half of all global cases [1]. Between 2000 and 2021, approximately 2 billion malaria infections and 11.7 million fatalities were averted globally [1] using several malaria intervention strategies, including insecticide-treated nets, indoor spraying, prophylactic treatments, and antimalarial medications, particularly Artemisinin-based Combination Therapies (ACTs) [1,2,3,4].
In malaria-endemic nations in Africa, ACTs such as artemether/lumefantrine and artesunate/amodiaquine have proven to be highly efficient in clearing malaria parasites [5, 6]. Artemether and Artesunate are fast-acting artemisinin derivatives that swiftly reduce parasite burden [7, 8]. These drugs are metabolised into dihydroartemisinin by the liver [7, 8], with the generation of reactive free radicals (in the presence of haeme) within the parasite, damaging the parasite's lipids, proteins, and DNA, resulting in parasite death. The lumefantrine and amodiaquine components of A/L and A/A, on the other hand, are longer-acting antimalarials that prevent parasite recrudescence, ensure long-term parasite clearance [8,9,10], and reduce the ability of the parasite to detoxify haeme, leading to the accumulation of toxic haeme molecules, ultimately causing parasite death [3]. Lumefantrine and amodiaquine is extensively metabolised in the liver to produce desbutyl-lumefantrine and desethyl-amodiaquine which is active against malaria parasites [7, 11],
A/L and A/A can cause various adverse effects, including nausea, vomiting, dizziness, headaches, skin rashes, gastrointestinal problems, and hepatic dysfunction, and should be used with caution in individuals with pre-existing liver illnesses [3, 12]. The specific process by which A/L and A/A toxicity occurs is unknown; however, it is considered to be linked to the metabolism of the drug by the liver and its activities in the blood [3]. Repetitive use of A/L and A/A can increase toxicity, especially in high-risk populations, such as pregnant women, children, and travellers from non-endemic countries who take these drugs as preventive measures, as well as in areas with high rates of drug resistance, recurrent infections, and antimalarial drug misuse [13,14,15,16,17,18,19,20].
Previous studies have shown that both A/L and A/A can cause oxidative stress [14, 21,22,23,24,25,26,27], as well as elevated liver function markers (aspartate transaminase (AST), alanine transaminase (ALT), total protein, and bilirubin) [14, 21], but little is known about the levels of oxidative stress in the plasma and liver caused by repeated therapeutic treatment with A/L or A/A. Although a study of repeated ACT treatments revealed that when rats were administered oral doses of A/L for six weeks, hepatotoxicity was observed, as indicated by an increase in the activity of liver enzymes such as glutamyltransferase, AST, and ALT; however, the study did not explore the use of A/A (another ACT alternative), compare different repeated treatment periods, or examine oxidative stress markers [18]. Our team also demonstrated that repeated A/L and A/A administration in mice influences haematological parameters [28]. Additionally, our previous study on the repeated use of antimalarial drugs in liver cell lines, including the individual component drugs artesunate, amodiaquine, artemether, and lumefantrine, showed significantly decreased cell viability for up to 72 h, likely due to oxidative stress [29]. However, the oxidative stress and liver function effect of ACT administered therapeutically on a two-week interval basis, which is reflective of common user practice during repeated drug abuse, has not yet been explored. Consequently, this study aimed to evaluate the effects of repeated A/L and A/A treatments on oxidative stress and liver function markers in the plasma and liver of mice.
Methods
Animals’ procurement and management
This study used 45 mature male BALB/c mice weighing an average of 24 g and were 8 weeks old. Mice were obtained from the Institute of Advanced Medical Research and Training at the University College Hospital (UCH) in Ibadan, Nigeria. The mice were housed in plastic cages with dry wood shavings as bedding and fed standard feed produced by Ladokun Feed Limited (Ibadan, Oyo State, Nigeria). The mice were provided with food and water and kept on a 12-h light/12-h dark cycle.
Antimalaria drug
Artemether/lumefantrine (A/L) (Lumartem Antimalarial Tablet, 20 mg/120 mg) was obtained from Cipla Pharmaceuticals Limited in Mumbai, India, and Artesunate/Amodiaquine (A/A) (Camosunate; 100 mg/300 mg) was procured from Geneith Pharmaceuticals Limited in Lagos, Nigeria. Therapeutic doses were orally administered to all treatment groups according to the manufacturer's instructions. A therapeutic dose of 1.14/6.84 mg/kg/d of artemether/lumefantrine was administered in six doses at 0, 8, 24, 36, 48, and 60 h, while artesunate/amodiaquine was given three consecutive days per week at a dose of 2.86/8.58 mg/kg/d [30, 31].
Research design
A total of 45 male mice were randomly assigned to three groups using a previously described method [32]. Each group consisted of 15 mice kept in three cages, each containing five mice [33].
-
Group 1: Received only distilled water (Control),
-
Group 2: Were administered Artemether / Lumefantrine (A/L) and
-
Group 3: Were administered Artesunate / Amodiaquine (A/A)
The drugs were administered three consecutive days per week, with a two-week break between each repeated treatment, for a total of six cycles of exposure. Daily weight was measured, and plasma glucose level, plasma and liver tissue oxidative stress, and liver function markers were determined after the first (baseline) and repeated exposure periods of the second, third, and sixth periods. The experiments were performed in accordance with the Guide for the Care and Use of Laboratory Animals of the National Institutes of Health (NIH Publication No. 85–23, updated in 1996). The experimental protocol was approved by the College of Veterinary Medicine Research Ethics Committee of the Federal University of Agriculture, Abeokuta (FUNAAB/COLVET/CREC/2019/07/01).
Glucose concentration
The plasma glucose concentration was determined following the method described in [34].
Oxidative stress markers
Plasma and liver homogenates were evaluated for oxidative stress markers. The concentration of malondialdehyde (MDA) was evaluated using the thiobarbituric acid-reactive substances (TBARS) – malondialdehyde (MDA) technique [35]. The concentration of glutathione (GSH) was determined using the method described by Ilman ([36]. Glutathione peroxidase (GPx) activity was assessed following the method described by Rotruck et al. [37]. Superoxide dismutase (SOD) activity was determined using the method described by Marklund and Marklund [38]. Catalase (CAT) activity was determined according to the method described by Shangari and O’Brien [39].
Liver function markers
The activities of aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), total protein, and bilirubin were determined in plasma and liver homogenates using commercially available kits obtained from Fortress Diagnostics Limited (UK) following the manufacturer’s instructions. ALT and AST levels were measured using the method described by Reitman and Frankel [40], whereas ALP levels were measured using the method reported by Rec [41]. Total bilirubin and protein concentrations were determined according to the method described by Tietz [42].
Histopathological analysis of the liver
Part of the collected liver tissue was stored in 10% formalin in appropriately labelled bottles. Thereafter, the organs were dehydrated by passing them through increasing concentrations of ethanol (50, 70, 80, 90, and 100% for one hour each). Thereafter, the organs were impregnated with three changes of molten xylene and replaced with paraffin wax. The organs were embedded in molten paraffin wax and allowed to solidify. The blocks were mounted on a microtome and sectioned at 5 µm. Each sectioned tissue was mounted on a slide and placed on a hot plate to melt the wax. The tissues were stained with haematoxylin and eosin. The stained slides were observed under a compound microscope for observable aberrations, and photomicrographs of the slides were obtained.
Statistical analysis
Graphs were generated using GraphPad Prism 9.0, with one-way analysis of variance (ANOVA) to determine the significance of the differences between the treated and control groups. The results are shown as mean ± standard error of the mean (SEM) (n = 3). The Shapiro–Wilk test was initially employed to check whether the distribution of the data was normal. Significance was set at p < 0.05, p < 0.01, and p < 0.001 compared to the relevant control group.
Results
Effects of repeated therapeutic treatment with artemether/lumefantrine (A/L) or artesunate/amodiaquine (A/A) on mouse weight and glucose levels
Table 1 shows the observed increase in the percentage change in the body weight of mice administered either artemether/lumefantrine (A/L) or artesunate/amodiaquine (A/A) during the first, second, third, and sixth exposure periods, as well as in the control group. After the initial treatment with A/L, a marked increase in glucose concentration was observed. However, subsequent treatment with A/L or A/A after the second, third, and sixth exposure periods did not lead to any noteworthy alterations in glucose concentration compared to the control group, as shown in Table 1.
The impact of repeated treatment with either artemether/lumefantrine (A/L) or artesunate/amodiaquine (A/A) on oxidative stress markers in mice
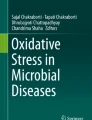
Plasma malondialdehyde (MDA) concentrations were significantly higher than those in the control group after treatment with A/L or A/A during the first (134% or 107%) (p < 0.001), second (133% or 74%) (p < 0.001), third (142% or 64%) (p < 0.001), and sixth (90% (p < 0.001) or 31% (p < 0.05)) exposure periods (Fig. 1A). Following the first, second, and third exposure periods, there were no significant alterations in MDA concentrations in the liver between the treatment groups (A/L or A/A) and the control group (Fig. 1B). Nevertheless, after the sixth exposure period, the administration of A/A significantly increased (p < 0.01) the liver MDA concentration by 37%, whereas A/L administration led to a significant decrease (p < 0.01) in the liver MDA concentration by 35% compared to the control group. (Fig. 1B).

(A) Plasma Malondialdehyde (MDA) concentration, (B) Liver Malondialdehyde (MDA) concentration, (C) Plasma Glutathione (GSH) concentration, (D) Liver Glutathione (GSH) concentration of mice after the 1st, 2nd 3rd, and 6th treatment with artemether/lumefantrine (A/L) or artesunate/amodiaquine (A/A). Values are expressed as mean ± SEM (n = 3), and a, b, and c indicate significant differences at p < 0.05, p < 0.01, and p < 0.001, respectively, compared to the corresponding control groups
Except for the A/L treatment after the third exposure period, which exhibited a significant increase in plasma glutathione (GSH) by 9% (p < 0.05) (Fig. 1C), no significant alterations were observed in either plasma or liver GSH concentrations following single and repeated treatments (Fig. 1C and D).
A significant increase in plasma Glutathione Peroxidase (GPx) activity of 87% (p < 0.001) was observed after the first treatment with A/L compared to that in the control group (Fig. 2A). Repeated treatment with A/L or A/A for the second and third periods significantly increased Plasma GPx by (50% (p < 0.05) or 72% (p < 0.001)) and (40% (p < 0.05) or 26% (p < 0.05)) respectively, compared to the control group, while after the sixth treatment, no significant alteration was observed compared to the control group (Fig. 2A). Treatment with A/A after the first, second, third, and sixth exposure periods significantly increased liver GPx activity by 68% (p < 0.001), 18% (p < 0.01), 22% (p < 0.001), and 17% (p < 0.01), respectively, compared to the control group (Fig. 2B). Treatment with A/L significantly increased (p < 0.001) liver GPx activity (p < 0.001) by 19% after the first exposure period, but no significant changes were observed after the second, third, and sixth exposure periods compared to the control group (Fig. 2B).

(A) Plasma Glutathione peroxidase (GPx) activities (B) Liver Glutathione peroxidase (GPx) activities (C) Plasma superoxide dismutase (SOD) activities (D) Liver superoxide dismutase (SOD) activities of mice after the 1st, 2nd, 3rd, and 6th exposures to either artemether/lumefantrine (A/L) or artesunate/amodiaquine (A/A). Values are expressed as mean ± SEM (n = 3), and a, b, and c indicate significant differences at p < 0.05, p < 0.01, and p < 0.001, respectively, compared to the corresponding control groups
Plasma superoxide dismutase (SOD) activity increased by 116% (p < 0.001) and 50% (p < 0.001) after exposure to A/L for the first and third treatment periods, respectively, and by 81% (p < 0.01) after treatment with A/A for the second treatment period, compared to the control groups (Fig. 2C). No significant increase in plasma SOD activity was observed after exposure to either A/L or A/A for the 6th treatment period (Fig. 2C). Liver SOD activity significantly increased (85%, p < 0.001) after the first A/A treatment period, whereas no significant changes were observed after repeated treatment periods (Fig. 2D).
Plasma Catalase (CAT) activity significantly increased after treatment with either A/L or A/A for the first (563% or 452%; p < 0.001), second (452% or 414%; p < 0.001), third (260%; p < 0.01 or 437%; p < 0.001), and sixth (792%; p < 0.001 or 454%; p < 0.05) exposures compared to the control group (Fig. 3A). In the liver, CAT activity increased significantly (p < 0.001) after A/L or A/A treatment for the first (60% or 47%), second (34% or 35%), and sixth (32% or 25%) exposure periods, whereas only A/L exposure after the third period significantly increased liver CAT activity by 22% compared to the control group (Fig. 3B).

(A) Plasma Catalase (CAT) Activities (B) Liver Catalase (CAT) Activities (C) Plasma Total Protein (TP) concentration (D) Liver Total Protein Concentration of mice after the 1st, 2nd, 3rd, and 6th treatments with either artemether/lumefantrine (A/L) or artesunate/amodiaquine (A/A) compared to the control group. Values are expressed as mean ± SEM (n = 3), and a, b, and c indicate significant differences at p < 0.05, p < 0.01, and p < 0.001, respectively, compared to the corresponding control groups
Effects of repeated therapeutic treatment with either artemether/ lumefantrine (A/L) or artesunate/amodiaquine (A/A) on mice Liver function markers
Treatment with A/L or A/A significantly reduced (p < 0.001) the plasma total protein content after the first (44% or 23%), second (25% or 40%), third (32% or 28%), and sixth (32% or 32%) treatments compared to the control group (Fig. 3C). After the third A/L or A/A exposure period, the total hepatic protein level significantly decreased (p < 0.001) by 20% or 24%, respectively (Fig. 3D), whereas after the sixth exposure period, no significant decrease was observed compared to that in the control group (Fig. 3D).
The plasma Aspartate Aminotransferase (AST) activities significantly increased after A/L treatment for the second and sixth periods by 74% and 84% (p < 0.05), while Treatment with A/A for the second, third, and sixth periods by 137%, 100%, and 187%, respectively (p < 0.001), compared to the control group (Fig. 4A). Liver AST activity significantly decreased after exposure to both A/L or A/A for the first (59% or 57%; p < 0.001), second (56% or 72%; p < 0.001), third (38%; p < 0.05 or 61%; p < 0.001), and sixth (71% or 58%; p < 0.001) periods, respectively, compared to the control group (Fig. 4B).

(A) Plasma Aspartate Transaminase (AST) activities (B) Liver Aspartate Transaminase (AST) activities (C) Plasma Alanine Transaminase (ALT) activities (D) Liver Alanine Transaminase (ALT) activities of mice after the 1st, 2nd, 3rd, and 6th exposures to either artemether/lumefantrine (A/L) or artesunate/amodiaquine (A/A) compared to the control. Values are expressed as mean ± SEM (n = 3), and a, b, and c indicate significant differences at p < 0.05, p < 0.01, and p < 0.001, respectively, compared to the corresponding control groups
Plasma Alanine Aminotransferase (ALT) activity significantly increased (p < 0.001) following the first treatment with A/L or A/A by 246% or 102%, respectively, whereas repeated treatment with A/L and A/A did not significantly alter ALT plasma activity compared to the control group (Fig. 4C). Exposure to A/L during the first exposure period significantly increased (p < 0.001) liver ALT activity by 253%, whereas repeated treatment with A/L and A/A during the second, third, and sixth exposure periods did not significantly alter liver ALT activity compared to that in the control group (Fig. 4D).
The plasma Alkaline Phosphatase (ALP) activity significantly increased after Treatment with A/L for the 2nd and 3rd exposure periods by 98% (p < 0.05) and 432% (p < 0.001), respectively, while A/A treatment after the 1st, 2nd, 3rd, and 6th exposure periods by 213% (p < 0.001), 163% (p < 0.001), 355% (p < 0.001), and 106% (p < 0.01), respectively, compared to the control group (Fig. 5A). Only A/L treatment after the first exposure period significantly increased (p < 0.001) liver ALP activity by 273%, whereas repeated exposure to A/L and A/A did not significantly alter liver ALP activity (Fig. 5B).

(A) Plasma Alkaline Phosphatase (ALP) Activities (B) Liver Alkaline Phosphatase (ALP) activities (C) Plasma Bilirubin Concentration (D) Liver Bilirubin Concentration; of mice after the 1st, 2nd, 3rd and 6th treatment with either Artemether/Lumefantrine (A/L) or Artesunate/Amodiaquine (A/A) compared to the control group. Values are expressed as mean ± SEM (n = 3), and a, b, and c indicate significant differences at p < 0.05, p < 0.01, and p < 0.001, respectively, compared to the corresponding control groups
Plasma bilirubin levels increased significantly after A/L treatment following the first, second, and third exposures by 35% (p < 0.001), 21% (p < 0.01), and 40% (p < 0.001), respectively, while A/A Treatment following the first, third, and sixth exposure periods by 19% (p < 0.05), 28% (p < 0.001), and 34% (p < 0.001), respectively, compared to the control group (Fig. 5C). liver bilirubin levels did not change significantly after repeated exposure to A/L or A/A (Fig. 5D).
Single and repeated administration of AL or AA resulted in diverse levels of hepatocyte degeneration and blood vessel congestion in the mouse liver tissue, as opposed to the control group, which exhibited a normal histological appearance (Figs. 6 and 7).

Liver Histology section (× 400; H & E) of mice treated with distilled water (control) (CTL) artemether/lumefantrine (A/L) or artesunate/amodiaquine (A/A) after the (A) first and (B) second exposure periods. Congestion of blood vessels (arrow) and degeneration of hepatocytes (bent arrow)

Liver Histology section (× 400; H & E) of mice treated with distilled water (control), artemether/lumefantrine (A/L), and artesunate/amodiaquine (A/A) after the (C) third and (D) sixth periods. Congestion of blood vessels (arrow) and degeneration of hepatocytes (bent arrow)
Discussion
This study is the first to investigate the effects of six consecutive repeated therapeutic treatments with artesunate/amodiaquine (A/A) or artesunate/lumefantrine (A/L) on oxidative stress and liver function markers in mice at two-week intervals. The goal was to simulate a scenario in which an individual takes antimalarial drugs prophylactically every two weeks, for a maximum of six cycles.
The results showed that neither single nor repeated treatments with A/L or A/A affected the normal growth of the mice or caused a decrease in the plasma glucose level. However, the plasma concentration of malondialdehyde (MDA), a marker of lipid peroxidation, increased to a similar level in both single and repeated treatments. Previous studies have reported elevated MDA levels following A/L and A/A administration [14, 21]. Nevertheless, this study found that either single or repeated therapeutic use of A/L or A/A caused comparable lipid peroxidation or oxidative stress in mice. This could be because the mice were administered the drugs therapeutically after each treatment and were given a rest period before the next treatment, thus not allowing for cumulative effects. Interestingly, the plasma MDA concentration after the sixth A/L or A/A treatment did not increase, but was lower than that seen during the first three treatments. This could be attributed to the acclimatisation of mice to oxidative stress caused by the treatment over time [43]. Furthermore, A/L had a more pronounced effect on plasma MDA concentration than A/A after each successive treatment, suggesting that A/L may induce greater lipid peroxidation and oxidative stress in the plasma than A/A. The difference in the plasma oxidative stress response between A/L and A/A may be linked to the pharmacokinetics and pharmacodynamics of the drugs. It is possible that one of the component drugs in A/L may have a more powerful effect on oxidative stress pathways in the plasma than the other, or the combination of drugs in A/L may interact differently in the plasma with the host's response to oxidative stress than A/A.[7, 44].
The study also found that after the sixth treatment with A/A, there was a significant increase in liver MDA concentration, indicating that prolonged use of A/A could potentially trigger more oxidative stress and lipid peroxidation in the liver than A/L. The amodiaquine component of A/A is likely responsible for this increase, since the liver is responsible for its biotransformation and clearance, which can induce liver cell toxicity and lead to cumulative effects observed after the sixth treatment [45].
Repeated or one-time exposure to either A/L or A/A resulted in a significant increase in the activity of glutathione peroxidase (GPx) and catalase (CAT) in the plasma and liver. This increase in antioxidant activity may be attributed to an adaptive response to oxidative stress caused by exposure to A/L, A/A, or their metabolites in mice [46, 47]. The GPx/GSH/SOD/CAT antioxidant system plays an important role in the regulation of oxidative stress [48]. GPx reduces hydrogen peroxide and lipid hydroperoxides, whereas CAT decomposes hydrogen peroxide into water and oxygen [48]. Our results suggest that the observed increase in antioxidant activity may be attributed to the upregulation of antioxidant defense mechanisms, which help eliminate reactive oxygen species when these drugs are taken repeatedly but therapeutically [23, 46, 47]. This finding is contrary to that of Adebayo et al., [49] who revealed that the treatment of mice with A/A led to a significant decrease in GSH, CAT, and SOD activities, and that of Idowu et al., [14] who revealed decreased SOD and CAT levels in rats treated with A/L. However, the results of this study are consistent with those of Abolaji et al. [21], who showed that the activities of GPx, GST, and SOD increased in the treated groups, and that of Anyasor et al.[23], who also reported that treatment of mice with A/L increased hepatic GSH, GST, and CAT activities [23].
On the liver function side, both A/L and A/A led to increased plasma levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and bilirubin after therapeutic exposure, either as a single or repeated exposure, up to six times. Elevated plasma liver enzyme and bilirubin levels indicate potential liver damage caused by drug administration. The generation of reactive species during A/L and A/A metabolic biotransformations in the liver may explain the observed increase in liver enzyme levels. During drug metabolism, they can induce oxidative stress in organs, leading to potential tissue damage and a subsequent increase in serum enzyme activity[14, 27]. This explanation is further supported by the decrease in liver AST activity following exposure to A/A or A/L (Fig. 4B), as this could have leaked out to the plasma, increasing its level in the plasma. The components of A/L or A/A responsible for this increase in liver enzyme levels could be lumefantrine and amodiaquine, as artemisinin and its derivatives (artemether or artesunate) are known to have low toxicological effects [50]. The present findings are in line with earlier studies which revealed an increase in transaminase levels following therapeutic doses of artemether, lumefantrine, and A/L [18, 21, 25]. In another study, mice infected with Plasmodium berghei and treated with A/L and A/A showed elevated levels of AST, ALT, and ALP [25]. Additionally, a separate study discovered that combining A/L or A/A with paracetamol resulted in increased AST, ALT, and ALP levels in humans [22]. Our research has made a valuable contribution to the existing knowledge by demonstrating that the increase in these liver function markers was quite similar after each treatment, whether after a single treatment or each repeated treatment, as long as the drugs are administered therapeutically and at appropriate intervals.
Moreover, this study revealed that both A/L and A/A caused similar degeneration of hepatocytes and blood congestion in the liver tissue after single and repeated treatments. This deterioration of hepatocytes could lead to impaired drug metabolism and clearance, potentially resulting in increased drug accumulation and toxicity, whereas blood vessel congestion could hinder proper blood flow and oxygen delivery to the liver tissue, further compromising its function [51, 52]. This pathological observation may have caused low protein synthesis, contributing to the decreased plasma and liver total protein levels observed after the first and repeated exposures to A/L and A/A [50, 53].
Conclusions
In conclusion, these results indicate that both single and repeated administration of A/L or A/A induce significant levels of oxidative stress in the plasma and may cause liver damage. However, prolonged A/A use results in higher levels of oxidative stress in the liver. The observed increase in antioxidant levels may counteract the stress induced by these drugs. Therefore, therapeutic treatment with either A/L or A/A, whether single or repeated, requires careful monitoring of hepatic function. Further research is needed to comprehensively investigate the impact of A/L and A/A on individuals taking these drugs as prophylactic measures to facilitate a more accurate translation of these findings to human subjects.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- W.H.O:
-
World Health Organization
- ACTs:
-
Artemisinin Combination Therapies
- A/L:
-
Artemether Lumefantrine
- MDA:
-
Malondialdehyde
- GSH:
-
Glutathione
- GPx:
-
Glutathione peroxidase
- SOD:
-
Superoxide dismutase
- CAT:
-
Catalase
- AST:
-
Aspartate Aminotransferase
- ALT:
-
Plasma Alanine Aminotransferase
- ALP:
-
Alkaline Phosphatase
References
W.H.O (2022) World malaria report 2022. https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022. Accessed 17 Mar 2023
Abolaji AO, Osedeme F, Olusemire O (2014) Artesunate-amodiaquine combination therapy in the absence of malarial parasite infection induces oxidative damage in female rats. Cell Biochem Funct 32:303–308. https://doi.org/10.1002/CBF.3020
Audu D, Petagine L, Idowu OA et al (2023) Biomarkers of the toxic effects of chemotherapeutic agents: a focus on antimalarials. pp 1–27. https://doi.org/10.1007/978-3-030-87225-0_73-2
Wangdi K, Furuya-Kanamori L, Clark J, et al (2018) Comparative effectiveness of malaria prevention measures: a systematic review and network meta-analysis. Parasit Vectors 11. https://doi.org/10.1186/S13071-018-2783-Y
Obiebi IP (2019) Adherence to antimalarial drug policy among doctors in Delta State, Nigeria: Implications for malaria control. Ghana Med J 53:109–116. https://doi.org/10.4314/gmj.v53i2.5
Ouji M, Augereau JM, Paloque L, Benoit-Vical F (2018) Plasmodium falciparum resistance to artemisinin-based combination therapies: A sword of Damocles in the path toward malaria elimination. Parasite 25:24. https://doi.org/10.1051/PARASITE/2018021
Kerb R, Fux R, Mörike K et al (2009) Pharmacogenetics of antimalarial drugs: effect on metabolism and transport. Lancet Infect Dis 9:760–774. https://doi.org/10.1016/S1473-3099(09)70320-2
Mwesigwa J, Parikh S, McGee B et al (2010) Pharmacokinetics of artemether-lumefantrine and artesunate-amodiaquine in children in Kampala, Uganda. Antimicrob Agents Chemother 54:52–59. https://doi.org/10.1128/AAC.00679-09
Egunsola O, Oshikoya KA (2013) Comparative safety of artemether-lumefantrine and other artemisinin-based combinations in children: a systematic review. Malar J 12. https://doi.org/10.1186/1475-2875-12-385
Rakotoarisoa MA, Fenomanana J, Dodoson BT et al (2022) Comparative effect of artemether-lumefantrine and artesunate-amodiaquine on gametocyte clearance in children with uncomplicated Plasmodium falciparum malaria in Madagascar. Malar J 21:331. https://doi.org/10.1186/s12936-022-04369-2
Hodoameda P, Duah-Quashie NO, Quashie NB (2022) Assessing the Roles of Molecular Markers of Antimalarial Drug Resistance and the Host Pharmacogenetics in Drug-Resistant Malaria. J Trop Med 2022:1–9. https://doi.org/10.1155/2022/3492696
Alkadi HO (2007) Antimalarial drug toxicity: A review. Chemotherapy 53:385–391. https://doi.org/10.1159/000109767
Cohen J, Fink G, Berg K, et al (2012) Feasibility of Distributing Rapid Diagnostic Tests for Malaria in the Retail Sector: Evidence from an Implementation Study in Uganda. PLoS ONE 7. https://doi.org/10.1371/journal.pone.0048296
Idowu ET, Alimba CG, Olowu EA, Otubanjo AO (2015) Artemether-Lumefantrine treatment combined with albendazole and ivermectin induced genotoxicity and hepatotoxicity through oxidative stress in Wistar rats. Egyptian Journal of Basic and Applied Sciences 2:110–119. https://doi.org/10.1016/j.ejbas.2015.03.001
Mbonye AK, Ndyomugyenyi R, Turinde A et al (2010) The feasibility of introducing rapid diagnostic tests for malaria in drug shops in Uganda. Malar J 9:1–8. https://doi.org/10.1186/1475-2875-9-367
Mbonye AK, Lal S, Cundill B et al (2013) Treatment of fevers prior to introducing rapid diagnostic tests for malaria in registered drug shops in Uganda. Malar J 12:1–10. https://doi.org/10.1186/1475-2875-12-131
Nwokolo E, Ujuju C, Anyanti J et al (2018) Misuse of Artemisinin Combination Therapies by Clients of Medicine Retailers Suspected to Have Malaria Without Prior Parasitological Confirmation in Nigeria. Kerman Univ Med Sci 7:542–548. https://doi.org/10.15171/ijhpm.2017.122
Owumi SE, Gbadegesin MA, Odunola OA et al (2015) Toxicity associated with repeated administration of artemether-lumefantrine in rats. Environ Toxicol 30:301–307. https://doi.org/10.1002/tox.21907
Rusk A, Goodman C, Naanyu V, et al (2013) Expanding access to malaria diagnosis through retail shops in western kenya: What do shop workers think? Malar Res Treat 2013. https://doi.org/10.1155/2013/398143
Yeung S, Patouillard E, Allen H, Socheat D (2011) Socially-marketed rapid diagnostic tests and ACT in the private sector: Ten years of experience in Cambodia. Malar J 10. https://doi.org/10.1186/1475-2875-10-243
Abolaji AO, Eteng MU, Omonua O, Adenrele Y (2013) Influence of coadministration of artemether and lumefantrine on selected plasma biochemical and erythrocyte oxidative stress indices in female Wistar rats. Hum Exp Toxicol 32:206–215. https://doi.org/10.1177/0960327112464666
Aghahowa SE, Ozolua RI, Bafor EE et al (2021) Toxicological effect of Artemisinin-Based Combination Therapies plus Paracetamol in malaria patients. Toxicol Rep 8:1930–1936. https://doi.org/10.1016/j.toxrep.2021.11.007
Anyasor GN, Oyewole IO, Ogunwenmo KO, Ayowole A (2012) Coartemether induced oxidative and hepatic damage in plasmodium berghei strain anka infected mice. Bull Environ Contam Toxicol 88:108–111. https://doi.org/10.1007/s00128-011-0460-3
Bukunola A, Olugbenga O, Aramide A, Emmanuel A (2014) Comparative study of protective effect of separate administration of vitamin c and folic acid in ACT therapy induced hepatic injury. academicjournals.org 9:189–194. https://doi.org/10.5897/SRE2013.5678
Edagha I, Ekpo A, Edagha E et al (2019) Investigating the comparative effects of six artemisinin-based combination therapies on Plasmodium-induced hepatorenal toxicity. Niger Med J 60:211. https://doi.org/10.4103/nmj.nmj_152_18
Silva-Pinto A, Ruas R, Almeida F, et al (2017) Artemether-lumefantrine and liver enzyme abnormalities in non-severe Plasmodium falciparum malaria in returned travellers: A retrospective comparative study with quinine-doxycycline in a Portuguese centre. Malar J 16. https://doi.org/10.1186/S12936-017-1698-Y
Ugian E, Dasofunjo K, … JN-J of A, 2013 undefined (2013) Effect of artemisinin-based combination therapy on some selected liver function indices of pregnant Wistar Albino rats. japsonline.com 3:152–154. https://doi.org/10.7324/JAPS.2013.3926
Audu D, Ajoke O, Vinood B, Mshelbwala F (2022) The effects of repeated therapeutic administration of artesunate-amodiaquine and artemether-lumefantrine on haematological markers in healthy mice. https://doi.org/10.21203/rs.3.rs-2186132/v1
Audu D, Patel V, Idowu OA, et al (2023) Repeated treatment with antimalarial agents causes in vitro liver toxicity. Liver Res. https://doi.org/10.17140/LROJ-4-113
Daikwo OA, Kawu MU, Magaji RA, Eze ED (2018) Effect of Prolonged Administration of Artemether-Lumefantrine on Testicular Biomarkers of Oxidative Stress: Ameliorative Effect of Vitamin E. Basic Sciences of Medicine 7:1–6. https://doi.org/10.5923/j.medicine.20180701.01
Otuechere CA, Edewor G, Kale OE, Ekor M (2012) Subacute therapeutic dosing of artemether-lumefantrine and artesunate-amodiaquine combination preserves plasma cholesterol, renal antioxidant status, and organ weights in rats. Malar Res Treat 2012. https://doi.org/10.1155/2012/257986
Johnson PD, Besselsen DG (2002) Practical aspects of experimental design in animal research. ILAR J 43:202–206. https://doi.org/10.1093/ilar.43.4.202
Charan J, Kantharia N (2013) How to calculate sample size in animal studies? J Pharmacol Pharmacother 4:303–306. https://doi.org/10.4103/0976-500X.119726
Gros M, Smrekar M (1967) An aniline-acetic acid method for body fluid glucose determination. Clin Chim Acta 17:518–519. https://doi.org/10.1016/0009-8981(67)90232-X
Beuge J, Aust S (1978) The thiobarbituric acid assay
Ellman GL (1959) Tissue sulfhydryl groups. Arch Biochem Biophys 82:70–77. https://doi.org/10.1016/0003-9861(59)90090-6
Rotruck JT, Pope AL, Ganther HE et al (1973) Selenium: Biochemical role as a component of glatathione peroxidase. Science 179:588–590. https://doi.org/10.1126/SCIENCE.179.4073.588
Marklund S, Marklund G (1974) Involvement of the Superoxide Anion Radical in the Autoxidation of Pyrogallol and a Convenient Assay for Superoxide Dismutase. Eur J Biochem 47:469–474. https://doi.org/10.1111/j.1432-1033.1974.tb03714.x
Shangari N, O’Brien PJ (2006) Catalase activity assays. Current protocols in toxicology / editorial board, Mahin D Maines (editor-in-chief) . [et al] Chapter 7: https://doi.org/10.1002/0471140856.tx0707s27
Reitman S, Frankel S (1957) Determination of glutamate-pyruvate transaminase (ALT) and aspartate amino transferase (AST). J Clin Pathol 28:56
Rec GSCC (1972) Colorimetric method for serum alkaline phosphatase determination. Journal of Clinical Biochemistry 10:182–184
Tietz NW (1995) Clinical guide to laboratory tests, 3rd edn. W.B. Saunders Co., Philadelphia
Pickering AM, Vojtovich L, Tower J, Davies KJA (2013) Oxidative stress adaptation with acute, chronic, and repeated stress. Free Radical Biol Med 55:109–118. https://doi.org/10.1016/j.freeradbiomed.2012.11.001
White NJ, Van Vugt M, Ezzet F (1999) Clinical Pharmacokinetics and Pharmacodynamics of Artemether-Lumefantrine. Clin Pharmacokinet 37:105–125. https://doi.org/10.2165/00003088-199937020-00002
Li XQ, Björkman A, Andersson TB et al (2002) Amodiaquine Clearance and Its Metabolism toN-Desethylamodiaquine Is Mediated by CYP2C8: A New High Affinity and Turnover Enzyme-Specific Probe Substrate. J Pharmacol Exp Ther 300:399–407. https://doi.org/10.1124/JPET.300.2.399
Christou K, Gourgoulianis KI (2007) Reactive oxygen metabolites (ROMs) as an index of oxidative stress in obstructive sleep apnea patients. Oxidative Stress and Neurodegenerative Disorders 247–265. https://doi.org/10.1016/B978-044452809-4/50152-6
Li S, Tan HY, Wang N et al (2015) The role of oxidative stress and antioxidants in liver diseases. Int J Mol Sci 16:26087–26124. https://doi.org/10.3390/ijms161125942
Ighodaro OM, Akinloye OA (2018) First line defence antioxidants-superoxide dismutase (SOD), catalase (CAT) and glutathione peroxidase (GPX): Their fundamental role in the entire antioxidant defence grid. Alexandria J Med 54:287–293. https://doi.org/10.1016/J.AJME.2017.09.001
Adebayo AH, Okenze GN, Yakubu OF, Abikoye ME (2018) Biochemical and histopathological effects of coadministration of amodiaquine, artesunate, and selenium on Plasmodium berghei infected mice. Asian J Pharm Clin Res 11:13–16
Chinwendu Amorha K, Ugwuowo OB, Ayogu EE et al (2018) Evaluation of the hepatic effect of concomitant administration of ciprofloxacin and some antimalarial drugs in Plasmodium berghei infected mice: An in vivo study. Pak J Pharm Sci 31:1805–1811
Ward L, Wilcock J, Butler P (2021) Drug Metabolism Assessment: Hepatocytes. The ADME Encyclopedia: A Comprehensive Guide on Biopharmacy and Pharmacokinetics. Springer International Publishing, Cham, pp 1–12
Dutta S, Mishra SP, Sahu AK, Mishra K, Kashyap P, Sahu B (2021) Hepatocytes and their role in metabolism. Drug Metab 3
Sen S, De B, Devanna N, Chakraborty R (2013) Cisplatin-induced nephrotoxicity in mice: Protective role of Leea asiatica leaves. Ren Fail 35:1412–1417. https://doi.org/10.3109/0886022X.2013.829405
Acknowledgements
I want to thank the Nigerian Federal Government Tertiary Education Trust Fund (TETfund) for the grant support of this work.
Funding
The research Animal and laboratory work was funded by the Nigeria Federal Government Tertiary education trust fund (TETfund).
Author information
Authors and Affiliations
Contributions
DA, OAI, and ABI came up with the experiment's idea. DA, OAI, ABI, and FMM designed the research methodology and conducted the experiments. VAB provided technical assistance for the liver study. AD and VAB drafted the manuscript. The final version was read, edited, and approved by all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The College of Veterinary Medicine research ethics committee at the Federal University of Agriculture, Abeokuta, Approved the experimental protocol (FUNAAB/COLVET/CREC/2019/07/01). The experiments were conducted in accordance with the National Institutes of Health's Guide for the Care and Use of Laboratory Animals (NIH Publication No. 85–23, revised in 1996).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Audu, D., Patel, V.B., Idowu, O.A. et al. Baseline and recurrent exposure to the standard dose of artemisinin-based combination therapies (ACTs) induces oxidative stress and liver damage in mice (BALB/c). Egypt Liver Journal 13, 53 (2023). https://doi.org/10.1186/s43066-023-00291-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-023-00291-7