
Abstract
Background and aim
Currently, nonalcoholic liver disease (NAFLD) is the most predominant chronic liver disorder. NAFLD has been linked to hepatic and extrahepatic morbidities. We aimed to investigate the role of acoustic radiation force impulse (ARFI), hepatorenal index (HRI), and serum microRNA-130b as non-invasive predictors for chronic kidney disease (CKD) in NAFLD patients.
Material and methods
In a case–control design, we included 40 NAFLD patients (20 NAFLD with CKD and 20 NAFLD without CKD) and 20 healthy controls. After clinical evaluation, laboratory assessments including liver test profile, renal function test, and quantification of microRNA-130b were done. Liver steatosis and stiffness were evaluated using HRI and ARFI.
Results
HRI and ARFI readings were significantly higher among NAFLD with CKD patients compared to other groups (P < 0.001). The median values of microRNA-130b were 32.1, 27.01, and 25.36 copies/µl in NAFLD with CKD, NAFLD without CKD, and healthy controls, respectively, with significant differences between groups (P < 0.05). ARFI values and HRI were positively correlated with microRNA-130b (P < 0.05). At a cutoff value > 28.13 copies/µl, microRNA-130b could differentiate between “NAFLD with CKD” and “NAFLD without CKD” patients with a sensitivity and specificity of 75% and 70%, respectively (AUC = 71.9%, P = 0.018).
Conclusions
Serum microRNA-130b, HRI, and ARFI are valuable noninvasive markers for the assessment of NAFLD. MicroRNA-130b is suggested as a sensitive biomarker for the prediction of CKD among NAFLD patients with good sensitivity and specificity.
Similar content being viewed by others


Introduction
Currently, non-alcoholic liver disease (NAFLD) is the most predominant chronic liver disorder worldwide [1]. NAFLD progression to fibrosis is affected by several factors including insulin resistance (IR), lipotoxicity, gut microbiota, oxidative stress, and genetic factors [2, 3]. Noninvasive diagnosis of NAFLD can be achieved by many tools, including the acoustic radiation force impulse (ARFI) which uses short-duration acoustic pulses, transient elastography (TE), and the hepatorenal index [4,5,6]. There is growing evidence that the synthesis and release of pro-inflammatory cytokines in NAFLD are connected to the development of chronic kidney disease (CKD) among NAFLD patients [7]. The prevalence of CKD in patients with NAFLD ~ 20–55%. The coexistence of NAFLD and CKD has a deleterious impact on outcomes, especially cardiovascular morbidity and mortality. So, the early recognition and screening for CKD in NAFLD patients are of clinical importance to allow for earlier introduction of relevant strategies [8].
Recently, microRNAs (miRNAs) have been of growing public interest [9]. A miRNA is a form of small, single-stranded RNA, 18–25 nucleotides, which is transcribed from DNA, instead of being translated into protein, and modulates the functions of other genes in protein synthesis [10]. MicroRNAs have been linked to manipulating vital renal functions. The progression of renal illnesses such as diabetic kidney disease (DKD), acute kidney injury, lupus nephritis, and polycystic kidney disease has been linked to changes in the expression of microRNAs. In addition, microRNAs have potential diagnostic and therapeutic targets. MicroRNA-21, miRNA-192, and miRNA-29 were found to be involved in the pathogenesis of DKD and could be employed as DKD biomarkers [11, 12]. We aimed to investigate microRNA 130b as a potential noninvasive biomarker for the early detection of CKD among NAFLD patients.
Subjects and methods
In a case–control design, we included 40 NAFLD patients (20 patients with CKD “group I” and 20 patients without CKD “group II”). An age- and sex-matched 20 healthy subjects were included in “group III.” Patients were recruited from the Internal Medicine Department, Faculty of Medicine, Alexandria University. The diagnosis of NAFLD was based on the evidence of hepatic steatosis by ultrasound (elevated hepatorenal echogenicity, vascular blurring of portal or hepatic veins) [4] and the absence of secondary factors hepatic fat accumulation (e.g., alcohol consumption, viral hepatitis, steatogenic drugs, or monogenic inherited disorders) [13].
The definition of CKD was based on either of the following presents for > 3 months [14]: (a) markers of kidney damage (one or more): [albuminuria (albumin excretion rate (AER) ≥ 30 mg/24 h or equivalent albumin-to-creatinine ratio (ACR) ≥ 30 mg/dl, urine sediment abnormalities such as isolated microscopic hematuria with dysmorphic red blood cells, red oval fat bodies or fatty casts, white blood cell casts, blood cell casts, granular casts or renal tubular epithelial cells], b) Glomerular filtration rate (GFR) < 60 ml/min/1.73 m2.
Exclusion criteria
We excluded patients with age > 50 years, diabetes mellitus, systemic hypertension, viral hepatitis C and/or B, autoimmune liver diseases, metabolic liver diseases, alcohol consumption, hepatocellular carcinoma or other malignancies, history of liver or kidney transplantation, known patients with CKD, or structural kidney abnormalities (e.g., severe renal cortical scarring, incidental large or numerous renal cysts or solid mass lesions) due to any other causes, hematological diseases, pregnancy, urinary tract disorders, and prostatic disorders (in men). Also, patients on nephrotoxic or steatogenic drugs (e.g., amiodarone, methotrexate, tamoxifen, corticosteroids, valproate) were not included. To avoid non-reliable ARFI measurements, patients with BMI > 30 kg/m2 were excluded [6].
All participants were subjected to history taking, physical examination, and anthropometric measure calculations. Complete hemogram, serum aspartate and alanine aminotransferases (AST and ALT), liver profile, lipid profile, fasting plasma glucose (FPG), glycated hemoglobin (HbA1c), serum creatinine, uric acid, and blood urea nitrogen, urine analysis, and urinary albumin creatinine ratio (uACR) were measured. Quantification of microRNA-130b expression using real-time quantitative reverse transcription PCR was done using miRNA easy Mini Kit (Qiagen, Germany) [15]. Acoustic radiation force impulse (ARFI) imaging and hepatorenal index (HRI) assessment via hepatic ultrasonography by a single experienced radiologist were done using a Siemens Acuson S2000 US System (Mochida Siemens Medical System, Tokyo, Japan) following the guidance on technique as described elsewhere. Caution was observed with placing the region of interest within the renal parenchyma while avoiding renal sinus fat, perinephric fat, and areas of artifacts [6, 16]. Hepatic steatosis was classified as mild (HRI of 1.05–1.24), moderate (HRI of 1.25–1.64), and severe (HRI > 1.65) [5].
Statistical analysis
Analysis was done by Statistical Package for Social Sciences (SPSS version 26.0) software. The normality of the data was evaluated. The data were expressed as mean ± SD, median (minimum–maximum), or proportions as appropriate. Student’s t-test or the Mann–Whitney U-test to compare means was used as appropriate. A comparison between proportions was determined by the chi-square (χ2) test or Fisher’s exact test (FET). ANOVA test with post hoc was used as appropriate. Correlation between different parameters in each group was done using Spearman correlation. The sensitivity and specificity of microRNA-130b were evaluated by receiver operating characteristic curve (ROC) analysis. Statistical significance was assessed at P ≤ 0.05. All calculated P-values were two-tailed.
Results
Demographic data
Age and sex showed no statistically significant difference in the different studied groups. The median values of BMI were 29.5 kg/m2, 28.0 kg/m2, and 24.6 kg/m2 for groups I, II, and III, respectively, with a statistical significance difference (P = 0.045). Table 1 shows the baseline clinico-laboratory data of the three study groups with their statistical significance.
Hepatorenal index (HRI)
The median values of HRI were 1.5, 1.3, and 1.02 in groups I, II, and III respectively. There was a statistically significant difference between groups I and II (P < 0.001), groups I and III (P < 0.001), and groups II and III (P = 0.002) as regards HRI readings (Table 2).
Acoustic radiofrequency impulse (ARFI)
The median value of ARFI was 2.97 m/s, 2.45 m/s, and 1.84 m/s in groups I, II, and III, respectively. There was a statistically significant difference between groups I and II (P = 0.002), between groups I and III (P < 0.001), and between groups II and III as regards ARFI (P < 0.001) (Table 2).
MicroRNA-130b
The median value of microRNA-130b was 32.1 copies/µl, 27.01 copies/µl, and 25.36 copies/µl in groups I, II, and III, respectively. There was a significant difference between groups I and II (P = 0.032), groups I and III (P < 0.001), and groups II and III (P = 0.045) as regards microRNA-130b levels (Table 2).
Correlation analysis
In the current study, a positive correlation was found between HRI and ARFI in NAFLD patients with CKD (P < 0.001). In addition, HRI positively correlated with microRNA-130b (P < 0.001). Moreover, ARFI showed also a positive correlation with microRNA-130b (P = 0.029). In NAFLD patients without CKD, ARFI positively correlated with microRNA-130b (P = 0.002) (Fig. 1a–c).

Correlations in group I. a Between HRI and ARFI readings. b Between HRI and microRNA-130b. c Between ARFI reading and microRNA-130b
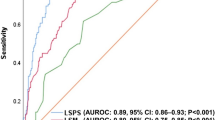
Diagnostic performance of microRNA-130b
By ROC analysis, microRNA-130b showed a significant diagnostic performance in the discrimination between patients (groups I + II) from control cases. At a cutoff value > 27.55 copies/µl, microRNA-130b could achieve this differentiation with a sensitivity of 60%, and a specificity of 85%, and with positive predictive value (PPV) and negative predictive value (NPV) of 88.9% and 51.5%, respectively (AUC = 78.3%, P < 0.001) (Fig. 2a).microRNA-130b showed a significant diagnostic performance in the discrimination between patients with “NAFLD with CKD” and patients with “NAFLD without CKD.” At a cutoff value > 28.13 copies/µl, microRNA-130b could achieve this differentiation with a sensitivity of 75%, and a specificity of 70%, and with PPV and NPV of 71.4% and 73.7%, respectively (AUC = 71.9%, P = 0.018) (Fig. 2b).

Diagnostic performance and ROC analysis of microRNA-130b in discrimination of different study groups. a All patients vs. healthy control. b Nonalcoholic fatty liver disease associated with chronic kidney disease vs. nonalcoholic fatty liver disease but without chronic kidney disease. c Nonalcoholic fatty liver disease without chronic kidney disease vs. healthy control
In addition, microRNA-130b has a significant diagnostic performance to discriminate between “NAFLD without CKD” patients from the control group. At a cutoff value > 24.81 copies/µl, microRNA-130b had a sensitivity, specificity, PPV, and NPV of 75%, 60%, 65.2%, and 70.6%, respectively (AUC = 70.6%, P = 0.026) (Fig. 2c).
Discussion
Currently, NAFLD represents the upcoming epidemic of chronic liver disease worldwide after the elimination of the hepatitis C virus [1]. There is growing evidence that the synthesis and release of pro-inflammatory cytokines in NAFLD are connected to the development of CKD among NAFLD patients [7].
Recently, microRNAs have been linked to the manipulation of vital renal functions. The progression of renal illnesses such as DKD, acute kidney injury, lupus nephritis, and polycystic kidney disease has been linked to changes in the expression of microRNAs. In addition, microRNAs have potential diagnostic and therapeutic targets [12, 13].
Our obtained results showed a significant difference between study groups as regards the HRI values. The same results apply to ARFI readings also. The hepatorenal index is considered a valid tool for detecting and grading fatty liver disorders in the previous report, and its utility for diagnosis and grading of liver steatosis has been studied. In addition, ARFI has been studied as a non-invasive tool for the assessment of liver steatosis in NAFLD [11, 17,18,19,20].
MicroRNA-130b is anticipated to be convoluted in pathophysiological procedures such as oxidative stress and insulin resistance which is the main underlying pathophysiological mechanism in NAFLD [12].
In our study, there microRNA-130b showed arithmetical variance in NAFLD patients with CKD than those without CKD (P = 0.032), also showed arithmetical variance between NAFLD patients with CKD and control, and between NAFLD patients and control (P < 0.001 and P = 0.045) respectively.
MicroRNA-130b downregulation has been linked to a reduction of lipid storage in hepatocytes and improving insulin sensitivity in rat models. miR-130b-5p repression was found to decrease fat accumulation through insulin-like growth factor binding protein 2 (IGFBP2) upregulation in NAFLD murine models [21]. Growing evidence revealed that miR-130b is upregulated in a variety of diseases. For example, hepatocellular carcinoma tissues showed high expression of microRNA-130b compared to nearby cirrhotic nonmalignant liver tissues [22]. In addition, microRNA-130b has been linked to tumor cell initiation, growth, and apoptosis regulation [23]. These findings explain the higher levels of microRNA-130b among NAFLD patients compared to healthy control and represent a novel insight into the pathogenesis of NAFLD.
In our study, NAFLD patients with CKD had significantly higher levels of microRNA-130b compared to NAFLD without CKD and healthy subjects. In addition, microRNA-130b could discriminate patients with NAFLD and CKD from patients with NAFLD only with high sensitivity and specificity. This highlights the possible link and role of microRNA-130b in the development of CKD among NAFLD patients.
In recent years, a link between NAFLD and CKD has been established, irrespective of the existence of potential confounding disorders such as obesity, hypertension, and type 2 diabetes [24, 25].microRNA-130b has been linked to the development of CKD. Its level is upregulated in patients with early lupus nephritis and is positively correlated with renal damage and chronicity index. The increased expression of microRNA-130b has been associated with overexpression of α-smooth muscle actin and reduced expression of E-cadherin in the presence of transforming growth factor-β1 (TGFBR1). This was hypothesized to promote epithelial-mesenchymal transition, favoring renal tubular fibrosis [26, 27]. In addition, the link of miRNA-130 to TGFBR1 and TGFBR2 is of special importance as it may influence the fibrosis progression in NAFLD and may explain the pathogenesis of CKD in NAFLD patients, a point of potential therapeutic implication in the future [28].
On the other hand, contradictory data about the role of microRNA-130b in renal tubular function manipulation have been elucidated. Bai and colleagues (2016) found that microRNA-130b downregulation was associated with high serum creatinine and β2-microglobulin and with high Snail expression leading to increased tubulointerstitial fibrosis in diabetic nephropathy. However, this contradiction in results may be attributed to the presence of diabetes among their cohort. This concludes the role of microRNA-130b in the manipulation of renal tubular function is not fully clear and opens the way for more studies [29].
We admit that our study has some limitations. The small sample size is one of these limitations, but the financial aspect of the higher number was a conflicting obstacle. We did not use liver biopsy in our diagnosis of NAFLD. This was due to its invasive nature and the resistance of NAFLD patients to such invasive maneuvers. In conclusion, the positive correlation between ARFI, HRI, and serum microRNA-130b, together with good diagnostic performance of microRNA-130b in discrimination of NAFLD patients with and without CKD, introduces these parameters as new non-invasive biomarkers for assessment of NAFLD and to predict chronic kidney disease, and we recommend further wide-scale evaluation of their utility in clinical practice.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the article.
References
Angulo P (2002) Nonalcoholic fatty liver disease. N Engl J Med 346(16):1221–1231
Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, Charlton M, Sanyal AJ (2012) The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 55(6):2005–2023
Starley BQ, Calcagno CJ, Harrison SA (2010) Nonalcoholic fatty liver disease and hepatocellular carcinoma: a weighty connection. Hepatology 51(5):1820–1832
Schwenzer NF, Springer F, Schraml C, Stefan N, Machann J, Schick F (2009) Non-invasive assessment and quantification of liver steatosis by ultrasound computed tomography and magnetic resonance. J Hepatol 51(3):433–445
Wong VWS, Vergniol J, Wong GLH, Foucher J, Chan HLY, Le Bail B, Choi PCL, Kowo M, Chan AWH, Merrouche W, Sung JJY, de Lédinghen V (2009) Diagnosis of fibrosis and cirrhosis using liver stiffness measurement in nonalcoholic fatty liver disease. Hepatology 51(2):454–462
Lupsor M, Badea R, Stefanescu H, Sparchez Z, Branda H, Serban A, Maniu A (2009) Performance of a new elastographic method (ARFI technology) compared to unidimensional transient elastography in the noninvasive assessment of chronic hepatitis C Preliminary results. J Gastrointestin Liver Dis 18(3):303–310
Musso G, Gambino R, Tabibian JH, Ekstedt M, Kechagias S, Hamaguchi M, Hultcrantz R, Hagström H, Yoon SK, Charatcharoenwitthaya P, George J, Barrera F, Hafliðadóttir S, Björnsson ES, Armstrong MJ, Hopkins LJ, Gao X, Francque S, Verrijken A, Cassader M (2014) Association of non-alcoholic fatty liver disease with chronic kidney disease: a systematic review and meta-analysis. PLoS Med 11(7):e1001680
Cheung A, Ahmed A (2021) Non-alcoholic fatty liver disease and chronic kidney disease: a review of links and risks. Clin Exp Gastroenterol 17(14):457–465. https://doi.org/10.2147/CEG.S226130. PMID:34819740;PMCID:PMC8607580
Cermelli S, Ruggieri A, Marrero JA, Ioannou GN, Beretta L (2011) Circulating MicroRNAs in patients with chronic hepatitis C and non-alcoholic fatty liver disease. PLoS One 6(8):e23937
Ying SY, Chang DC, Lin SL (2007) The MicroRNA (miRNA): overview of the RNA genes that modulate gene function. Mol Biotechnol 38(3):257–268
Bhatt K, Kato M, Natarajan R (2016) Mini-review: emerging roles of microRNAs in the pathophysiology of renal diseases. Am J Physiol Renal Physiol 310(2):F109–F118
Chien HY, Chen CY, Chiu YH, Lin YC, Li WC (2016) Differential microRNA profiles predict diabetic nephropathy progression in Taiwan. Int J Med Sci 13(6):457–465
Chalasani N, Younossi Z, Lavine JE, Charlton M, Cusi K, Rinella M, Harrison SA, Brunt EM, Sanyal AJ (2017) The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology 67(1):328–357
Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, Zeeuw DD, Hostetter TH, Lameire N, Eknoyan G (2005) Definition and classification of chronic kidney disease: a position statement from kidney disease: Improving Global Outcomes (KDIGO). Kidney Int 67(6):2089–2100
Yamada H, Suzuki K, Ichino N, Ando Y, Sawada A, Osakabe K, Sugimoto K, Ohashi K, Teradaira R, Inoue T, Hamajima N, Hashimoto S (2013) Associations between circulating microRNAs (miR-21, miR-34a, miR-122 and miR-451) and non-alcoholic fatty liver. Clin Chim Acta 424:99–103
Chauhan A, Sultan LR, Furth EE, Jones LP, Khungar V, Sehgal CM (2016) Diagnostic accuracy of hepatorenal index in the detection and grading of hepatic steatosis. J Clin Ultrasound 44(9):580–586. https://doi.org/10.1002/jcu.22382
Kramer H, Pickhardt PJ, Kliewer MA, Hernando D, Chen GH, Zagzebski JA, Reeder SB (2017) Accuracy of liver fat quantification with advanced CT, MRI, and ultrasound techniques: prospective comparison with MR spectroscopy. Am J Roentgenol 208(1):92–100
Liu H, Fu J, Hong R, Liu L, Li F (2015) Acoustic radiation force impulse elastography for the non-invasive evaluation of hepatic fibrosis in non-alcoholic fatty liver disease patients: a systematic review & meta-analysis. PLoS One 10(7):e0127782
Piazzolla VA, Mangia A (2020) Noninvasive diagnosis of NAFLD and NASH. Cells 9(4):1005. https://doi.org/10.3390/cells9041005
Isaksen VT, Larsen MA, Goll R, Florholmen JR, Paulssen EJ (2016) Hepatic steatosis, detected by hepatorenal index in ultrasonography, as a predictor of insulin resistance in obese subjects. BMC Obes 3(1):39
Liu X, Chen S, Zhang L (2020) Downregulated microRNA-130b-5p prevents lipid accumulation and insulin resistance in a murine model of nonalcoholic fatty liver disease. Am J Physiol Endocrinol Metab 319(1):E34–E42
Liu AM, Yao TJ, Wang W, Wong KF, Lee NP, Fan ST, Poon RTP, Gao C, Luk JM (2012) Circulating miR-15b and miR-130b in serum as potential markers for detecting hepatocellular carcinoma: a retrospective cohort study. BMJ Open 2(2):e000825
Ma S, Tang KH, Chan YP, Lee TK, Kwan PS, Castilho A, Ng I, Man K, Wong N, To KF, Zheng BJ, Lai PB, Lo CM, Chan KW, Guan XY (2010) miR-130b promotes CD133+ liver tumor-initiating cell growth and self-renewal via tumor protein 53-induced nuclear protein 1. Cell Stem Cell 7(6):694–707
Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C (2016) Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol 65(3):589–600
Nagy J, Kovács T (2019) A brief review on the rising incidence of chronic kidney diseases and non-alcoholic fatty liver disease. Physiol Int 106(4):305–310
Wang W, Mou S, Wang L, Zhang M, Shao X, Fang W, Lu R, Qi C, Fan Z, Cao Q, Wang Q, Fang Y, Ni Z (2015) Up-regulation of serum MiR-130b-3p level is associated with renal damage in early lupus nephritis. Sci Rep 5(1):12644
Colangelo T, Fucci A, Votino C, Sabatino L, Pancione M, Laudanna C, Binaschi M, Bigioni M, Alberto Maggi C, Parente D, Forte N, Colantuoni V (2013) MicroRNA-130b promotes tumor development and is associated with poor prognosis in colorectal cancer. Neoplasia 15(9):1086–1099
Fang Z, Dou G, Wang L (2021) MicroRNAs in the pathogenesis of nonalcoholic fatty liver disease. Int J Biol Sci 17(7):1851–1863. https://doi.org/10.7150/ijbs.59588. PMID:33994867;PMCID:PMC8120467
Bai X, Geng J, Zhou Z, Tian J, Li X (2016) MicroRNA-130b improves renal tubulointerstitial fibrosis via repression of Snail-induced epithelial-mesenchymal transition in diabetic nephropathy. Sci Rep 6(1):20475
Acknowledgements
Not applicable
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
ME, study concept and design; ASE and MT, study concept; EEH, clinical examination and cases enrollment; ARFI, examination, data collection, and first draft; SAL, study design; ARFI, examination; and HRI, calculation and first draft. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This work was carried out following the Declaration of Helsinki for experiments 1975 and its later amendments. The study protocol was approved by the ethical committee of the Faculty of Medicine, Alexandria University, number 0201088. All patients signed a written informed consent before inclusion in the study.
Consent for publication
The authors declare that they consent to the publication of this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hassafy, M.Y.E., Elhadidi, A.S., Tahoon, M.M. et al. Liver stiffness, hepatorenal index, and microRNA-130b as predictors for chronic kidney disease in patients with non-alcoholic fatty liver disease. Egypt Liver Journal 13, 37 (2023). https://doi.org/10.1186/s43066-023-00269-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-023-00269-5