
Abstract
Background
Incidence of malignancy in architectural distortion (AD) is variable, and as a standard of care, all the architectural distortions are biopsied. It is important to identify benign and malignant characteristics of ADs on imaging to predict the probability of malignancies as well as to establish radiological–pathological concordance. The aim of our study was to analyse the utility of contrast-enhanced mammography (CEM) in primary AD, to describe and evaluate the accuracy of CEM parameters and derive a novel scoring system to differentiate benign and malignant AD.
Results
Forty-six patients with 49 ADs were evaluated with a median age, 51 years (age range—34–72 years) and all were women. Of the 49 ADs, 65.3% (32/49) were benign, and 34.69% (17/49) were malignant. The CEM parameters which predicted malignancy were moderate or marked density, size > 0.95 cm, CT ratio > 1.31, mass morphology and washout kinetics. The absence of enhancement and enhancing AD with AD score of 0 had a 100% NPV for malignancy. Enhancing architectural distortion with a score of 3 or more had 100% PPV for malignancy. A score of 1 or 2 was indeterminate, and an individualised decision was recommended.
Conclusions
In primary AD, several CEM features have significantly predicted malignancy when the score is 3 and above. A biopsy may be avoided in non-enhancing AD and enhancing AD with a score of 0 due to high NPV.
Key points
-
1.
Incidence of malignancy in architectural distortion is variable and all are biopsied.
-
2.
Contrast-enhanced mammography parameters and architectural distortion score helps to differentiate benign and malignant causes.
-
3.
Biopsy can be avoided in non-enhancing architectural distortion and surgery should be advised when score is 3 and above even with benign histopathology results.
Similar content being viewed by others


Background
Architectural distortion (AD) is defined as “thin straight lines or spiculations radiating from a point, and focal retraction, distortion or straightening of the anterior or posterior edge of the parenchyma”, according to the American College of Radiology—Breast Imaging Reporting And Data System (ACR-BIRADS) atlas [1].
AD can be primary or secondary to an infection, trauma, or breast interventions. The differential diagnosis for primary AD includes fibrocystic disease, radial scar, complex sclerosing lesion, stromal sclerosis, high-risk lesions and in situ or invasive malignancy [2].
Primary AD is associated with malignancy in 23.7% to 74.5% of patients [3,4,5,6,7]; hence, all architectural distortions are biopsied. With the widespread availability of Digital Breast Tomosynthesis (DBT), more AD is detected with a low rate of malignancy [5]. Hence, it is essential to characterise AD further. Also, it is crucial to establish radiological–pathological concordance after the biopsy results to decide on the lesions’ excision [6].
So far, several studies have evaluated the usefulness of various imaging modalities, including digital breast tomosynthesis (DBT), ultrasonography (USG) and magnetic resonance imaging (MRI) to differentiate benign and malignant architectural distortions [5, 6, 8,9,10,11].
DBT and USG are not accurate enough to predict or exclude malignancy in architectural distortions. MRI is useful in ruling out malignancy in AD because of its high negative predictive value when they do not enhance [7, 12, 13]. But MRI has several limitations, such as availability, duration of the study and high cost.
Contrast-enhanced mammography (CEM) uses the same principle of MRI, i.e. neo angiogenesis in detecting malignancies [14]. However, compared to MRI, CEM is easy to implement in clinical practice, has relatively low cost and acts as a quick one-stop solution [14]. To the best of our knowledge, there are only two published studies evaluating the role of CEM in AD, and both showed promising results [15, 16].
In this study, we aimed to evaluate the utility of CEM in predicting malignancy in primary AD, described and assessed certain CEM parameters. We also derived a scoring system attempting to differentiate benign and malignant causes of AD.
Methods
This is a retrospective observational study approved by our institutional review board. The need for informed consent was waived.
The search of the radiological database from 1 April 2021 to 31 January 2023 identified 212 architectural distortions in 203 patients. Of these, 155 were excluded as they were AD secondary to surgery or trauma. Eight more patients were excluded because either CEM or biopsy was not done, leaving 49 architectural distortions in 46 female patients as the cohort as shown in Fig. 1.

Patient flow
When architectural distortions were detected in digital breast tomosynthesis (DBT) with synthesised 2D images, as an institutional protocol, we performed 2D contrast-enhanced mammography for further characterisation of these lesions after obtaining informed consent.
All the studies were performed using the 3Dimensions Mammography System (Hologic). The contrast dose was 1.5 ml/kg of iodinated contrast media (Iohexol 350 mg, OMNIPAQUE, GE healthcare). The contrast was injected intravenously at a rate of 3 ml/sec. After 2 min of contrast injection, low- and high-energy images of CC and MLO views of both breasts were obtained within a 6-min window period. No adverse events were noted while performing CEM in the study population.
All patients underwent a biopsy on the same day with either a 14G core or 10G vacuum-assisted biopsy (VAB) using mammography guidance or USG when localised on ultrasound. One patient in the study population had undergone an excision biopsy after wire localisation as an USG correlate was not identified, and a mammographic biopsy could not be performed due to the posterior location of AD.
The following features were evaluated retrospectively by three different readers—Dr RR, Dr.PS and Dr SP with more than 15 years, 6 years and three years of experience in breast imaging, respectively. The consensus opinion was the agreement of at least two of three breast radiologists. All the three radiologists read in the order of synthesised 2D images, tomo images and recombined images in the same sitting for interpretation. The low-energy images were not used for interpretation.
The readers were blinded to the histopathology, and the CEM features were categorised as follows:
-
1.
Detection of architectural distortion—in 3D or both in 2D and 3D
-
2.
Characteristics of AD in CEM:
-
1.
Presence or absence of enhancement.
-
2.
The density of enhancement in the first (CC) view—categorised as no enhancement, mild, moderate and marked enhancements using imaging reference standards from our patients (Fig. 2).
-
3.
The longest dimension of the AD on CEM.
-
4.
The longest dimension of the architectural distortion on recombined image and tomosynthesis images is calculated. The ratio between the longest dimension of AD in recombined and tomosynthesis images was calculated, and it is described as contrast/tomo ratio (C/T ratio).
-
5.
Morphology of enhancement: mass or non-mass enhancement.
-
6.
Relative change in density of enhancement in the first (CC) and second (MLO) views was divided into three categories (similar to kinetic information in MRI): 1. Increase in density 2. No change in density 3. Decrease in density.
-
1.

Imaging reference standards for assigning density of enhancement. Architectural distortions are marked by white arrows in a–d. a no enhancement. b Minimal enhancement. c Moderate enhancement. d Marked enhancement
For all the architectural distortions which showed enhancement, a scoring system was developed to increase diagnostic accuracy and remove subjective variability among radiologists. Enhancing architectural distortions were assigned a score of either 0 or 1 based on the imaging findings on each CEM parameter described above (Fig. 3 and Table 1). The moderate and marked density of enhancement was grouped for scoring and was assigned a score of 1 for statistical analysis. Similarly, for relative change in density, the increase and no change in density were grouped and were assigned a score of 0 for statistical analysis. The minimum and maximum scores would be 0 and 5, respectively.

Schematic diagram showing benign and malignant CEM characteristics of architectural distortion
Pathological results were analysed, and the lesions were categorised into benign, malignant and high-risk lesions (atypical ductal hyperplasia, atypical lobular hyperplasia and lobular carcinoma in situ). All high-risk lesions in core needle biopsy underwent surgical excision. When they were upgraded to invasive carcinoma or ductal carcinoma in situ after surgical excision, they were classified as malignant lesions. High-risk lesions after surgical excision that were not upgraded were classified as benign for statistical purposes. Malignant lesions were considered true positives for analysis.
Statistical analysis
Receiver operating characteristic curve (ROC) analysis and Youden index were performed for enhancement size and contrast/tomo ratio of AD to determine the optimal cut-off value for maximising specificity and sensitivity.
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and diagnostic accuracy of CEM were calculated in the AD evaluation using these six parameters, considering histopathologically proven malignant lesions as true positives.
The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and diagnostic accuracy of AD scores in predicting malignant architectural distortions were calculated.
Results
Forty-six patients with 49 ADs were evaluated with a median age, 51 years (age range—34–72 years) and all were women.
Of the 49 architectural distortions, 40 (81.63%) showed enhancement, and nine (18.36%) did not. Of the 49 ADs, 65.3% (32/49) were benign, and 34.69% (17/49) were malignant. Table 2 shows the basic demographics of study population.
38.8% (19/49) of AD were seen both in 2D and DBT. Out of 19 ADs that were seen in both 2D and DBT images, 63.2% (12/19) were malignant and only 36.8% (7/19) were benign. When the AD was seen in both 2D and 3D, they were more likely malignant. 61.2% (30/49) of the AD were detected in DBT only, out of which 83.33% (25/30) were benign and 16.67% (5/30) were malignant. AD detection only by DBT is significantly associated with benign histopathology with a P value of < 0.05.
Out of five malignant architectural distortions detected only by DBT, 40% (2/5) were invasive lobular carcinomas and 60% (3/5) were invasive ductal carcinomas. Out of 12 malignant architectural distortions detected by 2D plus DBT, 66.67% (8/12) were invasive ductal carcinomas, 16.67% (2/12) were ductal carcinoma in situ, 8.33% (1/12) was a tubular carcinoma, and only 8.33% (1/12) was invasive lobular carcinoma.
From the ROC analysis, a cut-off ratio of 1.31 and a size of 0.95 cm was derived for differentiating between benign and malignant lesions.
Our study found that AD, which showed no or mild enhancement and non-mass morphology with an enhancement size of ≤ 0.95 cm and C/T ratio of ≤ 1.31 in recombined images, was more likely to be benign. Architectural distortions, seen as moderate or marked density-enhancing masses with an enhancement size > 0.95 cm and a C/T ratio of > 1.31 in recombined images, were highly suspicious of malignancy. The sensitivity, specificity, positive predictive value and negative predictive value of each parameter are listed in Table 3.
The absence of enhancement had a 100% NPV for malignancy in our study (Fig. 4) (9/49). All nine lesions that did not enhance in CEM were proven benign on histopathology. All the AD which showed a decrease in density on delayed recombined image akin to early washout was malignant (PPV—100%).

a–c a Spot tomosynthesis image shows an architectural distortion in the upper central quadrant of the left breast (white arrow). On post-contrast recombined images b and c there was no enhancement of the architectural distortion. On histopathology, it was proven to be sclerosing adenosis and is concordant
The distribution of benign and malignant histopathology for all the enhancing AD based on the score is shown in Figs. 5, 6, 7, 8 and Table 4.

Distribution of benign and malignant histopathology based on the AD score

a–e CEM features of a benign AD (marked by white arrows in a–c). a Tomosynthesis image shows an architectural distortion in the inner quadrant of the left breast. Post-contrast recombined CC (early, b) and MLO (delayed, c) images show heterogeneous focal non-mass enhancement in the area of architectural distortion. The density of enhancement is mild, enhancing size is 0.7 cm (< 0.95), contrast/tomo ratio is 1.2 (< 1.31) (d and e), and there is relative increase in density in delayed phase compared to early phase. The architectural distortion score is 0. Final histopathology was radial scar which is concordant

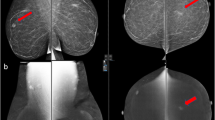
a–e CEM features of a malignant AD (Marked by white arrows in a–c). a Spot tomosynthesis image shows an architectural distortion in the upper quadrant of the right breast. Post-contrast recombined CC (early, b) and MLO (delayed, c) images show heterogeneously enhancing irregular mass in the area of architectural distortion. The density of enhancement is marked, enhancing size is 1.72 cm (> 0.95), contrast/tomo ratio is 2.1 (> 1.31) (d and e) and there is relative decrease in density in delayed phase compared to early phase. The architectural distortion score is 5. Final histopathology was invasive ductal carcinoma and is concordant

a–e CEM features of a malignant AD (Marked by white arrows in a–c). a Spot tomosynthesis image shows an architectural distortion in the upper outer quadrant of the right breast. Post-contrast recombined CC (early) and MLO (delayed) images b and c show non-mass enhancement in the area of architectural distortion. The density of enhancement is marked, enhancing size is 1.81 cm (> 0.95), contrast/tomo ratio is 1.5 (> 1.31) d and e and there is relative decrease in density in delayed phase compared to early phase. The architectural distortion score is 4. Biopsy from the AD was suggestive of benign proliferative breast disease which was considered discordant and she was referred for surgical excision. Final histopathology was suggestive of invasive lobular carcinoma, lobular carcinoma in situ, atypical lobular hyperplasia, sclerosing adenosis and intraductal papillomatosis
The receiver operating characteristic (ROC) curve showed high diagnostic accuracy for architectural distortion scores in predicting malignancy with an area under the curve of 0.959 (Fig. 9).

Receiver operating characteristic (ROC) curve for predicting malignancies in architectural distortion using architectural distortion score with area under the curve of 0.959
The accuracy of CEM in predicting malignant AD was independent of detection by only tomosynthesis or 2D plus tomosynthesis (mean score of 3.8 for only tomosynthesis detected ADs and 3.5 for 2D plus tomosynthesis).
Discussion
In this study, we evaluated the utility of CEM in predicting malignancy in primary AD. We have attempted to describe certain CEM parameters which helped to differentiate benign and malignant aetiology with a novel scoring system.
In our study, the incidence of malignancy in primary AD was 34.69% (17/49), well within the range reported in the previous literature [3,4,5,6,7].
Our study proved that non-enhancing AD had a 100% negative predictive value for malignancy.
The study by Goh et al. [15] in 2021 showed that the absence of enhancement in ADs had 100% negative predictive value for malignancy. A study by Patel et al. [16] in 2017 evaluated the role of CEM in predicting malignancy in 49 architectural distortions. In their research, all except one architectural distortion which did not enhance were benign. One malignant AD thought to have no enhancement was in the background of marked BPE.
We described five CEM parameters to differentiate benign and malignant AD. Among them, three were described first in the literature and were C/T ratio, enhancing morphology and relative change in density.
We found that when AD showed no or mild enhancement, non-mass morphology with an enhancement size of ≤ 0.95 cm and C/T ratio of ≤ 1.31 in recombined images, they were more likely to be benign. Architectural distortions, seen as moderate or marked density-enhancing masses with an enhancement size > 0.95 cm and a C/T ratio of > 1.31 in recombined images, were highly suspicious of malignancy.
A study by Goh et al. [15] in 2021, in addition to the presence or absence of enhancement, also studied several CEM features such as degree enhancement of AD, enhancing morphology (enhancement as foci versus mass and non-mass enhancement), size of enhancement with the size cut-off and enhancing spiculations. Factors showing significant association with malignancy in their study were marked intensity of enhancement and presence of enhancing spiculations.
The three new CEM parameters we have described in this study also had high diagnostic accuracy. When the C/T ratio is > 1.31, the sensitivity, specificity, PPV and NPV in predicting malignancy were 76.5%, 87%, 81.3% and 83.3%, respectively. When AD presents as a mass rather than a non-mass enhancement in recombined images, the sensitivity, specificity, PPV and NPV in predicting malignancy were 76.5%, 91.3%, 86.7% and 84%, respectively.
If the AD shows washout in the delayed image, which was subjectively assessed by comparing the density of enhancement in CC (early) and MLO (delayed) views, it is more likely to be malignant. This had 100% positive predictive value. This parameter is identical to the washout kinetics in MRI [17].
Using this simple, reproducible and novel scoring system based on CEM parameters of AD described in this study, we can differentiate benign and malignant ADs. ADs with a score of 0 had a 100% negative predictive value for malignancy, similar to non-enhancing AD. Hence, a benign biopsy report is considered concordant, and the patient can be safely followed up. In future, a biopsy may be avoided entirely. When the AD scored three or more using the described CEM parameters, it was always malignant. A benign biopsy report for a score of 3 and above should be considered discordant, and further surgical excision is recommended to exclude malignancy.
The score of 1 and 2 could be considered a grey zone because the benign and the malignant causes overlap.
Limitations
The study has a few limitations. Firstly, it was a retrospective single-centre study with a limited sample size, but our results were consistent with other retrospective studies. Secondly, inter-reader agreement was not checked for the described CEM parameters. Lastly, as the study aimed to study the utility of CEM, comparison with other modalities like MRI was not evaluated.
Conclusions
In primary architectural distortion, several CEM features were significantly associated with final pathology, the scoring system appears to be promising and may help to recommend appropriate management. There may be a paradigm shift in the imaging and management recommendations of AD with the use of CEM in future.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available to maintain the anonymity but are available from the corresponding author on reasonable request.
Abbreviations
- CEM:
-
Contrast-enhanced mammography
- AD:
-
Architectural distortion
- PP:
-
Positive predictive value
- NP:
-
Negative predictive value
- C:
-
Craniocaudal
- MLO:
-
Mediolateral oblique
- MRI:
-
Magnetic resonance imaging
- C/T Ratio:
-
Contrast/tomosynthesis ratio
- ROC:
-
Receiver operating characteristic curve
- VAB:
-
Vacuum-assisted biopsy
- DBT:
-
Digital breast tomosynthesis
- USG:
-
Ultrasonogram
- ACR:
-
American College of Radiology
- BIRADS:
-
Breast imaging reporting and data system
References
D’Orsi CJ (2013) ACR BI-RADS breast imaging and reporting data system breast imaging atlas, 5th edn. American College of Radiology, Reston
Gaur S, Dialani V, Slanetz PJ, Eisenberg RL (2013) Architectural distortion of the breast. AJR Am J Roentgenol 201(5):W662–W670. https://doi.org/10.2214/AJR.12.10153
Venkatesan A, Chu P, Kerlikowske K, Sickles EA, Smith-Bindman R (2009) Positive predictive value of specific mammographic findings according to reader and patient variables. Radiology 250:648–657
Bahl M, Baker JA, Kinsey EN, Ghate SV (2015) Architectural distortion on mammography: correlation with pathologic outcomes and predictors of malignancy. AJR 205:1339–1345
Bahl M, Lamb LR, Lehman CD (2017) Pathologic outcomes of architectural distortion on digital 2D versus tomosynthesis mammography. AJR Am J Roentgenol 209(5):1162–1167. https://doi.org/10.2214/AJR.17.17979
Durand MA, Wang S, Hooley RJ, Raghu M, Philpotts LE (2016) Tomosynthesis-detected architectural distortion: management algorithm with radiologic-pathologic correlation. Radiographics 36(2):311–321. https://doi.org/10.1148/rg.2016150093
Mei H, Xu J, Yao G, Wang Y (2020) The diagnostic value of MRI for architectural distortion is categorised as BI-RADS category 3–4 by mammography. Gland Surg 9(4):1008–1018. https://doi.org/10.21037/gs-20-505.PMID:32953609;PMCID:PMC7475343
Alshafeiy TI, Nguyen JV, Rochman CM, Nicholson BT, Patrie JT, Harvey JA (2018) Outcome of architectural distortion detected only at breast Tomosynthesis versus 2D mammography. Radiology 288(1):38–46. https://doi.org/10.1148/radiol.2018171159
Pujara AC, Hui J, Wang LC (2019) Architectural distortion in the era of digital breast tomosynthesis: outcomes and implications for management. Clin Imaging 54:133–137. https://doi.org/10.1016/j.clinimag.2019.01.004
Vijapura C, Yang L, **ong J, Fajardo LL (2018) Imaging features of nonmalignant and malignant architectural distortion detected by tomosynthesis. AJR Am J Roentgenol 211(6):1397–1404. https://doi.org/10.2214/AJR.18.19658
Si L, Zhai R, Liu X, Yang K, Wang L, Jiang T (2016) MRI in the differential diagnosis of primary architectural distortion detected by mammography. Diagn Interv Radiol 22(2):141–150. https://doi.org/10.5152/dir.2016.15017
Giess CS, Chikarmane SA, Sippo DA, Birdwell RL (2017) Clinical utility of breast MRI in the diagnosis of malignancy after inconclusive or equivocal mammographic diagnostic evaluation. AJR Am J Roentgenol 208(6):1378–1385. https://doi.org/10.2214/AJR.16.16751
Ferre R, Kuzmiak CM (2022) Meta-analysis: architectural distortion and breast MRI. Breast Dis 41(1):205–214. https://doi.org/10.3233/BD-210045
Jochelson MS, Lobbes MBI (2021) Contrast-enhanced mammography: state of the art. Radiology 299(1):36–48. https://doi.org/10.1148/radiol.2021201948
Goh Y, Chan CW, Pillay P et al (2021) Architecture distortion score (ADS) in malignancy risk stratification of architecture distortion on contrast-enhanced digital mammography. Eur Radiol. 31(5):2657–2666. https://doi.org/10.1007/s00330-020-07395-3
Patel BK, Naylor ME, Kosiorek HE et al (2017) Clinical utility of contrast-enhanced spectral mammography as an adjunct for tomosynthesis-detected architectural distortion. Clin Imaging. 46:44–52. https://doi.org/10.1016/j.clinimag.2017.07.003
Subramaniam P, Renganathan R, Suganya P et al (2023) Diagnostic accuracy of subjective kinetic assessment of masses in contrast-enhanced mammography in comparison with contrast-enhanced magnetic resonance imaging. Egypt J Radiol Nucl Med 54:89. https://doi.org/10.1186/s43055-023-01039-4
Acknowledgements
Not applicable.
Funding
No funding was required for the study.
Author information
Authors and Affiliations
Contributions
All the authors have contributed in conceptualising and designing the study, retrieval, analysis and interpretation of data. All authors of this paper have read and approved the final version submitted. The contents of this manuscript have not been copyrighted or published previously. The contents of this manuscript are not now under consideration for publication elsewhere. The contents of this manuscript will not be copyrighted, submitted, or published elsewhere, while acceptance by the Journal is under consideration. There are no directly related manuscripts or abstracts, published or unpublished, by any authors of this paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was taken from the institutional KMCH ethics committee, Kovai Medical Centre and Hospital limited, (EC/AP/1001/02/2023). As ours is a retrospective observational study, informed consent was waived off by the review board of Kovai Medical Centre and Hospital limited.
Consent for publication
We have used images maintaining the anonymity of the participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Renganathan, R., Subramaniam, P., Mandal, A. et al. Novel scoring system using contrast-enhanced mammography to differentiate benign and malignant architectural distortion. Egypt J Radiol Nucl Med 54, 193 (2023). https://doi.org/10.1186/s43055-023-01132-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01132-8