
Abstract
Background
Dietary components can influence the effects of genetic background in breast cancer (BC). This review study aimed to investigate the effect of dietary components on the expression level of BC-related genes.
Methods
In this narrative review, Embase, PubMed, PsycInfo, and the Cochrane databases were used to collect the related papers with interactions of BC, genetics, and dietary intake. Appropriate keywords such as BC, gene expression, mutation, nutrient, and diet (alone and together) were applied for data collection.
Results
The association of BC with some genes including the BC1 gene (BRCA1), the human epidermal growth factor receptor 2 (HER2), and the fat mass and obesity-associated (FTO) gene can be affected by dietary components. Moderate B12 supplementation may be protective against BC in people with the inherited mutation of BRCA. The olive oil may have a protective effect against BC through several mechanisms such as suppressing HER-2 expression. Furthermore, high glycemic index foods may increase the risk of BC by the activation of the phosphoinositide 3-kinase/protein kinase B (PI3K/AKT) pathway and the up-regulation of FTO gene expression.
Conclusion
There are interactions between BC, BC-related genes, and dietary intake. Dietary components such as macronutrients, micronutrients, and phytochemicals may regulate the expression level of BC-related genes. Further longitudinal studies are needed to confirm the associations between BC-related genes and diet and to discover the underlying mechanisms.
Similar content being viewed by others


Introduction
Breast cancer (BC) is one of the main health challenges worldwide [1, 2] and is considered the most prevalent type of malignancy [3,4,5] and the second cause of cancer-related mortality in women [4, 6]. Annually, there are about 14 million diagnosed BC cases and 8 million cancer-related deaths around the world [7]. However, developed countries are more prone to BC and cancer-related deaths, which are likely to be due to an unhealthy environment and lifestyle [8]. Thus, comprehensive preventive approaches are needed to suppress these predisposing factors [9]. Generally, the etiology of BC is highly complex [4, 10] and refers to multifactorial causes, which can be genetic non-modifiable factors, non-genetic non-modifiable factors (e.g., age, race, menstrual/menopausal age, breast characteristics, and reproductive factors), and non-genetic modifiable factors (e.g., lifestyle) [2, 8].
Some genes were reported to have crucial roles in the development of BC. For example, BRCA1 (breast cancer type 1) is a tumor suppressor gene in humans [11] that plays a key role in deoxyribonucleic acid (DNA) repair [12]. BRCA1 mutations exist in nearly 2% of BC patients [8] and increase the risk of mortality in their carriers compared to the others [13]. Further, human epidermal growth factor receptor 2 (HER2) is a human proto-oncogene [14] that controls cell division and repair in breast tissues [15] The overexpression of HER2 was found in 15–20% of BC [14] and was associated with a more invasive form of BC with less recovery [2, 14, 16, 17]. Furthermore, the fat mass and obesity-associated (FTO) gene, as a strong genetic predictor of obesity [18], is a protein-coding gene [19] and recent studies identified its possible role in several types of malignant cancers such as BC [20]. The FTO gene up-regulation in human breast tissues is reported to be related to the higher breast cell proliferation that can lead to the development and progression of BC [21].
On the other hand, diet, environment, physical activity, body mass index (BMI), smoking, and alcohol use are among non-genetic modifiable risk factors [10, 22,23,24] that have significant roles in BC [25, 26] and represent 30–35% of all types of cancers [7, 9]. Interestingly, dietary factors can regulate the expression of some cancer-related genes [27]. In addition, the mutations of some specific genes may influence the level of nutrient requirements and body response to cancer-related dietary compounds. For example, it was reported that lifestyle and diet have the potential to alter the level of FTO gene expression [27]. However, the effect of the modification of a diet on the consequences of BC is unclear [28]. Nutrition is considered to play a key role in the inhibition and excitation of BC-related genes [1, 5]. Dietary components can influence the expression of genes that are involved in critical metabolic pathways [29] through epigenetic mechanisms [29, 30] including transcription, maturing, and stability of ribonucleic acids (RNAs), translation into proteins, and post-translational modifications (PTMs) [31].
In general, there are contradictory results on the association between diets and BC risk, [32] and the overall impact of diet on the risk of BC is unknown [25, 31]. For example, Farvid et al. concluded that the higher intake of fruits and vegetables is associated with a lower HER2 overexpression and lower risk of BC [4]. However, Pierce et al. reported that a diet high in vegetables, fruit, and fiber had no effect on prognosis following treatment for BC [33]. Also, most of the previous studies investigated the relationship between dietary components and cancer-related gene expression with BC risk in isolation, and thus few studies assessed the interactions between dietary intake, BC-related genes, and BC. Therefore, this study aimed to evaluate the associations between the risk of BC, dietary intake, and BC-related genes expression.
Methods
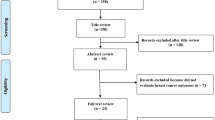
Embase, PubMed, PsycInfo, and the Cochrane databases were used for identifying the related articles. Appropriate keywords including gene or expression or regulation or genetic or mutation or polymorphism AND nutrient or diet or nutrition or macronutrient or micronutrient or vitamin or mineral or protein or carbohydrate or fat or lipid AND breast cancer or breast malignancy or breast tumor were used. All articles published in English from June 1990 to August 2022 which examined the interaction of BC with gene expression and diet were included in the present study. Studies of other cancers, have focused on factors other than gene expression (such as genotype and gene polymorphisms), that only focused on BC and diet, or that only considered BC and genes were excluded from the present study. Also, only genes were included which their interactions with both BC and diet were already investigated at least in two original research. Based on the collected studies, BRCA1, HER2, and FTO genes have been identified. The interactions of nutrients with BC and the expression of BC related genes as well as the mechanisms of their effects were explored.
Results
BRCA1 gene
The breast cancer 1 gene (BRCA1) encodes a tumor suppressor protein that is involved in DNA repair and maintenance of gene stability. Women carrying a mutated copy of BRCA1 gene have 45–70% elevated risk of develo** BC [34].
Some nutrients may influence the association between BRCA1 and BC [35]. For example, moderate B12 supplementation may be protective against BC, particularly in a person who has an inherited mutation of BRCA [36]. Vitamin B12 is essential for DNA synthesis, repair, and methylation by participating in one-carbon metabolism, and B12 deficiency causes chromosome breaks. Thus, sufficient B12 levels may prevent aberrant gene expression, DNA instability, and cancer development. Also, folic acid may have similar effects in the prevention of chromosomal inconsistency, DNA repair, and neoplastic transformation, especially in a person who has an inherited mutation of BRCA [37].
In human BC cells in which aromatic hydrocarbon receptors (AhR) are activated, the hypermethylation of BRCA1 was associated with reduced BRCA-1 and estrogen receptor alpha (ERα) expression. Accordingly, some studies proposed a causative role for AhR in the etiology of breast tumorigenesis. Genistein (GEN), as a common dietary isoflavone, exerts antagonistic effects on DNA methyltransferase (DNMT) enzymes. GEN may have a protective effect against cell proliferation through AhR-mediated BRCA1 CpG methylation in ERα-positive BC cells. Several mechanisms have been proposed for the association between GEN and BRCA1–related BC including rescued BRCA-1 protein expression, reduced DNMT-1 and cyclin D1 expression, reduced BRCA1 CpG methylation, and increased p53 levels [38] (Fig. 1).

Interactions between dietary intake and BRCA1 (breast cancer 1) gene. DNAMT DNA Methyltransferases; AhR Aromatic hydrocarbon receptors
Moreover, BC is potently inhibited by vitamin D3's active form, 1α,25-dihydroxy vitamin D3. BRCA1 and vitamin D3 are both linked to the up-regulation of another tumor suppressor gene, CDKN1A, encoded by p21waf1, the G1 cell cycle inhibitor. The BRCA1 gene can bind to the vitamin D receptor (VDR) and co-occupies the vitamin D responsive elements (VDRE) at the CDKN1A promoter (p21waf1), where acetylation of histone H3 and H4 is increased. Cooperation between BRCA1 and vitamin D may have a crucial role for histone acetylation of the p21waf1 promoter and for growth inhibition of BC cells [39].
HER2 gene
Approximately 10–35% of all types of BC have the overexpression of the human epidermal growth factor receptor 2 (HER2) oncogene which is associated with BC prognosis and response to treatment [40].
HER2 and fatty acids
Some studies indicated that HER2 positive BC cells contain large amounts of endogenous saturated fatty acids (FAs) and neutral fats and generally exhibit a pro-lipogenic phenotype. Small amounts of exogenous palmitate were reported to be toxic to HER2-positive BC cells; thus their effects were studied in Michigan Cancer Foundation-7 (MCF7) and SKBR which are HER2-negative and HER2-positive BC cell lines, respectively. In HER2—positive SKBR3 cells, exogenous palmitate induces a partial estrogen receptor (ER) stress response through the activation of Inositol-requiring enzyme 1 (IRE1) and activating transcription factor 6 (ATF6), two of the three major regulators of ER stress [41]. IRE1 was activated in response to ER-stress, resulting in a non-canonical splicing mechanism wherein the mRNA transcript of X-box binding protein 1 (XBP1) is spliced to give rise to a transcriptionally active variant that up-regulates many genes that are involved in the UPR/ER-stress including many resident ER protein folding chaperones. In addition, ATF6 activity, which is a transmembrane ER protein, was induced by ER-stress [42]. Interestingly, no changes in protein levels or relative phosphorylation rates were detected for the third major regulator of ER stress, namely, the endoplasmic reticulum kinase such as PKR (PERK). This ER stress response was accompanied by a significant reduction in HER2 and HER3 protein levels by interfering with FA synthesis, without creating any changes in phosphorylation [41]. Further, high intensity or prolonged duration of ER-stress can lead to apoptosis through the induction of the pro-apoptotic regulator DNA-damage-inducible transcript 3 (DDIT3/CHOP), thus the increase in DDIT3/CHOP expression with palmitate treatment is responsible for the increase in cell death in the SKBR3 cell line [42]. On the other hand, exogenous palmitate sensitizes HER2-positive BC cells to trastuzumab treatment [41].
Furthermore, alpha-linolenic acid (ALA) supplementation specifically suppresses the overexpression of HER2 in cultured HER2-amplified BC cells [43]. A randomized, double-blind, placebo-controlled study assessed the effects of dietary flaxseed, which is high in ALA (57% of total fatty acids), on tumor biological markers in postmenopausal BC patients. According to the results of this study, flaxseed consumption of 25 g per day significantly reduced the proliferation, apoptosis, and cell signaling by reducing HER2 expression in breast tumors. A decrease in HEB2 expression (71%) and an increase in apoptosis (30.7%) were observed in the flaxseed group but not in the placebo group [44]. Flaxseed oil and n-3 fatty acids were also reported to exert further anticancer effects including reducing the expression of other growth factor receptors such as epidermal growth factor receptors (EGFR) and insulin-like growth factor I receptors (IGF-IR) as well as reducing the expression and activity of fatty acid synthetases (FASN) and enhancing the expression of the tumor suppressor phosphatase and tensin homologs (PTEN) [45]. In summary, these findings suggest that Flaxseed oil reduces tumorigenesis and modulates HER2 expression and growth factor receptor signaling pathways.
HER2 and olive oil
Olive oil was reported to act as a protective factor against several malignancies, especially BC. The fundamental characteristics of olive oil are a high ω − 9 MUFA level, a low ω − 6/ω − 3 PUFA ratio, and the presence of a large number of phenolic compounds including simple phenols, lignans, and secoiridoids such as deacetoxy oleuropein aglycone, oleuropein aglycone, and ligstroside aglycone [46]. A recent study found that olive oil suppressed Her-2 expression and synergistically enhanced the trastuzumab efficacy by promoting DNA fragmentation associated with apoptotic cell death, and dramatically increased both the expression and the nuclear accumulation of p27Kip1 (a cyclin-dependent kinase) in BC cells with HER-2 oncogene amplification. Finally, olive oil co-exposure significantly enhanced the ability of trastuzumab to inhibit the signaling pathway downstream of HER-2, including phosphoproteins such as protein kinase B (AKT) and mitogen-activated protein kinase (MAPK) [47]. Oleuropein aglycone was reported to be the strongest extra virgin olive oil phenol, which reduces the viability of BC cells. It was found that BC cells with HER2 oncogene-overexpression exhibit an exacerbated sensitivity to oleuropein aglycone-induced cytotoxicity. Oleuropein aglycone preferentially induces apoptotic cell death and synergistically enhances trastuzumab-efficacy in HER2-overexpressing BC cells [46] (Fig. 2).

Interactions between dietary intake and HER2 (human epidermal growth factor receptor2) gene. ER Estrogen receptor; IRE1 Inositol-requiring enzyme 1; ATF6 Activating transcription factor 6; PKR Protein kinase R; ↑: Increase; ↓: Decrease
HER2 and phytochemicals
Green tea contains polyphenolic catechin epigallocatechin-gallate (EGCG). Regular consumption of green tea was associated with the prevention of BC through induce apoptosis and inhibit cell proliferation. EGCG may inhibit HER2 and STAT3 phosphorylation in HER2-overexpressing BT-474 BC cells lead to enhanced apoptosis due to loss of nuclear integrity, DNA fragmentation, and further dispersion in the cytoplasm [48].
Genistein treatment of BT-474 HER2-positive cells for five days inhibited total and phosphorylated HER2 protein independently of ER status in vitro experiments [49]. Furthermore, genistein treatment of MCF-7/HER2 and BT-474 BCE cells inhibited the growth of cells by deregulating HER2 [48].The natural flavonol kaempferol is found in a variety of plants and plant-derivatives, including broccoli, tea, and tomato. The administration of 10 mM Kaempferol or 50 mM Kaempferol to MDAMB453 BC cells resulted in cell cycle arrest and apoptosis, which was associated with phosphorylated p53 upregulation [48].
The chemopreventive and therapeutic effects of resveratrol have been observed in HER2-positive BC [50]. In human and mouse HER2-positive BC cells, resveratrol 4.4–50 mM for 4 h inhibited proliferation through inhibition of the FASN signaling pathway and by downregulating HER2 and p185HER2/neu [48].
FTO gene
The fat mass and obesity-associated (FTO) gene expression in BC cells was reported to be significantly higher compared to the normal breast cells, which represents FTO as a potential new marker for the early diagnosis of BC. The findings of a recent study demonstrated that the ATP levels, pyruvate kinase hexokinase activity, and the content of lactic acid significantly decreased in cells that were transfected with the FTO mRNA inhibitor. The overexpression of the FTO gene could promote glycolysis in BC cells (the Warburg effect). Furthermore, the expression of the FTO gene can influence the energy metabolism of BC cells through the PI3K/AKT signaling pathway [51].
Some studies suggested that the level of calories and the level of macronutrients intake have the potential to change the FTO gene expression level. For instance, one study indicated that increasing glucose administration increased FTO gene expression at 48 h post-intervention [52]. High levels of blood glucose and insulin apply some of their effects through the steady activation of the phosphoinositide 3-kinase/protein kinase B (PI3K/AKT) pathway that is involved in cell survival, and eventually, increase the risk of cancer. However, the underlying mechanism of the effect of carbohydrates on PI3K/AKT pathway is unclear [53].
Moreover, recent studies found that there is a mutual interaction between the FTO gene and the intake of protein. According to some clinical trial studies higher protein intake was significantly associated with the up-regulation of the FTO gene. FTO may be involved in pairing cell accessibility to amino acids with the mammalian Target of Rapamycin Complex 1 (MTORC1) signaling pathway. MTORC1 mTOR signaling which is over active in multiple cancer types including BC [54] was reported to be impaired in the absence of FTO [55, 56]. Regarding the effects of micronutrients on FTO gene, a recent study reported that B12 supplementation influences regulation of FTO gene through methylation of microRNA 21 (miR21) [57].
In general, the results of the present study showed that dietary components may change the expression of some BC-related genes and thereby cause a change in the risk of BC. Future research in this field of nutritional genomics can help provide practical nutritional recommendations to prevent BC. However, this study had some limitations. First, few genes were investigated on the interaction of BC with genes and diet. Second, the number of papers examining the interaction of these genes with BC and diet was not sufficient for meta-analysis. Further longitudinal studies on the effects of dietary components on the expression level of different BC-related genes are required to confirm the interactions between BC, genes, and diet and to uncover the underlying mechanisms (Fig. 3 and Table 1).

Interactions between diet intake and fat mass and obesity-associated (FTO) gene expression. PI3K/AKT Phosphoinositide 3-kinase/protein kinase B; mTORC1 Mammalian Target of Rapamycin Complex 1; ↑: Increase; +: Promote
Conclusion
BRCA1, HER2, and FTO may have mutual associations with BC and dietary intake. The expression level of BRCA1, HER2, and FTO genes play important roles in the development of BC and may be regulated by dietary components. The results of this study, if confirmed in future research, can help provide nutritional strategies to regulate the expression of genes related to BC and ultimately prevent BC. Further longitudinal studies are required to confirm the associations between BC-related genes and diet and to uncover the underlying mechanisms.
Availability of data and materials
Not applicable.
Abbreviations
- ATF6:
-
Activating transcription factor 6
- ALA:
-
Alpha-linolenic acid
- AhR:
-
Aromatic hydrocarbon receptors
- BMI:
-
Body mass index
- BC:
-
Breast cancer
- BRCA1:
-
Breast cancer 1 gene
- DNA:
-
Deoxyribonucleic acid
- DNMT:
-
DNA methyltransferase
- DDIT3/CHOP:
-
DNA-damage-inducible transcript 3
- EGFR:
-
Epidermal growth factor receptors
- EGCG:
-
Epigallocatechin-gallate
- ERα:
-
Estrogen receptor alpha
- FTO:
-
Fat mass and obesity-associated gene
- FASN:
-
Fatty acid synthetases
- FA:
-
Fatty acids
- GEN:
-
Genistein
- HER2:
-
Human epidermal growth factor receptor 2
- IGF-IR:
-
Insulin-like growth factor I receptors
- MTORC1:
-
Mammalian target of rapamycin complex 1
- MCF7:
-
Michigan cancer foundation-7
- MAPK:
-
Mitogen-activated protein kinase
- OA:
-
Oleic acid
- PTEN:
-
Phosphatase and tensin homologs
- PI3K/AKT:
-
Phosphoinositide 3-kinase/protein kinase B
- PTMs:
-
Post-translational modifications
- AKT:
-
Protein kinase B
- RNAs:
-
Ribonucleic acids
- VDR:
-
Vitamin D receptor
- VDRE:
-
Vitamin D responsive elements
- XBP1:
-
X-box binding protein 1
References
Sellami M, Bragazzi NL (2020) Nutrigenomics and breast cancer: state-of-art, future perspectives and insights for prevention. Nutrients 12(2):512
Winters S, Martin C, Murphy D, Shokar NK (2017) Breast cancer epidemiology, prevention, and screening. Prog Mol Biol Transl Sci 151:1–32
Hsu LS, Chang CH, Lee YJ, Wang CJ (2019) Nelumbo nucifera leaves prevent NMU-induced mammary tumor through downregulation of fatty acid synthase, estrogen receptor-α and Her2 expression. Am J Chin Med 47(8):1885–1899
Farvid MS, Chen WY, Rosner BA, Tamimi RM, Willett WC, Eliassen AH (2019) Fruit and vegetable consumption and breast cancer incidence: repeated measures over 30 years of follow-up. Int J Cancer 144(7):1496–1510
Donovan MG, Selmin OI, Doetschman TC, Romagnolo DF (2019) Epigenetic activation of BRCA1 by genistein in vivo and triple negative breast cancer cells linked to antagonism toward aryl hydrocarbon receptor. Nutrients 11(11):2559
Brown JC, Ligibel JA (2018) Lifestyle interventions for breast cancer prevention. Curr Breast Cancer Rep 10(3):202–208
Iqbal J, Abbasi B, Khalil A, Ali B, Mahmood T, Kanwal S et al (2018) Dietary isoflavones, the modulator of breast carcinogenesis: current landscape and future perspectives. Asian Pac J Trop Med 11(3):186–193
Rojas K, Stuckey A (2016) Breast cancer epidemiology and risk factors. Clin Obstet Gynecol 59(4):651–672
Castelló A, Boldo E, Pérez-Gómez B, Lope V, Altzibar JM, Martín V et al (2017) Adherence to the western, prudent and mediterranean dietary patterns and breast cancer risk: MCC-Spain study. Maturitas 103:8–15
Naushad SM, Janaki Ramaiah M, Pavithrakumari M, Jayapriya J, Hussain T, Alrokayan SA et al (2016) Artificial neural network-based exploration of gene-nutrient interactions in folate and xenobiotic metabolic pathways that modulate susceptibility to breast cancer. Gene 580(2):159–168
Sattar SA, Khashman B, Abdulla K, Al-Obaidie S, Fadhil N (2020) Expression of Brca1 in a group of Iraqi patients with breast cancer. Pharm Biol Sci 13(4):10–14.
Jackson KC, Tarpey MD, Valencia AP, Iñigo MR, Pratt SJ, Patteson DJ et al (2018) Induced Cre-mediated knockdown of Brca1 in skeletal muscle reduces mitochondrial respiration and prevents glucose intolerance in adult mice on a high-fat diet. FASEB J 32(6):3070–3084
Sturgeon KM, Dean LT, Heroux M, Kane J, Bauer T, Palmer E et al (2017) Commercially available lifestyle modification program: randomized controlled trial addressing heart and bone health in BRCA1/2+ breast cancer survivors after risk-reducing sal**o-oophorectomy. J Cancer Surviv 11(2):246–255
Ahn S, Woo JW, Lee K, Park SY (2020) HER2 status in breast cancer: changes in guidelines and complicating factors for interpretation. J Pathol Transl Med 54(1):34–44
Wilson FR, Coombes ME, Wylie Q, Yurchenko M, Brezden-Masley C, Hutton B et al (2017) Herceptin® (trastuzumab) in HER2-positive early breast cancer: protocol for a systematic review and cumulative network meta-analysis. Syst Rev 6(1):1–8
Stocker A, Trojan A, Elfgen C, Hilbers ML, Moskovszky L, Varga Z (2020) Differential prognostic value of positive HER2 status determined by immunohistochemistry or fluorescence in situ hybridization in breast cancer. Breast Cancer Res Treat 183(2):311–319
Wang T, Xu Y, Sheng S, Yuan H, Ouyang T, Li J et al (2017) HER2 somatic mutations are associated with poor survival in HER2-negative breast cancers. Cancer Sci 108(4):671–677
Surendran S, Jayashri R, Drysdale L, Bodhini D, Lakshmipriya N, Shanthi Rani CS et al (2019) Evidence for the association between FTO gene variants and vitamin B12 concentrations in an Asian Indian population. Genes Nutr 14(1):26
Xu D, Shao W, Jiang Y, Wang X, Liu Y, Liu X (2017) FTO expression is associated with the occurrence of gastric cancer and prognosis. Oncol Rep 38(4):2285–2292
Chen J, Du B (2019) Novel positioning from obesity to cancer: FTO, an m(6)A RNA demethylase, regulates tumour progression. J Cancer Res Clin Oncol 145(1):19–29
Niu Y, Lin Z, Wan A, Chen H, Liang H, Sun L et al (2019) RNA N6-methyladenosine demethylase FTO promotes breast tumor progression through inhibiting BNIP3. Mol Cancer 18(1):46
Matejcic M, de Batlle J, Ricci C, Biessy C, Perrier F, Huybrechts I et al (2017) Biomarkers of folate and vitamin B12 and breast cancer risk: report from the EPIC cohort. Int J Cancer 140(6):1246–1259
Rajendran P, Alzahrani AM, Rengarajan T, Veeraraghavan VP, Krishna MS (2020) Consumption of reused vegetable oil intensifies BRCA1 mutations. Crit Rev Food Sci Nutr 62(5):1222–1229
Boldo E, Castelló A, Aragonés N, Amiano P, Pérez-Gómez B, Castaño-Vinyals G et al (2018) Meat intake, methods and degrees of cooking and breast cancer risk in the MCC-Spain study. Maturitas 110:62–70
Arthur R, Wassertheil-Smoller S, Manson JE, Luo J, Snetselaar L, Hastert T et al (2018) The combined association of modifiable risk factors with breast cancer risk in the women’s health initiative. Cancer Prev Res 11(6):317–326
Dani C, Gonçalves LK, Proença IT, Andrade FO, Hilakivi-Clarke L (2020) Effects of maternal grape juice intake on unfolded protein response in the mammary glands of offspring of high fat diet fed rat dams. Nutrients 12(8):1–16
Franzago M, Santurbano D, Vitacolonna E, Stuppia L (2020) Genes and diet in the prevention of chronic diseases in future generations. Int J Mol Sci 21(7):2633
Hensing W, Santa-Maria CA, Peterson LL, Sheng JY (2020) Landmark trials in the medical oncology management of early stage breast cancer. Semin Oncol 47(5):278–292
Ramos-Lopez O, Milagro FI, Allayee H, Chmurzynska A, Choi MS, Curi R et al (2017) Guide for current nutrigenetic, nutrigenomic, and nutriepigenetic approaches for precision nutrition involving the prevention and management of chronic diseases associated with obesity. J Nutrigenet Nutrigenomics 10(1–2):43–62
Zhang Y, Kutateladze TG (2018) Diet and the epigenome. Nat Commun 9(1):3375
Herrera-Marcos LV, Lou-Bonafonte JM, Arnal C, Navarro MA, Osada J (2017) Transcriptomics and the mediterranean diet: a systematic review. Nutrients 9(5):472
Tabung FK, Steck SE, Liese AD, Zhang J, Ma Y, Johnson KC et al (2016) Patterns of change over time and history of the inflammatory potential of diet and risk of breast cancer among postmenopausal women. Breast Cancer Res Treat 159(1):139–149
Pierce JP, Natarajan L, Caan BJ, Parker BA, Greenberg ER, Flatt SW et al (2007) Influence of a diet very high in vegetables, fruit, and fiber and low in fat on prognosis following treatment for breast cancer: the Women’s Healthy Eating and Living (WHEL) randomized trial. JAMA 298(3):289–298
Kim SJ, Zuchniak A, Sohn KJ, Lubinski J, Demsky R, Eisen A et al (2016) Plasma folate, Vitamin B-6, and Vitamin B-12 and breast cancer risk in BRCA1- and BRCA2-mutation carriers: a prospective study. Am J Clin Nutr 104(3):671–677
Pirouzpanah S, Taleban F-A, Mehdipour P, Atri M (2015) Association of folate and other one-carbon related nutrients with hypermethylation status and expression of RARB, BRCA1, and RASSF1A genes in breast cancer patients. J Mol Med 93(8):917–934
Kim SJ, Zhang CXW, Demsky R, Armel S, Kim YI, Narod SA et al (2019) Folic acid supplement use and breast cancer risk in BRCA1 and BRCA2 mutation carriers: a case-control study. Breast Cancer Res Treat 174(3):741–748
Wu W, Kang S, Zhang D (2013) Association of vitamin B6, vitamin B12 and methionine with risk of breast cancer: a dose-response meta-analysis. Br J Cancer 109(7):1926–1944
Romagnolo DF, Donovan MG, Papoutsis AJ, Doetschman TC, Selmin OI (2017) Genistein prevents BRCA1 CpG methylation and proliferation in human breast cancer cells with activated aromatic hydrocarbon receptor. Curr Dev Nutr 1(6):562
Pickholtz I, Saadyan S, Keshet GI, Wang VS, Cohen R, Bouwman P et al (2014) Cooperation between BRCA1 and vitamin D is critical for histone acetylation of the p21waf1 promoter and for growth inhibition of breast cancer cells and cancer stem-like cells. Oncotarget 5(23):11827
Gheni N, Westenberg D (2020) Quantitative real-time PCR assay with immunohistochemical evaluation of HER2/neu oncogene in breast cancer patients and its correlation with clinicopathological findings. Indian J Pathol Microbiol 63(Supplement):S123–S128
Baumann J, Wong J, Sun Y, Conklin DS (2016) Palmitate-induced ER stress increases trastuzumab sensitivity in HER2/neu-positive breast cancer cells. BMC Cancer 16(1):1–5
Baumann J, Sevinsky C, Conklin DS (2013) Lipid biology of breast cancer. Biochim Biophys Acta 1831(10):1509–1517
Menéndez JA, Vázquez-Martín A, Ropero S, Colomer R, Lupu R (2006) HER2 (erbB-2)-targeted effects of the omega-3 polyunsaturated fatty acid, alpha-linolenic acid (ALA; 18:3n–3), in breast cancer cells: the “fat features” of the “Mediterranean diet” as an “anti-HER2 cocktail.” Clin Transl Oncol 8(11):812–820
Thompson LU, Chen JM, Li T, Strasser-Weippl K, Goss PE (2005) Dietary flaxseed alters tumor biological markers in postmenopausal breast cancer. Clin Cancer Res 11(10):3828–3835
Mason JK, Fu M, Chen J, Thompson LU (2015) Flaxseed oil enhances the effectiveness of trastuzumab in reducing the growth of HER2-overexpressing human breast tumors (BT-474). J Nutr Biochem 26(1):16–23
Menendez JA, Vazquez-Martin A, Colomer R, Brunet J, Carrasco-Pancorbo A, Garcia-Villalba R et al (2007) Olive oil’s bitter principle reverses acquired autoresistance to trastuzumab (Herceptin) in HER2-overexpressing breast cancer cells. BMC Cancer 7:80
LeMay-Nedjelski L, Mason-Ennis JK, Taibi A, Comelli EM, Thompson LU (2018) Omega-3 polyunsaturated fatty acids time-dependently reduce cell viability and oncogenic MicroRNA-21 expression in estrogen receptor-positive breast cancer cells (MCF-7). Int J Mol Sci 19(1):244
Zabaleta ME, Forbes-Hernández TY, Simal-Gandara J, Quiles JL, Cianciosi D, Bullon B et al (2020) Effect of polyphenols on HER2-positive breast cancer and related miRNAs: epigenomic regulation. Food Res Int 137:109623
Sakla MS, Shenouda NS, Ansell PJ, Macdonald RS, Lubahn DB (2007) Genistein affects HER2 protein concentration, activation, and promoter regulation in BT-474 human breast cancer cells. Endocrine 32(1):69–78
Carlos-Reyes Á, López-González JS, Meneses-Flores M, Gallardo-Rincón D, Ruíz-García E, Marchat LA et al (2019) Dietary compounds as epigenetic modulating agents in cancer. Front Genet 10:79
Liu Y, Wang R, Zhang L, Li J, Lou K, Shi B (2017) The lipid metabolism gene FTO influences breast cancer cell energy metabolism via the PI3K/AKT signaling pathway. Oncol Lett 13(6):4685–4690
Doaei S, Kalantari N, Mohammadi NK, Tabesh GA, Gholamalizadeh M (2017) Macronutrients and the FTO gene expression in hypothalamus; a systematic review of experimental studies. Indian Heart J 69(2):277–281
Doaei S, Gholamalizadeh M, Akbari ME, Akbari S, Feradova H, Rahimzadeh G et al (2019) Dietary carbohydrate promotes cell survival in cancer via the up-regulation of fat mass and obesity-associated gene expression level. Malays J Med Sci 26(2):8–17
Hare SH, Harvey AJ (2017) mTOR function and therapeutic targeting in breast cancer. Am J Cancer Res 7(3):383
Vahid F, Hekmatdoost A, Mirmajidi S, Doaei S, Rahmani D, Faghfoori Z (2019) Association between index of nutritional quality and nonalcoholic fatty liver disease: the role of vitamin D and B group. Am J Med Sci 358(3):212–218
Speakman JR (2015) The “fat mass and obesity related” (FTO) gene: mechanisms of impact on obesity and energy balance. Curr Obes Rep 4(1):73–91
Yadav DK, Shrestha S, Lillycrop KA, Joglekar CV, Pan H, Holbrook JD et al (2018) Vitamin B(12) supplementation influences methylation of genes associated with type 2 diabetes and its intermediate traits. Epigenomics 10(1):71–90
Acknowledgments
Not applicable.
Funding
Funding for this study was provided by School of Nutrition and Food Sciences, National Nutrition and Food Technology Research Institute, Shahid Beheshti University of Medical Sciences (Code 27870).
Author information
Authors and Affiliations
Contributions
FB, SD, KA, NHA, AH, SA, and MGH designed the study, and carried out the data collection. AEB, MA, AH, and SD were involved in the design of the study, analysis of the data, and critically reviewed the manuscript. This study was conducted at the Shahid Beheshti University of Medical Sciences, Tehran, Iran. All authors read and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by The Shahid-Beheshti University of Medical Sciences (code: IR.SBMU.NNFTRI.REC.1400.041).
Consent for publication
Institutional consent forms were used in this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bourbour, F., Pourtaheri, A., Abbasi, K. et al. Interactions dietary components with expression level of breast cancer-related genes. Egypt J Med Hum Genet 23, 165 (2022). https://doi.org/10.1186/s43042-022-00375-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43042-022-00375-w