
Abstract
Background
Ultrasound (US)-guided quadratus lumborum block (QLB) and transversus abdominis plane block (TAP) are used as a part of multimodal analgesia for postoperative pain after abdominal procedures, as they improve postoperative pain.
Results
QLB group showed significantly better visual analog score (VAS) scores from 6 h till 24 h postoperative. Time for the first request for pethidine was significantly longer in the QLB group (398.3 ± 23.7 min) than in the TAP group (80.3 ± 20.7 min), (p < 0.0001 and its total consumption was significantly lesser (p = 0.007) in the QLB group (68.33 ± 66.28) than in TAP group (120.0 ± 76.11). Also, the sensory level was higher in the QLB group (8.3 ± 0.63 segments) than in the TAP group (6.2 ± 0.79 segments), (p < 0.001). Moreover, only 2 patients (6.67%) in the QLB group experienced nausea and/or vomiting versus 9 (30%) in TAP group with significant value.
Conclusions
QLB was more effective in providing visceral and somatic pain analgesia after total abdominal hysterectomy (TAH) in comparison to TAP block, QLB resulted in wider sensory blockade compared to TAP block with less incidence of postoperative nausea and/or vomiting.
Similar content being viewed by others

Background
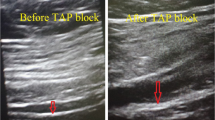
Enhanced recovery after surgery is a multimodal perioperative care pathway that promotes preoperative organ function and reduces the stress response generated by surgical trauma to achieve and improve speedy recovery (Shida et al., 2015). Opioids, the popular painkiller, have several side effects such as sedation, dizziness, nausea, vomiting, constipation, physical dependence, tolerance, pruritis, and respiratory depression (Woodhouse & Mather, 1998). As a result, various approaches are required to control postoperative pain and reduce opioid usage and adverse effects (Ng et al., 2002). The sensory nerves of the anterolateral abdominal wall, T6-L1, that travel to innervate the abdomen are blocked during the TAP block (Almarakbi & Kaki, 2014). After lower abdominal surgery, a TAP block can provide effective analgesia (Wegner et al., 2017).
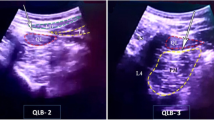
QLB block is classified anatomically into 3 groups: QLB 1 (Lateral approach) provides analgesia from T7 to L1 (Abrahams & Derby, 2016). QLB 2 is conducted by injection medication at the site posterior to the quadratus lumborum muscle from the posterior abdominal wall (Blanco et al., 2015). QLB 3, also referred to as transmuscular quadratus lumborum block, aimed at the anterior border of quadratus lumborum and posterior to psoas major, so that the anesthetic can spread to the thoracic paravertebral space (Hansen et al., 2016).
In comparison to the TAP block, Blanco’s QLB has an advantage in extending the local anesthetic agent beyond the transversus abdominis plane to the thoracic paravertebral area. This increased distribution of local anesthetic agents causes significant analgesia and prolongs the effect of the injected local anesthetic solution (Blanco et al., 2016).
This study aims to compare the effect of ultrasound-guided bilateral QLB versus bilateral ultrasound-guided TAP block on intraoperative and postoperative analgesia in patients undergoing total abdominal hysterectomy under general anesthesia, compare sensory level between QLB and TAP groups, and compare the incidence of postoperative nausea and vomiting.
Methods
Ethical approval for this study (FMASU M D 237/2019) was provided by the Ethics committee of Ain Shams University hospital, Abbasia, Cairo, Egypt on 20 August 2019. Written informed consent was obtained from all subjects. This trial followed the CONSORT statement. This prospective randomized interventional study was conducted at Ain-Shams University gynecology and obstetrics hospital in the operating rooms from September 2019 to January 2021
Sixty adult female patients American Society of anesthesiologists (ASA) Physical Status Class I and II, scheduled for TAH were randomized into two equal groups (TAP group and QLB group). Randomization was performed using a computer-generated random number table in opaque sealed envelopes with a 1:1 allocation ratio by an anesthesiologist not directly involved in the trial.
-
Group TAP (n = 30): where each patient received general anesthesia plus bilateral TAP block.
-
Group QLB (n = 30): where each patient received general anesthesia plus bilateral QL block.
Inclusion criteria
-
1.
Female, aged ≥ 45–≤ 60 years.
-
2.
ASA physical status classes I and II.
-
3.
Scheduled for total abdominal hysterectomy.
Exclusion criteria
-
1.
Included patients who refused to participate in this study.
-
2.
Had a body mass index (BMI) of more than 30 kg/m.
-
3.
ASA physical status more than II, or had major disease, e.g., cardiac, renal, respiratory, neurologic, or hepatic.
-
4.
Patients using anticoagulants or with coagulopathy.
-
5.
Infection at the site of injection.
-
6.
Allergy or contraindications to local anesthetics.
Anesthesia and surgical procedure
On arrival of the patients to the operating room, electrocardiography (ECG), noninvasive blood pressure, and pulse oximetry were applied. Baseline parameters such as systolic blood pressure (SBP), diastolic blood pressure (DBP), mean blood pressure (MABP), heart rate (HR), and arterial oxygen saturation (SpO2) were recorded. An intravenous (IV) line was inserted, and IV fluid started. For both groups, general anesthesia was induced with IV injection of fentanyl (1 μg/kg) and propofol (2 mg/kg) then, atracurium (0.5 mg/kg) was injected for endotracheal intubation then capnography was connected, and mechanical ventilation was used to maintain the end-expiratory CO2 (ETCO2) values between 34 and 36 mmHg. Anesthesia was maintained with isoflurane 1–2% in a 40% oxygen-air mixture. An incremental dose of atracurium (0.1 mg/kg) was given every 30 min or when needed. After endotracheal intubation, stabilization of the patient’s vital data, and before the start of the surgery, the anesthesiologist (who was blinded to the collected data until the end of the study) performed the block techniques and administered the medication. Both blocks were performed under complete aseptic precautions using an ultrasound machine with a high-frequency linear probe covered with a sterile sheath (Sonoscape® SSI 6000, Chinawith12 6 MHz high-frequency linear probe) and 100 mm needle (BBraun Medical Inc., Bethlehem, PA, USA).
Intraoperative fentanyl 50 ug was given if the HR or the blood pressure or both increase > 20% of the baseline. Isoflurane was discontinued on completion of the surgical procedure, and neostigmine 0.04 mg/kg plus atropine 0.02 mg/kg was administered to reverse the effect of atracurium. After emergence from anesthesia and achieving an appropriate level of consciousness, the patient was discharged from the operating room to the postanesthesia care unit (PACU).
Then, we recorded postoperative total dose of pethidine used/24 h, VAS for pain at 0, 2, 4, 6, 12, 18, and 24 h postoperatively also blood pressure and heart rate 0, 30 min, 2, 4, 6, 12, 18 and 24 h were recorded, the total dose of fentanyl used intraoperative, the number of patients needed rescue analgesia and any side effect. The sensory level between QLB and TAP groups was compared. Also, the incidence of postoperative nausea and vomiting between both groups was compared.
When VAS score was 3 or more, the patient request, heart rate > 110 beats per minute and or mean arterial blood pressure > 20% from the baseline, 50 mg pethidine was given intravenously. No other analgesic drugs were given except pethidine. The total amount of pethidine consumed in 24 hours was recorded.
Patient-reported outcomes
Primary outcome
The total dose of pethidine used postoperatively/patient rescue analgesia for 24 h.
Secondary outcome
VAS for pain (recorded at 0, 2, 4, 6, 12, 18, and 24 h postoperative).
Incidence of postoperative adverse effects.
The number of patients needed rescue analgesia.
Assessment of sensory level in both groups.
The total dose of fentanyl used intraoperatively.
Sample size calculation
The sample size was calculated using the STATA® version 10 programs, setting the alpha error 5% and power at 90%. Results from a previous study (Yousef, 2018) showed that 77% of TAP group cases needed analgesia postoperatively compared to 27% of the QL group. Calculation according to these values produced a sample size of 30 patients per group taking into account a 20% dropout rate.
Statistical analysis
Data were analyzed using Statistical Package for Social Science (SPSS) version 22.0. Quantitative data were expressed as mean ± standard deviation (SD). Qualitative data were expressed as frequency and percentage. The following tests were used: Independent-samples t test of significance was used when comparing between two means, chi-square (χ2) test of significance was used to compare proportions between two qualitative parameters, Mann-Whitney U test: for two-group comparisons in non-parametric data, the confidence interval was set to 95% and the margin of error accepted was set to 5%. So, we set the significance level at a p value < 0.001 was considered significant.
Results
Seventy-two patients were eligible for the study, 2 patients did not meet inclusion criteria and ten patients denied consenting for the study. So, 60 patients were enrolled in the study: 30 patients in each group (Fig. 1).

Consort patient flowchart
Postoperative vital data in the form of MABP and HR were compared in the 2 groups and there were no statistical differences between the groups at 1st 6 h then TAP block group had more increase in blood pressure and HR further on (Fig. 2). The 2 groups were not statistically different for demographic data (Table 1). MABP and HR were significantly higher in the TAP group than in the QLB group with a p value less than 0.05.

Comparison between both groups as MABP and HR
At PACU arrival till the first 6 h postoperative, the QLB group exhibited better clinical pain scores than the TAP block group, however without statistically significant difference between the two groups. Then, QLB group started to show better VAS scores with significant differences till 24 h postoperative (Table 2). Sensory level was higher in the QLB group than in the TAP group (Table 3).
As regards the total dose of narcotics used in each group, intraoperative fentanyl showed no difference between the two groups, but postoperative pethidine consumption was more in the TAP group than the QLP group (P < 0.001) (Table 4).
Nausea and vomiting were also examined between the groups and there was a significant difference as the TAP group had more postoperative nausea and vomiting mostly related to more narcotic consumption and more pain score.
Table 5 shows the statistically significant difference between groups as regards nausea and vomiting.
Discussion
One of the most prevalent medical procedures that cause considerable postoperative pain is hysterectomy (Wright et al., 2013). Poor pain control after abdominal hysterectomy is linked to a longer hospital stay and recovery time, as well as psychological changes, quality of life, and patient satisfaction (Blanton et al., 2017). Postoperative pain control after hysterectomy prevents the development of chronic pain (Katz & Seltzer, 2009).
In postoperative treatment, adequate and safe postoperative analgesia is critical (Baik et al., 2014). Unfortunately, the usage of opioids has side effects such as nausea and vomiting, as well as the risk of long-term dependence (Clarke et al., 2014). The sensory afferent nerves that run between the abdominal muscles are blocked by the TAP block, which reduces surgical incisional pain (McDonnell et al., 2007).
The current study also calculated and compared the standard deviation for each of the two groups analyzed, as well as the postoperative VAS score, initial time to rescue analgesia, and total amount of opioids (pethidine) administered in the first 24 h. When compared to the QLB group, TAP block patients showed higher values. The effects of QLB and TAP blocks in this study resulted in a lower incidence and severity of postoperative pain, as well as a lower incidence of total opioid demand. QLB was found to be more effective than TAP block in this clinical trial. The QLB approach was found to be superior to the TAP block approach in terms of analgesia (pethidine), total pethidine consumption, and VAS score. TAP patients had higher pain ratings and were the first to request assistance.
Also, there is less incidence of postoperative nausea and vomiting in the QLB group. The current study’s findings were congruent with Yousef’s findings on the same topic, in which she compared QLB and TAP blocks on 60 females undergoing total abdominal hysterectomy under general anesthesia and separated them into two groups. The findings corroborated our findings in terms of total opioid use and pain control duration in the first 24 h after QLB duration (Yousef, 2018).
The findings of this study backed up Blanco et al.’s findings from 2016, which revealed that the QLB provides longer-lasting analgesia than the TAP block. Furthermore, their findings demonstrate that using QLB as the default approach can dramatically minimize opiate consumption and deleterious effects after cesarean delivery (Blanco et al., 2016).
Furthermore, the findings backed with Blanco et al.’s findings from 2016, which looked at the effects of QLB versus placebo on patient-controlled analgesia (PCA) morphine doses and postcesarean demand. Six and twelve hours after surgery, patients who took QLB had considerably lower morphine intake than control groups. They also required much less morphine at all times following the Caesarean procedure. The VAS scores in the QLB group were considerably higher than in the control group (Blanco et al., 2016).
Aditianingsih et al. investigated the analgesic impact of recurrent QLB versus continuous epidural analgesia after laparoscopic nephrectomy in terms of total opioid dose, hemodynamic changes, and postoperative nausea and vomiting, QLB used the same total amount of opioids as epidural analgesia to control pain in 65 patients in the first 24 h after surgery, with no difference in the incidence of postoperative nausea and vomiting (Aditianingsih et al., 2019).
However, Borys et al. found that the TAB or QL block did not manage postoperative persistent pain, such as neuropathic pain. They measure postoperative pain for the first, third, and sixth months after CS surgery, but we did not address these topics here whoever was successful in managing pain in the first 24 h postoperatively using the QLB approach, as previously mentioned (Borys et al., 2019).
Conclusions
Our results showed that QLB was more effective in providing analgesia after TAH in comparison to TAP block and even more time covering to rescue opioids, sensory level was higher in the QLB group than in the TAP group with less incidence of postoperative nausea and/or vomiting.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- US:
-
Ultrasound
- QLB:
-
Quadratus lumborum block
- TAP:
-
Transversus abdominis plane
- TAH:
-
Total abdominal hysterectomy
- ASA:
-
American Society of anesthesiologists
- ECG:
-
Electrocardiography
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- MABP:
-
Mean arterial blood pressure
- Spo2:
-
Arterial oxygen saturation
- Etco2:
-
End-tidal co2
- VAS:
-
Score visual analog score
- PACU:
-
Postanesthesia care unit
- SPSS:
-
Statistical Package for Social Science
References
Abrahams M, Derby R, Horn J-L (2016) Update on ultrasound for truncal blocks: a review of the evidence. Reg Anesth Pain Med 2:275–288
Aditianingsih D, Pryambodho AN, Tantri AR, Mochtar CA (2019) A randomized controlled trial on the analgesic effect of repeated Quadratus Lumborum block versus continuous epidural analgesia following laparoscopic nephrectomy. BMC Anesthesiol. 19(1):221
Almarakbi WA, Kaki AM (2014) Addition of dexmedetomidine to bupivacaine in transversus abdominis plane block potentiates postoperative pain relief among abdominal hysterectomy patients: a prospective randomized controlled trial. Saudi J Anaesth. 8:161–166
Baik JS, Oh A-Y, Cho CW, Shin H-J, Han SH, Ryu JH (2014) Thoracic paravertebral block for nephrectomy: a randomized, controlled, observer-blinded study. Pain Med. 15(5):850–856. https://doi.org/10.1111/pme.12320
Blanco R, Ansari T, Girgis E (2015) Quadratus lumborum block for postoperative pain after cesarean section: a randomized controlled trial. Eur J Anaesthesiol. 32(11):812–818. https://doi.org/10.1097/EJA.0000000000000299
Blanco R, Ansari T, Riad W, Shetty N (2016) Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: a randomized controlled trial. Reg Anesth Pain Med. 41(6):757–762
Blanton E, Lamvu G, Patanwala I et al (2017) Non-opioid pain management in benign minimally invasive hysterectomy: a systematic review. Am J Obstet Gynecol. 216:557–567
Borys M, Potręć-Studzińska B, Wiech M et al (2019) Transversus abdominis plane block and quadratus lumborum block did not reduce the incidence or severity of chronic postsurgical pain following cesarean section: a prospective, observational study. Anaesthesiol Intensive Ther. 51(4):257–261
Clarke H, Soneji N, Ko DT et al (2014) Rates and risk factors for prolonged opioid use after major surgery: population-based cohort study. BMJ. 348:1251
Hansen CK, Dam M, Bendtsen TF, Borglum J (2016) Ultrasound-guided quadratus lumborum blocks: definition of the clinically relevant endpoint of injection and the safest approach. An A Case Rep. 6(2):39. https://doi.org/10.1213/XAA.0000000000000270
Katz J, Seltzer Z (2009) Transition from acute to chronic postsurgical pain: risk factors and protective factors. Expert Rev Neurother. 9:723–744
McDonnell JG, O'Donnell B, Curley G et al (2007) The analgesic efficacy of transversus abdominis plane block after abdominal surgery: a prospective randomized controlled trial. Anesth Analg 104:193–197
Ng A, Swami A, Smith G, Davidson AC, Emembolu J (2002) The analgesic effects of intraperitoneal and incisional bupivacaine with epinephrine after total abdominal hysterectomy. Anesth Analg 95:158–162
Shida D, Tagawa K, Inada K, Nasu K, Seyama Y, Maeshiro T et al (2015) Enhanced recovery after surgery (ERAS) protocols for colorectal cancer in Japan. BMC Surg. 15:90. https://doi.org/10.1186/s12893-015-0079-0
Wegner R, Akwar D, Reyes S et al (2017) Evaluating the adjuvant effect of dexamethasone to ropivacaine in transversus abdominus plain block for inguinal hernia repair and spermatocelectomy: a Randomized control trial. Pain Physician 20:413–418
Woodhouse A, Mather LE (1998) The effect of duration of dose delivery with patient-controlled analgesia on the incidence of nausea and vomiting after hysterectomy. Br J Clin Pharmacol 45:57–62
Wright JD, Herzog TJ, Tsui J et al (2013) Nationwide trends in the performance of - inpatient hysterectomy in the United States. Obstet Gynecol. 122:233–241
Yousef NK (2018) Quadratus lumborum block versus transversus abdominis plane block in patients undergoing total abdominal hysterectomy: a randomized prospective controlled trial. Anesth Essays Res. 12(3):742–747
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
Study supervision: HA, AK. Drafting the article: AA and YA. Conception and design: AA and YA. Statistical analysis: AK and HA. Acquisition of data: AE and AA. Analysis and interpretation of data: AE and AA. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Administrative/technical/material support: all authors. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for this study (FMASU M D 237/2019) was provided by the Ethics committee of Ain Shams University hospital, Abbasia, Cairo, Egypt on 20/8/2019. Written informed consent was obtained from all subjects.
Consent for publication
Not applicable.
Competing interests
All authors declare that they no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alansary, A.M., Kamaly, A.M., Abdel Hamid, H.S. et al. Ultrasound-guided quadratus lumborum block versus transversus abdominis plane block in patients undergoing total abdominal hysterectomy. Ain-Shams J Anesthesiol 14, 22 (2022). https://doi.org/10.1186/s42077-022-00224-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42077-022-00224-3