
Abstract
Background
The aim of this study was to evaluate the efficacy of fluorine 18 (18F) labeled fibroblast activation protein inhibitor (FAPI) in identifying mediastinal and hilar lymph node metastases and to develop a model to quantitatively and repeatedly identify lymph node status.
Methods
Twenty-seven patients with 137 lymph nodes were identified by two PET/CT images. The sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of lymph node status were analyzed, and the optimal cut-off value was identified by ROC analysis.
Results
The SUVmax of metastatic lymph nodes on 18F-FAPI was higher than that on 18F-FDG PET/CT (10.87 ± 7.29 vs 6.08 ± 5.37, p < 0.001). 18F-FAPI presented much greater lymph node detection sensitivity, specificity, accuracy, PPV and NPV than 18F-FDG PET/CT (84% vs. 71%; 92% vs. 67%; 90% vs. 69%, 84% vs. 52%, and 92% vs. 83%, respectively). Additionally, the diagnostic effectiveness of 18F-FAPI in small lymph nodes was greater than that of 18F-FDG PET/CT (specificity: 96% vs. 72%; accuracy: 93% vs. 73%; PPV: 77% vs. 33%, respectively). Notably, the optimal cut-off value for specificity and PPV of 18F-FAPI SUVmax was 5.3; the optimal cut-off value for sensitivity and NPV was 2.5.
Conclusion
18F-FAPI showed promising diagnostic efficacy in metastatic mediastinal and hilar lymph nodes from lung cancer patients, with a higher SUVmax, especially in small metastatic nodes, compared with 18F-FDG. In addition, this exploratory work recommended optimal SUVmax cutoff values to distinguish between nonmetastatic and metastatic lymph nodes, thereby advancing the development of image-guided radiation.
Trial registration ClinicalTrials.gov identifier: ChiCTR2000036091.
Similar content being viewed by others


Background
Lung cancer is the oncologic disease with the highest mortality rate worldwide, and it accounts for over 20% of cancer-related deaths each year [1]. For patients with locally advanced lung cancer, regional lymph node staging is very important, as it guides the choice of treatment. Histopathological and imaging examinations are the most commonly used methods to predict mediastinal and hilar lymph node staging in patients with lung cancer.
Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is the “gold standard” for the evaluation of mediastinal and hilar lymph nodes in patients with lung cancer and is recommended by the National Comprehensive Cancer Network [2]; however, the diagnostic accuracy of EBUS-TBNA is insufficient due to intratumor heterogeneity and endoscopist skills [3, 4]. On the other hand, enhanced computed tomography (CT) is a commonly used imaging technique for evaluating mediastinal and hilar lymph nodes in patients with lung cancer, and a cutoff value of 10 mm for the short-axis diameter has been suggested to define abnormal lymph nodes [5, 6]. However, a retrospective study involving 2817 mediastinal and hilar lymph nodes revealed that the sensitivities of enhanced CT in diagnosing mediastinal and hilar lymph nodes were only 18.9% and 17.0%, respectively [7]. 18F-fluorodeoxyglucose ([18F]-FDG) positron emission tomography/computed tomography (PET/CT) is always recommended for tumor diagnosis and staging [8], but it is not sufficiently specific for diagnosing lymph nodes, as inflammatory lesions also demonstrate enhanced FDG uptake [9, 10].
68Ga/18F-labeled fibroblast-activation protein inhibitor (FAPI) PET/CT has been used in various kinds of tumors and demonstrated a complementary role in discriminating malignant from benign lesions [11], and it can reveal more metastatic lymph nodes in various cancers than 18F-FDG [12,13,14,15]. A recent case report demonstrated that 68Ga-FAPI PET/CT scans downstage the TNM stage of squamous cell lung cancer due to the lack of FAPI uptake in the enlarged right lower paratracheal lymph node [10]. These encouraging results prompted us to compare 18F-AlF-FAPI-04 (18F-FAPI) PET/CT to 18F-FDG PET/CT for identifying mediastinal and hilar lymph nodes in lung cancer patients.
This study aims to compare the diagnostic efficacy of 18F-FAPI PET/CT and 18F-FDG PET/CT in patients with locally advanced lung cancer for the diagnosis of metastatic mediastinal and hilar lymph nodes. More importantly, an optimal SUVmax cutoff value should be determined to quantitatively and frequently diagnoses lymph nodes, especially in small lymph nodes.
Methods
Study participants
Twenty-seven patients diagnosed with lung cancer referred to staging of disease were prospectively recruited and underwent both 18F-FDG PET/CT and 18F-FAPI PET/CT scans. The patients were enrolled as part of a larger ongoing study in our institution to evaluate the role of 18F-FAPI PET/CT in the imaging of mediastinal and hilar lymph node metastasis in lung cancer patients (ClinicalTrials.gov identifier: ChiCTR2000036091). The inclusion criteria were as follows: (i) patients diagnosed with lung cancer pathologically; (ii) paired 18F-FDG and 18F-FAPI PET/CT were performed within one week. The exclusion criteria were (i) pregnant patients, (ii) patients with another malignant disease, and (iii) participants who were unwilling to undergo 18F-FDG or 18F-FAPI PET/CT examination. This study was approved by the institutional review board (IRB) of the Shanghai Proton and Heavy Ion Center (SPHIC) (ethical code: 2106-49-01) and conducted in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards, and all subjects signed an informed consent form. The final diagnosis was confirmed by EBUS or follow-up. Follow-up contrast-enhanced CT was performed 6 months after treatment. Lymph nodes in the follow-up images were considered malignant based on the following criteria: (i) the morphology, growth pattern and enhancement pattern of the nodes were consistent with the characteristics of malignant tumors, (ii) tumor progression after treatment, and (iii) tumor shrinkage after treatment.
Radiopharmaceuticals and PET/CT imaging
The synthesis of [18F]-FDG was based on a cyclotron (Siemens CTI RDS Eclips ST, Knoxville, TN). 18F-AlF-FAPI-04 preparation was performed according to a published procedure [16]. The radiochemical purity was over 95%.
Paired 18F-FDG and 18F-FAPI scans were performed within 7 days. For 18F-FDG PET/CT, patients were required to fast for at least 6 h, and their blood glucose level had to be under 11.1 mmol/L. For 18F-FAPI PET/CT, no specific preparation was requested. The imaging procedures were carried out on a Biography 16 PET/CT scanner (Siemens Healthcare, Erlangen, Germany) one hour after 18F-FDG (~ 0.1 mCi/kg, 370 MBq/kg) or 18F-FAPI (~ 0.1 mCi/kg, 370 MBq/kg) injection. PET image datasets were iteratively reconstructed using an ordered-subset expectation maximization iterative reconstruction by applying CT data for attenuation correction.
Image interpretation
Two experienced nuclear medicine physicians analyzed and interpreted the images in a blinded manner, and in cases of disagreement, a consensus was reached. SUVmax for each lymph node was calculated by placing a spheroid-shaped volume of interest within the node on a multimodality computer platform (Syngo, Siemens, Knoxville, Tennessee, USA). Positive 18F-FDG and 18F-FAPI uptake was defined as focal avidity greater than the background of the mediastinal blood pool. Lymph nodes were assessed using enhanced CT scans, and nodes with short-axis diameters less than 10 mm were defined as small lymph nodes; otherwise, they were defined as large lymph nodes.
Statistical analyses
Data were analyzed by SPSS statistical software (version 25.0, SPSS, IBM Inc., New York, USA). Demographic data and PET/CT parameters were summarized as the mean with standard deviation or frequencies with percentages. The Wilcoxon signed-rank test was used to analyze the differences between PET/CT parameters. P < 0.05 was considered statistically significant, and all analyses were two sided.
Results
Patient characteristics
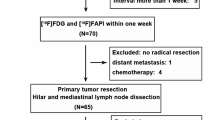
A total of 36 patients with locally advanced lung cancer were registered in the study, and they underwent PET/CT for tumor staging. Four patients had a second primary tumor and 5 patients missed in the follow-up period; these patients were excluded from the study (Fig. 1). Finally, 27 patients with 137 mediastinal and hilar lymph nodes were included. Of the 137 lymph nodes, 106 were mediastinal lymph nodes and 31 were hilar lymph nodes. The clinical characteristics of these patients are shown in Table 1.

Flow diagram shows participant selection details. FAPI fibroblast activation protein inhibitor, FDG fluorodeoxyglucose, 18F = fluorine 18
In the evaluation of the lymph nodes, histopathological examination or contrast-enhanced CT was used. Fourteen nodes in 6 patients were confirmed with pathologic examination, and 123 nodes in 21 patients were confirmed with contrast-enhanced CT before treatment and the follow-up enhanced CT images. Finally, forty-five out of 137 lymph nodes were found to be cancerous, including 32 mediastinal and 13 hilar lymph nodes. In addition, 85 lymph nodes (62%, 85/137) with a short-axis diameter less than 10 mm were defined as small lymph nodes, including 13 metastatic and 72 nonmetastatic lymph nodes.
Improved metastatic lymph node detection with 18F-FAPI PET/CT
In all 137 lymph nodes, the 18F-FAPI-derived SUVmax was 4.80 ± 6.11, and the 18F-FDG-derived SUVmax was 4.33 ± 3.69, p = 0.414. In all 45 metastatic lymph nodes, the mean value of SUVmax on 18F-FAPI PET/CT images was 10.87 ± 7.29, and SUVmax on 18F-FDG PET/CT images was 6.08 ± 5.37, p = 0.001, while in 92 benign lymph nodes, the SUVmax of 68 Ga-FAPI PET/CT was 1.87 ± 1.82, and the SUVmax of 18F-FDG PET/CT was 3.47 ± 2.04, p < 0.001. In summary, 18F-FAPI PET/CT showed a much higher SUVmax value than 18F-FDG PET/CT in metastatic lymph nodes but a much lower SUVmax value than 18F-FDG in benign lymph nodes. Moreover, in 18F-FDG PET/CT, the SUVmax values in metastatic and nonmetastatic lymph nodes presented substantial overlap, although the p-value was less than 0.05. However, in 18F-FAPI PET/CT, there was no overlap, and the p value was less than 0.001, Fig. 2a.

Comparison of the performance of 18F-FAPI and.18F-FDG PET/CT in diagnosing mediastinal and hilar lymph nodes. Comparison of the tracer uptakes a and ROC analysis of SUVmax derived from the two PET/CTs for identifying lymph nodes status b
In addition to the correction between SUVmax and the nature of lymph nodes, the relationship between SUVmax and the diameters of these nodes were compared. However, neither SUVmax of 18F-FAPI nor SUVmax of 18F-FDG had significant correction with the size of nodes (r2 = 0.26 and 0.28, respectively), Fig. 3. In summary, there was a difference between SUVmax of 18F-FAPI and the nature of lymph nodes, but no relationship in SUVmax and lymph node size.

The correction between short diameter of lymph nodes and SUVmax. The correction between short diameter of lymph nodes and 18F-FAPI SUVmax a and.18F-FDG PAPI SUVmax b
Additionally, 18F-FAPI was a superior method in evaluating mediastinal hilar lymph nodes, with a larger area under the receiver operating characteristic (ROC) curve comparing with 18F-FDG (0.901 vs. 0.721). The optimal cutoff value for diagnosis of 18F-FAPI and 18F-FDG PET/CT was 2.5 and 3.4 by ROC analysis, respectively (Fig. 2b). On 18F-FAPI PET/CT, the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value were 84%, 92%, 90%, 84%, and 92%, respectively. In 18F-FDG PET/CT imaging, the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value were 71%, 67%, 69%, 52%, and 83%, respectively (Table 2).
18F-FAPI PET/CT improves the diagnostic accuracy for small metastatic lymph nodes
When small LNs were considered, 18F-FAPI performed much better than 18F-FDG PET/CT. A total of 85 lymph nodes with a short-axis diameter less than 10 mm were confirmed to be small lymph nodes, including 13 metastatic and 72 nonmetastatic nodes. In 18F-FAPI PET/CT, the SUVmax of small metastatic lymph nodes was substantially higher than that of small nonmetastatic lymph nodes (9.29 ± 7.57 vs. 1.67 ± 1.73, p = 0.001). Similarly, the SUVmax based on 18F-FDG was greater in small metastatic lymph nodes than in small nonmetastatic nodes (4.37 ± 1.85 vs. 3.10 ± 1.86, p = 0.001). As a result, 18F-FAPI presented much higher specificity, accuracy, and positive prediction value (PPV) than 18F-FDG PET/CT (specificity: 96% vs. 72%; accuracy: 93% vs. 73%; PPV: 77% vs. 33%, respectively). In 18F-FDG PET, false-positives were observed in 20 patients due to inflammation. However, in 18F-FAPI PET, only 3 false-positives were observed. The diagnostic efficacies of the two procedures are compared in Table 3. A typical case showing false-positive 18F-FDG uptake and true-negative 18F-FAPI uptake in mediastinal and hilar lymph nodes is shown in Fig. 4, and a representative case displaying intense 18F-FAPI but negative 18F-FDG uptake in small metastatic lymph nodes is shown in Fig. 5.

A 79-year-old man with a diagnosis of lung cancer. Lymph nodes in region 4R and 10L with intense 18F-FDG uptake (a, red arrows) and no 18F-FAPI uptake (b, red arrows) were confirmed as nonmetastatic lymph nodes pathologically

A 58-year-old man with a diagnosis of lung cancer. Small (0.7 * 0.7 cm) metastatic lymph nodes in region 4R showed no 18F-FDG-avidity (a, red arrows), but remarkable.18F-FAPI-avidity (b, red arrows)
SUVmax cut-off values for differentiating metastatic from benign lymph nodes
Figure 6 demonstrates the distribution of SUVmax in metastatic and nonmetastatic lymph nodes. In the nonmetastatic group, 90 lymph nodes had the 18F-FAPI SUVmax smaller than 5.3, and only 2 nodes had SUVmax larger than 5.3, resulting in a high specificity (98%). As a result, we evaluated the diagnostic performance of 18F-FAPI when choosing 5.3 as a cut-off value. The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value were 73%, 98%, 90%, 94%, and 88%, respectively. Additionally, mean value is commonly used in data analysis, so we investigated the diagnostic performance when SUVmax was 3.5, which was the mean SUVmax value (Table 4). As aforementioned, 2.5 was also an optimal cutoff value for diagnosis, so we compared the diagnostic performance when the cutoff values were 5.3, 3.5 and 2.5 (Table 4). All the three values demonstrated similar diagnostic accuracy, but when the cut-off value was 5.3, the 18F-FAPI SUVmax could improve specificity and PPV. When the cutoff value was 2.5, SUVmax could improve sensitivity and NPV.

The SUVmax of every lymph node and the optimal cut-off value for the evaluation of metastatic and nonmetastatic lymph nodes. 98% (90/92) nonmetastatic nodes had a 18F-FAPI-derived SUVmax less than 5.3 and 73% (33 of 45) metastatic nodes showed a 18F-FAPI-derived SUVmax larger than 5.3 a. The SUVmax of metastatic nodes derived from.18F-FDG overlapped that of nonmetastatic nodes b
In FDG PET/CT, the values of 3.5 and 5.3 were inapplicable, because the SUVmax of nonmetastatic lymph nodes overlapped with that of metastatic lymph nodes.
Discussion
The present study indicated that 18F-FAPI PET/CT had much higher diagnostic efficacy in mediastinal and hilar lymph nodes in patients with lung cancer, especially in small metastatic lymph nodes (size less than 10 mm), when compared with 18F-FDG. Additionally, two cutoff values were identified in this study. The optimal cut-off value for specificity and PPV of 18F-FAPI SUVmax was 5.3; the optimal cut-off value for sensitivity and NPV was 2.5; this result means that a noninvasive and accurate diagnostic model could be established with 18F-FAPI PET/CT.
A study has shown that intrathoracic nodal status is considered to be positive for metastatic spread if the FDG activity of the node is higher than the mediastinal background [17]; however, a high level of FDG uptake can also be noted in various benign conditions, such as different infective/inflammatory processes [18, 19]. A previous study indicated that a benign mediastinal lymph node with 34.5 mm in size was FDG-avid [20]. In the present study, metastatic lymph nodes had significantly higher FAPI-derived SUVmax than nonmetastatic lymph nodes, but in 18F-FDG PET/CT imaging, although metastatic lymph nodes showed higher uptake than nonmetastatic nodes, the SUVmax in metastatic lymph nodes exhibited substantial overlap that in nonmetastatic lymph nodes. This finding suggested that 18F-FAPI PET/CT may help address the limitation of 18F-FDG in diagnosing lymph nodes and expand the clinical indications of PET/CT. In addition, our study showed that 18F-FAPI PET/CT was more sensitive and specific than 18F-FDG in diagnosing mediastinal and hilar lymph nodes, consistent with previous studies [21]. The variable positive predictive rate for the assessment of mediastinal lymph node involvement with 18F-FDG PET/CT has also been recognized, ranging from 32.3% to 89% [22, 23]. The low and dispersive predictive rate limits the application of 18F-FDG in the assessment of mediastinal lymph nodes, and our results suggest that 18F-FAPI PET/CT might be an alternative imaging technique.
Additionally, according to ACCP evidenced-based clinical practice guidelines, lymph nodes with short-axis diameters larger than 10 mm were considered abnormal lymph nodes [6]. As a result, in the present study, lymph nodes with short-axis diameters less than 10 mm were defined as small lymph nodes. The size of the lymph nodes was an important factor affecting the diagnostic efficiency on imaging scans, including CT and PET/CT scans. For very small lesions (< 10 mm), visibility is low due to the partial volume effect and low tumor metabolic activity [24, 25]. However, previous studies indicated that FAPI PET/CT was better than FDG PET/CT in diagnosing metastatic lymph nodes. A recent study indicated that 68 Ga-FAPI PET/CT had a diagnostic accuracy of 100% in diagnosing metastatic lymph nodes from non-small cell lung cancer, while 18F-FDG had an accuracy of 30% [26]. Lijuan Wang et al. showed that 68 Ga-FAPI detected 356 lymph nodes, while 18F-FDG PET/CT detected 320 nodes, and 22 among the 36 lymph nodes detected only by FAPI PET/CT had a diameter shorter than 10 mm [27]. In the present study, the number of small positive lymph nodes detected by the two PET/CTs was the same, but the specificity and accuracy for diagnosing small lymph nodes were higher for 18F-FAPI than for 18F-FDG. Previous studies indicated that in the earlier stage of metastatic lymph node, the number of tumor cells was small and could not be detected by 18F-FDG [28, 29]. Before tumor cells are located in the lymph nodes, they secrete some factors to promote premetastatic lymph nodes by activating fibroblast reticular cells, which differentiate into CAFs and express high levels of FAP [30,31,32]. This may explain why 18F-FAPI PET/CT is better in detecting small metastatic lymph nodes.
Another important finding of this study is the diagnostic cut-off values. As the pathologic gold standard, the sensitivity of EBUS in mediastinal staging for lung cancer ranges from 45 to 93%, and the NPV was 93% [33]. In this study, using SUVmax 2.5 as the cut-off value, the sensitivity was 84% and the NPV was 92%, which was similar to that of the EBUS method. When the cut-off was 5.3, the specificity and PPV were highly increased. To the best of our knowledge, cut-off values for SUVmax to identify lymph node status have not been investigated previously. Such a reference value may provide a simple, powerful and repeatable clinical tool for the prediction of lymph nodes in patients with lung cancer.
This systematic study investigated the value of 18F-FAPI PET/CT in diagnosing mediastinal and hilar lymph nodes in patients with lung cancer and obtained two optimal values for discriminating metastatic from benign nodes. Our results indicated the value of 18F-FAPI PET/CT in the detection of mediastinal and hilar lymph nodes secondary to lung cancer. However, there were some limitations in this study. First, this was a single-center study with a small sample size. Second, not all lymph nodes were diagnosed by pathology due to the difficulty of obtaining tissue samples. However, the results were obtained with enhanced CT and follow-up.
Conclusion
18F-FAPI showed promising diagnostic efficiency in metastatic mediastinal and hilar lymph nodes from lung cancer patients with a better sensitivity and negative predictive value, particularly in small nodes (size less than 10 mm), than 18F-FDG. Additionally, this preliminary study proposed optimal cutoff values of 5.3 to distinguish nonmetastatic from metastatic nodes, which could obtain a similar sensitivity of 94.29% with EBUS and a much higher NPV of nonmetastatic LNs.
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- FAP:
-
Fibroblast activation protein
- FAPI:
-
Fibroblast activation protein inhibitor
- 18F-FDG:
-
Fluorine 18 fluorodeoxyglucose
- 18F-FAPI:
-
Fluorine 18-labeled fibroblast activation protein inhibitor
- SUVmax:
-
Maximum standardized uptake value
- PPV:
-
Positive predictive value
- NPV:
-
Negative predictive value
References
Oliver AL. Lung cancer: epidemiology and screening. Surg Clin North Am. 2022;102:335–44. https://doi.org/10.1016/j.suc.2021.12.001.
Ettinger DS, Wood DE, Akerley W, Bazhenova LA, Borghaei H, Camidge DR, et al. Non-small cell lung cancer version 62015. J Natl Compr Canc Netw. 2015. https://doi.org/10.6004/jnccn.2015.0071.
Jalil BA, Yasufuku K, Khan AM. Uses, limitations, and complications of endobronchial ultrasound. Proc (Bayl Univ Med Cent). 2015;28:325–30. https://doi.org/10.1080/08998280.2015.11929263.
Schmid-Bindert G, Jiang H, Kähler G, Saur J, Henzler T, Wang H, et al. Predicting malignancy in mediastinal lymph nodes by endobronchial ultrasound: a new ultrasound scoring system. Respirology. 2012;17:1190–8. https://doi.org/10.1111/j.1440-1843.2012.02223.x.
Silvestri GA, Tanoue LT, Margolis ML, Barker J, Detterbeck F. The noninvasive staging of non-small cell lung cancer: the guidelines. Chest. 2003;123:147s-s156. https://doi.org/10.1378/chest.123.1_suppl.147s.
Silvestri GA, Gould MK, Margolis ML, Tanoue LT, McCrory D, Toloza E, et al. Noninvasive staging of non-small cell lung cancer: ACCP evidenced-based clinical practice guidelines. Chest. 2007. https://doi.org/10.1378/chest.07-1360.
Fréchet B, Kazakov J, Thiffault V, Ferraro P, Liberman M. Diagnostic accuracy of mediastinal lymph node staging techniques in the preoperative assessment of nonsmall cell lung cancer patients. J Bronchology Interv Pulmonol. 2018;25:17–24. https://doi.org/10.1097/lbr.0000000000000425.
Kandathil A, Kay FU, Butt YM, Wachsmann JW, Subramaniam RM. Role of FDG PET/CT in the of TNM staging of non-small cell lung cancer. Radiographics. 2018. https://doi.org/10.1148/rg.2018180060.
González-Cruz C, Bodet D, Muñoz-Couselo E, García-Patos V. Mediastinal FDG-positive lymph nodes simulating melanoma progression: drug-induced sarcoidosis like/lymphadenopathy related to ipilimumab. BMJ Case Rep. 2021. https://doi.org/10.1136/bcr-2020-237310.
Shang Q, Zhao L, Pang Y, Meng T, Chen H. Differentiation of reactive lymph nodes and tumor metastatic lymph nodes With 68Ga-FAPI PET/CT in a patient with squamous cell lung cancer. Clin Nucl Med. 2022;47:458–61. https://doi.org/10.1097/rlu.0000000000003998.
Guglielmo P, Guerra L. Radiolabeled fibroblast activation protein inhibitor (FAPI) PET in oncology: has the time come for 18F-fluorodeoxyglucose to think to a well-deserved retirement? ClinTransl Imaging. 2021;9:1–2. https://doi.org/10.1007/s40336-020-00402-z.
Çermik TF, Ergül N, Yılmaz B, Mercanoğlu G. Tumor imaging with 68Ga-DOTA-FAPI-04 PET/CT: comparison with 18F-FDG PET/CT in 22 different cancer types. Clin Nucl Med. 2022;47:e333–9. https://doi.org/10.1097/rlu.0000000000004073.
Kratochwil C, Flechsig P, Lindner T, Abderrahim L, Altmann A, Mier W, et al. (68)Ga-FAPI PET/CT: tracer uptake in 28 different kinds of cancer. J Nucl Med. 2019;60:801–5. https://doi.org/10.2967/jnumed.119.227967.
Giesel FL, Adeberg S, Syed M, Lindner T, Jiménez-Franco LD, Mavriopoulou E, et al. FAPI-74 PET/CT using either (18)F-AlF or Cold-Kit (68)Ga labeling: biodistribution, radiation dosimetry, and tumor delineation in lung cancer patients. J Nucl Med. 2021;62:201–7. https://doi.org/10.2967/jnumed.120.245084.
Pang Y, Zhao L. Comparison of (68)Ga-FAPI and (18)F-FDG uptake in gastric. Duodenal Colorectal Cancers. 2021;298:393–402. https://doi.org/10.1148/radiol.2020203275.
Kou Y, Jiang X, Yao Y, Shen J, Jiang X, Chen S, et al. Physiological tracer distribution and benign lesion incidental uptake of Al18F-NOTA-FAPI-04 on PET/CT imaging. Nucl Med Commun. 2022;43:847–54. https://doi.org/10.1097/mnm.0000000000001563.
Gunluoglu MZ, Melek H, Medetoglu B, Demir A, Kara HV, Dincer SI. The validity of preoperative lymph node staging guidelines of European society of thoracic surgeons in non-small-cell lung cancer patients. Eur J Cardiothorac Surg. 2011;40:287–90. https://doi.org/10.1016/j.ejcts.2010.11.030.
Ding RL, Cao HY, Hu Y, Shang CL, **e F, Zhang ZH, et al. Lymph node tuberculosis mimicking malignancy on (18)F-FDG PET/CT in two patients: a case report. Exp Ther Med. 2017;13:3369–73. https://doi.org/10.3892/etm.2017.4421.
Maccarone MT. FDG-PET Scan in sarcoidosis: clinical and imaging indications. Curr Med Imaging Rev. 2019;15:4–9. https://doi.org/10.2174/1573405614666180626120832.
T Fujiwara T Nakajima. The combination of endobronchial elastography and sonographic findings during endobronchial ultrasound-guided transbronchial needle aspiration for predicting nodal metastasis. 2019;10:2000-5. https://doi.org/10.1111/1759-7714.13186
Qin C, Shao F, Gai Y, Liu Q, Ruan W, Liu F, et al. (68)Ga-DOTA-FAPI-04 PET/MR in the evaluation of gastric carcinomas: comparison with (18)F-FDG PET/CT. J Nucl Med. 2022;63:81–8. https://doi.org/10.2967/jnumed.120.258467.
Lin WY, Hsu WH, Lin KH, Wang SJ. Role of preoperative PET-CT in assessing mediastinal and hilar lymph node status in early stage lung cancer. J Chin Med Assoc. 2012;75:203–8. https://doi.org/10.1016/j.jcma.2012.04.004.
Nakanishi K, Nakamura S, Sugiyama T, Kadomatsu Y, Ueno H, Goto M, et al. Diagnostic utility of metabolic parameters on FDG PET/CT for lymph node metastasis in patients with cN2 non-small cell lung cancer. BMC Cancer. 2021;21:983. https://doi.org/10.1186/s12885-021-08688-6.
Spadafora M, Pace L, Evangelista L, Mansi L, Del Prete F, Saladini G, et al. Risk-related (18)F-FDG PET/CT and new diagnostic strategies in patients with solitary pulmonary nodule: the ITALIAN multicenter trial. Eur J Nucl Med Mol Imaging. 2018;45:1908–14. https://doi.org/10.1007/s00259-018-4043-y.
Redondo-Cerezo E, Martínez-Cara JG, Jiménez-Rosales R, Valverde-López F, Caballero-Mateos A, Jérvez-Puente P, et al. Endoscopic ultrasound in gastric cancer staging before and after neoadjuvant chemotherapy a comparison with PET-CT in a clinical series. United Eur Gastroenterol J. 2017;5:641–7. https://doi.org/10.1177/2050640616684697.
Zhou X, Wang S, Xu X, Meng X, Zhang H, Zhang A, et al. Higher accuracy of [(68) Ga]Ga-DOTA-FAPI-04 PET/CT comparing with 2-[(18)F]FDG PET/CT in clinical staging of NSCLC. Eur J Nucl Med Mol Imaging. 2022;49:2983–93. https://doi.org/10.1007/s00259-022-05818-5.
Wang L, Tang G. Comparison of (68)Ga-FAPI and (18)F-FDG PET/CT in the evaluation of advanced lung cancer. Radiolog. 2022. https://doi.org/10.1148/radiol.211424.
Stahlie EHA, van der Hiel B, Bruining A, van de Wiel B, Schrage YM, Wouters M, et al. The value of lymph node ultrasound and whole body (18)F-FDG PET/CT in stage IIB/C melanoma patients prior to SLNB. Eur J Surg Oncol. 2021;47:1157–62. https://doi.org/10.1016/j.ejso.2020.12.007.
Calais J, Mona CE. Will FAPI PET/CT replace FDG PET/CT in the next decade? point-an important diagnostic, phenotypic, and biomarker role. AJR Am J Roentgenol. 2021;216:305–6. https://doi.org/10.2214/ajr.20.24302.
Rovera C, Berestjuk I,Lecacheur M. 2022. Secretion of IL1 by Dedifferentiated Melanoma Cells Inhibits JAK1-STAT3-Driven Actomyosin Contractility of Lymph Node Fibroblastic Reticular Cells. https://doi.org/10.1158/0008-5472.CAN-21-0501
Nizri E, Bar-David S, Aizic A, Sternbach N, Lahat G, Wolf I, et al. Desmoplasia in lymph node metastasis of pancreatic adenocarcinoma reveals activation of cancer-associated fibroblasts pattern and T-helper 2 immune cell infiltration. Pancreas. 2019;48:367–73. https://doi.org/10.1097/mpa.0000000000001261.
Itou RA, Uyama N, Hirota S, Kawada N, Wu S, Miyashita S, et al. Immunohistochemical characterization of cancer-associated fibroblasts at the primary sites and in the metastatic lymph nodes of human intrahepatic cholangiocarcinoma. Hum Pathol. 2019;83:77–89. https://doi.org/10.1016/j.humpath.2018.08.016.
Vilmann P, Clementsen PF, Colella S, Siemsen M, De Leyn P, Dumonceau JM, et al. Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer: european society of gastrointestinal endoscopy (ESGE) guideline, in cooperation with the european respiratory society (ERS) and the European society of thoracic surgeons (ESTS). Endoscopy. 2015;47:545–59. https://doi.org/10.1055/s-0034-1392040.
Acknowledgements
We thank all the staff at the Department of Nuclear Medicine in our center for their excellent technical assistance. We would also like to thank the multidisciplinary team in our hospital for the great help to our work.
Funding
This research was supported by Pudong New area science and technology development foundation (No. PKJ2018-Y49), Pudong New area science and technology development foundation (No. PKJ 2020-Y56), and Natural Science Foundation of Shanghai (21ZR460300).
Author information
Authors and Affiliations
Contributions
YS, YS and JC contributed to the study conception and design; Material preparation, data collection and analysis were performed by all authors. The first draft of the manuscript was written by YS and YS. JC and JM revised the manuscript with constructive ideas. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the institutional review board (IRB) of the Shanghai Proton and Heavy Ion Center (SPHIC) (Ethical Code: 2106-49-01). Informed consent was obtained from all individual participants included in the study.
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sun, Y., Sun, Y., Li, Z. et al. 18F-FAPI PET/CT performs better in evaluating mediastinal and hilar lymph nodes in patients with lung cancer: comparison with 18F-FDG PET/CT. Eur J Med Res 29, 9 (2024). https://doi.org/10.1186/s40001-023-01494-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01494-9