
Abstract
Background
Mandible tumors are very rare. One of the main methods of the treatments is resection of the tumor and then reconstruction of the mandible. The donor site is often distant tissue—fibula or ilium. Following this, it is necessary to improve the patient in two ways, on one hand restoring the function of the mandible, and on the other hand, improving the donor site area. For that reason, physiotherapy after tumor resection and reconstruction of the mandible is very complicated. The aim of this bibliographic review was to find the methods of the reconstruction of the mandible in the context of patients’ functional assessment after surgeries to create effective physiotherapeutic procedures in the feature.
Methods
PEDro, Medline (PubMed), Cochrane Clinical Trials were searched.
Results
767 articles were found. 40 articles were included to this literature review.
Conclusions
Authors showed different kinds of surgeries strategy for patients with tumors of the mandible. They also showed manners of patients’ functional assessment in the localization of transplantation and donor site. It could be useful for physiotherapists during planning of comprehensive physiotherapy.
Similar content being viewed by others

Introduction
Primary tumors are one of the rarest and enhance 3% of all bone tumors [1]. They are also a small percentage of all cancers in the pediatric population. One should pay attention that their development is connected with bone growth retardation, appearing big deformation of the face, and also the necessity of conducting of complicated surgeries with the transplantation of tissues simultaneously [2]. The location of odontogenic tumors such as odontoma or ameloblastoma is most often the interior of the jaw bone or the surrounding soft tissues [1, 3, 4]. These tumors are formed from inactive cells forming the teeth (enamel, dentine, pulp) and jaw bones and the moment of their formation may coincide with the development of the oral cavity [4]. On the other hand, non-odontogenic tumors, such as central giant cell granulomas or fibro-osseous lesions, are formed from bone or mesenchymal tissue and are often malignant [3,4,5]. The etiology of mandibular tumors remains unknown, which often makes accurate diagnosis difficult [1, 5]. Currently, the most commonly used and most effective method of treating pathological changes in the mandible is its partial resection with simultaneous reconstruction in the form of free flaps most often fibula or the wing of ilium [6,7,8]. In the case of malignant tumors, adjuvant radiotherapy or chemotherapy is also used [7]. Reconstructive surgery brings not only benefits such as the reconstruction of the removed part of the mandible but is also burdened with some risks and complications resulting from the collection of tissues from other areas of the body. In the case of taking a graft from the fibula, patients often report pain and sensory disturbances at the donor site, as well as a feeling of ankle instability [9, 10]. In some patients, a clear decrease in gait speed, contracture of the flexor hallucis longus, limitation of the range of motion of the dorsal and plantar flexion in the ankle joint, as well as muscle weakness or contracture of the toes can be seen [9, 11, 12]. On the other hand, people undergoing reconstruction with iliac crest free flap collection struggle with limitation of the range of motion in the hip joint or stiffness of the Achilles tendon [13, 14]. The aim of the study was to review the methods of mandibular reconstruction with particular emphasis on the functional assessment after transplantation, both in the context of the mandible function and the function of the donor site, which may be the basis for future programming of physiotherapeutic procedures. Attention was paid to the possible effects of transplants and their impact on the possibilities of rehabilitation procedures.
Materials and methods
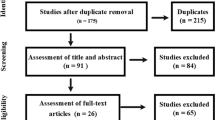
PEDro, Medline (PubMed), Cochrane Clinical Trials database were searched. Different combinations of the keywords were used: mandibular cancer, mandibular tumor, mandibular tumour, jaw cancer, jaw tumor, jaw tumour, treatment, therapy, reconstruction, physiotherapy, physical therapy, scar, fibula free flap, costal graft, rib graft, scapula graft, occlusion, complication, gait, assessment, evaluation, function. The research started with the main phrase: ((treatment OR therapy) AND (child* OR pediatric*) AND ((mandibular cancer*) OR (mandibular tumor*) OR (mandible cancer*) OR (mandible tumor*) OR (jaw* cancer*) OR (jaw* tumor*))). Then, due to the small number of publications found, additional phrases were used: ((mandible) AND (reconstruction) AND (physiotherapy)), (jaw) AND (reconstruction) AND (physiotherapy)), ((physical therapy) AND (mandible) AND (reconstruction)), ((mandible reconstruction) AND (scar), ((free flap iliac) AND (mandibula*)), ((rib graft) AND (mandibula*)), ((costal graft) AND (mandibula*)), ((scapula graft) AND (mandible*)), ((costal graft) AND (physiotherapy)), ((rib graft) AND (physiotherapy)), ((scapula graft) AND (physiotherapy)), ((free flap) AND (physiotherapy)), ((occlusion) AND (mandible reconstruction)), ((complication) AND (mandible reconstruction)), ((gait) AND (mandible reconstruction)), ((gait) AND (free flap)), ((mandible reconstruction) AND ((assessment) OR (evaluation))), ((mandible reconstruction) AND (function)). Due to the significantly limited number of publications related to the topic above and the high heterogeneity of research, the qualitative assessment of the found publications was omitted. Inclusion criteria were clinical trials and case studies concerning mandibular reconstruction methods in populations where the majority of the patients had oncological diagnosis within the mandible. Selected studies could use any surgical protocols during reconstruction procedures, as well as any method of assessing the patient's postoperative condition, including short-term and/or long-term effects. Articles in Polish and English, which were published in the years 2015–2022, were analyzed. All the articles which were meta-analyses, systematic reviews, included non-autologous transplants, did not contain postoperative and/or short-term and/or long-term assessment of the patient's condition were excluded. Figure 1 summarizes the search results.

Summary of the search results
Results
40 articles were qualified for the bibliographic review. They described the surgical procedure, the function of the mandible, mouth, speech apparatus, esophagus assessed by the researchers, as well as the function associated with the donor site and in some cases other ailments accompanying patients after mandibular reconstruction. The most frequently mentioned methods of mandibular reconstruction in the literature were those using fibula free flap and iliac crest free flap. A detailed summary of the included articles is in Tables 1, 2, 3.
Evaluation of the jaw, mouth, speech apparatus, esophagus function
In the articles selected for review, the authors most often made a functional assessment directly related to the place after mandibular reconstruction. The evaluation referred among others to the range of mouth opening, chewing, swallowing, speech quality, speech understanding and tongue mobility. In most instances, function control is based on subjective patients’ assessment using standardized scales and questionnaires such as the Functional Intraoral Glasgow Scale, Head and Neck Performance Status Scale, University of Washington Quality-of-Life, Oral Health Impact Profile, Eating Ability Evaluation Questionnaire, or 14-item Oral Health Impact Profile Questionnaire [15,16,17,18,19,20]. Methods of objective function assessment, such as measurements of the range of mouth opening or measurements of bite strength, appeared much less frequently in research [21,22,23]. Sakuraba et al. [22] assessed the mandible function taking into account not only the subjective feelings of the patient but also the objectified measurements using the GM10 bite force meter. This gauge was placed between the first premolar and the second molar. However, bilateral measurement comparing the healthy and transplanted sides was only possible in 9 patients and the result was the average of 5 trials. On the healthy side, the mean strength in individual patients was between 88.6 N and 383.2 N, while on the transplanted side only 12.4 N to 73.6 N, indicating a significant weakening of the bite force on the transplanted side of the mandible. In a similar way, the bite strength was also assessed by Bouchet et al. [15]. Using FlexiForce, they made 5 measurements for each patient and averaged the results, obtaining bite strength for the healthy side and the transplanted side. The strength for the healthy side was between 160 and 563 N, and for the transplanted side between 50 and 462 N, which also indicated a significant reduction in strength on the transplanted side of the mandible. Yamamoto [24] compared the strength of the occlusion before resection and reconstruction of the mandible with the condition after surgery. The results indicated a significant improvement in bite strength, however, the publication does not specify the measuring tool that was used to conduct the study. Chewing performance was also investigated in a relatively objective manner in the Zhang et al. [25] study. Patients underwent a Masticatory performance test consisting of chewing 5 g of peanuts, rinsing the mouth, spitting its contents into a measuring cylinder, and then sifting through a mesh with 2 mm holes. Based on the weight of the food residues on the mesh, the result of chewing efficiency was given as a percentage and indicated a significant deterioration in chewing performance after the procedure. In the same study, patients were also asked to subjectively assess chewing sensations using the University of Washington quality of life questionnaire [25]. It also confirmed a significant deterioration in chewing function. An important objective parameter assessed by the other researchers was also the range of mouth opening, which in the examined patients ranged from 2 to 9.5 cm [15, 17, 21, 23, 26,27,28,29]. Generally, these values indicated an improvement in the extent of oral opening compared to the state before surgery, but not in all patients [26]. The significance of the functioning of the mouth, mandible, and speech apparatus was also the subject of research by other authors, but their tools of assessment were mostly questionnaires and scales [30,31,32,33,34,35,36,37,38]. An interesting fact is a discrepancy among the assessments of patients after the procedure, ranging from excellent speech and swallowing function, through good and acceptable jaw function, to difficulties during chewing and swallowing food.
Evaluation of the global function associated with the donor site
The authors of the selected study also performed a functional assessment of the patient related to the donor site. Most often it is an assessment of the function of the lower limb due to the fact of taking a graft from the fibula or iliac crest free flap. Among all selected articles, 4 presented a comprehensive description of the patients’ condition related to the possibilities of moving and performing activities of everyday life. It is worth noting that only in these publications did the authors use objective assessment tools such as a dynamometer, Footscan platform, or mechanographic platform. An extensive analysis of lower limb function can be found in the article by Rendenbach et al. [39], in which patients underwent mandibular reconstruction with fibula free flap. The subjects were subjected to the evaluation of jump mechanography, which included its height, speed, as well as maximum force, and peak power. The results of the analysis showed a significant reduction in the height of the jump. On the other hand, the examination of maximum peak strength and power showed a decrease in values in both donor and untreated limbs, but these differences were not significant. In the case of both limbs, there was also an increase in the number of motions in the anteroposterior direction in the one-leg standing, but most of these results were statistically insignificant. Significant imbalances were noted only in the anteroposterior direction. The range of motion of the ankle joint was clearly decreased in dorsal and plantar flexion. A year later, Rendenbach et al. [14] also analyzed the function of patients whose mandibular reconstruction was performed from the iliac crest free flap. Although the assessment of the subjects on the Esslinger Fitness Index scale, in jum** tests, the test of getting up from the chair, and the balance test showed no significant differences before and after the procedure. There was a significantly worse range of motion of the hip joint, limitation of mobility in the lumbar spine, as well as occasional limitations of everyday activities such as getting up from sitting or lying down, or playing sports. The subjects did not complain about lim** and sensory disturbances. Xu et al. [40] assessed lower limb function before surgery and then 3, 6, and 9 months after surgery. Among other things, they investigated the peak torque/weight for the ankle joint using an isokinetic dynamometer at angular velocity of 30, 60, and 90 degrees per second. The results clearly indicated a significant decrease in torque of the plantar and dorsal flexion of the ankle joint. Electromyography examination was also performed on the patient's calf in the area of the superficial peroneal nerve. In some patients, the conduction velocity and response amplitude dropped by almost half. Also, the response peak latency was doubled. Gait analysis was also carried out using the Footscan platform reporting the occurrence of asymmetry and changes in pressure distribution during standing and movement. In statics, in the donor limb, a clear transfer of the pressure to the heel part of the sole was shown. On the other hand, in the second limb, a significant increase in metatarsal pressure was noted. The other authors focused mainly on collecting data from the subjective patients’ assessment, in which the vast majority did not report major complications associated with collection. Some patients had slight limitations in the performance of everyday activities or weakness of the donor limb [14, 39, 41].
Other ailments evaluation
The authors of the selected articles made an additional assessment that also included other complaints reported by patients. They concerned both the craniofacial area and donor sites. These included sensory disturbances in the lips and graft area, or pain in the oral cavity [15,16,17, 20, 34, 42]. Some patients also experienced neuropathic pain or local pain in the limb, as well as sense weakness in the donor site area or complete loss of sense along the peroneal nerve [14, 20, 40, 41, 43,44,45,46]. In some cases, scar hypertrophy, cold sensitivity at the donor site, and femoral nerve palsy also occurred [13, 40, 47].
Discussion
The basis for effective treatment of any patient with planned tumor resection and subsequent mandible reconstruction should be the ability of the evaluation and prediction not only the short- but also long-term effects of surgeries in the context of the patients’ functioning. The mandibular reconstruction procedure is an extremely complicated procedure itself which is constantly being improved, among others through the use of 3D planning technology or computer-aided design and manufacturing during reconstruction surgery (CAD-CAM) [15, 48, 49]. In addition to the development of treatment technology, the methods of patients’ function assessing should also be developed. Whatis worth mentioning is that the aim of the vast majority of studies published in the years 2015–2022 was to describe the course of reconstruction and assess the patient’s condition immediately after the procedure to detect early postoperative complications such as wound infection, correct healing, hematomas or fistulas, and not a long-term assessment of the function of the mouth, temporomandibular joint and donor site [50]. After analyzing the collected articles, in the assessment of the long-term functioning of patients, one can notice a tendency of the authors to take into account largely only subjective assessments of patients on the basis of scales and questionnaires. On one hand, this is a positive tendency, because it puts the patient's feelings first, but from a scientific point of view, it is unreliable and not very objective. There is a definite lack of studies that assess the patient's function using objective tools that give results in the form of specific numerical values that allow intragroup and intergroup comparisons. An example is the study of subjective feelings of patients (instead of making objective measurements) in the assessment of ankle instability or decrease in muscle strength [10]. However, the least discussed topic is the objective assessment of the temporomandibular joint. A possible reason is the lack of technologically advanced equipment that would enable an objective examination of the patient. For example, among the selected articles, only one team assessed bite strength using a dedicated device [22]. Other assessments were carried out using modified devices and adapted to a specific study or with the help of original tests [15, 46]. The assessment of the patient's function itself is certainly an extremely important task, but the fact of what will happen to this knowledge in the next stage of restoring the patient to full fitness seems equally important. Sakuraba et al. [22] and Bouchet et al. [15] indicated a significant weakening of the bite force on the reconstructed side of the mandible, while Rendenbach et al. [39] mentioned significantly reduced lower limb strength and gait problems in some transplant patients. For physiotherapists, this may be a field for work on improving the measured parameters, and ultimately it may also have its effect in improving patients' satisfaction with the chewing or movement function. Early postoperative assessment of the patient is particularly important due to the possibility of complications of the transplanted site associated with potential blood supply disorders or its necrosis [51, 52], but later in the postoperative period, physiotherapists could assess the holistic patient's function and, on this basis, begin to introduce adequate rehabilitation. Some studies encompass postoperative physiotherapy of the patient, including the improvement of the function of the oral cavity and temporomandibular joint, or the improvement of the function of the lower limb as a donor site [14, 27, 30, 41, 53]. Taking into account the above considerations and the goal set for physiotherapy, its planning should be based on an objective assessment both in terms of functional and morphological changes, not only within the transplanted fragment of the mandible and adjacent areas, but also within the donor site. This is due to the fact that many researchers and patients subjectively notice deficits in functioning after treatment. However, to address the existing limitations, an objective assessment should be carried out, which is lacking in the published literature. Taking into account the complaints reported by patients noted in the lists above it would be possible to propose as a standard: an objective assessment of structural changes within the foot (claw toe), assessment of changes in gait parameters, examination of TMJ function, examination of possible imbalances and distribution of the general center of mass, examination of strength and muscle mass. Evaluation of the above parameters, performed with validated measuring devices, could indicate direct improvement needs involving both TMJ function and the donor area.
Summary
The review shows different strategies for the treatment of mandible tumors, the most popular of which were reconstructions using fibula free flap and iliac crest free flap and furthermore different methods of functional assessment resulting from measurement techniques within the face and the donor site. However, to a large extent, the authors devote attention to subjective assessments of the postoperative condition of patients, omitting in many cases an objective assessment. The analyzed literature also does not indicate clear directions of postoperative physiotherapy of patients, however, on its basis it can be assumed that patients should undergo comprehensive rehabilitation including improvement of the function of the jaw, TMJ, soft tissues of the head and neck, as well as activities related to the rehabilitation of the donor site. From the physiotherapy point of view, this creates real benefits for planning a comprehensive rehabilitation procedure involving the activation of the mandible, TMJ along with soft tissues, as well as the distant area, constituting donor sites for tissue acquisition. Some researchers assessed the function or facial aesthetics of their patients for a period ranging from six months to even 38 years after surgery [14, 16, 17, 19,20,21,22,23,24,25,26,27, 30, 32,33,34,35, 37, 40, 43,44,45,46, 53,54,55]. Such a long-term analysis may be important for physiotherapists in terms of reliable assessment of the patient's condition at individual stages of rehabilitation. Because of the fact that these treatments could be introduced, the quality of patients' lives will effectively improve, however, more research is needed in this area.
Availability of data and materials
Not applicable.
References
Dabholkar JP, Vora K, Vaidya A, Sharma A. Benign jaw tumors. Indian J Otolaryngol Head Neck Surg. 2009;61(3):240–4.
Akhiwu BI, Osunde DO, Akhiwu HO, Aliyu I, Omeje KU, Ojukwu B, et al. Paediatric jaw tumours: experiences and findings from a resource limited tertiary health care center. Pan Afr Med J. 2020;36:111.
McCarthy EF. Fibro-Osseous lesions of the maxillofacial bones. Head Neck Pathol. 2013;7(1):5–10.
Perry KS, Tkaczuk AT, Caccamese JF, Ord RA, Pereira KD. Tumors of the pediatric maxillofacial skeleton. Otolaryngol Head Neck Surg. 2015;141(1):40.
Dyalram D, Aslam-Pervez N, Lubek JE. Nonodontogenic tumors of the jaws. Oral Maxillofac Surg Clin North Am. 2016;28(1):59–65.
Brown JS, Lowe D, Kanatas A, Schache A. Mandibular reconstruction with vascularised bone flaps: A systematic review over 25 years. Br J Oral Maxillofac Surg. 2017;55(2):113–26.
Petrovic I, Ahmed ZU, Hay A, Rosen EB, Lu C, Hameed M, et al. Sarcomas of the mandible. J Surg Oncol. 2019;120(2):109–16.
Vacher C, Lkah C. The osteomuscular dorsal scapular (OMDS) flap: an alternative technique of mandibular reconstruction. J Plast Reconstr Aesthet Surg. 2010;63(2):198–204.
Bodde EWH, De Visser E, Duysens JEJ, Hartman EHM. Donor-site morbidity after free vascularized autogenous fibular transfer: Subjective and quantitative analyses. Plast Reconstr Surg. 2003;111(7):2237–42.
Momoh AO, Yu P, Skoracki RJ, Liu S, Feng L, Hanasono MM. A prospective cohort study of fibula free flap donor-site morbidity in 157 consecutive patients. Plast Reconstr Surg. 2011;128(3):714–20.
Sagalongos OS, Valerio IL, Hsieh CH, Kuo YR, Wang LY, Rong LH, et al. Qualitative and quantitative analyses of donor-site morbidity following suprafascial versus subfascial free fibula flap harvesting. Plast Reconstr Surg. 2011;128(1):137–45.
Sassu P, Acland RD, Salgado CJ, Mardini S, Ozyurekoglu T. Anatomy and vascularization of the flexor hallucis longus muscle and its implication in free fibula flap transfer. Ann Plast Surg. 2010;64(2):233–7.
Li H, Tan MDM, Alexander S, Grinsell D, Ramakrishnan A. Comparative osteoradionecrosis rates in bony reconstructions for head and neck malignancy. J Plast Reconstr Aesthet Surg. 2019;72(9):1478–83.
Rendenbach C, Goehler F, Hansen L, Kohlmeier C, Amling M, Hanken H, et al. Evaluation of long-term functional donor-site morbidity after deep circumflex iliac crest artery bone flap harvest. Microsurgery. 2018;39(4):304–9.
Bouchet B, Raoul G, Julieron B, Wojcik T. Functional and morphologic outcomes of CAD/CAM-assisted versus conventional microvascular fibular free flap reconstruction of the mandible: a retrospective study of 25 cases. J Stomatol Oral Maxillofac Surg. 2018;119(6):455–60.
Gravvanis A, Anterriotis D. Kakagia D Mandibular condyle reconstruction with fibula free-tissue transfer. J Craniofac Surg. 2017;28(8):1955–9.
Jarefors E, Hansson T. Functional outcome in 17 patients whose mandibles were reconstructed with free fibular flaps. J Plast Surg Hand Surg. 2016;51(3):178–81.
Okoturo E. Non-vascularised iliac crest bone graft for immediate reconstruction of lateral mandibular defect. Oral Maxillofac Surg. 2016;20(4):425–9.
Olvera-Caballero C, Cortes-Aroche S, Vazquez-de-Lara LG. Functional and aesthetic osseous free flap mandible reconstruction using a low-cost method. Plast Reconstr Surg Glob Open. 2019;7(11): e2465.
Zavala A, Ore JF, Broggi A, De Pawlikowski W. Pediatric mandibular reconstruction using the vascularized fibula free flap. Ann Plast Surg. 2021;87(6):662–8.
Lv M, Yang X, Gupta A, Shen Y, Li J, Sun J. Sequential application of novel guiding plate system for accurate transoral mandibular reconstruction. Oral Oncol. 2020;111: 104846.
Sakuraba M, Miyamoto S, Fujiki M, Higashino T, Oshima A, Hayashi R. Analysis of functional outcomes in patients with mandible reconstruction using vascularized fibular grafts. Microsurgery. 2015;37(2):101–4.
Zhang C, Zeng Y, Zhou L, Tang X. The application of chimeric deep circumflex iliac artery perforator flap for oromandibular reconstruction. Medicine. 2021;100(14): e25458.
Yamamoto N, Morikawa T, Yakushiji T, Shibahara T. Mandibular reconstruction with free vascularized fibular graft. Bull Tokyo Dent Coll. 2018;59(4):299–311.
Zhang J, Wang Y, Yuan L, Wang W. Masticatory performance in patients undergoing free fibula flap for mandible reconstruction. BMC Oral Health. 2022;22(1):78.
Devireddy SK, Senthil Murugan M, Kishore Kumar RV, Gali R, Kanubaddy SR, Sunayana M. Evaluation of non-vascular fibula graft for mandibular reconstruction. J Oral Maxillofac Surg. 2015;14(2):299–307.
Dowgierd K, Pokrowiecki R, Borowiec M, Kozakiewicz M, Smyczek D, Krakowczyk Ł. A protocol for the use of a combined microvascular free flap with custom-made 3d-printed total temporomandibular joint (TMJ) prosthesis for mandible reconstruction in children. Appl Sci. 2021;11(5):2176.
Johnson OK. Sharma K Ameloblastoma resection with immediate rib reconstruction: Addressing the problem of mandibular angle and central bone bulk. Trop Doct. 2017;47(4):384–8.
Zheng L, Wu W, Shi Y, Zhang J. Mandibular reconstruction with a deep circumflex iliac artery flap using computer-assisted and intraoral anastomosis techniques. J Oral Maxillofac Surg. 2019;77(12):2567–72.
Abramowicz S, Goudy SL, Mitchell CE, Prickett K, Marchica C, Austin TM, et al. A protocol for resection and immediate reconstruction of pediatric mandibles using microvascular free fibula flaps. J Oral Maxillofac Surg. 2020;79(2):475–82.
Askin SB, Aksu AE, Calis M, Tulunoğlu I, Safak T, Tözüm TF. Report of multidisciplinary treatment of an extensive mandibular ameloblastoma with free iliac crest bone flap, dental implants, and acellular dermal matrix graft. J Oral Implantol. 2015;41(1):107–11.
Comini LV, Mannelli G, Tamburini A, Innocenti M, Spinelli G. Pediatric malignant mandibular tumors: Personal experience and literature options discussion. Orl. 2021;83:263–71.
Guo B, Fang X, Shan Y, Li J, Shen Y, Ma C. Salvage mandibular reconstruction: multi-institutional analysis of 17 patients. Int J Oral Maxillofac Surg. 2021;51(2):191–9.
Hu Y, Cao R, Wang Z, Hong W, Zheng C. Reconstruction of deep circumflex iliac artery free flap for multiple recurrent ameloblastoma in mandible. J Craniofac Surg. 2019;30(2):557–62.
Khachatryan L, Khachatryan G, Hakobyan G. The treatment of lower jaw defects using vascularized fibula graft and dental implants. J Craniofac Surg. 2018;29(8):2214–7.
Lin B, Yang H, Yang H, Shen S. Vascularized combined with nonvascularized fibula flap for mandibular reconstruction. J Craniofac Surg. 2019;30(4):e365–9.
Tarsitano A, Battaglia S, Ramieri V, Cascone P, Ciocca L, Scotti R, et al. Short-term outcomes of mandibular reconstruction in oncological patients using a CAD/CAM prosthesis including a condyle supporting a fibular free flap. J Craniomaxillofac Surg. 2017;45(2):330–7.
Tian T, Zhang T, Ma Q, Zhang Q, Cai X. Reconstruction of mandible: a fully digital workflow from visualized iliac bone grafting to implant restoration. J Oral Maxillofac Surg. 2017;75(7):1403.e1-1403.e10.
Rendenbach C, Rashad A, Hansen L, Kohlmeier C, Dyck ML, Suling A, et al. Functional donor site morbidity longer than one year after fibula free flap: a prospective biomechanical analysis. Microsurgery. 2017;38(4):395–401.
Xu ZF, Bai S, Zhang ZQ, Duan WY, Wang ZQ, Sun CF. A critical assessment of the fibula flap donor site. Head Neck. 2016;39(2):279–87.
Maben D, Anehosur V, Kumar N. Assessment of donor site morbidity following fibula flap transfer. J Maxillofac Oral Surg. 2020;20:258–63.
Abdelrehem A, Shi J, Wang X, Wu Z, Mashrah MA, Zhang C, et al. Novel loop neurorrhaphy technique to preserve lower lip sensate in mandibular reconstruction using an innervated vascularized iliac bone flap. Head Neck. 2022;44(1):46–58.
Kalwagadda S, Kumar B, Nair SC, Shah AK, Shroff SS. Management of ameloblastoma with free tissue flap in comparison with other reconstructive options available. J Oral Maxillofac Surg. 2019;19(2):283–8.
Shahzad F, Henderson PW, Matros E, Cordeiro PG. Long-term growth, functional, and aesthetic outcomes after fibula free flap reconstruction for mandibulectomy performed in children. Plast Reconstr Surg Glob Open. 2022;10(7): e4449.
Zou D, Huang W, Wang F, Wang S, Zhang Z, Zhang C, et al. Autologous ilium grafts: Long-term results on immediate or staged functional rehabilitation of mandibular segmental defects using dental implants after tumor resection. Clin Implant Dent Relat Res. 2013;17(4):779–89.
Zhang M, Rao P, **a D, Sun L, Cai X, **ao J. Functional reconstruction of mandibular segment defects with individual preformed reconstruction plate and computed tomographic angiography-aided iliac crest flap. J Oral Maxillofac Surg. 2019;77(6):1293–304.
Bachelet JT, Bourlet J, Château J, Jacquemart M, Dufour C, Mojallal A, et al. Costal grafting in mandibular reconstruction. Plast Reconstr Surg Glob Open. 2015;3(11): e565.
Chang EI, Boukovalas S, Liu J, Largo RD, Hanasono MM, Garvey PB. Reconstruction of posterior mandibulectomy defects in the modern era of virtual planning and three-dimensional modeling. Plast Reconstr Surg. 2019;144(3):453e–62e.
Dowgierd K, Pokrowiecki R, Wolanski W, Kawlewska E, Kozakiewicz M, Wos J, et al. Analysis of the effects of mandibular reconstruction based on microvascular free flaps after oncological resections in 21 patients, using 3D planning, surgical templates and individual implants. Oral Oncol. 2022;127: 105800.
Wilkman T, Husso A, Lassus P. Clinical comparison of scapular, fibular, and iliac crest osseal free flaps in maxillofacial reconstructions. Scand J Surg. 2018;108(1):76–82.
Akinbami B. Reconstruction of continuity defects of the mandible with non-vascularized bone grafts. Systematic LIter Rev Craniomaxillofac Trauma Reconstr. 2016;9(3):195–205.
Wijbenga JG, Schepers RH, Werker PMN, Witjes MJH, Dijkstra PU. A systematic review of functional outcome and quality of life following reconstruction of maxillofacial defects using vascularized free fibula flaps and dental rehabilitation reveals poor data quality. J Plast Reconstr Aesthet Surg. 2016;69(8):1024–36.
Khatib B, Pogrel MA. Desmoplastic fibroma of the mandible in young children—a case series. Int J Oral Maxillofac Surg. 2017;46(2):173–80.
Puricelli E, Chem RC. Thirty-eight-year follow-up of the first patient of mandibular reconstruction with free vascularized fibula flap. Head Face Med. 2021;17(1):46.
Valentini V, Califano L, Cassoni A, Marco DM, Raponi I, Priore P, et al. Maxillo-Mandibular reconstruction in pediatric patients. J Craniofac Surg. 2018;29(3):761–6.
Sakata Y, Nishioka T, Asamura S. Application of free iliac bone flap based on superficial circumflex iliac perforators in mandibular reconstruction. J Craniofac Surg. 2021;33(3):e253–5.
Zhu Y, Xu W, Zhang C, Yang W. Facial nerve preservation during giant mandibular tumor surgery. J Craniofac Surg. 2017;28(2):e115–7.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
JW: data collection and research, analysis, manuscript preparation; AM: review conception, critical revision; ŁK: review conception, critical revision; WW: review conception, analysis; AL: review conception, critical revision; KD: review conception, critical revision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors report there are no competing interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Walatek, J., Myśliwiec, A., Krakowczyk, Ł. et al. Planning of physiotherapeutic procedure in patients after mandible reconstruction taking into account donor site: a literature review. Eur J Med Res 28, 386 (2023). https://doi.org/10.1186/s40001-023-01386-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01386-y