
Abstract
Background
Studies examining factors associated with patient referral to early supported discharge (ESD)/outpatient rehabilitation (OPR) programs and utilization of ESD/OPR services after discharge from inpatient stroke rehabilitation (IPR) are scarce. Accordingly, we examined utilization of ESD/OPR services following discharge from IPR and patient factors associated with service utilization.
Methods
Stroke patients discharged from IPR facilities in Alberta between April 2014 and March 2016 were included and followed for one year for ESD/OPR service utilization. Multivariable linear and negative binomial regressions were used to examine association of patients’ factors with ESD/OPR use.
Results
We included 752 patients (34.4% of 2,187 patients discharged from IPR) who had 40,772 ESD/OPR visits during one year of follow-up in the analysis. Mean and median ESD/OPR visits were 54.2 and 36 visits, respectively. Unadjusted ESD/OPR visits were lower in females and patients aged ≥ 60 years but were similar between urban and rural areas. After adjustment for patient factors, patients in urban areas and discharged home after IPR were associated with 83.5% and 61.9%, respectively, increase in ESD/OPR visits, while having a right-body stroke was associated with 23.5% increase. Older patients used ESD/OPR less than their younger counterparts (1.4% decrease per one year of older age). Available factors explained 12.3% of variation in ESD/OPR use.
Conclusion
ESD/OPR utilization after IPR in Alberta was low and varied across age and geographic locations. Factors associated with use of ESD/OPR were identified but they could not fully explain variation of ESD/OPR use.
Similar content being viewed by others

Text box 1. Contributions to the literature | |
|---|---|
•Currently, little is known about factors associated with patient referral to early supported discharge or outpatient stroke rehabilitation (ESD/OPR) programs and the utilization of ESD/OPR service use after discharge from inpatient rehabilitation (IPR). | |
•Our study identified patient demographic and clinical factors (such as residing in urban versus rural areas, being discharged home after IPR, and the presence of certain comorbidities) associated with use of ESD/OPR. These factors did not fully explain variation in ESD/OPR use. | |
•Further research and richer data on patients’ clinical and socio-economic characteristics are needed to better understand factors associated with ESD/OPR use among stroke survivors. |
Introduction
Stroke is one of the leading causes of death and disability in Canada [1, 2]. Approximately 50% of patients who have suffered a stroke live with permanent disabilities [3]. It has been estimated that stroke was associated with 288,427 disability adjusted life years (DALY’s) in Canada in 2016 [2].
Stroke rehabilitation is an important component of post-stroke care to help stroke survivors return to their maximum functional level, develop skills, and live independently. Patients with moderate severity stroke often receive a substantial part of their rehabilitation in inpatient rehabilitation (IPR) facilities. The Canadian Best Practice Recommendations for Stroke Care recommends that stroke patients with ongoing rehabilitation needs should have access to outpatient rehabilitation (OPR) services following discharge [4], and it has been shown that the continuum of care (including emergency response, inpatient acute care, inpatient and outpatient rehabilitation, home-based and community care, and long-term care) for stroke patients results in better patient outcomes [5]. OPR services include hospital based or community based programs [6] and are designed for stroke patients who have continued rehabilitation goals following discharge from acute care or IPR. These services should include the same elements as in IPR services and should be provided for at least 45 min per day per discipline for three to five days per week. The full course of OPR therapy should ideally take at least 8 weeks [7]. Alternative services such as early supported discharge (ESD) have also been developed to facilitate earlier discharge from an acute stroke service or IPR for a select group of patients (that is, patients with mild to moderate disability who are medically stable and have access to appropriate nursing care and other support services such as family/care giver and home services [7]), provide equivalent or improved patient and caregiver outcomes, and reduce healthcare resource use [8,9,10]. ESD involves a multidisciplinary team of therapists, nurses, and doctors who coordinate through regular meetings to provide services to patients [11]. These services should be provided for at least 5 days per week at the same intensity level as provided through IPR, and if possible, provided by the same medical team that provided IPR to the patient [7]. Studies have established that the most cost-effective method of providing rehabilitation depends on both the types of services available and patient characteristics implying that a single rehabilitation service may not provide equal health and economic benefits for all patients and situations [12, 13]. For example, for some patients, inpatient rehabilitation may be the most cost-effective rehabilitation service; while for other patients, home or community rehabilitation may be the most cost-effective model of care [14].
Studies examining factors associated with patient referral to ESD/OPR programs and utilization of ESD/OPR services after discharge from IPR are scarce. To our knowledge, there has been only one study by Janzen et al. examining factors associated with referral to outpatient services after IPR within the Canadian health care system [13]. The authors suggested that an improved understanding of current practices in OPR is a necessary step towards develo** recommendations for streamlining the care continuum and optimizing health care delivery [13]. Accordingly, we conducted a population-based retrospective cohort study of patients with stroke who were discharged from IPR between 2014 and 2016 in Alberta, Canada to examine ESD/OPR utilization, and its association with patient and geographical factors following discharge from IPR. Our study findings could provide better insights into the use of ESD/OPR services and its barriers and facilitators. It could help clinicians, stroke care professionals, and policy makers improve stroke management and care programs.
Methods
Data sources and study population
Alberta has a universal coverage and publicly funded health care system that serves a population of more than 4 million people in a large and diverse geographical area. Alberta Health Services (AHS) is the sole healthcare service provider in Alberta and its operation is organized into five geographical health zones (Calgary, Central, Edmonton, North, and South), where Calgary and Edmonton zones are most urbanized and populous (Supplementary Fig. 1) [15]. The ESD/OPR services were successfully piloted in Calgary and Edmonton during 2007–2011 and have been part of the Cardiovascular Health and Stroke Strategic Clinical Network (SCN) in Alberta since 2012. Currently, there are seven ESD/OPR sites in Edmonton, Calgary, Grand Prairie, Camrose, Red Deer, Medicine Hat, and Lethbridge (Agnes Lehman, AHS, personal communication). The ESD/OPR services in Alberta include occupational therapy, physical and physiotherapy, recreation therapy, speech language pathology, psychology, respiratory therapy, social work, and other rehabilitation therapies. These services were provided either face-to-face, at a facility or at the patient’s home, or on the telephone.
We used a previously reported cohort of 2,187 patients who were admitted to 10 IPR facilities in Alberta, Canada between 1 April 2014 and 31 March 2017 (years 2014 to 2016) and survived the IPR episode to identify patients who used ESD/OPR services. Briefly, this IPR patient cohort was those who aged ≥ 18 years, had home as the pre-stroke living setting, were admitted to an IPR facility within 30 days of an acute stroke episode, and discharged alive. This IPR patient cohort was created by linking the National Rehabilitation Reporting System (NRS) [16], Discharge Abstract Database (DAD), and Alberta Health Care Insurance Plan (AHCIP) Registry [17]. Detailed patient selection and characteristics of this IPR patient cohort were described previously [18].
We linked this IPR patient cohort to the ESD/OPR database obtained from AHS, which provides detailed information on a service visit (e.g., facility and date and type of service provided). All patients were followed for one year from the IPR discharge date (index date) for ESD/OPR service utilization. The end date of the follow-up period was 31 March 2018. If a patient had more than one IPR admission during the study period, the last discharge date was used as the index date. Patients who did not have any ESD/OPR visit during one year of follow-up, had rehabilitation services in more than one health zone in Alberta, or did not have active AHCIP coverage (e.g., due to death or emigration) before the end of one year follow-up were excluded.
ESD/OPR service utilization
We reported ESD/OPR service utilization during one year of follow-up as the number of visits per patient. We examined overall ESD/OPR service use and use by sex, age group, urban/rural residence, and health zones (Calgary, Edmonton, and others). We consulted with rehabilitation physicians and grouped occupational therapy, physical therapy, and physiotherapy together because of their similarities and reported five main groups of services: occupational/physical/physiotherapy, psychology, recreation therapy, social work, and speech-language pathology.
Statistical analysis
Patient characteristics were summarized using mean (standard deviation [SD]), median (interquartile range [IQR]), count, and percentage, as appropriate. Multivariable linear regression (MLR) with the natural log of the number of visits as the dependent variable was used to examine association of patient and geographical factors with ESD/OPR service use. This method was previously used to study LOS at IPR [18, 19]. Similar to previously reported studies assessing IPR LOS or referral patterns to ESD/OPR services [13, 18, 20], we included patients’ age, sex, body mass index (BMI), FIM score at IPR discharge, comorbidities, residence location, median household income, acute care LOS of the associated acute stroke episode, LOS of the associated IPR admission, year of discharge from IPR, stroke type, stroke position (that is, the side of the body affected by stroke), and health zone [15] in the regression model. We used the likelihood-ratio (LR) test to assess the goodness of fit of the unconstrained model (that is, the model with all patient-level factors) versus the constrained model (that is, the model that only included statistically significant factors). A factor remained in the final constrained model if the LR test results were significant at a 10% level. We did not use the traditional stop** rule of 5% significant level because it has been reported that a strict rule could lead to exclusion of important variables [21,22,23].
We used previously validated ICD-10 codes to identify patients’ comorbidities [24]. Patients were considered to have the comorbidities in question if the ICD-10 codes corresponding to those comorbidities were recorded in any diagnostic field at admission to IPR, or in any diagnostic field at hospitalizations during the two years prior to IPR admission. The second digit of the patients’ postal code was used to identify their area of residence [25]. All analyses were performed using Stata version 14 (Stata Corporation, College Station, Texas). Two-sided P values < 0.05 were considered statistically significant.
Sensitivity analysis
In addition to the MLR regression method, we used a multivariable negative binomial (MNB) regression to model the number of ESD/OPR visits as a count variable and ascertain robustness of the regression approach. We included patient-level factors described in the MLR model above and use the LR test to examine inclusion of those factors in the final constrained MNB regression model.
Ethics approval
This study was conducted as part of a large health evidence review on optimizing stroke rehabilitation practice in Alberta [26], and funded by Alberta Health. Data were provided by Alberta Health subject to the Alberta Health Information Act [27], and approval from a research ethics board was not required.
Results
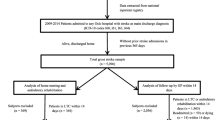
There were 2,187 patients who had home as their pre-stroke living setting, were admitted to 10 IPR facilities in Alberta between 2014 and 2016, and survived the IPR admission [18]. Of them, 792 (36.2%) used ESD/OPR services during follow-up. After excluding 1,395 (56.2%) patients who did not receive ESD/OPR services during one year post IPR discharge, and 40 patients for other reasons (i.e., patients who had ESD/OPR visits in more than one health zone during follow-up and patients with missing data for the variables used in the analysis), the final study cohort included 752 (34.4%) patients who had 40,772 outpatient rehabilitation visits during one-year post-IPR discharge. A flowchart depicting patient selection is presented in Fig. 1.

Patient selection flowchart
Detailed characteristics of the studied population are presented in Supplementary Table 1. Most patients were male (63.6%) and 60 years of age or older (58.8%). Hypertension (76.9%), dyslipidemia (41.1%), and diabetes (29.8%) were the most common comorbidities. Mean acute care LOS of the associated acute stroke episode was 29.4 days, while mean LOS of the associated IPR episode was 58.1 days. FIM score (mean = 109.8) at IPR discharge ranged between 37 and 126. More than 90% of the patients were discharged home following IPR. Most patients (88.9%) lived in urban areas and almost half were in the Calgary zone.
ESD/OPR service utilization
The average number of ESD/OPR visits per patient was 54.2 (SD = 56.5), and the median number of ESD/OPR visits was 36 (IQR = 12–79). The mean number of visits was lower among female patients compared with male patients (48.7 vs. 57.4 visits, p = 0.048) though the median number of visits was similar between the two sex groups (33 vs. 37, p = 0.291). The number of visits were higher in patients aged < 60 years (mean = 60.3 visits, < 0.05) compared with older patient groups. There were no differences in ESD/OPR use between urban and rural areas (mean = 54.4 vs. 52.8 visits, p = 0.810). Patients in the Calgary zone had the lowest number of visits (mean = 42.2 visits, p < 0.05) compared with patients in the other two zone groups (Table 1).
The utilization of ESD/OPR services by types and by health zones and urban/rural residency is presented in Tables 2 and 3, respectively. Occupational/physical/physiotherapy was the most used service. Psychology service was only available in Calgary and Edmonton zones, but the utilization was low (0.3 and 4.6 visits per patient in Calgary and Edmonton, respectively). Use of other types of services was lower in Calgary and Edmonton, compared to other zones (all pairwise p < 0.05). The mean number of visits to social workers was lower in urban areas (1.2 visits) compared to that in rural areas (2.3 visits; p = 0.019), but there were no differences in types of services between urban and rural areas for other four groups of ESD/OPR services (Table 3).
The final MLR model predicting the natural logarithm of the number of ESD/OPR visits included age, whether the patient was discharged home after IPR, acute care LOS of the associated acute stroke episode, BMI, urban living location, stroke position, presence of peripheral vascular disease, and health zone. They explained 12.3% of the variation in the frequency of ESD/OPR visits during the study period (Table 4). A one-year increase in age was associated with a reduction in the mean number of visits by 1.4% (p = 0.001). Living in an urban (versus rural) area and being discharged home (as opposed to other locations) after IPR were both associated with an increase in the mean number of visits by 83.5% (p < 0.001) and 61.9% (p = 0.006), respectively. A one-day increase in acute care LOS of the associated acute stroke episode and a one-unit increase in the body mass index were both associated with a slight increase in the mean number of visits by 0.5% (p = 0.003) and 0.3% (p = 0.034), respectively. Having a right-body stroke (as opposed to left-body) was associated with an increase in the average number of visits by 23.5% (p = 0.047). Being in the Edmonton zone and other zones was associated with a higher mean number of visits by 28.5% (p = 0.031) and 247.3% (p < 0.001), respectively, compared with being in the Calgary zone.
Sensitivity analysis
Table 5 presents detailed results of the MNB regression analysis of ESD/OPR service use. The MNB model is generally consistent with the MLR model, except for the presence of male sex and three comorbidities (hypertension, diabetes, and dyslipidemia) in the MNB. Also, being discharged home following IPR had a significant effect in the MLR but not the MNB model.
Discussion
Using a population-based cohort of patients who were discharged from 10 IPR facilities in Alberta between 2014 and 2016, we found that only 36.2% of the stroke patients used ESD/OPR services during one year after IPR discharge. Overall, use of ESD/OPR services was lower among female and older patients. Patients in the Calgary zone had the lowest number of visits compared with those in Edmonton or other zones. Occupational/physical/physiotherapy was the most used service and there were no differences in types of ESD/OPR services between urban and rural residents, except for visits to social workers. Regression analyses indicated that factors such as age, health zone, acute care LOS of the associated acute stroke episode, BMI, and stroke position, were consistently associated with ESD/OPR service use. The MLR model appeared to be a better fit for our data, with a higher R-squared value than in the MNB model (12% versus 2%, respectively).
The Canadian Stroke Best Practice Recommendations indicate that a patient is a suitable candidate for OPR if the patient’s rehabilitation needs can be met in the community, the patient meets the general inclusion criteria for stroke rehabilitation (as described in the Canadian Stroke Best Practice Recommendations document [4]), the patient is medically stable, ready to participate in rehabilitation, can be accompanied by a caregiver to the therapy sessions if necessary, and can organize transportation to and from the rehabilitation center [4]. While we did not assess factors associated with whether a patient receives ESD/OPR services, patients who did not receive any ESD/OPR services in our study sample may not have been suitable candidates for it based on their medical condition, the patients’ rehabilitation needs could not be met in the community, and/or the patients may not have had the required assistance (if needed) for participation in ESD/OPR.
Studies examining the factors that determine transitions from IPR to community/outpatient stroke rehabilitation among stroke patients, including which patients get referred to ESD/OPR and which referred patients attend the therapy program, are scarce. Sandel et al. 2009, studied the demographic, socioeconomic, and geographical disparities in access to a variety of post-acute stroke rehabilitation services (including inpatient rehabilitation hospital [IRH], skilled nursing facility [SNF], home health care [HH] and outpatient, or no rehabilitation services) during the year after stroke in the United States, but did not specifically examine the factors associated with the receipt/number of visits of outpatient stroke rehabilitation following receipt of IPR services. They found that the percentage of individuals in the SNF and HH categories as the highest utilized post-acute care service categories decreased between 1996 and 2003, while the percentage of individuals in the outpatient services category as the sole post-cate care treatment increased over time [28]. Freburger et al. [29] also found demographic differences in post-acute rehabilitation care (that is, receiving HH versus no HH among those discharged to home, and receiving IRH versus SNF among those discharged to institutions) among patients in selected states in the United States, even after controlling for factors such as illness severity, comorbidities, and supply. More specifically, they found that Blacks, women, older individuals, and lower income individuals were more likely to get discharged to an institution versus home, while Hispanics and the uninsured were less likely to receive institutional care. Conditional on being discharged home, racial minorities, women, older individuals, and lower income individuals were more likely to receive HH than no HH, while the uninsured were less likely to receive it. Chan et al. [30] used the same cohort used by Sandel et al. to examine disparities associated with the number of outpatient rehabilitation visits during the year following discharge from acute care. Similar to our findings, Chan et al. found age to be negatively associated with the number of outpatient visits and the acute care LOS to be positively associated with the number of visits. However, the study did not specifically examine the number of outpatient rehabilitation visits among those who had received IPR services. They also did not include patient comorbidities in their analysis, which were found to be highly correlated with the number of ESD/OPR visits in the present study. Further, we used two different models to examine the factors associated with the number of ESD/OPR visits and found consistent results. It should be noted that studies by Sandel et al., Freburger et al., and Chan et al. used United States data, so there may be variations between the results of these studies and the present study due to the differences between the United States and Canada healthcare systems as reported previously [31].
Janzen et al. performed a retrospective chart review of a cohort of 1,497 stroke patients who were from an IPR facility between 1 January 2009 and 1 March 2016 within the Southwest Local Health Integration Network geographical boundaries in Ontario [13]. Among these patients, 891 were referred to an OPR program, and 721 of these attended the program. Those who were referred were significantly younger, had higher FIM scores at discharge, and had shorter IPR LOS compared with those who were not referred. Also, most of the referred patients were discharged home following IPR. Patients who attended the program (that is, patients who received the OPR therapy) were, again, significantly younger and had higher discharge FIM scores but did not have a significantly different stroke severity compared with those who did not attend the program. In addition, among patients who received OPR therapy, the average number of visits was 32.2 (standard deviation: 26.2). Our study differs from Janzen et al. in that we examined the factors that were associated with the utilization of ESD/OPR services (by those who received any service). We also looked at a wider range of patient factors than Janzen et al., including more detailed patient characteristics (specifically for predicting the frequency of visits). Unlike Janzen et al. who found that getting referred to OPR services and/or receiving any OPR services was significantly associated with the discharge FIM score and IPR LOS, we did not find any of those factors to be significantly associated with the utilization of ESD/OPR services received. Instead, we found the LOS of the associated acute stroke episode to have a positive and significant effect on the number of ESD/OPR visits. However, low R-squared value of 12% suggests that there could be other factors that we did not observe in the data and hence could not control for. Further research and richer data on patients’ clinical and socio-economic characteristics are needed to fill this gap.
Optimal allocation of healthcare resources between acute care and rehabilitation, and among segments of rehabilitation including inpatient rehabilitation, OPR, and ESD is another key challenge for healthcare planners in responding to the increasing demand for provision of care to stroke survivors [32]. Yan et al. used a stroke rehabilitation optimal model, combining discrete event simulation with a genetic algorithm, that changes care capacity across segments of rehabilitation to identify an optimal solution for minimizing wait times in each segment in Alberta. Their model predicted that if ESD and OPR could be provided to additional 138 and 262 stroke survivors, respectively (compared with the status quo), it would result in cost savings of $25.45 million annually [32].
Another challenge in the delivery of post-stroke rehabilitation services is in their delivery to patients residing in rural settings as they have been shown to have decreased access to healthcare, including rehabilitation services, compared with those residing in urban areas [33, 34]. This may partly explain our finding regarding a higher utilization of ESD/OPR services among urban residents than rural residents. Allen et al. suggested providing home-based specialized rehabilitation services for rural residents as a potential solution to this problem and found that providing this service will result in functional gains for rural resident comparable to those living in urban settings [35]. However, successful home-based rehabilitation partly depends on effective communication and collaboration between the caregiver, patient, and therapist [36, 37]. Fisher et al. also suggested that (a) develo** strategic networks can help understand the needs of these patients at an organizational level and (b) the existing gap in skill mix and staff establishment among teams providing rehabilitation services is one reason for the unmet needs of patients with more severe disabilities [38].
Although this study contributes to knowledge of the clinical and socio-demographic factors associated with utilization of ESD/OPR services following discharge from IPR among stroke patients, it has limitations. The administrative data sets did not include several clinical data elements of the acute stroke episode [18]. These clinical data, such as the severity of specific impairments (that is, ataxia or aphasia) which may not be fully captured in the FIM score, can be associated with increased LOS at IPR [39]. We expect these factors to contribute to the number of ESD/OPR visits following discharge from IPR as well. Thus, more detailed information about the patients’ clinical characteristics could facilitate better understanding about the association between those factors and the utilization of ESD/OPR services received.
Conclusion
Our population-base cohort study of patients with inpatient stroke rehabilitation found that utilization of early support discharge and outpatient rehabilitation in Alberta was low and it varied according to patient sex, age, area of residence and service type. Factors associated with utilization of outpatient rehabilitation were generally consistent with those reported in the literature, suggesting that our study findings could be considered in other jurisdictions with similar health care systems. Future research with additional clinical data is warranted to further improve understanding of outpatient stroke rehabilitation and support better care for patients with stroke.
Data availability
The data that support the findings of this study are available from Alberta Health. However, restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission from Alberta Health.
References
Statistics Canada. Table: 13-10-0394-01: Leading causes of death, total population, by age group Ottawa, ON: Statistics Canada; 2019 [cited 2019 October 17]. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401.
GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the global burden of Disease Study 2016. Lancet Neurol. 2019;18(5):439–58.
Mittmann N, Seung SJ, Hill MD, et al. Impact of disability status on ischemic stroke costs in Canada in the first year. Can J Neurol Sci Le J Canadien des Sci Neurologiques. 2012;39(6):793–800.
Hebert D, Lindsay MP, McIntyre A, et al. Canadian stroke best practice recommendations: stroke rehabilitation practice guidelines, update 2015. Int J Stroke. 2016;11(4):459–84.
Cameron JI, Tsoi C, Marsella A. Optimizing stroke systems of care by enhancing transitions across care environments. Stroke. 2008;39(9):2637–43.
Teasell R, Meyer MJ, McClure A, et al. Stroke rehabilitation: an international perspective. Top Stroke Rehabil. 2009;16(1):44–56.
Teasell R, Salbach NM, Foley N et al. Canadian Stroke Best Practice Recommendations: Rehabilitation, Recovery, and Community Participation following Stroke. Part One: Rehabilitation and Recovery Following Stroke; 6th Edition Update 2019. International Journal of Stroke. 2020 2020/10/01;15(7):763–788.
Langhorne P, Taylor G, Murray G et al. Early supported discharge services for stroke patients: a meta-analysis of individual patients’ data. Lancet. 2005 2005/02/05/;365(9458):501–6.
Fearon P, Langhorne P, Early Supported Discharge Trialists. Services for reducing duration of hospital care for acute stroke patients. Cochrane Database Syst Reviews. 2012;9:CD000443.
Langhorne P, Baylan S, Early Supported Discharge Trialists. Early supported discharge services for people with acute stroke [Review]. Cochrane Database Syst Reviews. 2017 (7):CD000443.
Langhorne P, Baylan S. Early supported discharge services for people with acute stroke. Cochrane Database Syst Reviews. 2017 (7).
Brusco NK, Taylor NF, Watts JJ, et al. Economic evaluation of adult rehabilitation: a systematic review and meta-analysis of randomized controlled trials in a variety of settings. Arch Phys Med Rehabil. 2014;95(1):94–e1164.
Janzen S, Mirkowski M, McIntyre A, et al. Referral patterns of stroke rehabilitation inpatients to a model system of outpatient services in Ontario, Canada: a 7-year retrospective analysis. BMC Health Serv Res. 2019;19(1):399.
Brusco NK, Taylor NF, Watts JJ, et al. Economic evaluation of Adult Rehabilitation: a systematic review and Meta-analysis of Randomized controlled trials in a Variety of settings [Review]. Arch Phys Med Rehabil. 2014;95(1):94–116.
AHS Map and Zone Overview. Alberta Health Services; [cited 2021]. https://www.albertahealthservices.ca/assets/about/publications/ahs-ar-2021/zones.html.
Canadian Institute for Health Information. National Rehabilitation Reporting System Metadata CIHI2019 [cited 2019 August 12]. https://www.cihi.ca/en/national-rehabilitation-reporting-system-metadata.
Alberta Health Analytics and Performance Reporting Branch. Overview of administrative health datasets. Governement of Alberta; 2017.
Tran DT, Yan C, Dukelow SP et al. Length of Stay and Home Discharge for patients with Inpatient Stroke Rehabilitation. Can J Neurol Sci / J Canadien Des Sci Neurologiques. 2021:1–9.
Grant C, Goldsmith CH, Anton HA. Inpatient stroke rehabilitation lengths of stay in Canada derived from the National Rehabilitation Reporting System, 2008 and 2009. Arch Phys Med Rehabil. 2014;95(1):74–8.
Rice DB, McIntyre A, Mirkowski M, et al. Patient-centered goal setting in a hospital-based Outpatient Stroke Rehabilitation Center [Article]. Pm&R. 2017;9(9):856–65.
Bursac Z, Gauss CH, Williams DK, et al. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:17.
Bendel RB, Afifi AA. Comparison of stop** rules in Forward Stepwise Regression. J Am Stat Assoc. 1977 1977/03/01;72(357):46–53.
Mickey RM, Greenland S. The impact of confounder selection criteria on effect estimation. Am J Epidemiol. 1989;129(1):125–37.
Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–9.
Statistics Canada. Postal Code Conversion File (PCCF), Reference Guide 2011 [cited 2019 February 2]. https://www150.statcan.gc.ca/n1/pub/92-153-g/2011002/tech-eng.htm.
Institute of Health Economics. In: Economics IH, editor. Optimizing stroke rehabilitation practice in Alberta: evidence synthesis and economic evaluation. Edmonton: Institute of Health Economics; 2021.
Government of Alberta. Health Information Act Alberta: Government of Alberta. 2022. https://open.alberta.ca/publications/h05.
Sandel ME, Wang H, Terdiman J, et al. Disparities in stroke rehabilitation: results of a study in an integrated health system in northern California. Pm r. 2009;1(1):29–40.
Freburger JK, Holmes GM, Ku LJ, et al. Disparities in postacute rehabilitation care for stroke: an analysis of the state inpatient databases. Arch Phys Med Rehabil. 2011;92(8):1220–9.
Chan L, Wang H, Terdiman J, et al. Disparities in outpatient and home health service utilization following stroke: results of a 9-year cohort study in Northern California. PM & R: the journal of injury. Function Rehabilitation. 2009;1(11):997–1003.
Kaul P, Reed SD, Hernandez AF, et al. Differences in treatment, outcomes, and quality of life among patients with heart failure in Canada and the United States. JACC Heart Fail. 2013;1(6):523–30.
Yan C, McClure N, Dukelow SP et al. Optimal Planning of Health Services through genetic algorithm and Discrete Event Simulation: a proposed model and its application to Stroke Rehabilitation Care. MDM Policy & Practice. 2022 2022/07/01;7(2):23814683221134098.
Jia H, Cowper DC, Tang Y, et al. Postacute stroke rehabilitation utilization: are there differences between rural-urban patients and taxonomies? J Rural Health. 2012 Summer;28(3):242–7.
Rodriguez D, Cox M, Zimmer LO, et al. Similar secondary stroke prevention and medication persistence rates among rural and urban patients. J Rural Health. 2011 Winter;27(4):401–8.
Allen L, McIntyre A, Janzen S, et al. Community Stroke Rehabilitation: how do rural residents fare compared with their urban counterparts? Can J Neurol Sci. 2016;43(1):98–104.
Lavis H, van Vliet P, Tavener M. Stroke survivor, caregiver and therapist experiences of home-based stroke rehabilitation: a thematic synthesis of qualitative studies. Phys Therapy Reviews. 2023 2023/03/04;28(2):157–73.
Connor EO, Dolan E, Horgan F, et al. A qualitative evidence synthesis exploring people after stroke, family members, carers and healthcare professionals’ experiences of early supported discharge (ESD) after stroke. PLoS ONE. 2023;18(2):e0281583.
Rebecca JF, Lal R, Frances R-B, et al. Barriers and facilitators in providing home-based rehabilitation for stroke survivors with severe disability in the UK: an online focus group study with multidisciplinary rehabilitation teams. BMJ Open. 2023;13(8):e071217.
Lai W, Buttineau M, Harvey JK, et al. Clinical and psychosocial predictors of exceeding target length of stay during inpatient stroke rehabilitation. Top Stroke Rehabil. 2017;24(7):510–6.
Acknowledgements
The authors thank Alberta Health, Alberta Health Services, and the Expert Advisory Group (EAG) for providing data access and expert inputs during EAG meetings.
Funding
Production of this document has been made possible by a financial contribution from the Government of Alberta (grant numbers: 12651 and 8491). The views expressed herein do not necessarily represent the official policy of the Government of Alberta.
Author information
Authors and Affiliations
Contributions
N.R., D.T., S.D., and J.R. conceptualized the study. N.R. carried out analyses and drafted the manuscript. All the authors contributed to the writing. All the authors critically reviewed the manuscript for intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Razavilar, N., Tran, D.T., Dukelow, S.P. et al. Utilization of early supported discharge and outpatient rehabilitation services following inpatient stroke rehabilitation. Arch Public Health 82, 80 (2024). https://doi.org/10.1186/s13690-024-01300-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-024-01300-w