
Abstract
Background
To evaluate the utility of 68Ga-DOTATATE and 18F-FDG PET/MR for prediction of grade and stage of pancreatic neuroendocrine tumors (PNETs), and to examine the correlation between parameters obtained from FDG PET and diffusion-weighted imaging (DWI) MR parameters.
Methods
A retrospective study using 68Ga-DOTATATE and 18F-FDG PET/MR imaging was performed between April 2020 and May 2022 on 46 individuals with histologically confirmed PNETs. Metabolic tumor volume (MTV), maximum standardized uptake value (FSUVmax), and tumor lesion glycolysis (TLG) for FDG; somatostatin receptor density (SRD), maximum standardized uptake value (GSUVmax), and total lesion somatostatin receptor density (TLSRD) for DOTATATE; and minimum and mean apparent diffusion coefficient (ADCmin and ADCmean) values for MRI, respectively. We performed Spearman’s correlation analysis to examine the links between these variables and primary tumor stage and grading.
Results
Higher PNET grading was associated with higher FSUVmax, MTV, and TLG values (P < 0.05). TLG, SRD, ADCmin, and ADCmean values were correlated with N staging, while SRD, MTV, ADCmin, TLG, and ADCmean were associated with M staging. Notably, ADCmin was a negative correlation between FSUVmax (r = − 0.52; P < 0.001), MTV (r = − 0.50; P < 0.001), and TLG (r = − 0.56; P < 0.001).
Conclusions
This study highlights significant correlative relationships between FDG PET-derived parameters and ADCmin. ADCmin may offer utility as a tool for PNET staging and grading in lieu of FDG PET. 68Ga-DOTATATE PET/MR alone may be a sufficient alternative to dual tracer PET/MR when conducting grading and staging of primary PNETs.
Similar content being viewed by others
Introduction
Pancreatic neuroendocrine tumors (PNETs) show great variation in their degrees of aggressiveness, their histological subtypes, and their clinical manifestations [1], resulting in the need for different treatment strategies and corresponding variability in patient prognostic outcomes [2].
The PNET categorization systems developed by the World Health Organization (WHO) and European Neuroendocrine Tumor Society (ENETS) are both widely used in clinical practice. The ENETS system entails the classification of PNETs and gastrointestinal NETs through the use of a four-stage TNM (tumor-node-metastasis) system, whereas the WHO system is based upon analyses of tumor cell proliferation through the detection of mitotic counts and Ki-67 expression levels. In recent reports, tumor grading and staging have been found to offer independent but complementary insight into the overall characteristics of a given malignancy [3, 4]. Noninvasive tumor grading and staging in particular would be of clinical benefit, which could reduce risks associated with invasive biopsy, aiding in preoperative assessments aimed at selecting the most optimal therapeutic strategy.
Currently, 68Ga-DOTA peptide-based imaging approaches are the gold standard used for assessing well-differentiated NETs exhibiting high levels of somatostatin receptor (SSTR) density [5]. However, since SSTR expression is lower on high-grade poorly differentiated NETs, 18F-FDG PET imaging is more reliable for evaluating these tumors [6]. 68Ga-DOTANOC PET-based SUVmax values can serve as a reflection of SSTR2 density [7], whereas 18F-FDG PET uptake values correspond to increases in metabolic activity at the cellular and tissue levels. Previous research efforts have demonstrated the complementary value of combining quantitative parameters derived from 68Ga-DOTA-peptides and 18F-FDG PET imaging analyses when evaluating PNET aggressiveness and conducting prognostic assessments [8, 9]. In contrast, apparent diffusion coefficient (ADC) values derived from diffusion-weighted imaging (DWI) from the MR sequence of PET/MR correlate with tumor cellularity such that they may offer value when evaluating tumor grading [10, 11]. While DWI and 18F-FDG PET offer insight into distinct molecular characteristics, glucose metabolic activity and tumor cellularity have also been reported to be positively correlated with one another [12]. When assessing tumor aggressiveness, the properties revealed by FDG and ADC are similar [13, 14]. However, evidence regarding the associations between MR and PET-derived parameters from PNET patient 18F-FDG and 68Ga-DOTATATE dual tracer PET/MR scanning is lacking at present. Therefore, this research was designed to further investigate the value of these various imaging measures in the preoperative grading and staging of primary PNETs.
Materials and methods
Patient selection
Our institution's ethics committee approved this retrospective research. Patients suspected of having PNET based on imaging results, clinical symptoms, and/or high tumor marker levels were recruited in this research between April 2020 and May 2022 and underwent 68Ga-DOTATATE PET/MR and 18F-FDG PET/MR scans retrospectively. Patients were included if they met the following criteria: a definitive biopsy- or surgical pathology-based histological diagnosis; adequate imaging quality for these analyses; and no previous therapy (surgery, radiotherapy, or chemotherapy). In total, 46 PNET patients were selected based on this criteria. The 2019 WHO classification system was used for tumor grading [15], while the ENETS system was used for tumor N and M staging [16].
18F-FDG and 68Ga-DOTATATE PET/MR analyses
Each patient had a PET/MR scan on two different days during a 2-week period. After fasting for at least 6 h, patients’ blood glucose levels were guaranteed to be below 11.1 mmol/L before the scan. 18F-FDG PET/MRI scans were performed 45–90 min after 2–5 MBq/kg 18F-FDG was injected intravenously (i.v.). After i.v. injection of 2.0 MBq/kg 68Ga-DOTATATE, PET/MRI scanning was commenced 45–60 min later. These studies used an integrated PET/MR scanner (Biograph mMR; Siemens Healthineers, Erlangen, Germany). Four different bed positions were used to acquire PET data from the middle of the thighs to the base of the skull (4 min each position), and then a single bed position was used to get data from the head (8 min total). While being scanned, patients remained supine with their arms at their sides. For the purpose of PET data reconstruction, a 3D attenuation-weighted ordered-subset expectation–maximization approach was used (2 iterations, 21 subsets, 256 × 256 matrices). The reconstructed images were smoothed using a Gaussian smoothing kernel that had a full width at half maximum (FWHM) of 6 mm. Cross-sectional T2-weighted 2D HASTE, echo-planar DWI (b values: 50 and 800 s/mm2), cross-sectional T1-weighted imaging, and T1WI-Dixon sequences were all collected concurrently with PET image collection. The ADC value was determined using a single exponential function (b values of 50 and 800 s/mm2).
Quantitative image analyses
The LIFEx platform v5.1 [17] was used to extract all imaging parameters. Two nuclear medicine doctors, JG and SX, who had each worked with 18F-FDG and 68Ga-DOTATATAE PET/MR imaging for more than three years, hand-drew 3D volumes of interest (VOIs). Then, the 18F-FDG PET FSUVmax, MTV, and TLG parameters, as well as the 68Ga-DOTATATE PET maximum standardised uptake value (GSUVmax), somatostatin receptor density (SRD), and total lesion somatostatin receptor density (TLSRD) parameters, were taken from these primary tumors [8]. MTV was measured based on tumor segmentation using a 40% FSUVmax threshold, while TLG was defined as FSUVmean x MTV. SRD was measured based on tumor segmentation using a 40% GSUVmax threshold, with TLSRD similarly being defined as GSUVmean × SRD. The ADCmean and ADCmin values from primary tumors were measured using an MR ADC map while avoiding vessels, necrotic areas, and imaging artifacts.
Statistical analysis
Continuous data that follow a normal distribution are represented as means and standard deviations (SD), whereas data that do not follow a normal distribution are reported as medians and interquartile ranges (IQR). Proportional frequencies are presented for categorical variables. Differences in tumor staging and grading were assessed with Mann–Whitney U tests, while binary variables were assessed with Fisher’s exact tests. Spearman rank correlation coefficients were used to analyze the correlation between imaging parameters and the Ki-67 index. Intraclass correlation coefficient (ICC) was used to analyze the inter-observer reproducibility. The imaging parameters associated with tumor grade and stage were analyzed using a forward logistic regression model (Wald method) in a multivariate analysis. This study used SPSS 26.0 (SPSS, IL, USA) with a significance threshold of P < 0.05 for all statistical analysis.
Results
Patient characteristics
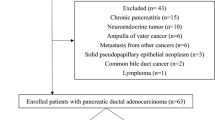
Forty-six patients with histologically confirmed PNETs were scanned with 68Ga-DOTATATE PET/MR and 18F-FDG PET/MR between April 2020 and May 2022. The patients comprised 25 women (54.3%) and 21 men (45.7%), aged 22–75 y (median age, 52 y). Two of these 46 patients (4.3%) were diagnosed with multiple endocrine neoplasia type I syndrome. There were 29 patients with G1 tumors, 14 with G2 tumors, and 3 with NEC (a more severe kind of cancer) tumors. ENET N staging for these patients was as follows: N0 (n = 39), N1 (n = 7). ENET M staging for these patients was as follows: M0 (n = 36), M1 (n = 10). Table 1 provides a summary of the patient characteristics. The mean tumor size was 3.2 ± 2.8 cm (0.6–13.8 cm). A strong correlation was found between tumor size and MTV (r = 0.84, P < 0.001), TLG (r = 0.87, P < 0.001), SRD (r = 0.82, P < 0.001), TLSRD (r = 0.68, P < 0.001), and FSUVmax (r = 0.76, P < 0.001). Tumor size negatively correlated with ADCmin (r = − 0.59, P < 0.001) and ADCmean (r = − 0.44, P = 0.002). No significant correlation was found between tumor size and the GSUVmax (r = − 0.04, P = 0.81).
Inter-observer reproducibility of 68Ga-DOTATATE, 18F-FDG PET, and ADC parameters
A high interobserver agreement level was demonstrated for 68Ga-DOTATATE PET parameters (GSUVmax:0.99, P < 0.001; SRD:0.82, P < 0.001; TLSRD:0.95, P < 0.001) and 18F-FDG PET parameters (FSUVmax:0.99, P < 0.001; MTV: 0.89, P < 0.001; TLG:0.95, P < 0.001). The ICC of ADCmin and ADC mean was 0.82 and 0.91 (all P < 0.001).
Tumor grade, 68Ga-DOTATATE, 18F-FDG PET, and MR ADC relationships
Increases in the FSUVmax, MTV, and TLG 18F-FDG PET/MR parameters were observed with increasing tumor grade from G1 to G3, whereas GSUVmax values derived from 68Ga-DOTATATE PET/MR scans declined with tumor grade. SRD and TLSRD values rose with tumor grade. Significant decreases in ADCmin and ADCmean values were observed with increasing tumor grade. For further details regarding tumor characteristics, see Table 2.
Ki-67 index, 68Ga-DOTATATE, 18F-FDG PET, and ADC parameters correlate
Ki-67 index values were significantly positively correlated with FSUVmax (r = 0.45, P < 0.01), TLG (r = 0.48, P < 0.01), MTV (r = 0.42, P < 0.01), and SRD (r = 0.43, P < 0.01), whereas they were significantly negatively correlated with ADCmin (r = − 0.85, P < 0.01), GSUVmax (r = − 0.33, P = 0.03), and ADCmean (r = − 0.61, P < 0.01). Ki-67 index levels and TLSRD had a slight, nonsignificant connection (r = 0.19, P = 0.20).
Relationships between tumor staging and 68Ga-DOTATATE, 18F-FDG PET, and ADC parameters
Increases in TLG (P = 0.03), SRD (P = 0.01), decreases in ADCmin (P < 0.01), and decreases in ADCmean (P < 0.01) were all associated with increasing tumor N staging. MTV (P = 0.03), TLG values (P = 0.03), SRD (P < 0.01), ADCmin (P < 0.01), and ADCmean (P < 0.01) were linked with tumor M staging. Tumor staging was not significantly linked with any of the other examined characteristics (P > 0.05) (Table 3).
Relationships between 18F-FDG PET and MR parameters
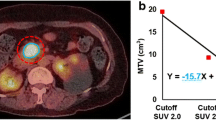
Correlation values of − 0.52 (P < 0.01), − 0.50 (P < 0.01), and − 0.56 (P < 0.01) were found between the 18F-FDG PET parameters FSUVmax, MTV, TLG and ADCmin, respectively (Fig. 1). There was no significant association between the parameters of ADCmean and 18F-FDG PET. These findings indicate that the ADCmin and FDG parameters have a negative connection, which may be predictive of PNET grade and staging.

The correlation between ADCmin and FSUVmax, MTV, and TLG. ADC Apparent diffusion coefficient, SUV Standard uptake value, MTV Metabolic tumor volume, TLG Total lesion glycolysis
Preoperative risk factors for tumor grade and stage
Multivariate analysis revealed that only ADCmin could predict the presence of lymph nodal and distant metastases (P = 0.005 and P = 0.006, respectively). ADCmin could also differentiate between PNET G1 and G2/3 (P = 0.002). Other imaging variables were not significantly associated with tumor grade and staging.
Discussion
The results of these analyses indicated that dual-tracer PET/MR can offer invaluable imaging data when conducting staging and grading assessments for PNET patients. Both tumor grade and Ki-67 index values were associated with several different parameters derived from dual-tracer PET/MR scans and were of value when predicting the M and N staging of primary PNETs. Strikingly, ADCmin was negatively correlated with FDG PET parameters (MTV, TLG, FSUVmax) in this study, suggesting that this PET/MR DWI-MR-derived ADCmin value can offer information equivalent to results derived from 18F-FDG PET scanning, thus potentially obviating the need for these 18F-FDG PET scans. As such, 68Ga-DOTATATE PET/MR alone rather than 18F- FDG and 68Ga-DOTATATE dual-tracer PET/MR is sufficient for PNET grading and stage.
Significant differences in both 18F-FDG uptake (MTV and TLG) and MR (ADCmin and ADCmean) parameters were observed when comparing PNETs of varying grades. Consistently, Ki-67 levels of primary neuroendocrine tumors were shown to have a positive connection between MTV and TLG levels by Abdulrezzak et al. [18]. Moreover, Chan et al. detected higher MTV values when assessing higher-grade tumors [19]. Increased Ki-67 expression is indicative of higher levels of cell proliferation, and the uptake of FDG is closely linked to this proliferative activity given that glycolytic activity is increased in rapidly proliferating cells such that they can generate the energy required for ongoing biosynthetic and replicative processes [20]. In other tumor types, correlations between Ki-67 index values and both ADCmin and ADCmean have been reported [21, 22], suggesting that these parameters are valuable biomarkers that reflect tumor biology in terms of proliferative activity. G3 PNETs in this study exhibited lower 68Ga-DOTATATE uptake levels as compared to G1 PNETs.
With respect to tumor staging, the present results revealed that the 18F-FDG-derived TLG and 68Ga-DOTATATE-derived SRD volumetric parameters from primary PNETs were capable of differentiating between different patient nodal (N0 and N1) and metastatic (M0 and M1) status. Moreover, MR-derived ADCmin and ADCmean values were significantly correlated with patient N and M staging. This could be a good help in identifying PNETs with malignant behavior. The potential utility of these PET/MR parameters has also been demonstrated in prior studies of PNET patients. For example, Langen et al. observed prognostic utility for both TLG and MTV in patients with high-grade gastroenteropancreatic neuroendocrine neoplasms [23]. De Robertis et al. observed a significant reduction in ADCmean values in individuals with stage III-IV lesions relative to individuals with lower tumor staging [24]. No associations were seen between SUVmax values obtained from 18F-FDG or 68Ga-DOTATATE PET/MR and N or M staging in patients with PNET. This may be attributable to the fact that SUVmax is based on a point-based tumor evaluation, whereas MTV can reflect the extent of the hypermetabolic tumor area. Higher numbers of hypermetabolic cells are more likely to correspond to nodal or distant metastasis. Moreover, in a multivariate analysis, the ADCmin of the primary tumor was the only significant predictor of tumor histological grading and stage, which could help predict tumor grade and stage for pretreatment tumor stratification.
Consistent with the present results, prior studies have not detected any significant correlations between ADCmean and FDG uptake parameters (FSUVmax, TLG, and MTV) [25, 26]. However, a correlation was detected between ADCmin values and MTV, TLG, and FSUVmax values, in line with prior studies on rectal cancer [27]. This is attributable to the fact that ADCmin values reflect the most highly proliferative areas of tumors and the regions with the greatest cell density [28]. As such, tumors exhibiting lower ADCmin values or higher FDG-derived TLG or MTV values are more likely to exhibit a higher Ki-67 index value and more advanced pathological staging. Moreover, the correlation between FDG parameters and ADCmin is relatively strong. Consequently, FDG and ADC values may have the potential to be interchangeably used when assessing the grading of PNET patients and evaluating tumor aggressiveness. Increased DOTATATE uptake indicates SSTR overexpression, which can identify patients to utilize peptide receptor radionuclide therapy (PPRT) [29] and may predict treatment response [30]. The DOTATATE and ADC values may provide complementary information to aid clinical decision-making and prognostication.
A key limitation of this study is the small size of the recruited patient population. As PNETs are a rare tumor type and dual-tracer PET/MR-based grading and staging of primary PNETs are only performed in some cases, however, recruiting a larger patient cohort will require future large-scale prospective research efforts. In addition, T staging was not taken into consideration in this study as they were high-grade PNET patients who could only undergo follow-up and were not eligible for surgical treatment.
Conclusions
In summary, these analyses of 18F-FDG and 68Ga-DOTATATE dual-tracer PET/MR parameters in PNET patients revealed MR-derived ADCmin values to be negatively correlated with 18F-FDG-derived MTV, TLG, and FSUVmax values. As such, 68Ga-DOTATATE PET/MR scanning alone is likely to be sufficient as a means of assessing the grading and staging of primary PNET tumors.
Availability of data and materials
All data in our study are available from the corresponding authors upon reasonable request.
Abbreviations
- PNET:
-
Pancreatic neuroendocrine tumor
- PET/MR:
-
Positron emission tomography/magnetic resonance
- DWI:
-
Diffusion-weighted imaging
- ADC:
-
Apparent diffusion coefficient
- VOI:
-
Volume of interest
- SUVmax:
-
Maximum standardized uptake value
- MTV:
-
Metabolic tumor volume
- TLG:
-
Total lesion glycolysis
References
Cives M, Strosberg JR. Gastroenteropancreatic neuroendocrine tumors. CA Cancer J Clin. 2018;68:471–87. https://doi.org/10.3322/caac.21493.
Hong X, Qiao S, Li F, Wang W, Jiang R, Wu H, et al. Whole-genome sequencing reveals distinct genetic bases for insulinomas and non-functional pancreatic neuroendocrine tumours: leading to a new classification system. Gut. 2020;69:877–87. https://doi.org/10.1136/gutjnl-2018-317233.
Scarpa A, Mantovani W, Capelli P, Beghelli S, Boninsegna L, Bettini R, et al. Pancreatic endocrine tumors: improved TNM staging and histopathological grading permit a clinically efficient prognostic stratification of patients. Mod Pathol Off J U S Can Acad Pathol. 2010;23:824–33. https://doi.org/10.1038/modpathol.2010.58.
Wang M, Ding D, Qin T, Wang H, Liu Y, Liu J, et al. New staging classification for pancreatic neuroendocrine neoplasms combining TNM stage and WHO grade classification. Cancer Lett. 2021;518:207–13. https://doi.org/10.1016/j.canlet.2021.07.018.
Sawicki LM, Deuschl C, Beiderwellen K, Ruhlmann V, Poeppel TD, Heusch P, et al. Evaluation of (68)Ga-DOTATOC PET/MRI for whole-body staging of neuroendocrine tumours in comparison with (68)Ga-DOTATOC PET/CT. Eur Radiol. 2017;27:4091–9. https://doi.org/10.1007/s00330-017-4803-2.
Lee H, Nakamoto R, Moore SE, Pantel AR, Eads JR, Aparici CM, et al. Combined quantification of (18)F-FDG and (68)Ga-DOTATATE PET/CT for prognosis in high-grade gastroenteropancreatic neuroendocrine neoplasms. Acad Radiol. 2021. https://doi.org/10.1016/j.acra.2021.10.004.
Rufini V, Lorusso M, Inzani F, Pasciuto T, Triumbari EKA, Grillo LR, et al. Correlation of somatostatin receptor PET/CT imaging features and immunohistochemistry in neuroendocrine tumors of the lung: a retrospective observational study. Eur J Nucl Med Mol Imaging. 2022. https://doi.org/10.1007/s00259-022-05848-z.
Mapelli P, Bezzi C, Palumbo D, Canevari C, Ghezzo S, Samanes Gajate AM, et al. (68)Ga-DOTATOC PET/MR imaging and radiomic parameters in predicting histopathological prognostic factors in patients with pancreatic neuroendocrine well-differentiated tumours. Eur J Nucl Med Mol Imaging. 2022;49:2352–63. https://doi.org/10.1007/s00259-022-05677-0.
Ezziddin S, Adler L, Sabet A, Pöppel TD, Grabellus F, Yüce A, et al. Prognostic stratification of metastatic gastroenteropancreatic neuroendocrine neoplasms by 18F-FDG PET: feasibility of a metabolic grading system. J Nucl Med Off Publ Soc Nucl Med. 2014;55:1260–6. https://doi.org/10.2967/jnumed.114.137166.
Besa C, Ward S, Cui Y, Jajamovich G, Kim M, Taouli B. Neuroendocrine liver metastases: value of apparent diffusion coefficient and enhancement ratios for characterization of histopathologic grade. J Magn Reson Imaging JMRI. 2016;44:1432–41. https://doi.org/10.1002/jmri.25320.
Wang Y, Chen ZE, Yaghmai V, Nikolaidis P, McCarthy RJ, Merrick L, et al. Diffusion-weighted MR imaging in pancreatic endocrine tumors correlated with histopathologic characteristics. J Magn Reson Imaging JMRI. 2011;33:1071–9. https://doi.org/10.1002/jmri.22541.
Bos R, van Der Hoeven JJ, van Der Wall E, van Der Groep P, van Diest PJ, Comans EF, et al. Biologic correlates of (18)fluorodeoxyglucose uptake in human breast cancer measured by positron emission tomography. J Clin Oncol Off J Am Soc Clin Oncol. 2002;20:379–87. https://doi.org/10.1200/jco.2002.20.2.379.
Mosavi F, Wassberg C, Selling J, Molin D, Ahlström H. Whole-body diffusion-weighted MRI and (18)F-FDG PET/CT can discriminate between different lymphoma subtypes. Clin Radiol. 2015;70:1229–36. https://doi.org/10.1016/j.crad.2015.06.087.
Choi SH, Paeng JC, Sohn CH, Pagsisihan JR, Kim YJ, Kim KG, et al. Correlation of 18F-FDG uptake with apparent diffusion coefficient ratio measured on standard and high b value diffusion MRI in head and neck cancer. J Nucl Med Off Publ Soc Nucl Med. 2011;52:1056–62. https://doi.org/10.2967/jnumed.111.089334.
Nagtegaal ID, Odze RD, Klimstra D, Paradis V, Rugge M, Schirmacher P, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020;76:182–8. https://doi.org/10.1111/his.13975.
Luo G, Javed A, Strosberg JR, ** K, Zhang Y, Liu C, et al. Modified staging classification for pancreatic neuroendocrine tumors on the basis of the American Joint Committee on Cancer and European Neuroendocrine Tumor Society Systems. J Clin Oncol Off J Am Soc Clin Oncol. 2017;35:274–80. https://doi.org/10.1200/jco.2016.67.8193.
Nioche C, Orlhac F, Boughdad S, Reuzé S, Goya-Outi J, Robert C, et al. LIFEx: a freeware for radiomic feature calculation in multimodality imaging to accelerate advances in the characterization of tumor heterogeneity. Can Res. 2018;78:4786–9. https://doi.org/10.1158/0008-5472.Can-18-0125.
Abdulrezzak U, Kurt YK, Kula M, Tutus A. Combined imaging with 68Ga-DOTA-TATE and 18F-FDG PET/CT on the basis of volumetric parameters in neuroendocrine tumors. Nucl Med Commun. 2016;37:874–81. https://doi.org/10.1097/mnm.0000000000000522.
Chan DL, Bernard EJ, Schembri G, Roach PJ, Johnson M, Pavlakis N, et al. High metabolic tumour volume on 18-fluorodeoxyglucose positron emission tomography predicts poor survival from neuroendocrine neoplasms. Neuroendocrinology. 2020;110:950–8. https://doi.org/10.1159/000504673.
Qu YH, Long N, Ran C, Sun J. The correlation of (18)F-FDG PET/CT metabolic parameters, clinicopathological factors, and prognosis in breast cancer. Clin Transl Oncol Off Publ Fed Span Oncol Soc Natl Cancer Inst Mexico. 2021;23:620–7. https://doi.org/10.1007/s12094-020-02457-w.
Wang Y, Bai G, Zhang X, Shan W, Xu L, Chen W. Correlation analysis of apparent diffusion coefficient value and P53 and Ki-67 expression in esophageal squamous cell carcinoma. Magn Reson Imaging. 2020;68:183–9. https://doi.org/10.1016/j.mri.2020.01.011.
Schob S, Meyer J, Gawlitza M, Frydrychowicz C, Müller W, Preuss M, et al. Diffusion-weighted MRI reflects proliferative activity in primary CNS lymphoma. PLoS ONE. 2016;11:e0161386. https://doi.org/10.1371/journal.pone.0161386.
Langen Stokmo H, Aly M, Bowitz Lothe IM, Borja AJ, Mehdizadeh Seraj S, Ghorpade R, et al. Volumetric parameters from [(18) F]FDG PET/CT predicts survival in patients with high-grade gastroenteropancreatic neuroendocrine neoplasms. J Neuroendocrinol. 2022. https://doi.org/10.1111/jne.13170.
De Robertis R, Cingarlini S, Tinazzi Martini P, Ortolani S, Butturini G, Landoni L, et al. Pancreatic neuroendocrine neoplasms: magnetic resonance imaging features according to grade and stage. World J Gastroenterol. 2017;23:275–85. https://doi.org/10.3748/wjg.v23.i2.275.
Freihat O, Zoltán T, Pinter T, Kedves A, Sipos D, Repa I, et al. Correlation between tissue cellularity and metabolism represented by diffusion-weighted imaging (DWI) and 18F-FDG PET/MRI in head and neck cancer (HNC). Cancers. 2022. https://doi.org/10.3390/cancers14030847.
Jeong JH, Cho IH, Chun KA, Kong EJ, Kwon SD, Kim JH. Correlation between apparent diffusion coefficients and standardized uptake values in hybrid (18)F-FDG PET/MR: preliminary results in rectal cancer. Nucl Med Mol Imaging. 2016;50:150–6. https://doi.org/10.1007/s13139-015-0390-9.
Hu S, **ng X, Liu J, Liu X, Li J, ** W, et al. Correlation between apparent diffusion coefficient and tumor-stroma ratio in hybrid (18)F-FDG PET/MRI: preliminary results of a rectal cancer cohort study. Quant Imaging Med Surg. 2022;12:4213–25. https://doi.org/10.21037/qims-21-938.
Lee EJ, terBrugge K, Mikulis D, Choi DS, Bae JM, Lee SK, et al. Diagnostic value of peritumoral minimum apparent diffusion coefficient for differentiation of glioblastoma multiforme from solitary metastatic lesions. AJR Am J Roentgenol. 2011;196:71–6. https://doi.org/10.2214/ajr.10.4752.
Ambrosini V, Kunikowska J, Baudin E, Bodei L, Bouvier C, Capdevila J, et al. Consensus on molecular imaging and theranostics in neuroendocrine neoplasms. Eur J Cancer (Oxford, England: 1990). 2021;146:56–73. https://doi.org/10.1016/j.ejca.2021.01.008.
Sharma R, Wang WM, Yusuf S, Evans J, Ramaswami R, Wernig F, et al. (68)Ga-DOTATATE PET/CT parameters predict response to peptide receptor radionuclide therapy in neuroendocrine tumours. Radiother Oncol J Eur Soc Ther Radiol Oncol. 2019;141:108–15. https://doi.org/10.1016/j.radonc.2019.09.003.
Acknowledgements
Not applicable.
Funding
This research was supported by the National Natural Science Foundation of China (NSFC: 81971644), the Guangci Clinical New Technology Sailing Plan of Rui** Hospital (YW20210025), the Shanghai Jiaotong University School of Medicine (KY20192098), and the Shanghai Municipal Key Clinical Specialty (shslczdzk03403).
Author information
Authors and Affiliations
Contributions
Study concept and design: YFZ. Acquisition and interpretation of image: JG and HJJ. Analysis and interpretation of data: JG and SX. Draft of the initial manuscript: JG. Further review and editing of the manuscript: YFZ and YP. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This retrospective research was approved by Rui** Hospital Ethics Committee, Shanghai Jiao Tong University School of Medicine (Reference number: 2020-52), and the written informed consent was waived. All procedures were performed in accordance with the 1964 Helsinki declaration and its later amendments and comparable ethical standards.
Consent for publication
Not applicable.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gao, J., Xu, S., Ju, H. et al. The potential application of MR-derived ADCmin values from 68Ga-DOTATATE and 18F-FDG dual tracer PET/MR as replacements for FDG PET in assessment of grade and stage of pancreatic neuroendocrine tumors. EJNMMI Res 13, 10 (2023). https://doi.org/10.1186/s13550-023-00960-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13550-023-00960-z