
Abstract
Background
Gastrointestinal symptoms and inflammatory gastrointestinal diseases exist at higher rates in the autistic population. It is not clear however whether autism is associated with elevated gastrointestinal inflammation as studies examining non-invasive faecal biomarkers report conflicting findings. To understand the research landscape and identify gaps, we performed a systematic review and meta-analysis of studies measuring non-invasive markers of gastrointestinal inflammation in autistic and non-autistic samples. Our examination focused on faecal biomarkers as sampling is non-invasive and these markers are a direct reflection of inflammatory processes in the gastrointestinal tract.
Methods
We extracted data from case–control studies examining faecal markers of gastrointestinal inflammation. We searched PubMed, Embase, Cochrane CENTRAL, CINAHL, PsycINFO, Web of Science Core Collection and Epistemonikos and forward and backwards citations of included studies published up to April 14, 2023 (PROSPERO CRD42022369279).
Results
There were few studies examining faecal markers of gastrointestinal inflammation in the autistic population, and many established markers have not been studied. Meta-analyses of studies examining calprotectin (n = 9) and lactoferrin (n = 3) were carried out. A total of 508 autistic children and adolescents and 397 non-autistic children and adolescents were included in the meta-analysis of calprotectin studies which found no significant group differences (ROM: 1.30 [0.91, 1.86]). Estimated differences in calprotectin were lower in studies with siblings and studies which did not exclude non-autistic controls with gastrointestinal symptoms. A total of 139 autistic participants and 75 non-autistic controls were included in the meta-analysis of lactoferrin studies which found no significant group differences (ROM: 1.27 [0.79, 2.04]).
Limitations
All studies included in this systematic review and meta-analysis examined children and adolescents. Many studies included non-autistic controls with gastrointestinal symptoms which limit the validity of their findings. The majority of studies of gastrointestinal inflammation focused on children under 12 with few studies including adolescent participants. Most studies that included participants aged four or under did not account for the impact of age on calprotectin levels. Future studies should screen for relevant confounders, include larger samples and explore gastrointestinal inflammation in autistic adolescents and adults.
Conclusions
There is no evidence to suggest higher levels of gastrointestinal inflammation as measured by calprotectin and lactoferrin are present in autistic children and adolescents at the population level. Preliminary evidence suggests however that higher calprotectin levels may be present in a subset of autistic participants, who may be clinically characterised by more severe gastrointestinal symptoms and higher levels of autistic traits.
Similar content being viewed by others


Introduction
Autism is a neurodevelopmental condition associated with increased rates of co-occurring medical conditions including gastrointestinal (GI) disorders [1]. In addition, several studies report higher rates of GI symptoms in paediatric [2, 3] and adult autistic populations [4]. Higher GI symptom rates in autism likely stem from a combination of multifactorial causes, involving genetic, environmental, and behavioural factors. Several gene mutations linked to autism are associated with GI symptoms including impaired motility, constipation and gastro-oesophageal reflux (e.g. CHD8, NOS1, FOXP1 and TCF4) [5]. Autistic traits, such as high levels of restricted and repetitive behaviours and interests, are also associated with less diverse diets in some autistic people [6], which could exacerbate GI issues and contribute to microbial dysbiosis [7]. GI issues interact with other conditions and may worsen sleep problems and increase rates of self-injurious and aggressive behaviours, particularly among non-verbal autistic children [8,9,10]. Higher rates of internalising symptoms, including anxiety and social withdrawal, which present at elevated rates in the autistic population, have a bidirectional relationship with GI problems such as constipation, diarrhoea, nausea, and stomach pain [11].
There has been little research examining whether these higher rates of GI symptoms are associated with dysregulated immune responses within the GI tract, prompting investigations into whether low-grade GI inflammation is present in the autistic population [12]. Epidemiological evidence from a recent meta-analysis suggests that autistic people are more likely to be diagnosed with inflammatory bowel disease (IBD) than non-autistic people highlighting the need to screen for GI inflammation in the autistic population [13]. Comparisons of endoscopic findings have been limited to small sample sizes and have found conflicting evidence as to whether GI inflammation is present in the autistic population [3, 14]. While endoscopy remains the gold standard to identify GI inflammation, inflammatory biomarkers measured in faecal samples are often used in research and clinical settings as non-invasive markers of GI inflammation to avoid the risks of endoscopy and general anaesthesia [15, 16]. The direct contact with mucosa of the GI tract makes faecal biomarkers a more direct, non-invasive marker of intestinal inflammation than plasma or serum biomarkers which could be elevated by non-GI causes of inflammation [17].
Biomarkers of interest include calprotectin and S100 calcium binding protein A12 (S100A12) which are released by neutrophils, monocytes and infiltrating macrophages in response to inflammation in the GI tract [17,18,19]. Other markers of interest include lactoferrin and secretory Immunoglobulin A (IgA) which are anti-inflammatory glycoproteins secreted by macrophages [15, 18]. Faecal measurements of the dimeric M2-isoform of pyruvate kinase (M2-PK), which is associated with increased cell turnover in the GI tract, is also used as a marker of GI inflammation [15, 19, 20]. Lysozymes are antimicrobial enzymes produced by neutrophils and neopterin which is released by activated T-lymphocytes, and macrophages have also been found to be upregulated in IBD [19]. Alpha1-antitrypsin (AAT), a serine protease inhibitor produced by a range of cells including: hepatocytes, neutrophils, monocytes-macrophages, enterocytes, and Paneth cells, and polymorphonuclear neutrophil elastase (PMN-E), a serine protease produced by neutrophils, are both upregulated in response to GI inflammation [19]. GI symptoms in autism have been explored in relation to the microbiome [21]; however, evidence of GI abnormalities as reflected in faecal biomarkers of inflammation has been conflicting. Given higher rates of GI symptoms in the autistic population and concerns of higher rates of inflammation-driven GI conditions, this paper sought to conduct a systematic review of markers of faecal markers of GI inflammation.
Materials and methods
The systematic review and meta-analysis were undertaken and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement [22] and was pre-registered on PROSPERO (CRD42022369279).
Literature search
We searched PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL, PsycINFO, Web of Science Core Collection and Epistemonikos using strategies developed for each database (Additional file 1). Scopus and Web of Science were used to examine backwards and forwards citations of all studies included in this review.
Selection of studies
The titles and abstracts of all studies retrieved by the search were reviewed by two researchers (NM and DM). The full texts of relevant studies were then screened by NM to identify eligible studies that met the inclusion and exclusion criteria. The criteria for inclusion were (1) the measurement of inflammatory biomarkers in faeces (2) autism diagnoses confirmed by standardised diagnostic tools or by a medical professional in line with the criteria outlined in the DSM-III, IV or 5 or ICD-10 or 11. The exclusion criteria were (1) studies of biopsies and endoscopies, as the focus of this review is on biospecimens collected using minimally invasive sampling procedures, (2) studies that did not provide data as absolute concentrations (e.g. relative data reported by Western blots) or insufficient information regarding the method of data quantification, (3) studies that only report data from analyses of the microbiome, as the focus of this meta-analysis is on markers of GI inflammation.
Data extraction and risk of bias
The means and standard deviations of the faecal biomarker levels in autistic and non-autistic cohorts were extracted if available. If means and standard deviations were not reported, they were derived from sample size, median, IQR, minimum, or maximum values [23]. Risk of bias in all included studies was assessed using a study specific adaptation of the Newcastle–Ottawa Scale (NOS) for case–control studies carried out by two researchers (NM and DM) (Additional file 1). We extracted the following data from all included studies: the age and sex of participants, measurement of concurrent psychiatric or medical conditions, country of publication and publication year, details of recruitment settings, any variables used to match participants, method of faecal biomarker quantification. As considerable interassay variability has been reported between different commercial calprotectin assays [24,25,26], details of the assays used by individual studies were also extracted. To examine the generalisability of the literature, the inclusion of autistic participants with limited verbal and/or cognitive abilities was also coded based on reports of communication ability, adaptive functioning or cognitive ability in line with the criteria developed by Stedman et al. [27].
Statistical analysis
Meta-analyses were performed when at least two studies that could be combined were identified. Random-effects meta-analyses were conducted in R 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria) using the metafor package. To control for the substantial variability in biomarker concentrations between laboratories and assays, the ratio of mean (RoM) faecal biomarker levels in autistic and non-autistic cohorts and standard errors were generated for each comparison, log transformed and pooled for meta-analysis [28]. Standardised mean differences were also calculated and pooled for all analyses. All major findings remained consistent with the analysis of RoM (Additional file 2: Figs. S1, S2). When multiple autistic cohorts were present within a single study, autistic cohorts were combined for the main analysis. When multiple control cohorts were present, individual ratios were generated. Heterogeneity was assessed using I2 [29].
Results
Systemic review of faecal biomarkers of inflammation
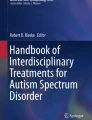
Many inflammatory markers used in studies of GI inflammation (e.g. M2-PK, S100A12, AAT) have not been examined in the autistic population. Single studies found lower faecal levels of lysozyme, particularly among those with higher probiotic usage [30], cortisol and glutamate metabolites [31] and comparable levels of PMN-E [30] among autistic participants relative to controls. A small Swedish study found that elevated rectal nitric oxide levels, defined as levels above < 250 parts per billion, were reported in 27% of surveyed autistic participants (6/22) and in 9% of surveyed controls (2/22) [32] (Fig. 1).

PRISMA flow diagram of search for faecal biomarkers in autism
Two studies examined the levels of secretory IgA in faecal samples, but the results of these studies could not be synthesised as one study reported results as optical densities rather than concentrations. Adams et al. found comparable levels of faecal IgA concentrations in 39 control children and adolescents and 58 autistic children and adolescents, (55 participants with a DSM-IV diagnosis of Autistic disorder and 3 with a diagnosis of Asperger’s disorder) [30]. Zhou et al. [ All data used for the meta-analysis is available in Additional file 3. Tye C, Runicles AK, Whitehouse AJ, Alvares GA. Characterizing the interplay between autism spectrum disorder and comorbid medical conditions: an integrative review. Front Psychiatry. 2018. https://doi.org/10.3389/fpsyt.2018.00751. McElhanon BO, McCracken C, Karpen S, Sharp WG. Gastrointestinal symptoms in autism spectrum disorder: a meta-analysis. Pediatrics. 2014;133(5):872–83. https://doi.org/10.1542/peds.2013-3995. Holingue C, Newill C, Lee L-C, Pasricha PJ, Daniele FM. Gastrointestinal symptoms in autism spectrum disorder: a review of the literature on ascertainment and prevalence. Autism Res. 2018;11(1):24–36. https://doi.org/10.1002/aur.1854. Warreman EB, Nooteboom LA, Terry MB, Hoek HW, Leenen PJM, VanRossum EFC, et al. Psychological, behavioural and biological factors associated with gastrointestinal symptoms in autistic adults and adults with autistic traits. Autism. 2023. https://doi.org/10.1177/13623613231155324. Niesler B, Rappold GA. Emerging evidence for gene mutations driving both brain and gut dysfunction in autism spectrum disorder. Mol Psychiatry. 2021;26(5):1442–4. https://doi.org/10.1038/s41380-020-0778-5. Mathew NE, Mallitt KA, Masi A, Katz T, Walker AK, Morris MJ, et al. Dietary intake in children on the autism spectrum is altered and linked to differences in autistic traits and sensory processing styles. Autism Res. 2022;15(10):1824–39. https://doi.org/10.1002/aur.2798. Yap CX, Henders AK, Alvares GA, Wood DLA, Krause L, Tyson GW, et al. Autism-related dietary preferences mediate autism-gut microbiome associations. Cell. 2021;184(24):5916-31.e17. https://doi.org/10.1016/j.cell.2021.10.015. Chakraborty P, Carpenter KLH, Major S, Deaver M, Vermeer S, Herold B, et al. Gastrointestinal problems are associated with increased repetitive behaviors but not social communication difficulties in young children with autism spectrum disorders. Autism. 2021;25(2):405–15. https://doi.org/10.1177/1362361320959503. Restrepo B, Angkustsiri K, Taylor SL, Rogers SJ, Cabral J, Heath B, et al. Developmental–behavioral profiles in children with autism spectrum disorder and co-occurring gastrointestinal symptoms. Autism Res. 2020;13(10):1778–89. https://doi.org/10.1002/aur.2354. Prosperi M, Santocchi E, Muratori F, Narducci C, Calderoni S, Tancredi R, et al. Vocal and motor behaviors as a possible expression of gastrointestinal problems in preschoolers with Autism Spectrum Disorder. BMC Pediatr. 2019;19(1):466. https://doi.org/10.1186/s12887-019-1841-8. Dovgan K, Gynegrowski K, Ferguson BJ. Bidirectional relationship between internalizing symptoms and gastrointestinal problems in youth with Autism Spectrum Disorder. J Autism Dev Disord. 2022. https://doi.org/10.1007/s10803-022-05539-6. Al-Ayadhi L, Zayed N, Bhat RS, Moubayed NMS, Al-Muammar MN, El-Ansary A. The use of biomarkers associated with leaky gut as a diagnostic tool for early intervention in autism spectrum disorder: a systematic review. Gut Pathogens. 2021;13(1):54. https://doi.org/10.1186/s13099-021-00448-y. Kim JY, Choi MJ, Ha S, Hwang J, Koyanagi A, Dragioti E, et al. Association between autism spectrum disorder and inflammatory bowel disease: a systematic review and meta-analysis. Autism Res. 2022;15(2):340–52. https://doi.org/10.1002/aur.2656. Kushak RI, Buie TM, Murray KF, Newburg DS, Chen C, Nestoridi E, et al. Evaluation of intestinal function in children with autism and gastrointestinal symptoms. J Pediatr Gastroenterol Nutr. 2016;62(5):687–91. https://doi.org/10.1097/mpg.0000000000001174. Pang T, Leach ST, Katz T, Day AS, Ooi CY. Fecal biomarkers of intestinal health and disease in children. Front Pediatr. 2014;2:6. https://doi.org/10.3389/fped.2014.00006. Bromke MA, Neubauer K, Kempiński R, Krzystek-Korpacka M. Faecal calprotectin in assessment of mucosal healing in adults with inflammatory bowel disease: a meta-analysis. J Clin Med. 2021;10(10):2203. https://doi.org/10.3390/jcm10102203. Manolakis AC, Kapsoritakis AN, Georgoulias P, Tzavara C, Valotassiou V, Kapsoritaki A, et al. Moderate performance of serum S100A12, in distinguishing inflammatory bowel disease from irritable bowel syndrome. BMC Gastroenterol. 2010;10:1–7. https://doi.org/10.1186/1471-230X-10-118. Siddiqui I, Majid H, Abid S. Update on clinical and research application of fecal biomarkers for gastrointestinal diseases. World J Gastrointest Pharmacol Ther. 2017;8(1):39. https://doi.org/10.4292/wjgpt.v8.i1.39. Di Ruscio M, Vernia F, Ciccone A, Frieri G, Latella G. Surrogate fecal biomarkers in inflammatory bowel disease: rivals or complementary tools of fecal calprotectin? Inflamm Bowel Dis. 2018;24(1):78–92. https://doi.org/10.1093/ibd/izx011. Sherwood RA. Faecal markers of gastrointestinal inflammation. J Clin Pathol. 2012;65(11):981–5. https://doi.org/10.1136/jclinpath-2012-200901. West KA, Yin X, Rutherford EM, Wee B, Choi J, Chrisman BS, et al. Multi-angle meta-analysis of the gut microbiome in Autism Spectrum Disorder: a step toward understanding patient subgroups. Sci Rep. 2022;12(1):17034. https://doi.org/10.1038/s41598-022-21327-9. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9. https://doi.org/10.7326/0003-4819-151-4-200908180-00135. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:1–13. https://doi.org/10.1186/1471-2288-14-135. Whitehead SJ, French J, Brookes MJ, Ford C, Gama R. Between-assay variability of faecal calprotectin enzyme-linked immunosorbent assay kits. Ann Clin Biochem. 2013;50(Pt 1):53–61. https://doi.org/10.1258/acb.2012.011272. Labaere D, Smismans A, Van Olmen A, Christiaens P, D’Haens G, Moons V, et al. Comparison of six different calprotectin assays for the assessment of inflammatory bowel disease. United Eur Gastroenterol J. 2014;2(1):30–7. https://doi.org/10.1177/2050640613518201. Goll R, Heitmann R, Moe ØK, Carlsen K, Florholmen J. Head to head comparison of two commercial fecal calprotectin kits as predictor of Mayo endoscopic sub-score and mucosal TNF expression in ulcerative colitis. PLoS ONE. 2019;14(12):e0224895. https://doi.org/10.1371/journal.pone.0224895. Stedman A, Taylor B, Erard M, Peura C, Siegel M. Are children severely affected by autism spectrum disorder underrepresented in treatment studies? An analysis of the literature. J Autism Dev Disord. 2019;49(4):1378–90. https://doi.org/10.1007/s10803-018-3844-y. Friedrich JO, Adhikari NKJ, Beyene J. The ratio of means method as an alternative to mean differences for analyzing continuous outcome variables in meta-analysis: a simulation study. BMC Med Res Methodol. 2008;8(1):32. https://doi.org/10.1186/1471-2288-8-32. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58. https://doi.org/10.1002/sim.1186. Adams JB, Johansen LJ, Powell LD, Quig D, Rubin RA. Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011;11(1):1–13. https://doi.org/10.1186/1471-230X-11-22. Wang M, Wan J, Rong H, He F, Wang H, Zhou J, et al. Alterations in gut glutamate metabolism associated with changes in gut microbiota composition in children with autism spectrum disorder. mSystems. 2019;4(1):e0032118. https://doi.org/10.1128/mSystems.00321-18. Fernell E, Fagerberg UL, Hellström PM. No evidence for a clear link between active intestinal inflammation and autism based on analyses of faecal calprotectin and rectal nitric oxide. Acta Paediatr (Oslo, Norway: 1992). 2007;96(7):1076–9. https://doi.org/10.1111/j.1651-2227.2007.00298.x. Zhou J, He F, Yang F, Yang Z, **e Y, Zhou S, et al. Increased stool immunoglobulin A level in children with autism spectrum disorders. Res Dev Disabil. 2018;82:90–4. https://doi.org/10.1016/j.ridd.2017.10.009. Wang M, Zhou J, He F, Cai C, Wang H, Wang Y, et al. Alteration of gut microbiota-associated epitopes in children with autism spectrum disorders. Brain Behav Immun. 2019;75:192–9. https://doi.org/10.1016/j.bbi.2018.10.006. Laghi L, Mastromarino P, Prosperi M, Morales MA, Calderoni S, Santocchi E, et al. Are fecal metabolome and microbiota profiles correlated with autism severity? A cross-sectional study on ASD preschoolers. Metabolites. 2021;11(10):654. https://doi.org/10.3390/metabo11100654. De Magistris L, Familiari V, Pascotto A, Sapone A, Frolli A, Iardino P, et al. Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives. J Pediatr Gastroenterol Nutr. 2010;51(4):418–24. https://doi.org/10.1097/MPG.0b013e3181dcc4a5. Yitik Tonkaz G, Esin IS, Turan B, Uslu H, Dursun OB. Determinants of leaky gut and gut microbiota differences in children with autism spectrum disorder and their siblings. J Autism Dev Disord. 2022;53:2703–16. https://doi.org/10.1007/s10803-022-05540-z. Alookaran J, Liu Y, Auchtung TA, Tahanan A, Hessabi M, Asgarisabet P, et al. Fungi: friend or foe? A mycobiome evaluation in children with autism and gastrointestinal symptoms. J Pediatr Gastroenterol Nutr. 2022. https://doi.org/10.1097/MPG.0000000000003349. Azouz HG, El-din Zakaria NH, Fouad Khalil A, Mohammad Naguib S, Khalil M. Gastrointestinal manifestations and their relation to faecal calprotectin in children with autism. Gastroenterol Rev. 2021;16(4):352–7. https://doi.org/10.5114/pg.2021.111420. Babinská K, Tomova A, Celušáková H, Babková J, Repiská G, Kubranská A, et al. Fecal calprotectin levels correlate with main domains of the autism diagnostic interview-revised (ADI-R) in a sample of individuals with autism spectrum disorders from Slovakia. Physiol Res. 2017;66(Suppl 4):S517–22. https://doi.org/10.33549/physiolres.933801. Iovene MR, Bombace F, Maresca R, Sapone A, Iardino P, Picardi A, et al. Intestinal dysbiosis and yeast isolation in stool of subjects with autism spectrum disorders. Mycopathologia. 2017;182(3–4):349–63. https://doi.org/10.1007/s11046-016-0068-6. Pusponegoro HD, Ismael S, Sastroasmoro S, Firmansyah A, Vandenplas Y. Maladaptive behavior and gastrointestinal disorders in children with autism spectrum disorder. J Pediatr Gastroenterol Nutr. 2015;18(4):230–7. https://doi.org/10.5223/pghn.2015.18.4.230. Strati F, Cavalieri D, Albanese D, De Felice C, Donati C, Hayek J, et al. New evidences on the altered gut microbiota in autism spectrum disorders. Microbiome. 2017;5(1):24. https://doi.org/10.1186/s40168-017-0242-1. Tomova A, Soltys K, Repiska G, Palkova L, Filcikova D, Minarik G, et al. Specificity of gut microbiota in children with autism spectrum disorder in Slovakia and its correlation with astrocytes activity marker and specific behavioural patterns. Physiol Behav. 2020;214:112745. https://doi.org/10.1016/j.physbeh.2019.112745. Fagerberg UL, Lööf L, Merzoug RD, Hansson L-O, Finkel Y. Fecal Calprotectin levels in healthy children studied with an improved assay. J Pediatr Gastroenterol Nutr. 2003. https://doi.org/10.1097/00005176-200310000-00013. Martirosian G, Ekiel A, Aptekorz M, Wiechuła B, Kazek B, Jankowska-Steifer E, et al. Fecal lactoferrin and Clostridium spp. in stools of autistic children. Anaerobe. 2011;17(1):43–5. https://doi.org/10.1016/j.anaerobe.2010.12.003. Koninckx CR, Donat E, Benninga MA, Broekaert IJ, Gottrand F, Kolho K-L, et al. The use of fecal calprotectin testing in paediatric disorders: a position paper of the European Society for Paediatric Gastroenterology and Nutrition Gastroenterology Committee. J Pediatr Gastroenterol Nutr. 2021;72(4):617–40. https://doi.org/10.1097/MPG.0000000000003046. Gorrindo P, Williams KC, Lee EB, Walker LS, McGrew SG, Levitt P. Gastrointestinal dysfunction in autism: parental report, clinical evaluation, and associated factors. Autism Res: Off J Int Soc Autism Res. 2012;5(2):101–8. https://doi.org/10.1002/aur.237. Penzol MJ, Salazar de Pablo G, Llorente C, Moreno C, Hernández P, Dorado ML, et al. Functional gastrointestinal disease in autism spectrum disorder: a retrospective descriptive study in a clinical sample. Front Psychiatry. 2019;10:179. https://doi.org/10.3389/fpsyt.2019.00179. Flagstad G, Helgeland H, Markestad T. Faecal calprotectin concentrations in children with functional gastrointestinal disorders diagnosed according to the Pediatric Rome III criteria. Acta Paediatr. 2010;99(5):734–7. https://doi.org/10.1111/j.1651-2227.2010.01698.x. Luna RA, Oezguen N, Balderas M, Venkatachalam A, Runge JK, Versalovic J, et al. Distinct microbiome-neuroimmune signatures correlate with functional abdominal pain in children with autism spectrum disorder. Cell Mol Gastroenterol Hepatol. 2017;3(2):218–30. https://doi.org/10.1016/j.jcmgh.2016.11.008. Ibrahim SH, Voigt RG, Katusic SK, Weaver AL, Barbaresi WJ. Incidence of gastrointestinal symptoms in children with autism: a population-based study. Pediatrics. 2009;124(2):680–6. https://doi.org/10.1542/peds.2008-2933. Harris HA, Micali N, Moll HA, van Berckelaer-Onnes I, Hillegers M, Jansen PW. The role of food selectivity in the association between child autistic traits and constipation. Int J Eat Disord. 2021;54(6):981–5. https://doi.org/10.1002/eat.23485. Bjarnason I. The use of fecal calprotectin in inflammatory bowel disease. Gastroenterol Hepatol. 2017;13(1):53–6. Jha AK, Chaudhary M, Dayal VM, Kumar A, Jha SK, Jha P, et al. Optimal cut-off value of fecal calprotectin for the evaluation of ulcerative colitis: an unsolved issue? JGH Open. 2018;2(5):207–13. https://doi.org/10.1002/jgh3.12074. Holingue C, Poku O, Pfeiffer D, Murray S, Fallin MD. Gastrointestinal concerns in children with autism spectrum disorder: a qualitative study of family experiences. Autism. 2022;26(7):1698–711. https://doi.org/10.1177/13623613211062667. Bramati-Castellarin I, Patel V, Drysdale I. Faecal calprotectin and a twenty-four-parameter questionnaire in autistic children with gastrointestinal symptoms. SM J Psychiatry Mental Health. 2017;2:1009. Adams JB, Johansen LJ, Powell LD, Quig D, Rubin RA. Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011;11:22. https://doi.org/10.1186/1471-230x-11-22. Schneiderman N, Ironson G, Siegel SD. Stress and health: psychological, behavioral, and biological determinants. Annu Rev Clin Psychol. 2005;1:607–28. https://doi.org/10.1146/annurev.clinpsy.1.102803.144141. Lichtiger S, Present DH, Kornbluth A, Gelernt I, Bauer J, Galler G, et al. Cyclosporine in severe ulcerative colitis refractory to steroid therapy. N Engl J Med. 1994;330(26):1841–5. https://doi.org/10.1056/NEJM199406303302601. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480–91. https://doi.org/10.1053/j.gastro.2005.11.061. Lord C, Rutter M, DiLavore P, Risi S, Gotham K, Bishop S. Autism diagnostic observation schedule, (ADOS-2) modules 1–4. Western Psychological Services; 2012. Schopler E, Reichler R, Rochen Renner B. The childhood autism rating scale. Western Psychological Services; 1998. Cohen IL SV. The PDD behavior inventory. Psychological Assessment Resources; 2005. Rutter M, Le Couteur A, Lord C. The autism diagnostic interview—revised (ADI-R). Los Angeles: Western Psychological Services; 2003. Tomova A, Keményová P, Filčíková D, Szapuová Ž, Kováč A, Babinská K, et al. Plasma levels of glial cell marker S100B in children with autism. Physiol Res. 2019;68(Suppl 3):S315–23. https://doi.org/10.33549/physiolres.934350. Butwicka A, Olén O, Larsson H, Halfvarson J, Almqvist C, Lichtenstein P, et al. Association of childhood-onset inflammatory bowel disease with risk of psychiatric disorders and suicide attempt. JAMA Pediatr. 2019;173(10):969–78. https://doi.org/10.1001/jamapediatrics.2019.2662. Mari A, Baker FA, Mahamid M, Yacoob A, Sbeit W, Khoury T. Clinical utility of fecal calprotectin: potential applications beyond inflammatory bowel disease for the primary care physician. Ann Gastroenterol. 2019;32(5):425. https://doi.org/10.20524/aog.2019.0394. Van Rheenen PF, Van de Vijver E, Fidler V. Faecal calprotectin for screening of patients with suspected inflammatory bowel disease: diagnostic meta-analysis. BMJ. 2010. https://doi.org/10.1136/bmj.c3369. Lundgren D, Eklöf V, Palmqvist R, Hultdin J, Karling P. Proton pump inhibitor use is associated with elevated faecal calprotectin levels. A cross-sectional study on subjects referred for colonoscopy. Scand J Gastroenterol. 2019;54(2):152–7. https://doi.org/10.1080/00365521.2019.1566493. Tibble JA, Sigthorsson G, Foster R, Scott D, Fagerhol MK, Roseth A, et al. High prevalence of NSAID enteropathy as shown by a simple faecal test. Gut. 1999;45(3):362. https://doi.org/10.1136/gut.45.3.362. Henderson P, Anderson NH, Wilson DC. The diagnostic accuracy of fecal calprotectin during the investigation of suspected pediatric inflammatory bowel disease: a systematic review and meta-analysis. Am J Gastroenterol. 2014;109(5):637–45. https://doi.org/10.1038/ajg.2013.131. Dai C, Jiang M, Sun M-J, Cao Q. Fecal lactoferrin for assessment of inflammatory bowel disease activity: a systematic review and meta-analysis. J Clin Gastroenterol. 2020;54(6):545–53. https://doi.org/10.1097/mcg.0000000000001212. Shaoul R, Sladek M, Turner D, Paeregaard A, Veres G, Wauters GV, et al. Limitations of fecal calprotectin at diagnosis in untreated pediatric Crohn’s disease. Inflamm Bowel Dis. 2012;18(8):1493–7. https://doi.org/10.1002/ibd.21875. Dai J, Liu W-Z, Zhao Y-P, Hu Y-B, Ge Z-Z. Relationship between fecal lactoferrin and inflammatory bowel disease. Scand J Gastroenterol. 2007;42(12):1440–4. https://doi.org/10.1080/00365520701427094. Garg M, Leach ST, Coffey MJ, Katz T, Strachan R, Pang T, et al. Age-dependent variation of fecal calprotectin in cystic fibrosis and healthy children. J Cyst Fibros. 2017;16(5):631–6. https://doi.org/10.1016/j.jcf.2017.03.010. Oord T, Hornung N. Fecal calprotectin in healthy children. Scand J Clin Lab Invest. 2014;74(3):254–8. https://doi.org/10.3109/00365513.2013.879732. Orfei M, Gasparetto M, Hensel KO, Zellweger F, Heuschkel RB, Zilbauer M. Guidance on the interpretation of faecal calprotectin levels in children. PLoS ONE. 2021;16(2):e0246091. https://doi.org/10.1371/journal.pone.0246091. Gabrielli AP, Manzardo AM, Butler MG. GeneAnalytics pathways and profiling of shared autism and cancer genes. Int J Mol Sci. 2019;20(5):1166. https://doi.org/10.3390/ijms20051166. Forés-Martos J, Catalá-López F, Sánchez-Valle J, Ibáñez K, Tejero H, Palma-Gudiel H, et al. Transcriptomic metaanalyses of autistic brains reveals shared gene expression and biological pathway abnormalities with cancer. Mol Autism. 2019;10(1):17. https://doi.org/10.1186/s13229-019-0262-8. Nisha E. Mathew is funded by the Australian Government Department of Education, Skills and Employment Research Training Program and a Neuroscience Research Australia top up award. Delyse McCaffrey is the Christie Scholar and supported by the NeuRA PhD Pearls Program and funded by the Australian Government Department of Education, Skills and Employment Research Training Program. Adam K. Walker is supported by the Schizophrenia Research Institute and Neuroscience Research Australia (Grant#: GXX0049). Chee Y. Ooi is supported by a National Health and Medical Research Council Investigator Grant (Grant#: APP1194358) funded by the Australian government. NM extracted the data, carried out statistical analysis, and wrote the first draft. DM extracted the data. KM advised on the statistical analysis. AKW, KM, AM, MJM and CYO supervised the work, provided relevant input and critically reviewed the manuscript for important intellectual content. All authors read and approved the final manuscript. Not applicable. The authors declare no competing interests. Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. Search strategy and study-specific adaptation of the Newcastle-Ottowa Scale for case-control studies. Additional analyses. Meta-analysis dataset. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data. Mathew, N.E., McCaffrey, D., Walker, A.K. et al. The search for gastrointestinal inflammation in autism: a systematic review and meta-analysis of non-invasive gastrointestinal markers.
Molecular Autism 15, 4 (2024). https://doi.org/10.1186/s13229-023-00575-0 Received: Accepted: Published: DOI: https://doi.org/10.1186/s13229-023-00575-0Availability of data and materials
References
Funding
Author information
Authors and Affiliations
Contributions
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Competing interests
Additional information
Publisher’s Note
Supplementary Information
Additional file 1.
Additional file 2.
Additional file 3.
Rights and permissions
About this article
Cite this article
Keywords
