
Abstract
Background
Gut dysbiosis contributes to the high risk of bloodstream infection (BSI) among premature infants. Most prior studies of the premature infant gut microbiota were conducted in Western countries and prior to development of current tools for strain-resolved analysis.
Methods
We performed metagenomic sequencing of weekly fecal samples from 75 premature infants at a single hospital in Singapore. We evaluated associations between clinical factors and gut microbiota composition using PERMANOVA and mixed effects linear regression. We used inStrain to perform strain-level analyses evaluating for gut colonization by BSI-causing strains.
Results
Median (interquartile range) gestation was 27 (25, 29) weeks, and 63% of infants were born via Cesarean section. Antibiotic exposures (PERMANOVA; R2 = 0.017, p = 0.001) and postnatal age (R2 = 0.015, p = 0.001) accounted for the largest amount of variability in gut microbiota composition. Increasing postnatal age was associated with higher relative abundances of several common pathogens (Enterococcus faecalis: p < 0.0001; Escherichia coli: p < 0.0001; Klebsiella aerogenes: p < 0.0001; Klebsiella pneumoniae: p < 0.0001). Antibiotic exposures were generally associated with lower relative abundances of both frequently beneficial bacteria (e.g., Bifidobacterium species) and common enteric pathogens (e.g., Enterobacter, Klebsiella species). We identified strains identical to the blood culture isolate in fecal samples from 12 of 16 (75%) infants who developed BSI, including all infections caused by typical enteric bacteria.
Conclusions
Antibiotic exposures were the dominant modifiable factor affecting gut microbiota composition in a large cohort of premature infants from South-East Asia. Strain-resolved analyses indicate that the gut is an important reservoir for organisms causing BSI among premature infants.
Similar content being viewed by others

Background
Sepsis remains a major cause of mortality and morbidity among premature infants. Early-onset sepsis (EOS; onset ≤ 72 h of birth) occurs in 1–2% of very low birth weight (VLBW) infants and is associated with a case-fatality rate of approximately 20% [1,2,3]. Late-onset sepsis (LOS; onset > 72 h after birth) affects up to 24% of VLBW infants and is associated with a 30% increase in mortality, with the risk of death being highly dependent on the causative pathogen [1, 4,5,6]. While EOS cases are believed to originate from direct acquisition of microorganisms during the birthing process, recent studies indicate that a large proportion of LOS cases may occur from translocation of microbes from the gut [7, 8]. Additionally, prior studies reported that LOS episodes among premature infants are often preceded by alterations of the gut microbiota, including losses of microbial diversity and commensal bacteria and high abundances of common enteric pathogens [8,9,10,11,12,13,14,15]. Recent evidence suggests that the altered gut microbiota of premature infants may promote a pro-inflammatory microenvironment that increases gut permeability and microbial translocation [16]. However, most studies of the premature infant gut microbiome were performed in the United States and Europe, with relatively little known regarding factors that impact the gut microbiome and precede LOS among premature infants in Asian settings [17,18,19]. Additionally, bioinformatic tools for measuring genetic heterogeneity between microbial populations have advanced substantially in recent years, providing the opportunity to study microbial strain dynamics within the premature infant gut with unparalleled resolution.
In this study, we analyze metagenomic sequencing data from 581 fecal samples collected from 75 premature infants cared for in a single neonatal intensive care unit (NICU) in Singapore. We identify patient and treatment factors that influence gut microbiome composition among infants cared for in this setting. Additionally, we use strain-resolved metagenomic analyses to describe the dynamics of gut colonization by microbial strains causing bloodstream infections (BSI) in this patient population.
Results
Description of the study population
We collected fecal samples up to twice weekly from birth through 65 days of age from 173 premature infants born at or before 30 weeks gestational age at the KK Women’s and Children’s Hospital (KKH) Neonatal Intensive Care Unit (NICU) between June 2019 and May 2021. The analyses presented herein were limited to 75 infants from whom once weekly fecal samples were selected for shotgun metagenomic sequencing. For the current analyses, we included all neonates who developed a BSI and a random sampling of the remaining infants who had available weekly fecal samples. Most (59%) infants in this study population were female and nearly two-thirds (63%) were born via Cesarean section (Table 1). Median (interquartile range [IQR]) gestational age and birthweight were 27 (25, 29) weeks and 955 (763, 1210) grams, respectively. The overwhelming majority (88%) of infants received one or more antibiotics during the study period, with aminoglycosides (88%) and penicillins (87%) being the most frequently administered antibiotic classes and gentamicin (85%) and benzylpenicillin (80%) being the most frequently prescribed antibiotics (Table 2). All infants received a single-strain probiotic (Bifidobacterium breve M16V) from the time that they started enteral feeding until 36 weeks adjusted gestational age. Four (5%) infants died prior to hospital discharge.
Gut microbiome composition is highly dynamic and shaped by antibiotic exposures
We performed shotgun metagenomic sequencing of weekly fecal samples, with 581 fecal samples [median (IQR) of 8 (7, 9) samples per infant] passing quality control procedures. A total of 9,605,942,085 metagenomic reads were included in gut microbiome analyses, with a median (IQR) sequencing depth of 5.9 (4.4, 34.9) million reads per sample. Median (IQR) Shannon index and number of unique microbial species in these fecal samples were 1.17 (0.79, 1.53) and 48 (32, 72) respectively (Fig. 1a, b). Shannon diversity and the number of unique microbial species in fecal samples increased with increasing postnatal age (linear mixed effects models; Shannon index: β = 0.11, p < 0.0001; number of species: β = 1.18, p < 0.0001). A total of 3,830 species were identified in these samples (Fig. 1c), with the most highly abundant species being B. breve (mean relative abundance of 24%), Klebsiella pneumoniae (22%), Escherichia coli (18%), Enterococcus faecalis (5%), Staphylococcus epidermidis (4%), and Klebsiella aerogenes (2%).

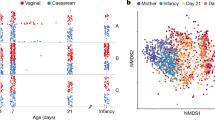
Premature infant gut microbiome alpha diversity and composition by postnatal age. Box and whisker plots of a the Shannon diversity index and b number of observed unique microbial species are shown by week of life. The horizontal lines represent the median value; boundaries of the rectangle correspond to the 25th and 75th percentiles; whiskers extend to values at 1.5 * the interquartile range; points represent outlier values. c Relative abundances of the 20 most highly abundant microbial species and BSI-causing species by postnatal age
We next sought to identify patient and treatment factors that influenced gut microbiome development among the study population. We found that antibiotic exposures (PERMANOVA on Bray–Curtis dissimilarity; R2 = 0.017, p = 0.001) and postnatal age (R2 = 0.015, p = 0.001) accounted for the largest variability in gut microbiota composition (Fig. 2a). Other factors that were associated with gut microbiome composition included race (R2 = 0.014, p = 0.001), enteral feeding type (R2 = 0.013, p = 0.003), probiotic exposure (R2 = 0.009, p = 0.001), gestational age (R2 = 0.007, p = 0.01), and delivery mode (R2 = 0.005, p = 0.02). We next used MaAsLin2 to fit linear mixed effects models evaluating associations between these same factors and the relative abundances of specific species within the gut microbiome [20]. Substantial shifts in the composition of the gut microbiota were seen among infants during the first months of life (Fig. 1c). Specifically, we found that increasing postnatal age was associated with increases in the relative abundances of several common pathogens (E. faecalis: p < 0.0001; E. coli: p < 0.0001; K. pneumoniae: p < 0.0001; K. aerogenes: p < 0.0001) and a decrease in the relative abundance of Staphylococcus epidermidis (p = 0.001; Additional file 1: Table S1). Antibiotic exposures were also associated with substantial shifts in the relative abundances of several microbial species. Penicillins and aminoglycosides were associated with decreases in the relative abundances of Bifidobacterium and Enterobacter species, respectively, while cephalosporins and carbapenems were associated with losses of several Enterobacter and Klebsiella species (Fig. 2b). Interestingly, receipt of carbapenems or metronidazole was associated with increases in the relative abundances of several staphylococcal species, including S. aureus (carbapenems: p = 0.01), S. capitis (carbapenems: p < 0.0001; metronidazole: p = 0.001), and S. epidermidis (carbapenems: p = 0.02). Most antibiotic exposures were associated with a decline in the relative abundance of the probiotic species, B. breve (penicillins: p = 0.001; cephalosporins: p = 0.001; vancomycin: p = 0.02; and metronidazole: p = 0.02), while probiotic exposure was associated with enrichment of the microbiome by this species (p < 0.0001).

Associations between clinical factors and gut microbiome composition. a Bubble plot depicting the amount of variation in gut microbial composition explained by given clinical variables and as measured by PERMANOVA. The size of bubbles represents the amount of variance explained by the variable; asterisks indicate statistical significance (p < 0.05). The first column depicts results from analyses of all samples adjusting for postnatal age; subsequent columns show results from analyses stratified by postnatal age. b Heatmap displaying associations between antibiotic and probiotic exposures and the relative abundances of microbial species within the gut microbiota as estimated by mixed effects linear regression. Only microbial species with a minimum mean relative abundance of 0.01% and a sample prevalence of at least 10% are shown. Boxes are shaded based on the direction and size of the effect as determined from the model beta coefficients; asterisks indicate statistical significance (p < 0.05)
Strain-level community genomic analyses identify BSI isolates within fecal samples
During the study period, 16 (21%) infants developed a BSI caused by the following organisms: Streptococcus agalactiae (n = 5), K. pneumoniae (n = 3), E. coli (n = 2), S. aureus (n = 2), S. epidermidis (n = 2), Proteus mirabilis (n = 1), and Streptococcus anginosus (n = 1). Consistent with prior studies, we detected the BSI species at a high relative abundance in fecal samples collected prior to or following onset of the BSI episode in most infants [11, 14]. We then used inStrain to evaluate for the presence of the BSI strain in fecal samples collected from that infant. Briefly, inStrain is a program that uses metagenomic sequencing data to profile microbial populations and to perform population comparisons that account for within-population genetic heterogeneity [21]. In comparing microbial populations, inStrain calculates a measure referred to as the population average nucleotide identity (popANI), in which nucleotide substitutions are only called if the two samples being compared do not share any alleles [22]. Using inStrain and a threshold for classifying strains as being identical set at a popANI at or above 99.999%, we identified strains identical to the blood culture isolate in 12 of 16 (75%) infants who experienced a BSI (Table 3). Fecal samples containing the BSI strain were identified preceding infection onset, during antibiotic treatment for the infection and, in some infants, for a prolonged period following completion of antibiotics (Fig. 3). Notably, identical strains were identified in the gut metagenomes of all infants who developed BSI caused by typical enteric bacteria (e.g., E. coli, K. pneumoniae, P. mirabilis) and both infants who developed BSI caused by S. epidermidis, a frequent member of the gut microbiota of infants, particularly those who are breastfeeding [23]. In contrast, neither infant with a BSI caused by S. aureus had an identical strain identified in one or more fecal samples. Finally, the BSI strain was identified in fecal samples from 3 of 5 infants who developed BSI caused by S. agalactiae (group B streptococcus), a common colonizer of the infant gut, oral cavity, and other mucosal surfaces [24]. Taken together, these results support the conclusion that the gut is an important source of BSIs caused by classical enteric bacteria and other bacteria previously demonstrated to be prevalent in the infant gut.

Time-series plots of gut microbiota composition among a subset of premature infants who developed BSI. The relative abundance of the BSI causative species is indicated by colored vertical bar for each fecal sample with sequencing data. Black vertical lines denote the timing of BSI episodes. Stars correspond to fecal samples in which the BSI strain was identified in strain-level analyses. Subject identifiers are atop each plot
Strain-level comparisons of group B streptococcal BSI isolates
Despite the study period spanning more than two years, all five BSIs caused by S. agalactiae were identified over a two-month period in 2021. We thus hypothesized that these infections resulted from infant-to-infant transmission or acquisition from a shared environmental source within the NICU environment. To evaluate this hypothesis, we again used inStrain to compare the genomic similarity of these S. agalactiae strains [21]. These analyses demonstrated that the blood culture isolates from infants PL2596 and YH3562 were identical, with 100% popANI and 0 population single nucleotide polymorphisms (SNPs) with more than 99.99% genome coverage overlap (Table 4). The remaining strains were found to be distinct from this shared strain and from each other, with the strain isolated from infant ZR1676 differing from the strain shared by PL2596 and YH3562 but by only 59–60 population SNPs. To further investigate this possible strain transmission between infants PL2596 and YH3562, we obtained additional clinical and epidemiological data from these infants. Infant YH3562 presented with EOS and had S. agalactiae identified in a blood culture obtained on the day of birth, with gut colonization identified through at least 56 days of age. Infant PL2596 was first identified to be colonized by this S. agalactiae strain at 56 days of age and subsequently developed LOS on day of life 65. Notably, these infants resided in the same room within the NICU and had shared clinical providers in the week preceding BSI onset in infant PL2596 and at a time at which infant YH3562 was known to have persistent gut colonization (Fig. 4). However, we did not collect environmental samples from surfaces and equipment within the NICU to confirm the source of transmission. Finally, we compared results from investigation of these S. agalactiae BSIs through use of whole-genome sequencing to findings obtained from multilocus sequence ty** (MLST), which remains a standard approach for evaluation of healthcare-associated infection clusters [25]. MLST analysis (Additional file 1: Table S2) classified these five strains as being from only two sequence types, ST17 and ST24, demonstrating the superior resolution of whole-genome sequencing with current genomic analysis tools relative to conventional genoty** methods.

Putative transmission of a Streptococcus agalactiae strain between infants with an epidemiological link. Times-series plots for two infants who developed BSI from the same strain of S. agalactiae. The green horizontal line indicates the time period during which the infants resided in the same room and had shared healthcare providers. The relative abundance of the shared BSI strain is indicated by a dark blue vertical line for each fecal sample sequenced, while the light blue vertical lines represent the relative abundance of other S. agalactiae strains. Numbers below these lines correspond to the infant age in days. Black vertical lines indicate the day of the BSI episode
Discussion
In this study, we profile the gut microbiomes of a large cohort of premature infants receiving care in a Singaporean NICU. We describe the substantial impact of clinical factors, including antibiotic and probiotic exposures, on development of the premature infant gut microbiota in this setting. We additionally use strain-resolved metagenomic analyses to confirm that most infants who develop BSI harbor strains identical to the BSI culture isolate within their gut microbiota. Finally, we investigate a potential cluster of BSIs caused by S. agalactiae using this same analysis approach and compare these findings to those obtained using conventional genoty** methods.
Due to their medical complexity and high risk of infection, premature infants often receive multiple courses of broad-spectrum antibiotics during the first several months of life. Such antibiotic exposures during early infancy were previously demonstrated to result in prolonged disruptions of the gut microbiota [18, 19]. In particular, ampicillin, cefepime, meropenem, and vancomycin are known to substantially reduce gut microbial diversity and delay maturation of the gut microbiota [18]. In the current study, we evaluated the effects of individual antibiotics on the relative abundances of specific microbial species within the premature infant gut. We found that cephalosporin and carbapenem exposures were associated with losses of Enterobacteriaceae, and carbapenem exposure was associated with higher relative abundance of S. epidermidis. These findings are congruent with analyses conducted by Gibson et al. in which cefotaxime and meropenem were associated with similar changes in the abundances of Enterobacteriaceae and S. epidermidis within the gut microbiomes of premature infants immediately following antibiotic exposure [19]. In contrast, Fouhy et al. observed higher relative abundances of Enterobacteriaceae among full-term infants treated with ampicillin and gentamicin [26]. The inconsistent associations between antibiotic exposures and losses or gains of individual taxa in the gut microbiota were noted in a recent systematic review [27]. These discrepancies are likely due to nuances in the individual antibiotic spectra of activity and further highlight the importance of evaluating the effects of individual antibiotics on the gut microbiome. Our findings and those of related studies help inform antimicrobial stewardship efforts and the judicious use of antibiotics in premature infants.
Probiotics are frequently administered to premature infants because of data suggesting that these products may reduce the risk of necrotizing enterocolitis and LOS [28,29,30,31]. The strain used in our cohort, B. breve M-16 V, is among the most commonly used probiotics in infants [25]. While genome sequencing enables analysis of entire genomes, MLST typically involves sequencing of seven housekee** genes that represent less than 1% of bacterial genomes [53]. The result is that whole-genome sequencing has far higher resolution for strain comparisons than MLST and other conventional genoty** methods, as has been demonstrated by several prior studies [54,55,56]. For instance, whole-genome sequencing recently demonstrated that K. pneumoniae sequence type 258, a frequent cause of healthcare-associated carbapenem-resistant Enterobacteriaceae infection, represents two distinct clades, disproving the hypothesis that the widespread infections attributed to this organism are caused by a single bacterial clone [56]. Although limited to investigation of a single infection cluster, our analysis similarly demonstrated the superiority of whole-genome sequencing for the differentiation of S. agalactiae strains. In a healthcare system increasingly strained for resources, use of whole-genome sequencing has the potential to inform infection control policies and improve allocation of the limited resources available for investigation of and response to infection clusters.
Our study has several limitations. Although we performed metagenomic sequencing on weekly samples collected from 75 premature infants, analyses may have been limited by the frequency and depth of sequencing of fecal samples. For instance, we may have underestimated the rapidity at which the gut microbiota changes during the first months of life, and higher sequencing depth may have enabled detection of additional BSI strains present within the gut microbiota at low abundance. Analyses evaluating for gut colonization among infants who experienced a BSI were limited by the relatively small number of infections that occurred in this cohort. Similarly, our comparison of whole-genome sequencing to MLST was limited to a single infection cluster. Finally, while we used a recently developed tool that represents a significant advance for comparison of microbial populations, our analyses did not quantify the relative abundances of specific strains within these populations.
Conclusions
To conclude, this study conducted in a Singaporean NICU provides data on the premature infant gut microbiota in an understudied geographical area and demonstrates the roles of antibiotics and probiotics in sha** gut microbiome maturation among premature infants in this setting. Additionally, we provide conclusive genomic data that support the gut as a reservoir for BSI among premature infants. Finally, this study adds to a growing body of literature demonstrating the potential utility of whole-genome sequencing for hospital infection prevention and control. These data provide a basis for future studies evaluating the utility of metagenomic sequencing for the identification of premature infants at high risk of BSI.
Methods
Study design and setting
This was a prospective cohort study of infants born at or before 30 weeks gestational age and admitted to the KKH NICU between June 2019 and May 2021. KKH is an 830-bed specialized maternal and pediatric hospital in Singapore that houses a 40-bed level 4 NICU. Infants were enrolled within 72 h of birth and followed through 65 days of age, hospital discharge, or death. First-line empiric antibiotics for EOS and LOS in the KKH NICU are penicillin plus gentamicin and cloxacillin plus amikacin, respectively. All infants routinely receive B. breve strain M-16 V (Morinaga Milk Industry Co., Tokyo, Japan) from the time they start enteral feeds through 36 weeks adjusted gestational age. Legal guardians provided written informed consent for infants to participate in the study. The study protocol was approved by the Singhealth Institutional Review Board (CIRB Ref. No. 2017/2117).
Study procedures
Demographic and clinical data were collected from the KKH VLBW registry and infant medical records. BSI was defined as a clinical episode with one or more positive blood cultures in the presence of signs or symptoms of infection. Blood cultures with coagulase-negative staphylococci, Bacillus, Corynebacterium, Micrococcus, and Propionibacterium species were considered contaminants unless two or more cultures grew the organism or the infant showed signs of sepsis and received intravenous antibiotics for at least five days. Fecal samples were collected into eNAT® (Copan Italia, Brescia, Italy), a guanidine thiocyanate-based medium that inactivates microorganisms and stabilizes microbial DNA [57]. Culture isolates from BSIs occurring among enrolled infants were obtained from the hospital microbiology laboratory and stored using Microbank™ cryopreservation vials (Pro-Lab Diagnostics, Richmond Hill, Ontario, Canada). Fecal samples and blood culture isolates were stored at −80 °C prior to being shipped on dry ice to Duke University. The Duke Microbiome Core extracted DNA from fecal samples and blood culture isolates using PowerSoil Pro Kits (Qiagen, Germantown, MD). The Duke Sequencing and Genomic Technologies Shared Resource then constructed libraries using Illumina DNA Library Prep Kits (Illumina, San Diego, CA) and sequenced these libraries on a NovaSeq6000 instrument (Illumina) as 150-bp paired-end reads. Samples were sequenced in two batches with inclusion of negative extraction and library preparation controls and the ZymoBIOMICS Gut Microbiome Standard (Zymo Research Corp, Irvine, CA) as a positive extraction control. One negative extraction control contained no quality-filtered reads, while the remaining negative controls contained 4–177 microbial reads, with the most abundant genera being Micrococcus and Streptococcus.
Bioinformatic processing of sequencing reads from fecal samples and blood culture isolates
Raw sequencing reads from fecal samples and blood culture isolates were quality-filtered and removed of host contamination (hg19 human reference genome) using KneadData v0.10.0. Kraken2 v2.1.2 was used for taxonomic classification and was run in paired-end mode with default parameters against a database of all complete bacterial, fungal, archaeal, and viral genomes in the NCBI Reference Sequence Database as of February 2023 [58,59,60]. The abundances of species were estimated using Bracken v2.6.2 with database construction performed using a read length of 150 bp and the default k-mer length of 35 bp. [61] Quality-filtered sequencing reads from blood culture isolates were assembled using SPAdes v3.15.3 [62]. Contigs shorter than 1000 bp were removed from these genome assemblies using BBMap v38.93 [63]. All genomes were determined to have ≥ 99% completeness and < 1% contamination as determined by checkM v1.1.3, with a median (IQR) genome coverage of 774 (356–1128) as calculated by BBMap (Additional file 1: Table S3) [64]. We pruned fecal samples with fewer than 10,000 quality-filtered sequencing reads.
Statistical analyses
We estimated alpha diversity using the phyloseq R package v1.42.0 and used mixed effects regression to evaluate associations between week of life and the Shannon diversity index (linear regression) and number of observed microbial species (negative binomial regression) in fecal samples [65]. Using the adonis2 function of the vegan package v2.6–4, we performed PERMANOVA on Bray–Curtis distances to evaluate associations between clinical factors and overall gut microbiome composition [66]. Analyses considered postnatal age, gestational age at birth, birthweight, patient race, sex, delivery mode, diet (breast milk, formula, or both), postnatal antibiotic exposures, and probiotic exposure with participant as a blocking factor to account for repeated sampling. Additional PERMANOVAs were performed on these clinical factors stratified by postnatal age. We then used the Maaslin2 package v1.12.0 to fit a linear mixed effects model evaluating associations between clinical factors, including specific antibiotic exposures, and the relative abundances of specific microbial species [20]. This model included postnatal age, gestational age at birth, birthweight, delivery mode, patient race, sex, percent of enteral feeds (expressed breast milk, pasteurized donor human milk, and formula), postnatal antibiotic exposures, and probiotic exposure. We included subject as a random effect and limited analyses to species that had a minimum mean relative abundance of 0.01% and a sample prevalence of at least 10%. Infants were considered exposed to an antibiotic or the probiotic if they received at least one dose since collection of the last sequenced fecal sample. If a subject started antibiotics or the probiotic on the day of fecal sample collection, the exposure was assigned to the next sequenced sample. Antibiotic exposures included antibiotics that were administered to at least 5% of the study population: aminoglycosides, carbapenems, cephalosporins, metronidazole, penicillins, and vancomycin.
Comparison of bacterial strains in blood culture isolates and fecal samples
We used inStrain v1.6.4 to perform genomic comparisons of bacterial strains in fecal samples and blood culture isolates [22]. To evaluate for the presence of the BSI strain in fecal samples from the same infant, we first mapped fecal and blood culture metagenomic sequencing reads against the assembled blood culture isolate genome using BWA v0.7.17 [67]. Pairs of samples with at least 50% coverage breadth at a depth of five or more reads were compared to identify SNPs and to calculate popANI values. To compare the genomic similarity of blood culture isolates from different infants, we de-replicated genomes using dRep v3.4.1 with the primary clustering threshold set to an average nucleotide identity of 95% [68]. We then mapped metagenomic sequencing reads from blood culture isolates against this de-replicated set of genomes using BWA and used inStrain to identify SNPs and calculate popANI values for each pairwise comparison [21, 67]. For all analyses, we set the threshold for classifying strains as being identical at a popANI of 99.999%, which was previously proposed as a highly stringent threshold for strain sameness within the limit of detection for metagenomic analyses [22].
Genotypic analyses using multilocus sequence ty**
DNA from S. agalactiae blood culture isolates was extracted using the ZymoBIOMICS DNA Mini Prep kit (Zymo Research Corp). Extracted DNA for each BSI isolate was then used as template DNA in PCR assays targeting housekee** genes (adhP, pheS, atr, glnA, sdhA, glcK, tkt), as described previously [69]. PCR products underwent Sanger sequencing and the resulting chromatograms were submitted to the public databases for molecular ty** and microbial genome diversity (PubMLST) for allele determination and identification of strain sequence type [70].
Data availability
The metagenomic data analyzed in this study are available on the NCBI Sequence Read Archive (BioProject PRJNA947616). The de-identified metadata and script used for data analyses are available upon request.
References
Hornik CP, Fort P, Clark RH, et al. Early and late onset sepsis in very-low-birth-weight infants from a large group of neonatal intensive care units. Early Hum Dev. 2012;88(Suppl 2):S69-74. https://doi.org/10.1016/S0378-3782(12)70019-1.
Gan MY, Lee WL, Yap BJ, et al. Contemporary trends in global mortality of sepsis among young infants less than 90 days: a systematic review and meta-analysis. Front Pediatr. 2022;10: 890767. https://doi.org/10.3389/fped.2022.890767.
Klinger G, Levy I, Sirota L, et al. Epidemiology and risk factors for early onset sepsis among very-low-birthweight infants. Am J Obstet Gynecol. 2009;201(1):38 e1-46. https://doi.org/10.1016/j.ajog.2009.03.006.
Stoll BJ, Hansen N, Fanaroff AA, et al. Late-onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics. 2002;110(2 Pt 1):285–91. https://doi.org/10.1542/peds.110.2.285.
Goh GL, Lim CSE, Sultana R, De La Puerta R, Rajadurai VS, Yeo KT. Risk factors for mortality from late-onset sepsis among preterm very-low-birthweight infants: a single-center cohort study from Singapore. Front Pediatr. 2021;9: 801955. https://doi.org/10.3389/fped.2021.801955.
Boghossian NS, Page GP, Bell EF, et al. Late-onset sepsis in very low birth weight infants from singleton and multiple-gestation births. J Pediatr. 2013;162(6):1120–4, 1124 e1. https://doi.org/10.1016/j.jpeds.2012.11.089.
Carl MA, Ndao IM, Springman AC, et al. Sepsis from the gut: the enteric habitat of bacteria that cause late-onset neonatal bloodstream infections. Clin Infect Dis. 2014;58(9):1211–8. https://doi.org/10.1093/cid/ciu084.
Smith A, Saiman L, Zhou J, Della-Latta P, Jia H, Graham PL 3rd. Concordance of gastrointestinal tract colonization and subsequent bloodstream infections with gram-negative bacilli in very low birth weight infants in the neonatal intensive care unit. Pediatr Infect Dis J. 2010;29(9):831–5. https://doi.org/10.1097/INF.0b013e3181e7884f.
Graspeuntner S, Waschina S, Kunzel S, et al. Gut dysbiosis with bacilli dominance and accumulation of fermentation products precedes late-onset sepsis in preterm infants. Clin Infect Dis. 2019;69(2):268–77. https://doi.org/10.1093/cid/ciy882.
Mai V, Torrazza RM, Ukhanova M, et al. Distortions in development of intestinal microbiota associated with late onset sepsis in preterm infants. PLoS ONE. 2013;8(1): e52876. https://doi.org/10.1371/journal.pone.0052876.
Stewart CJ, Embleton ND, Marrs ECL, et al. Longitudinal development of the gut microbiome and metabolome in preterm neonates with late onset sepsis and healthy controls. Microbiome. 2017;5(1):75. https://doi.org/10.1186/s40168-017-0295-1.
Mukhopadhyay S, Lee JJ, Hartman E, et al. Preterm infants at low risk for early-onset sepsis differ in early fecal microbiome assembly. Gut Microbes. 2022;14(1):2154091. https://doi.org/10.1080/19490976.2022.2154091.
Graham PL 3rd, Della-Latta P, Wu F, Zhou J, Saiman L. The gastrointestinal tract serves as the reservoir for Gram-negative pathogens in very low birth weight infants. Pediatr Infect Dis J. 2007;26(12):1153–6. https://doi.org/10.1097/INF.0b013e31814619d4.
El Manouni El Hassani S, Niemarkt HJ, Berkhout DJC, et al. Profound pathogen-specific alterations in intestinal microbiota composition precede late-onset sepsis in preterm infants: a longitudinal, multicenter, case-control study. Clin Infect Dis. 2021;73(1):e224–32. https://doi.org/10.1093/cid/ciaa1635.
Madan JC, Salari RC, Saxena D, et al. Gut microbial colonisation in premature neonates predicts neonatal sepsis. Arch Dis Child Fetal Neonatal Ed. 2012;97(6):F456–62. https://doi.org/10.1136/fetalneonatal-2011-301373.
Selma-Royo M, Calatayud Arroyo M, Garcia-Mantrana I, et al. Perinatal environment shapes microbiota colonization and infant growth: impact on host response and intestinal function. Microbiome. 2020;8(1):167. https://doi.org/10.1186/s40168-020-00940-8.
Avershina E, Storro O, Oien T, et al. Bifidobacterial succession and correlation networks in a large unselected cohort of mothers and their children. Appl Environ Microbiol. 2013;79(2):497–507. https://doi.org/10.1128/AEM.02359-12.
Gasparrini AJ, Wang B, Sun X, et al. Persistent metagenomic signatures of early-life hospitalization and antibiotic treatment in the infant gut microbiota and resistome. Nat Microbiol. 2019;4(12):2285–97. https://doi.org/10.1038/s41564-019-0550-2.
Gibson MK, Wang B, Ahmadi S, et al. Developmental dynamics of the preterm infant gut microbiota and antibiotic resistome. Nat Microbiol. 2016;1:16024. https://doi.org/10.1038/nmicrobiol.2016.24.
Mallick H, Rahnavard A, McIver LJ, et al. Multivariable association discovery in population-scale meta-omics studies. PLoS Comput Biol. 2021;17(11): e1009442. https://doi.org/10.1371/journal.pcbi.1009442.
Olm MR, Crits-Christoph A, Bouma-Gregson K, Firek BA, Morowitz MJ, Banfield JF. inStrain profiles population microdiversity from metagenomic data and sensitively detects shared microbial strains. Nat Biotechnol. 2021;39(6):727–36. https://doi.org/10.1038/s41587-020-00797-0.
Lou YC, Olm MR, Diamond S, et al. Infant gut strain persistence is associated with maternal origin, phylogeny, and traits including surface adhesion and iron acquisition. Cell Rep Med. 2021;2(9): 100393. https://doi.org/10.1016/j.xcrm.2021.100393.
Jimenez E, Delgado S, Maldonado A, et al. Staphylococcus epidermidis: a differential trait of the fecal microbiota of breast-fed infants. BMC Microbiol. 2008;8:143. https://doi.org/10.1186/1471-2180-8-143.
Tazi A, Plainvert C, Anselem O, et al. Risk factors for infant colonization by hypervirulent CC17 Group B Streptococcus: toward the understanding of late-onset disease. Clin Infect Dis. 2019;69(10):1740–8. https://doi.org/10.1093/cid/ciz033.
Jeffreys AJ, Royle NJ, Patel I, et al. Principles and recent advances in human DNA fingerprinting. EXS. 1991;58:1–19. https://doi.org/10.1007/978-3-0348-7312-3_1.
Fouhy F, Guinane CM, Hussey S, et al. High-throughput sequencing reveals the incomplete, short-term recovery of infant gut microbiota following parenteral antibiotic treatment with ampicillin and gentamicin. Antimicrob Agents Chemother. 2012;56(11):5811–20. https://doi.org/10.1128/AAC.00789-12.
McDonnell L, Gilkes A, Ashworth M, et al. Association between antibiotics and gut microbiome dysbiosis in children: systematic review and meta-analysis. Gut Microbes Jan-Dec. 2021;13(1):1–18. https://doi.org/10.1080/19490976.2020.1870402.
Costeloe K, Bowler U, Brocklehurst P, et al. A randomised controlled trial of the probiotic Bifidobacterium breve BBG-001 in preterm babies to prevent sepsis, necrotising enterocolitis and death: the Probiotics in Preterm infantS (PiPS) trial. Health Technol Assess. 2016;20(66):1–194. https://doi.org/10.3310/hta20660.
Sowden M, van Weissenbruch MM, Bulabula ANH, van Wyk L, Twisk J, van Niekerk E. Effect of a multi-strain probiotic on the incidence and severity of necrotizing enterocolitis and feeding intolerances in preterm neonates. Nutrients. 2022. https://doi.org/10.3390/nu14163305.
Jacobs SE, Tobin JM, Opie GF, et al. Probiotic effects on late-onset sepsis in very preterm infants: a randomized controlled trial. Pediatrics. 2013;132(6):1055–62. https://doi.org/10.1542/peds.2013-1339.
Rao SC, Athalye-Jape GK, Deshpande GC, Simmer KN, Patole SK. Probiotic supplementation and late-onset sepsis in preterm infants: a meta-analysis. Pediatrics. 2016;137(3): e20153684. https://doi.org/10.1542/peds.2015-3684.
Wong CB, Iwabuchi N, **ao JZ. Exploring the science behind Bifidobacterium breve M-16V in infant health. Nutrients. 2019. https://doi.org/10.3390/nu11081724.
Patole S, Keil AD, Chang A, et al. Effect of Bifidobacterium breve M-16V supplementation on fecal bifidobacteria in preterm neonates–a randomised double blind placebo controlled trial. PLoS ONE. 2014;9(3): e89511. https://doi.org/10.1371/journal.pone.0089511.
Chua MC, Ben-Amor K, Lay C, et al. Effect of synbiotic on the gut microbiota of cesarean delivered infants: a randomized, double-blind, multicenter study. J Pediatr Gastroenterol Nutr. 2017;65(1):102–6. https://doi.org/10.1097/MPG.0000000000001623.
Backhed F, Roswall J, Peng Y, et al. Dynamics and stabilization of the human gut microbiome during the first year of life. Cell Host Microbe. 2015;17(5):690–703. https://doi.org/10.1016/j.chom.2015.04.004.
Dogra S, Sakwinska O, Soh SE, et al. Dynamics of infant gut microbiota are influenced by delivery mode and gestational duration and are associated with subsequent adiposity. MBio. 2015. https://doi.org/10.1128/mBio.02419-14.
Morgan RL, Preidis GA, Kashyap PC, et al. Probiotics reduce mortality and morbidity in preterm, low-birth-weight infants: a systematic review and network meta-analysis of randomized trials. Gastroenterology. 2020;159(2):467–80. https://doi.org/10.1053/j.gastro.2020.05.096.
Samanta M, Sarkar M, Ghosh P, Ghosh J, Sinha M, Chatterjee S. Prophylactic probiotics for prevention of necrotizing enterocolitis in very low birth weight newborns. J Trop Pediatr. 2009;55(2):128–31. https://doi.org/10.1093/tropej/fmn091.
Oncel MY, Sari FN, Arayici S, et al. Lactobacillus Reuteri for the prevention of necrotising enterocolitis in very low birthweight infants: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2014;99(2):F110–5. https://doi.org/10.1136/archdischild-2013-304745.
Wandro S, Osborne S, Enriquez C, Bixby C, Arrieta A, Whiteson K. The microbiome and metabolome of preterm infant stool are personalized and not driven by health outcomes, including necrotizing enterocolitis and late-onset sepsis. mSphere. 2018. https://doi.org/10.1128/mSphere.00104-18.
Schwartz DJ, Shalon N, Wardenburg K, et al. Gut pathogen colonization precedes bloodstream infection in the neonatal intensive care unit. Sci Transl Med. 2023;15(694): eadg5562. https://doi.org/10.1126/scitranslmed.adg5562.
Amandito R, Malik A, Rohsiswatmo R. Metagenomic profiles of the early life microbiome of Indonesian inpatient neonates and their influence on clinical characteristics. Sci Rep. 2022;12(1):9413. https://doi.org/10.1038/s41598-022-13496-4.
Chang JY, Shin SM, Chun J, Lee JH, Seo JK. Pyrosequencing-based molecular monitoring of the intestinal bacterial colonization in preterm infants. J Pediatr Gastroenterol Nutr. 2011;53(5):512–9. https://doi.org/10.1097/MPG.0b013e318227e518.
Imoto N, Kano C, Aoyagi Y, et al. Administration of beta-lactam antibiotics and delivery method correlate with intestinal abundances of Bifidobacteria and Bacteroides in early infancy, in Japan. Sci Rep. 2021;11(1):6231. https://doi.org/10.1038/s41598-021-85670-z.
Itani T, Ayoub Moubareck C, Melki I, et al. Establishment and development of the intestinal microbiota of preterm infants in a Lebanese tertiary hospital. Anaerobe. 2017;43:4–14. https://doi.org/10.1016/j.anaerobe.2016.11.001.
Beller L, Deboutte W, Falony G, et al. Successional stages in infant gut microbiota maturation. MBio. 2021;12(6): e0185721. https://doi.org/10.1128/mBio.01857-21.
Lee SA, Lim JY, Kim BS, et al. Comparison of the gut microbiota profile in breast-fed and formula-fed Korean infants using pyrosequencing. Nutr Res Pract. 2015;9(3):242–8. https://doi.org/10.4162/nrp.2015.9.3.242.
Lundgren SN, Madan JC, Emond JA, et al. Maternal diet during pregnancy is related with the infant stool microbiome in a delivery mode-dependent manner. Microbiome. 2018;6(1):109. https://doi.org/10.1186/s40168-018-0490-8.
Quin C, Gibson DL. Human behavior, not race or geography, is the strongest predictor of microbial succession in the gut bacteriome of infants. Gut Microbes. 2020;11(5):1143–71. https://doi.org/10.1080/19490976.2020.1736973.
Kelly MS, Ward DV, Severyn CJ, et al. Gut colonization preceding mucosal barrier injury bloodstream infection in pediatric hematopoietic stem cell transplantation recipients. Biol Blood Marrow Transplant. 2019;25(11):2274–80. https://doi.org/10.1016/j.bbmt.2019.07.019.
Severyn CJ, Siranosian BA, Kong ST, et al. Microbiota dynamics in a randomized trial of gut decontamination during allogeneic hematopoietic cell transplantation. JCI Insight. 2022. https://doi.org/10.1172/jci.insight.154344.
Thanert R, Thanert A, Ou J, et al. Antibiotic-driven intestinal dysbiosis in pediatric short bowel syndrome is associated with persistently altered microbiome functions and gut-derived bloodstream infections. Gut Microbes. 2021;13(1):1940792. https://doi.org/10.1080/19490976.2021.1940792.
Tsang AKL, Lee HH, Yiu SM, Lau SKP, Woo PCY. Failure of phylogeny inferred from multilocus sequence ty** to represent bacterial phylogeny. Sci Rep. 2017;7(1):4536. https://doi.org/10.1038/s41598-017-04707-4.
Azarian T, Cook RL, Johnson JA, et al. Whole-genome sequencing for outbreak investigations of methicillin-resistant Staphylococcus aureus in the neonatal intensive care unit: time for routine practice? Infect Control Hosp Epidemiol. 2015;36(7):777–85. https://doi.org/10.1017/ice.2015.73.
Roetzer A, Diel R, Kohl TA, et al. Whole genome sequencing versus traditional genoty** for investigation of a Mycobacterium tuberculosis outbreak: a longitudinal molecular epidemiological study. PLoS Med. 2013;10(2): e1001387. https://doi.org/10.1371/journal.pmed.1001387.
Deleo FR, Chen L, Porcella SF, et al. Molecular dissection of the evolution of carbapenem-resistant multilocus sequence type 258 Klebsiella pneumoniae. Proc Natl Acad Sci U S A. 2014;111(13):4988–93. https://doi.org/10.1073/pnas.1321364111.
Young RR, Jenkins K, Araujo-Perez F, Seed PC, Kelly MS. Long-term stability of microbiome diversity and composition in fecal samples stored in eNAT medium. Microbiologyopen. 2020;9(7): e1046. https://doi.org/10.1002/mbo3.1046.
O’Leary NA, Wright MW, Brister JR, et al. Reference sequence (RefSeq) database at NCBI: current status, taxonomic expansion, and functional annotation. Nucleic Acids Res. 2016;44(D1):D733–45. https://doi.org/10.1093/nar/gkv1189.
Kneaddata. https://github.com/biobakery/kneaddata.
Wood DE, Lu J, Langmead B. Improved metagenomic analysis with Kraken 2. Genome Biol. 2019;20(1):257. https://doi.org/10.1186/s13059-019-1891-0.
Lu J, Breitwieser FP, Thielen P, Salzberg SL. Bracken: estimating species abundance in metagenomics data. Peerj Comput Sci. 2017;3: e104. https://doi.org/10.7717/peerj-cs.104.
Bankevich A, Nurk S, Antipov D, et al. SPAdes: a new genome assembly algorithm and its applications to single-cell sequencing. J Comput Biol. 2012;19(5):455–77. https://doi.org/10.1089/cmb.2012.0021.
BBMap short-read aligner, and other bioinformatics tools. 2016.
Parks DH, Imelfort M, Skennerton CT, Hugenholtz P, Tyson GW. CheckM: assessing the quality of microbial genomes recovered from isolates, single cells, and metagenomes. Genome Res. 2015;25(7):1043–55. https://doi.org/10.1101/gr.186072.114.
McMurdie PJ, Holmes S. phyloseq: an R package for reproducible interactive analysis and graphics of microbiome census data. PLoS ONE. 2013;8(4): e61217. https://doi.org/10.1371/journal.pone.0061217.
vegan: Community Ecology Package. 2022. https://cran.r-project.org/package=vegan.
Li H, Durbin R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics. 2009;25(14):1754–60. https://doi.org/10.1093/bioinformatics/btp324.
Olm MR, Brown CT, Brooks B, Banfield JF. dRep: a tool for fast and accurate genomic comparisons that enables improved genome recovery from metagenomes through de-replication. ISME J. 2017;11(12):2864–8. https://doi.org/10.1038/ismej.2017.126.
Jones N, Bohnsack JF, Takahashi S, et al. Multilocus sequence ty** system for group B streptococcus. J Clin Microbiol. 2003;41(6):2530–6. https://doi.org/10.1128/JCM.41.6.2530-2536.2003.
Jolley KA, Bray JE, Maiden MCJ. Open-access bacterial population genomics: BIGSdb software, the PubMLST.org website and their applications. Wellcome Open Res. 2018;3:124. https://doi.org/10.12688/wellcomeopenres.14826.1.
Acknowledgements
We would like to thank Ms. Irene Tan Guat Kuan and Dr. Matthias Maiwald from the Department of Pathology and Laboratory Medicine at KK Women’s & Children’s Hospital for facilitating the collection of BSI samples; the Duke University School of Medicine for use of the Microbiome Core, which performed the DNA extractions for this research; the Sequencing and Genomic Technologies Shared Resource, which performed library preparation and metagenomic sequencing of study samples; and Bobby Warren and the Disinfection, Resistance, and Transmission Epidemiology (DiRTE) laboratory, which provided multilocus sequence ty**. We especially thank all of the infants and families who participated in this study.
Funding
This study was supported by the Singhealth Duke-NUS Paediatric Academic Clinical Programme General Fund (02/FY2018/EX/18-A59). KTY received support from the Nurturing Clinician Scientist Scheme, Singhealth Duke-NUS Academic Clinical Programme (02/FY016/P2/17-A44). MSK was supported by a National Institutes of Health Career Development Award (K23-AI135090). SMH was supported by NICHD of the National Institutes of Health under award number K12HD105253. The authors would like to thank the Derfner Foundation for their generous contributions to the Department of Pediatrics at Duke University which have also supported this research.
Author information
Authors and Affiliations
Contributions
MSK and KTY were responsible for study conception and design; CSEL, CO, and MCC collected clinical data and participant samples; SMH and MSK performed analyses; SMH, MSK, KTY interpreted results. All authors reviewed and contributed to the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Legal guardians provided written informed consent for infants to participate in the study. The study protocol was approved by the Singhealth Institutional Review Board (CIRB Ref. No. 2017/2117).
Competing interests
The authors declare the following potential conflicts of interest, though neither of them is deemed relevant to the current work: MSK is a consultant for Merck & Co, Inc. and Invivyd.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: Table S1. Significant associations of clinical factors and antibiotic exposures and the relative abundances of microbial species within the gut microbiome. Table S2. Multilocus sequence ty** of Streptococcus agalactiae BSI isolates. Table S3. Statistics for genomes generated from BSI isolates.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Heston, S.M., Lim, C.S.E., Ong, C. et al. Strain-resolved metagenomic analysis of the gut as a reservoir for bloodstream infection pathogens among premature infants in Singapore. Gut Pathog 15, 55 (2023). https://doi.org/10.1186/s13099-023-00583-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13099-023-00583-8