
Abstract
Interactions between multiple genes and environmental factors could be related to the pathogenesis of type 1 diabetes (T1D). The Brazilian population results from different historical miscegenation events, resulting in a highly diverse genetic pool. This study aimed to analyze the mtDNA of patients with T1D and to investigate whether there is a relationship between maternal ancestry, self-reported color and the presence of T1D. The mtDNA control region of 204 patients with T1D residing in three geographic regions of Brazil was sequenced following the International Society for Forensic Genetics (ISFG) recommendations. We obtained a frequency of Native American matrilineal origin (43.6%), African origin (38.2%), and European origin (18.1%). For self-declared color, 42.6% of the patients with diabetes reported that they were White, 50.9% were Brown, and 5.4% were Black. Finally, when we compared the self-declaration data with maternal ancestral origin, we found that for the self-declared White group, there was a greater percentage of haplogroups of Native American origin (50.6%); for the self-declared Black group, there was a greater percentage of African haplogroups (90.9%); and for the Brown group, there was a similar percentage of Native American and African haplogroups (42.3% and 45.2%, respectively). The Brazilian population with diabetic has a maternal heritage of more than 80% Native American and African origin, corroborating the country’s colonization history.
Similar content being viewed by others

Introduction
Type 1 diabetes mellitus (T1D) is an inherited polygenic chronic autoimmune disease caused by immune destruction of pancreatic beta cells, resulting in insulin deficiency [1,2,3]. Most genes associated with T1D susceptibility are related to the immune response [4]. Genetic variation in the region known as the human leukocyte antigen complex (HLA), especially in class II HLA antigens, is associated with genetic risk in T1D patients [4,5,6]. Generally, the risk conferred by HLA system genes that is more prevalent in White, Caucasian, and European-American individuals [2, 3, 5].
Another molecular marker that could be included in ancestry studies in patients with T1D is mitochondrial DNA (mtDNA). Mitochondria are membranous organelles, formed by a double membrane, present in almost all eukaryotic cells [7,8,9]. They are fundamental for a variety of biological functions, being responsible for regulating a wide range of cellular processes such as ATP production through oxidative phosphorylation (OXPHOS), apoptosis, β-oxidation of fatty acids, calcium homeostasis regulation, production of reactive oxygen species (ROS), and iron-sulfur cluster biogenesis [7,8,9].
Mitochondria have their own DNA, mtDNA, which in mammals is present in thousands of copies per cell and is inherited in a non-Mendelian maternal manner. mtDNA is a circular double-stranded DNA molecule, consisting of a heavy strand (H) and a light strand (L), without histones and organized into nucleoprotein complexes called nucleoids. It has a size of 16.5 kb, containing 37 genes responsible for encoding 13 protein subunits of the OXPHOS system, as well as two rRNAs and a set of 22 tRNAs for mitochondrial translation [7, 8]. In addition to the coding region, mtDNA contains a non-coding control region, a short displacement loop, a hypervariable segment (HVS) known as the D-loop, which houses almost all mtDNA replication and transcription [9, 10].
Thus, mtDNA has many effects, including adaptive mechanisms to deal with environmental changes and mechanisms related to cellular physiology, growth characteristics and inflammatory systems. All the abovementioned actions have a great impact on a broad range of metabolic and degenerative diseases, such as cancer, diabetes, and aging, which are related to polymorphisms and mutations in these genes [11,12,13,14].
According to Cardena, mtDNA through hypervariable regions (HVS) could be a good marker for inferring probable maternal geographic origin [15]. Brazil has important genetic diversity due to its colonization of different migratory flows and miscegenation between Native American, European, and African individuals [16, 17]. Therefore, to date, no evaluation of mtDNA in patients with T1D has been carried out in Brazil. Thus, this pilot study aimed to analyze the maternal genetic origin of patients with T1D in a highly admixed population.
Materials and methods
This study, with 204 anonymized and not related to each other individuals with T1D, was derived from a nationwide multicenter cross-sectional study with 1760 patients conducted in five geographical regions (North, Northeast, Midwest, Southeast and South), as previously described [1]. The present sample (n = 204) comprised 86 men [42.2%]; 118 women [57.8%]) who had a mean age of 27.7 (SD ± 11.28) years at diagnosis of 13.2 years (SD ± 8.29) and a mean duration of diabetes of 13.5 years (SD ± 8.43). The distribution of the studied population according to the geographic regions of Brazil is described in Fig. 1.

Map of Brazil's geopolitical regions with a number of samples by region: Northeast Region (102) and North Region (7), together totaling 109 samples, Southeast Region: 82 samples; South Region: 13 samples. The samples from the North Region were added to the samples from the Northeast Region, due to their low sample number
The control region of mtDNA, between positions 16024 to 576, was amplified and sequenced. Conventional PCR was used for amplification using the L15900 and H639 primers at a concentration of 0.2 µM each. The control region was sequenced using the L15900, L16555, L314, H159 and H639 primers at a concentration of 0.25 µM each. Electrophoresis was performed on an ABI PRISM® 3500 automatic sequencer (Applied Biosystems, CA, USA). All forward and reverse sequences were aligned with the revised Cambridge Reference Sequence (rCRS) using the SeqScape Version 2.7 program (Applied Biosystems, CA, USA) following the updated nomenclature guidelines for mtDNA. The EMPOP program was used to assign sequences to haplotypes according to the most up-to-date version of the phylogenetic tree of the mtDNA, Phylotree.
Approval was obtained before the start of the study by the Research Ethics Committee of the HUPE-UERJ (Pedro Ernesto University Hospital, State University of Rio de Janeiro) with the number CAAE 53563115.2.1001.5259. All procedures performed were in accordance with the ethical standards of the Helsinki Declaration of 1964 and later versions. Informed consent was obtained from all patients prior to recruitment.
Results and discussion
The percentages of mtDNA haplogroups observed in patients with T1D in Brazil were Amerindian 43.6% (89 patients), African 38.2% (78 patients) and European 18.1% (37 patients). The most frequent haplogroup in the studied population was Amerindian origin C (34 patients; 16.7%), followed by African origin L3 (33 patients; 16.2%). The most common haplogroups of European ancestral origin in the population were U and J, which were observed in 8 patients (3.92%) for each haplogroup (Table 1).
Maternal lineages of African, European and Amerindian descent are expected to occur at different frequencies in Brazilian regions due to different interethnic crossings during the colonization period.
The most frequent subhaplogroup of Native American origin in the studied patients with T1D was C1b (24 patients, 11.7%), which was observed in 15 patients from the Northeast Region, 2 from the South Region and 7 from the Southeast Region. C1b is often defined as “Pan American”, as it is found in both North and South American Native Americans of Beringian origin. The C1 haplogroup was also the most frequently found in Botocudo origin (Brazil) individuals [18]. However, when comparing our results with those of other countries in South America, the most frequent haplogroup in Colombia was A2 (40%), while in our study population, it accounted for only 10.3% [18, 19].
The most frequent subhaplogroups of African origin in the studied patients with T1D were L3e and L1c (19 patients [9.3%] and 14 patients [6.8%], respectively). These subhaplogroups constitute approximately half of the African fraction of the Brazilian population (49%) studied by Alves-Silva and originated from Central Africa [20, 21].
Regarding haplogroups of European origin, our results revealed that haplogroups U and J were the most frequent (n = 8; 3.9% both). For the most common subhaplogroups, we found R0 (n = 6; 2.9%), which is frequently found in Western Europe [22].
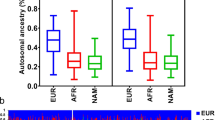
To determine whether there is any relationship between self-reported color and matrilineal ancestry haplogroups, we determined the distribution of the ancestry origins of the matrilineal lineages (African [AFR], European [EUR] and Native America [NAM]) by groups of self-reported colors (White, Black, Brown and Yellow) in patients with T1D, as shown in Fig. 2.

Distribution of matrilineal ancestral origin by self-reported color groups in patients with T1D (NAM: Native American; AFR: African; EUR: European)
In the present study, 42.6% (n = 87) of the patients self-declared White, 5.4% Black (n = 11) and 50.9% Brown (n = 104). Our data are similar to those of the last IBGE demographic census, 2010, which revealed that the Brazilian population comprises 47.7% Whites, 7.6% Blacks, 43% Browns, 1.1% Yellows and 0.4% Native Americans [23].
Additionally, in the present study, we observed a greater number of patients of native American origin with matrilineal ancestry. According to self-declaration, those who declared themselves White had predominantly Native American matrilineal ancestry (50.6%; 44 patients); those who declared themselves to be Brown had a similar frequency of African and Native American matrilineal ancestry (45.2% and 42.3%; 47 patients and 43 patients, respectively); and those who declared themselves Black had matrilineal ancestry of African origin (90.9%; 10 patients). ANOVA was used to validate our hypothesis, and a p value of 0.0513 indicated a tendency.
Conclusion
The present study of patients with T1D revealed that matrilineal ancestry of Native American origin was the most common, followed by that of African and European ancestry. Our data corroborate those of other studies, confirming the influence of Brazil’s historical colonization period on the formation of the genetic pool of the Brazilian population. Further studies with a large sample of patients with T1D in all geographic regions are needed to investigate this pattern for a better definition of the role of DNAmt in the pathogenesis of the disease.
Availability of data and materials
The used datasets and/or analyzed during the current study are available with the corresponding author upon reasonable request.
Abbreviations
- ISFG:
-
International Society for Forensic Genetics
- T1D:
-
Type 1 diabetes
- HLA:
-
Histocompatibility leukocyte antigen system
- mtDNA:
-
Mitocondrial DNA
- HVS:
-
Hypervariable segments
- rCRS:
-
Control region
- PCR:
-
Polymerase chain reaction
- OXPHOS:
-
Oxidative phosphorylation
- AFR:
-
African
- EUR:
-
European
- NAM:
-
Native American
References
Gomes MB, et al. Self-reported color-race and genomic ancestry in an admixed population: a contribution of a nationwide survey in patients with type 1 diabetes in Brazil. Diabetes Res Clin Pract. 2018;21(140):245–52.
Dimeglio LA, et al. Type 1 diabetes. Lancet. 2018;391(10138):2449–62.
Bluestone JA, et al. Genetics, pathogenesis and clinical interventions in type 1 diabetes. Nature. 2010;464(7293):1293–300.
Atkinson MA, et al. Diabetes tipo 1. Lancet. 2014;383(9911):69–82.
Maahs D, et al. Epidemiology of type 1 diabetes. Endocrinol Metab Clin N Am. 2010;39(3):481–97.
Norris JM, et al. Type 1 diabetes-early life origins and changing epidemiology. Lancet Diabetes Endocrinol. 2020;8(3):226–38.
Filograna R, Mennuni M, Alsina D, Larsson NG. Mitochondrial DNA copy number in human disease: the more the better? FEBS Lett. 2021;595(8):976–1002.
Stoccoro A, Coppedè F. Mitochondrial DNA methylation and human diseases. Int J Mol Sci Published. 2021. https://doi.org/10.3390/ijms22094594.
Yan C, Duanmu X, Zeng L, Liu B, Song Z. Mitochondrial DNA distribution mutations, and elimination. Cells. 2019. https://doi.org/10.3390/cells8040379.
Mohamed Yusoff AA, Mohd Khair SZN, Wan Abdullah WS, Abd Radzak SM, Abdullah JM. Somatic mitochondrial DNA D-loop mutations in meningioma discovered: a preliminary data. J Cancer Res Ther. 2020;16(6):1517–21. https://doi.org/10.4103/jcrt.JCRT_1132_16.
Wallace DC. Mitochondrial DNA variation in human radiation and disease. Cell. 2015;163(1):33–8. https://doi.org/10.1016/j.cell.2015.08.067.
Aboulmaouahib B, Kastenmüller G, Suhre K, et al. First mitochondrial genome-wide association study with metabolomics. Hum Mol Genet. 2022;31(19):3367–76. https://doi.org/10.1093/hmg/ddab312.
Liu E, Kaidonis G, Gillies MC, et al. Mitochondrial haplogroups are not associated with diabetic retinopathy in a large Australian and British Caucasian sample. Sci Rep. 2019;9(1):612. https://doi.org/10.1038/s41598-018-37388-8.
Wallace DC, Chalkia D. Mitochondrial DNA genetics and the heteroplasmy conundrum in evolution and disease. Cold Spring Harb Perspect Biol. 2013;5(11): a021220. https://doi.org/10.1101/cshperspect.a021220.
Cardena MMSG, et al. Relationship between self-declared ethnicity, mitochondrial haplogroup and genomic ancestry in individuals from southeast of Brazil. Ética Justiça. 2013;18:62–6.
Lins TC, et al. Genetic composition of Brazilian population samples based on a set of twenty-eight ancestry informative SNPs. Am J Hum Biol. 2010;22:187–92.
Pena SDJ, et al. The genomic ancestry of individuals from different geographical regions of Brazil is more uniform than expected. Belo Horizonte. 2011. https://doi.org/10.1371/journal.pone.0017063PLOSONE.
Gonçalves VF, et al. Identification of polynesian mtDNA haplogroups in remains of Botocudo Amerindians from Brazil. Proc Natl Acad Sci USA. 2013;110(16):6465–9.
Salas A, et al. The mtDNA ancestry of admixes Colombian populations. Am J Hum Biol. 2008;20:584–91.
Alves-Silva J, et al. The ancestry of Brazilian mtDNA lineages. Am J Hum Genet. 2000;67(2):444–61.
Poletto MM, et al. Mitochondrial DNA control region diversity in a population from Parana state-increasing the Brazilian forensic database. Int J Legal Med. 2019;133(2):347–51.
Álvarez-Iglesias V, et al. New population and phylogenetic features of the internal variation within mitochondrial DNA macro-haplogroup R0. PLoS ONE. 2009;4(4):1–9.
Ibge—Instituto Brasileiro De Geografia E Estatística. Censo Brasileiro de 2010 Rio de Janeiro IBGE. 2012
Acknowledgements
The authors would like to thank the volunteers who donated their samples for this study and to the Brazilian Type 1 Diabetes Study Group (BrazDiab1SG) (Additional Table 1).
Funding
CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) Grant number 88887.602580/2021-00; FAPERJ (Fundação do Amparo à Pesquisa do Estado do Rio de Janeiro), Grant number 260003/001128/2020, 26/200.521/2023 and CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico do Brasil) (grant number 563753/2010-2 and 304367/2021-4).
Author information
Authors and Affiliations
Contributions
RSA, DAS and MBR contributed to the study design and study conception. Material preparation and data collection were performed by RSA, DAS and MBR. LLF, SL, ABRG, ASD, and IJBA conducted the analyses. The first draft of the manuscript was written by LLF. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval was obtained before the start of the study by the Research Ethics Committee of the HUPE-UERJ (Pedro Ernesto University Hospital, State University of Rio de Janeiro) with the number CAAE 53563115.2.1001.5259. All procedures performed were in accordance with the ethical standards of the Helsinki Declaration of 1964 and later versions.
Informed consent
Informed consent was obtained from all patients prior to recruitment.
Competing interests
All the authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ferreira, L.L., Gonçalves, A.B.R., Adiala, I.J.B. et al. A pilot study of mitochondrial genomic ancestry in admixed Brazilian patients with type 1 diabetes. Diabetol Metab Syndr 16, 130 (2024). https://doi.org/10.1186/s13098-024-01342-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-024-01342-8