
Abstract
Background
As the common delayed complication of supracondylar fractures in children, cubitus valgus/varus deformity might lead to pain and loss of motion of the elbow. The current corrective treatment might not be accurate enough and even contribute to postoperative deformity. This study retrospectively analyzed the clinical value of preoperative simulated surgery on 3D model-assisted osteotomy feasibility verification and surgical guidance for cubitus valgus/varus deformity.
Methods
Seventeen patients were selected from January 2017 and November 2019. Deformities were analyzed from imaging data and 3D models and corrected after the simulated operations. The radiographic evaluation comprised osseous union, carrying angle, and anteversion angle of the distal humerus. The clinical evaluation was performed according to the Hospital for Special Surgery (HSS) scoring system.
Results
All patients underwent the operation successfully and had no postoperative deformity. The carrying angle was significantly improved postoperatively (P < 0.001). The anteversion angle of the distal humerus did not change significantly (P > 0.05). The HSS score rose after surgery (P < 0.001). The function of the elbow joint was excellent in seven cases and good in ten cases.
Conclusion
Simulated surgery on 3D model plays an important role in osteotomy plan and surgical guidance, contributing to good surgical efficacy.
Similar content being viewed by others


Background
Elbow deformities, comprising cubitus varus and cubitus valgus, are one of the most common delayed complications of the distal humerus fractures in children, especially supracondylar fractures of the humerus [1,2,3,4,5]. While most of supracondylar fractures in children could be treated conservatively [6], such as cast immobilization and elevated, straight-arm traction, approximately 20% of supracondylar fractures require surgical treatment [7]. Without proper treatment, the incidence of cubitus varus after supracondylar fracture of the humerus is as high as 50% [8]. Compared with cubitus valgus, cubitus varus is more common [9].
Elbow deformities are often regarded as cosmetic problems rather than diseases in need of treatment. However, in addition to appearance, the deformities also bring about varying degrees of damage to the function of the elbow, such as limitations in the functional activities of extension and flexion, traumatic ulnar neuritis, joint pain, and instability [10]. In the clinic, when these degrees of damage occur, correction is necessary. Previous studies [11,12,13] have described different corrective supracondylar osteotomies as the standard treatment for elbow deformities: open/closed wedge osteotomy, French osteotomy, and dome osteotomy.
Whether accurate osteotomy can be performed strictly according to the preoperative steps planned can affect surgical outcomes. However, in the past, osteotomy performance has been mostly based on the clinical experience of orthopedic surgeons, and traditional deformity correction is often limited to the two-dimensional plane, which easily leads to postoperative deformity [14, 15]. Currently, with the wide use of three-dimensional printing techniques in orthopedics, there have been some related reports about the successful application of three-dimensional printing techniques in the clinical treatment of elbow deformities worldwide [Full size image
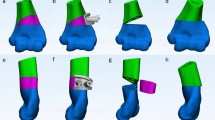
Finally, the angle was measured, the deformity was fixed, the orthopedic operation was successfully completed, and the key steps and correction angles in the simulated operation were recorded as a reference for the actual operation (Fig. 2G).
Intraoperative procedure
The patients were placed in the supine position under general anesthesia. A sterile tourniquet was applied. A posterior median incision was made in the elbow joint. Then, the skin, subcutaneous tissue, and deep fascia were cut open in turn. After exposure, the ulnar nerve was released and protected.
According to the plan from the preoperative simulated operation, osteotomy of the elbow joint (distal humerus or/and proximal ulna) was performed with determined correction angles at the determined osteotomy level (Fig. 3A). First, the position and direction of the bone cuts were marked with K-wires using fluoroscopy. Then, osteotomy was performed with an oscillating saw following the placed K-wires. The wedge-shaped bone mass was removed by vascular forceps (Fig. 3B). After closing the bone gap, the alignment of the upper limbs was readjusted until the result was satisfactory (Fig. 3C). All osteotomies were fixed with preoperatively shaped, locked, and suitable plates. During surgery, the key steps and key data were recorded.

Closed wedge osteotomy of the proximal ulna in one patient: A Osteotomy of the proximal ulna was performed. B The wedge-shaped bone was removed by vascular forceps. C The osteotomy site was closed and temporarily fixed
Radiographic and clinical evaluation
Before surgery and at the most follow-up evaluation, radiographic and clinical evaluations were conducted for all the patients. The disappearance of the osteotomy line and continuity of the trabecular bone indicated complete union. For all the patients, the carrying angle, humeral deformity angle (defined by the longitudinal humeral axis and the upper ulnar and radial articular surface lines), and ulnar deformity angle (if present) (defined by the ulnar surface line and the upper ulnar and radial articular surface lines) in the coronal plane, as well as the anteversion angle of the distal humerus in the sagittal plane, were measured on plain X-ray to make orthopedic plans.
During the follow-up, the carrying angle and anteversion angle of the distal humerus were measured on plain X-ray and used to evaluate the elbow. To better evaluate the carrying angle, the valgus direction was considered positive, and the valgus direction was considered negative. The ranges of motion of the elbow were given attention. The HSS (Hospital for Special Surgery) score [19] was used to evaluate preoperative and postoperative elbow function.
Statistical analysis
SPSS for Windows software (version 26.0, IBM®, Chicago, IL, USA) was used for statistical analysis. Statistical significance was set at P < 0.05. The Shapiro‒Wilk test was used to test the normality of the measurement data. Measurement data following a normal distribution are expressed as \(\overline{x }\)±s, and those with a nonnormal distribution are expressed as M(Q25–Q75). For preoperative and postoperative data, as well as postoperative and simulation-operative data, a paired sample t-test was used when the data followed a normal distribution, and the Frank Wilcoxon test was used when the data did not conform to a normal distribution.





