
Abstract
Background
Medication for opioid use disorder (MOUD) is the gold standard treatment for opioid use disorder. Traditionally, “success” in MOUD treatment is measured in terms of program retention, adherence to MOUD, and abstinence from opioid and other drug use. While clinically meaningful, these metrics may overlook other aspects of the lives of people with opioid use disorder (OUD) and surprisingly do not reflect the diagnostic criteria for OUD.
Methods
Authors identified items for a pilesorting task to identify participant-driven measures of MOUD treatment success through semi-structured interviews. Interviews were transcribed verbatim and coded in Nvivo using directed and conventional content analysis to identify measures related to treatment success and quality of life goals. Participants of a low-threshold MOUD program were recruited and asked to rank identified measures in order of importance to their own lives. Multidimensional scaling (MDS) compared the similarity of items while non-metric MDS in R specified a two-dimensional solution. Descriptive statistics of participant demographics were generated in SPSS.
Results
Sixteen semi-structured interviews were conducted between June and August 2020 in Philadelphia, PA, USA, and 23 measures were identified for a pilesorting activity. These were combined with 6 traditional measures for a total list of 29 items. Data from 28 people were included in pilesorting analysis. Participants identified a combination of traditional and stakeholder-defined recovery goals as highly important, however, we identified discrepancies between the most frequent and highest ranked items within the importance categories. Measures of success for participants in MOUD programs were complex, multi-dimensional, and varied by the individual. However, some key domains such as emotional well-being, decreased drug use, and attendance to basic functioning may have universal importance. The following clusters of importance were identified: emotional well-being, decreased drug use, and human functioning.
Conclusions
Outcomes from this research have practical applications for those working to provide services in MOUD programs. Programs can use aspects of these domains to both provide patient-centered care and to evaluate success. Specifics from the pilesorting results may also inform approaches to collaborative goal setting during treatment.
Similar content being viewed by others


Introduction
Opioid overdose deaths in the US surpassed 80,000 in 2021 [8]. Medication for opioid use disorder (MOUD) with methadone, buprenorphine, or naltrexone is the gold standard evidence-based treatment for opioid use disorder (OUD) [32, 33, 38]. MOUD is associated with longer retention in treatment [44] as well as decreased opioid use [29, 40] and mortality from overdose [48]. Other research suggests MOUD can reduce all-cause mortality and increase quality of life [11, 29]. However, access to and retention in MOUD remains limited in some settings [4, 13, 24]. Improving treatment engagement and outcomes requires consideration of misalignment between the programmatic and patients’ goals of treatment [19, 34].
Traditionally in the literature, “success” in MOUD treatment is measured in terms of program retention, adherence to MOUD, and abstinence from opioid and other drug use (e.g., cocaine, methamphetamine) [5, 20, 27, 31]. While clinically meaningful, these metrics may overlook other aspects of the lives of people with OUD and surprisingly do not reflect the diagnostic criteria for OUD, which include the highly personal repercussions of opioid use such as problems fulfilling obligations, recurring interpersonal problems, and giving up activities [2]. This is important because, as compared to people who are not using opioids, people who use opioids rate their quality of life lower in multiple areas across studies including social functioning, physical and emotional role limitations, general health, and mental health [11, 16]. MOUD treatment may also be considered successful, therefore, if participants report improvements in these areas of quality of life.
Some research on MOUD outcomes increasingly focuses on measuring changes in quality of life among people with OUD. Authors of a recent systematic review reported 12 domains of importance to people with OUD. While these included traditional metrics, such as treatment retention and abstinence from other drugs, they also placed importance on improvements in daily life, physical health, and discontinuing MOUD [42]. Authors called for deeper qualitative investigation into outcomes important to patients.
Hooker et al. [21] reported seven themes of program success for patients that included improvements in physical and mental health, goal-setting, and social relationships [21]. These studies, however, did not ask MOUD participants to rank items within themes, or the themes themselves, in terms of importance. Most studies have been conducted in settings outside of the United States, with different MOUD regulations and program structures [9, 18, 30, 39, 42, 43]. Two studies in the United States focused exclusively on participants in methadone programs [17, 36]. Without knowing outcome importance across multiple themes, MOUD programs will have difficulty establishing priorities with clients. In the present study, we report on ranked outcomes of participant-driven measures of success, gathered through MOUD program participants and the literature, within a multi-site, low-threshold MOUD program.
Materials and methods
This exploratory study had two arms of data collection: 1) the identification of items for the pilesorting task through semi-structured interviews and 2) the completion of the pilesorting task and collection of relevant participant demographic data. Pilesorting is a mixed-methods approach in which participants are given a stack of terms or domains and asked to sort them into meaningful ranks (e.g., in terms of importance) [46]. This study was designed, conducted, and analyzed by a cisgender female Assistant Professor with an MPH and PhD in Public Health (MKR), a cisgender female research coordinator with a BA in Anthropology (KRS), a cisgender female third-year medical student with a BS in Biology (FS), a cisgender male Assistant Professor with a PhD in Psychology (RH), a cisgender female second-year medical student with a masters in public health (ALC), a cisgender female Assistant Professor with a PhD in Psychology (ELK), and a cisgender female Associate Professor with an MPH, DrPH, and MD (LCW). Authors MKR, KRS, RH, ELK, and LCW all have previous experience with mixed-methods study design, implementation, and analysis. This research was approved by the Institutional Review Board at Thomas Jefferson University. Authors used the consolidated criteria for reporting qualitative research (COREQ) [45].
Setting and program description
Project HOME Health Services (PHHS) offers low-threshold MOUD services at three locations in Philadelphia, PA, USA 1) Stephen Klein Wellness Center (SKWC), a large primary-care clinic with integrated, on-site behavioral health, dental, and pharmacy services 2) Pathways to Housing PA (PTHPA), an embedded primary care clinic within a Housing First organization for people with experiences of chronic homelessness, serious mental illness, and substance use disorders, and 3) The Hub of Hope, a primary care clinic within a drop-in service center for people experiencing homelessness (for more details see [49]). We extended data collection to include participants of PTHPA MOUD groups, which also included people taking methadone.
Study design and analysis – qualitative interviews
Items for the pilesorting task were identified through a secondary analysis of qualitative interviews with participants in MOUD programs. The interviews were conducted with potential participants of a community advisory board and demographic data were not collected. As part of the semi-structured interview, patient-important measures of success were captured from participants within a singular MOUD program at the Pathways to Housing PA (PTHPA) site. Staff at PTHPA recruited participants between June to August 2020 and author ELK conducted all interviews. Individuals who were 18 years and older, English-speaking, and an active patient within the MOUD program at Pathways to Housing PA were eligible to participate. Potential participants were given all relevant study information, verbally consented, and asked to complete an interview with ELK over the phone or via Zoom. Virtual data collection was selected because of the COVID-19 pandemic. Participants who completed data collection over Zoom used an iPad in a private conference room in PTHPA. Sixteen interviews were conducted using an interview guide developed by authors LCW and ELK that assessed the following domains of interest: previous experience in MOUD program (“How has it been going in the medication-assisted treatment (MAT)/Suboxone program?”), motivation for treatment (“Why did you decide to start this Suboxone program?”, “Why do you continue to participate in this suboxone program?”), personal goals within MOUD program (“Do you have goals for yourself around Suboxone and drug use?”), and self-identified measures of success (“What does a good day look like for you?”, “How can we tell that people are doing well in this program?”). We used the language in prompts that participants were most familiar with (e.g., “MAT” instead of “MOUD”). Most interviews lasted 20–30 minutes; the shortest was 12 minutes and the longest was 44 minutes. At the completion of the interview, participants were compensated $20 and asked if they would be interested in joining a Patient Advisory Council for the MOUD program. Items from the interviews were supplemented with traditional outcome measures as traditionally used in MOUD program evaluations to create a final list of items for the pilesorting task (see Table 1).
Audio-recorded interviews were professionally transcribed verbatim and uploaded into qualitative data analysis software, Nvivo (released in March 2020). Interviews were analyzed by authors MKR, KRS, ELK, and LCW using a combination of directed and conventional content analysis to identify themes related to operationalizing treatment success and quality of life goals [23]. Four coders (authors ELK, MKR, KRS, and LCW) used a combination of a priori codes (e.g., “abstinence from opioids”) and open coding (e.g., “happiness”) to establish a codebook, then coded material in teams of two to three using an iterative process to identify themes related to MOUD treatment success. The team met weekly to discuss progress and resolve discrepancies by consensus. The team reviewed the themes and developed items for pilesorting using participants’ own words when possible (e.g., “Well, when people come, they share. They come every week and they share. You can tell by their sharing how well a person is doing” was grouped with similar comments to make the pilesorting card “Regularly contributing in MAT/Suboxone group”. Saturation for the initial study was achieved as determined by a lack of new domains raised in the three final interviews.
Study design and analysis - pilesorting
The pilesorting task was facilitated by authors MKR, KRS, and ALC between June and September 2021 at all three PHHS sites. Individuals were recruited by authors at MOUD program meetings and through staff referral at each community site. Individuals who were 18 years and older, English-speaking, and a patient within the MOUD program at their respective community site were eligible to participate. Eligible participants were given all relevant study information, verbally consented, and asked to fill out a demographic survey in a private space prior to beginning the pilesorting task. The demographic survey asked for data on participants’ age, race, ethnicity, gender, education level, housing status, history of substance use and treatment, and engagement with their current MOUD program.
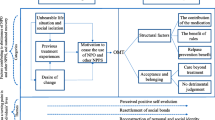
The interviewer then laid out the category titles out on a table in front of individual participants (see Fig. 1) and led with the following prompt: “Imagine it is 5 years from now, we run into each other on the street or in the grocery store. I see you and say ‘[Name of participant], it is good to see you! How are you doing?’ and you respond, ‘I’m doing great, everything is going so well’. We want to know how important each of these things are when you think about doing well or being successful in life or treatment”.

Visual of Pile-Sorting Task Activity. Note: Participants were able to place items under each bucket and then to rank order those items within each category of importance
The interviewer then handed the pile of cards to the participant and asked them to sort the cards into the four categories of High, Medium, Low, and No Importance without worrying about the order in each individual category. Once the participant had sorted each card into a pile, they were asked to then rank the cards from Most to Least Important within each category. Upon completion of the task, the interviewer thanked the participant and asked if there were any cards that were not in the pile that they thought should be there. These answers were recorded by the interviewer. Participants were compensated with $10 cash and the interviewers recorded the results in Qualtrics using the pick, sort, and rank function. Cards were always returned to the same order for the next participant. The process lasted from 15 to 30 minutes depending on how quickly the participant sorted each card.
Multidimensional scaling (MDS) is the method of choice for pilesorting data analysis [1, 6]. MDS is a data reduction technique in which a matrix of inter-item distances or similarity scores is projected onto a smaller dimensional surface. For example, items might be 15 cities and distances might be miles between each pair of cities. A two-dimensional solution applied to the matrix of inter-city distances will yield coordinates that can be plotted on a two-dimensional map. The map will accurately represent the distances and clustering of the 15 cities.
When items are conceptual, as in the current study, non-metric MDS can be used on a matrix of inter-item similarities. Borghati [6] reasoned that the greater number of participants who put two items in the same pile, the greater the similarity of the items (see also [1]). Thus, the overall inter-item similarity matrix was constructed by first constructing single-subject matrices. The single subject matrices were constructed as follows: a 29 by 29 item matrix with the items in Table 1 as rows and columns was filled with 1’s and 0’s according to whether that participant put the pair of items in the same pile. For example, if a participant put “taking my suboxone as prescribed” and “stop taking my suboxone someday” in the same pile, then the cell in the second row-first column of that single subject matrix would be filled with a 1. These single-subject matrices are symmetric with 1’s on the diagonal, so only the lower triangle is analyzed. Once each participant’s matrix was filled, the 28 single-subject matrices were added together to yield an overall interitem matrix. This overall inter-item similarity matrix represented similarity in terms of the number of participants who put the pair of terms in the same pile. For example, if 28 out of 28 participants put “taking my suboxone as prescribed” and “stop taking my suboxone someday” in the same pile, the overall inter-item matrix would have a 28 in the second row-first column. The process of creating the matrices was automated using the R Statistical Programming Environment [41].
Non-metric MDS was then performed in R on the overall similarity matrix specifying a two-dimensional solution. Prior to running MDS, the matrix was transformed into a dissimilarity matrix by subtracting each cell count from the highest off-diagonal cell count (23 in this case). This yielded a more stable solution and simply re-scaled the item distances while preserving the relationships. The goal of this non-metric MDS was to represent the distances among the items in a two-dimensional space. This kind of dimension reduction aids in interpreting the distances (and similarities) among the items and can yield insights into participants’ conceptualizations of concepts that can be used to make new questionnaires and surveys.
Results
Semi-structured interviews
A total of 16 semi-structured interviews were conducted with Pathways to Housing PA MOUD program participants between June and August 2020. No demographic data were collected and therefore, none are reported here. Analysis of themes resulted in items 1–23 in Table 1. An additional six items typically found in MOUD program evaluations (negative urine drug screens, incarceration and recidivism, HIV/HCV infection, hospitalization and Emergency Department utilization, and the reduction of overdose and pain) were added for a grand total of 29 items [3, 7, 11, 12, 14, 15, 25, 26, 28, 29, 40, 44, 49].
Pilesorting task
Thirty-one people provided informed consent. Among these, two were unable to complete the task and a third was ineligible, leaving a final dataset from 28 people. The median age of participants was 42 years old. Most participants identified as not Latino or Hispanic (96%), White (54%) or Black/African American (43%), and male (71%). Most had a Grade 12 or GED education (54%) and were living in their own home/apartment (57%). Only one participant was on methadone; the remainder (96%) were on buprenorphine The median age of first opioid use was 24. Seventy-one percent considered heroin/fentanyl to be their drug of choice and 46% had used heroin/fentanyl in last 30 days. Fifty-four percent reported taking buprenorphine 7 days a week. (see Table 2) One participant had also participated in the semi-structured interview.
Most reported participation in prior substance treatment programs, including outpatient (93%), inpatient (82%), AA/NA or another abstinence-based group (68%), individual therapy (68%), and methadone (57%). Forty-six percent of participants had participated in the buprenorphine program for 1 year or less. Before COVID-19, most participants were attending a buprenorphine group in person either once a week (32%) or not at all (61%). Since COVID-19, 43% of participants were communicating with their buprenorphine provider once a week or more.
Item frequency and rank did not perfectly overlap. Participants most frequently placed the following items in the High Importance bucket: stable housing (n = 25), no opioids (n = 23), no physical dependence (n = 23), being happy (n = 22), feeling neat and clean (n = 22), optimism (n = 21), self-worth (n = 20), and no arrests (n = 20). The most frequently placed items in the Medium Importance bucket were having a sense of community (n = 17), attending group (n = 12), and handling frustrations (n = 12). In the Low Importance bucket, participants most frequently selected decreasing ED or hospital visits (n = 3), decreasing OD (n = 6), having a sense of community (n = 6), abstinence from all drugs (n = 6), and less pain (n = 4). In the No Importance bucket, the most frequently placed items were being tested for HIV/HCV (N = 10), decreasing OD, (n = 10) decreasing ED or hospital visits (n = 8), and decreasing use of opioids (n = 7) (see Fig. 2). By contrast, the highest median ranked items in this High Importance bucket were abstinence from all drugs (median rank = 2), stable housing (median rank = 4) not using opioids (median rank = 5) and being happy (median rank = 5). The highest median ranked items in the Medium Importance bucket were decreasing opioid use (median rank = 1.5) and (re)connecting with family (median rank = 2). The highest median ranked items in the Low Importance bucket were not using opioids (median rank = 1), decreasing opioid use (median rank = 1.5), not using other non-opioid drugs (median rank = 1.5), and (re)connecting with family (median rank = 1.5). The highest median ranked items in the No Importance bucket were abstinence from all drugs (median rank = 1) and not being physically dependent on drugs (median rank = 1).

List of term numbers* and the frequency of bucket assignment from participants in MOUD programs in Philadelphia, PA (n = 28)
*Please see Table 2 to connect term number to corresponding term
The MDS solution and map are easier to interpret in relation to the ranking of items within each of the importance “buckets.” The importance of items was expressed in terms of frequency (e.g., how many participants placed the term in a bucket) and rank (e.g., the median location within a bucket where items were placed). Overall, every item (n = 29) was placed in the high importance bucket at by at least 1 participant, “Having a stable place to live” the only item to not appear in the medium importance bucket, “Managing money well” was the only item to not appear in the low importance bucket, and while 6 items did not appear in the no importance bucket: “Taking my suboxone as prescribed”, “Co** with difficult emotions”, “being happy”, “having self-worth”, “accomplishing daily goals/tasks”, and “feeling neat and clean.”
As described, non-metric MDS was used to map the inter-item similarities onto a two-dimensional map (see Fig. 3). Along with frequency information, this allows for an understanding of whether participants see different items as similar in terms of importance. This was done by interpreting closely plotted items as conceptual clusters [22]. Figure 3 illustrates three conceptual clusters of items. These clusters were identified through research team consensus. First, a primary cluster in the middle was comprised of three facets of emotional well-being (e.g., optimism, being happy, having a sense of self-worth), decreased drug use (e.g., no opioids, no physical dependence), and human functioning (e.g., stable housing, being neat and clean). All items within these clusters most often appeared in the high-importance bucket, with stable housing being the item with the greatest number of participants (n = 25) sorting it into the high-importance bucket.

Multi-Dimensional Scaling Map of MOUD Treatment Outcomes. Cluster 1 (Items 16, 17, 18): Being able to honestly communicate with others in MAT/Suboxone group, regularly contributing in MAT/Suboxone group (ex. Talking and sharing in group), regularly attending MAT/Suboxone group. Cluster 2 (Items 6, 3, 1): Not using other substances that are not opioids (ex. Cocaine, methamphetamine, alcohol), abstinence from all drugs, taking my Suboxone as prescribed. Cluster 3 (Items 4, 11, 12, 13, 22, 8, 20): not using opioids; being happy; having hopes, dreams and goals for the future (ex. Feeling hopeful/optimistic about the future); having self-worth (ex. Feeling good about myself on a daily basis); having a safe, stable place to live, not being physically dependent on drugs (ex. Not needing to get well/not having withdrawal); feeling neat and clean (ex. Being able to shower/use deodorant/brush my teeth, etc.). Note: The numbers reflect each of the items (see Table 1) and their relative proximity reflects their conceptual clustering, meaning that items that are further apart are less conceptually close
Items in the other clusters were more homogenous. In the second cluster were items related to buprenorphine groups (e.g., attending group, contributing to the group, and being honest in group). Items in this cluster were more uniformly distributed among the buckets by participants who mostly sorted them into the high and medium frequency buckets. The third cluster was related to traditional buprenorphine success metrics (e.g., taking my Suboxone as prescribed, abstinence, no other substances). Items in this cluster were most often sorted into the high importance bucket.
Participants added 18 additional items when asked whether anything important to them and their success was not on the list (“Are there any items that aren’t here that you think should be?”). These were categorized through discussion with the entire author group into improved relationships (e.g., having friends, being able to actively support family), personal well-being (e.g., talk therapy, taking care of medical needs, self-accountability), and daily life (e.g., having hobbies not related to drug use, exercise, spirituality).
Discussion
In this exploratory study, participants in MOUD services ranked the overall priority of participant-derived measures and traditional metrics in order of importance to their own lives and indicators of success from their MOUD treatment. Participants identified a combination of traditional and stakeholder-defined recovery goals as highly important, however, we identified discrepancies between the most frequent and highest ranked items within the importance categories. The main items identified as highly important and ranked highest by participants, which were clustered in the multi-dimensional scaling map, included stable housing, not using opioids, being happy, and having a sense of self-worth. This indicates that while the traditional goal of not using opioids specifically is of primary importance to PWUD, other facets of life that represent a more holistic sense of recovery are also important. For PWUD, other traditional outcomes of not being physically dependent on a drug and not being arrested were frequently named as highly important but did not rise to a level of high rank, indicating these might not be relevant current concerns for participants and reflect a point of divergence from providers’ primary priorities for them. These findings are part of a growing literature supporting an expanded understanding of how services providers could evaluate the progress of their participants that is more congruent with the treatment goals of their participants [21, 42].
Some traditional measures of MOUD success, such as being tested for HIV, decreasing overdose, and decreasing hospital visits are often used as measures for “quality of life” for people who use drugs [10, 35, 37, 47]. Our results were not aligned with these measures, nor were they in other recent literature with patient-derived measures of MOUD success [21, 42]. Facets of quality of life such as emotional regulation and housing stability took precedence over health-related variables. It should be noted that housing stability may have been especially important to participants in our study due to the participation of many participants in housing programs. Similarly, participants were recruited from organizations that provided other services to participants (e.g., health care, benefits coordination). If participants were having health-related needs met, they may have ranked related items as lower in importance.
In comparison to US-based studies with methadone program participants, our results had mixed support of findings from Gelpi-Acosta [17] and Mitchell et al. [36]. Participants from the former expressed a wish to avoid withdrawal, cease opioid use, and to have employment and family connections [17]. The latter echoed our findings more closely with participant emphases on stable housing, employment, and abstinence [36].
Unlike findings from some earlier work [36, 43], participants in our sample did not regularly emphasize the importance of a social network and social inclusion. However, responses to the open-ended question about what else comprised success resulted in some relationship-focused items, which could mean that the existing prompts related to social connection were less meaningful to participants. For example, our items indicating social connection were largely about desiring greater connections with others with lived experiences of drug use as opposed to greater connections with non-drug using peers. The open-ended responses, in contrast, included people not connected primarily through sharing a diagnosis of opioid use disorder. Expanding conceptualizations of what are meaningful elements of quality of life is important, as focusing solely on health-related quality of life measures for people with opioid use disorder is reductive, focusing almost exclusively on their lives as it relates to their drug use.
Outcomes from this research may have practical applications for those working to provide services in MOUD programs. In aggregate, participants placed a high number of terms in the High Importance category. This reflects that MOUD program participants have multiple, urgent, and likely competing demands. Therefore, choosing treatment priorities may feel difficult and overwhelming. Clinicians and others working with MOUD program participants in unstable circumstances should recognize how these competing demands may interfere with participants’ ability to consistently work towards a subset of goals at a time. Having conversations about how to prioritize these competing demands might help to mitigate these risks in conjunction with low-threshold programming (e.g., not adopting punitive policies for positive urine drug screens or missed appointments).
Specifics from the pilesorting results may inform approaches to collaborative goal setting during treatment. For example, most items about MOUD group were placed in close proximity to one another. To reduce the number of terms presented to clients during intake or goalsetting, a factor analysis can identify latent variables assessing the same domain. Our visual assessment of clusters identified the following latent variables as candidates for future measurement of treatment goals: emotional well-being (e.g., feeling happy and navigating difficult emotions), decreased drug use (e.g., abstinence of reduction of use), and attendance to basic functioning (e.g., being able to take care of daily needs and activities). Presenting these reduced categories to MOUD participants to identify their priority areas represents a truly patient-centered approach to working to achieve a range of life goals. As recommended elsewhere, these can be developed into scales and surveys for use with future patients to inform treatment structure [21, 42].
Limitations
The terms presented to participants were summarized from descriptions in the qualitative interviews and the literature and may have been interpreted differently by participants. Items from the qualitative interviews were generated by people experiencing chronic homelessness from whom we did not capture demographic data. They may have had different definitions of treatment success than participants at the other sites for the pilesorting activities. For example, unlike earlier work, participants in our sample did not regularly emphasize the importance of a social network and social inclusion [21, 42]. However, our social domains were largely about connections with others with lived experiences of drug use. Supporting the possible need to revise some items, responses to the open-ended question about what else comprised success resulted in some relationship-focused responses with those who are not involved in opioid use, which could mean that the existing prompts related to social connection were less meaningful to participants. Second, the definition of No Importance may differ across participants as they could place items in this bucket that were both not meaningful to them personally as well as items that were not applicable to them. For example, someone no longer at risk for HIV would place that item for the same bucket as they would for “contributing to MAT group”, which may not be an important facet if they don’t attend groups. Further, we collected data from a small sample participating in three MOUD programs in Philadelphia, PA, limiting generalizability of results. All but one of our participants was prescribed buprenorphine as MOUD, limiting our ability to generalize results to people on methadone. Our ability to generalize based on sample characteristics (e.g., only eight women) is restricted. A larger sample size could be stratified by participant time in treatment to determine whether those with greater time on MOUD had meaningfully different rankings than those newly enrolled in MOUD. Finally, data were collected during the COVID-19 pandemic, which may have influenced participant responses.
Conclusion
Measures of success for participants in MOUD programs are complex, multi-dimensional, and vary by the individual. However, some key domains such as emotional well-being, decreased drug use, and attendance to basic functioning may have universal importance. Programs can use aspects of these domains to both provide patient-centered care and to evaluate success.
Availability of data and materials
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
References
Albert SM. Cognition of caregiving tasks: multidimensional scaling of the caregiver task domain. Gerontologist. 1991;31(6):726–34. https://doi.org/10.1093/GERONT/31.6.726.
American Psychiatric Association. Opioid Use Disorder. https://www.psychiatry.org/patientsfamilies/addiction/opioid-use-disorder. Published November 2018. Accessed 24 Feb 2022.
Bachhuber MA, Thompson C, Prybylowski A, Benitez J, Mazzella S, Barclay D. Description and outcomes of a buprenorphine maintenance treatment program integrated within prevention point Philadelphia, an urban syringe exchange program. Subst Abus. 2018;39(2):167–72. https://doi.org/10.1080/08897077.2018.1443541.
Beetham T, Saloner B, Wakeman SE, Gaye M, Barnett ML. Access to office-based buprenorphine treatment in areas with high rates of opioid-related mortality: an audit study. Ann Intern Med. 2019;171(1):1–9. https://doi.org/10.7326/M18-3457/SUPPL_FILE/M18-3457_SUPPLEMENT.PDF.
Biondi BE, Zheng X, Frank CA, Petrakis I, Springer SA. A literature review examining primary outcomes of medication treatment studies for opioid use disorder: What outcome should be used to measure opioid treatment success? Am J Addict. 2020;29(4):249–67. https://doi.org/10.1111/AJAD.13051.
Borgatti SP. Elicitation techniques for cultural domain analysis. In: Schensul J, LeCompte M, editors. The Ethnographier’s toolkit. 3rd ed. Walnut Creek: Altmira Press; 1998. p. 1–26.
Bray JW, Aden B, Eggman AA, Hellerstein L, Wittenberg E, Nosyk B, et al. Quality of life as an outcome of opioid use disorder treatment: a systematic review. J Subst Abuse Treat. 2017;76:88. https://doi.org/10.1016/J.JSAT.2017.01.019.
Centers for Disease Control and Prevention. U.S. Overdose Deaths In 2021 Increased Half as Much as in 2020 - But Are Still Up 15%. https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/202205.htm. Published May 11, 2022. Accessed 4 July 2022.
Dale-Perera A, Alam F, Barker P. Opioid-dependence treatment in the era of recovery: Insights from a UK survey of physicians, patients and out-of-treatment opioid users. J Subst Use. 2015;20(5):354–62. https://doi.org/10.3109/14659891.2014.923532.
De Maeyer J, Vanderplasschen W, Broekaert E. Exploratory study on drug users’ perspectives on quality of life: more than health-related quality of life? Soc Indic Res. 2009;90(1):107–26. https://doi.org/10.1007/S11205-008-9315-7/TABLES/2.
De Maeyer J, Vanderplasschen W, Broekaert E. Quality of life among opiate-dependent individuals: a review of the literature. Int J Drug Policy. 2010;21(5):364–80. https://doi.org/10.1016/J.DRUGPO.2010.01.010.
Donroe JH, Bhatraju EP, Tsui JI, Edelman EJ. Identification and Management of Opioid use Disorder in primary care: an update. Curr Psychiatry Rep. 2020;22(5):1–11. https://doi.org/10.1007/S11920-020-01149-0/TABLES/3.
Drake C, Donohue JM, Nagy D, Mair C, Kraemer KL, Wallace DJ. Geographic access to buprenorphine prescribers for patients who use public transit. J Subst Abuse Treat. 2020;117:108093. https://doi.org/10.1016/J.JSAT.2020.108093.
Evans EA, Wilson D, Friedmann PD. Recidivism and mortality after in-jail buprenorphine treatment for opioid use disorder. Drug Alcohol Depend. 2022;231. https://doi.org/10.1016/J.DRUGALCDEP.2021.109254.
Fanucchi L, Springer SA, Korthuis PT. Medications for treatment of opioid use disorder among persons living with HIV. Curr HIV/AIDS Rep. 2019;16(1). https://doi.org/10.1007/S11904-019-00436-7.
Fischer JA, Conrad S, Clavarino AM, Kemp R, Najman JM. Quality of life of people who inject drugs: Characteristics and comparisons with other population samples. Qual Life Res. 2013;22(8):2113–21. https://doi.org/10.1007/S11136-013-0350-8/TABLES/4.
Gelpi-Acosta C. Challenging biopower: “liquid cuffs” and the “junkie” habitus. Drugs Educ Prev Policy. 2015;22(3):248–54. https://doi.org/10.3109/09687637.2014.987219.
Groshkova T, Metrebian N, Hallam C, Charles V, Martin A, Forzisi L, et al. Treatment expectations and satisfaction of treatment-refractory opioid-dependent patients in RIOTT, the randomised injectable opiate treatment trial, the UK’s first supervised injectable maintenance clinics. Drug Alcohol Rev. 2013;32(6):566–73. https://doi.org/10.1111/DAR.12062/SUPPINFO.
Gryczynski J, Mitchell SG, Jaffe JH, O’Grady KE, Olsen YK, Schwartz RP. Leaving buprenorphine treatment: patients’ reasons for cessation of care. J Subst Abuse Treat. 2014;46(3):356–61. https://doi.org/10.1016/J.JSAT.2013.10.004.
Hochheimer M, Unick GJ. Systematic review and meta-analysis of retention in treatment using medications for opioid use disorder by medication, race/ethnicity, and gender in the United States. Addict Behav. 2022;124:107113. https://doi.org/10.1016/J.ADDBEH.2021.107113.
Hooker SA, Sherman MD, Lonergan-Cullum M, Nissly T, Levy R. What is success in treatment for opioid use disorder? Perspectives of physicians and patients in primary care settings. J Subst Abuse Treat. 2022;108804. https://doi.org/10.1016/J.JSAT.2022.108804.
Hout MC, Papesh MH, Goldinger SD. Multidimensional scaling. Wiley Interdiscip Rev Cogn Sci. 2013;4(1):93–103. https://doi.org/10.1002/WCS.1203.
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88. https://doi.org/10.1177/1049732305276687.
Jones CW, Christman Z, Smith CM, Safferman MR, Salzman M, Baston K, et al. Comparison between buprenorphine provider availability and opioid deaths among US counties. J Subst Abuse Treat. 2018;93:19–25. https://doi.org/10.1016/J.JSAT.2018.07.008.
Korownyk C, Perry D, Ton J, Kolber MR, Garrison S, Thomas B, et al. Managing opioid use disorder in primary care: PEER simplified guideline. Canadian Family Physician. 2019;65(5):321–30.
Korthuis PT, McCarty D, Weimer M, Bougatsos C, Blazina I, Zakher B, et al. Primary care-based models for the treatment of opioid use disorder: a sco** review. Ann Intern Med. 2017;166(4):268–78. https://doi.org/10.7326/M16-2149.
Kumar N, Oles W, Howell BA, et al. The role of social network support in treatment outcomes for medication for opioid use disorder: A systematic review. J Subst Abuse Treat. 2021;127:108367. https://doi.org/10.1016/J.JSAT.2021.108367.
Lagisetty P, Klasa K, Bush C, Heisler M, Chopra V, Bohnert A. Primary care models for treating opioid use disorders: what actually works? A systematic review. PLoS One. 2017;12(10). https://doi.org/10.1371/JOURNAL.PONE.0186315.
Ma J, Bao YP, Wang RJ, Su MF, Liu MX, Li JQ, et al. Effects of medication-assisted treatment on mortality among opioids users: a systematic review and meta-analysis. Mol Psychiatry. 2018;24(12):1868–83. https://doi.org/10.1038/s41380-018-0094-5.
Marchand K, Foreman J, MacDonald S, Harrison S, Schechter MT, Oviedo-Joekes E. Building healthcare provider relationships for patient-centered care: a qualitative study of the experiences of people receiving injectable opioid agonist treatment. Subst Abuse Treat Prev Policy. 2020;15(1). https://doi.org/10.1186/S13011-020-0253-Y.
Mariolis T, Bosse J, Martin SA, et al. A systematic review of the effectiveness of buprenorphine for opioid use disorder compared to other treatments: implications for research and practice the impact of psychosocial treatment on medication treatment for opioid use disorder view project the effects of early adversity on chronic chronic HPA activity. View project a systematic review of the effectiveness of buprenorphine for opioid use disorder compared to other treatments: implications for research and practice. J Addict Res Ther. 2019;10(2). https://doi.org/10.4172/2155-6105.1000379.
Mattick RP, Breen C, Kimber J, Davoli M. Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane Database Syst Rev. 2009;3. https://doi.org/10.1002/14651858.CD002209.PUB2/INFORMATION/EN.
Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;2014(2). https://doi.org/10.1002/14651858.CD002207.PUB4.
McLean K, Kavanaugh PR. “They’re making it so hard for people to get help:” motivations for non-prescribed buprenorphine use in a time of treatment expansion. Int J Drug Policy. 2019;71:118–24. https://doi.org/10.1016/J.DRUGPO.2019.06.019.
Mcnamara KF, Biondi BE, Hernández-Ramírez RU, Taweh N, Grimshaw AA, Springer SA. A systematic review and Meta-analysis of studies evaluating the effect of medication treatment for opioid use disorder on infectious disease outcomes. Open Forum Infect Dis. 2021;8(8). https://doi.org/10.1093/OFID/OFAB289.
Mitchell SG, Morioka R, Reisinger HS, et al. Redefining retention: Recovery from the patient’s perspective. J Psychoactive Drugs. 2011;43(2):99–107. https://doi.org/10.1080/02791072.2011.587392.
Morgan JR, Schackman BR, Weinstein ZM, Walley AY, Linas BP. Overdose following initiation of naltrexone and buprenorphine medication treatment for opioid use disorder in a United States commercially insured cohort. Drug Alcohol Depend. 2019;200:34–9. https://doi.org/10.1016/J.DRUGALCDEP.2019.02.031.
Nielsen S, Tse WC, Larance B. Opioid agonist treatment for people who are dependent on pharmaceutical opioids. Cochrane Database Syst Rev. 2022;2022(9). https://doi.org/10.1002/14651858.CD011117.PUB3.
O’Reilly F, O’Connell D, O’Carroll A, Whitford DL, Long J. Sharing control: user involvement in general practice based methadone maintenance. Ir J Psychol Med. 2011;28(3):129–33. https://doi.org/10.1017/S079096670001209X.
Oesterle TS, Thusius NJ, Rummans TA, Gold MS. Medication-assisted treatment for opioid-use disorder. Mayo Clin Proc. 2019;94(10):2072–86. https://doi.org/10.1016/J.MAYOCP.2019.03.029/ATTACHMENT/381F99B4-6F42-4702-9F8C-16B6E0FF34D2/MMC1.MP4.
R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2015. Retrieved from https://www.r-project.org/
Sanger N, Panesar B, Dennis M, Rosic T, Rodrigues M, Lovell E, et al. The Inclusion of Patients’ Reported Outcomes to Inform Treatment Effectiveness Measures in Opioid Use Disorder. A Systematic Review. Patient Relat Outcome Meas. 2022;13:113. https://doi.org/10.2147/PROM.S297699.
Stöver H. Barriers to opioid substitution treatment access, entry and retention: a survey of opioid users, patients in treatment, and treating and non-treating physicians. Eur Addict Res. 2011;17(1):44–54. https://doi.org/10.1159/000320576.
Timko C, Schultz NR, Cucciare MA, Vittorio L, Garrison-Diehn C. Retention in medication-assisted treatment for opiate dependence: a systematic review. J Addict Dis. 2016;35(1):22–35. https://doi.org/10.1080/10550887.2016.1100960.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International J Qual Health Care. 2007;19(6):349–57. https://doi.org/10.1093/INTQHC/MZM042.
Trotter RT, Potter JM. Pile sorts, a cognitive anthropological model of drug and AIDS risks for Navajo teenagers: Assessment of a new evaluation tool. In: Drugs and Society. Vol 7. Taylor & Francis Group; 1993:23–39. https://doi.org/10.1300/J023v07n03_03.
Tysarowski M, Kazmi M, Barai R, Efobi R, Matassa D, Gordon E. Buprenorphine and methadone treatment is associated with less heart failure hospitalizations in patients with opioid use disorder. Circulation. 2020;142(Suppl_3). https://doi.org/10.1161/circ.142.suppl_3.16045.
Wakeman SE, Larochelle MR, Ameli O, Chaisson CE, McPheeters JT, Crown WH, et al. Comparative effectiveness of different treatment pathways for opioid use disorder. JAMA Netw Open. 2020;3(2):e1920622. https://doi.org/10.1001/jamanetworkopen.2019.20622.
Weinstein LC, Iqbal Q, Cunningham A, Debates R, Landistratis G, Doggett P, et al. Retention of patients with multiple vulnerabilities in a federally qualified health center buprenorphine program: Pennsylvania, 2017–2018. Am J Public Health. 2020;110(4):580–6. https://doi.org/10.2105/AJPH.2019.305525.
Acknowledgements
The authors would like to thank participants from semi-structured interviews and pilesorting activities. We would also like to thank staff from Pathways to Housing PA, the Hub of Hope, and Stephen Klein Wellness Center.
Funding
This work was supported by the Foundation for Opioid Response Efforts.
Author information
Authors and Affiliations
Contributions
Megan K. Reed: conceptualization, investigation, formal analysis, writing – original draft preparation. Kelsey R. Smith: conceptualization, project administration, investigation, formal analysis, writing – original draft preparation. Francesca Ciocco: conceptualization, formal analysis, writing – original draft preparation. Richard Hass: methodology, software, formal analysis, writing – original draft preparation. Avery Lin Cox: investigation, formal analysis, writing – original draft preparation. Erin L. Kelly: conceptualization, formal analysis, writing – review and editing. Lara Carson Weinstein: conceptualization, supervision, formal analysis, writing – review and editing, funding acquisition. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research was approved by the Institutional Review Board at Thomas Jefferson University. All study participants were provided with information about the study and provided verbal informed consent.
Consent for publication
Not applicable.
Competing interests
The authors report no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Reed, M.K., Smith, K.R., Ciocco, F. et al. Sorting through life: evaluating patient-important measures of success in a medication for opioid use disorder (MOUD) treatment program. Subst Abuse Treat Prev Policy 18, 4 (2023). https://doi.org/10.1186/s13011-022-00510-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13011-022-00510-1