
Abstract
Background
Electromyography (EMG) is a classical technique used to record electrical activity associated with muscle contraction and is widely applied in Biomechanics, Biomedical Engineering, Neuroscience and Rehabilitation Robotics. Determining muscle activation onset timing, which can be used to infer movement intention and trigger prostheses and robotic exoskeletons, is still a big challenge. The main goal of this paper was to perform a review of the state-of-the-art of EMG onset detection methods. Moreover, we compared the performance of the most commonly used methods on experimental EMG data.
Methods
A total of 156 papers published until March 2022 were included in the review. The papers were analyzed in terms of application domain, pre-processing method and EMG onset detection method. The three most commonly used methods [Single (ST), Double (DT) and Adaptive Threshold (AT)] were applied offline on experimental intramuscular and surface EMG signals obtained during contractions of ankle and knee joint muscles.
Results
Threshold-based methods are still the most commonly used to detect EMG onset. Compared to ST and AT, DT required more processing time and, therefore, increased onset timing detection, when applied on experimental data. The accuracy of these three methods was high (maximum error detection rate of 7.3%), demonstrating their ability to automatically detect the onset of muscle activity. Recently, other studies have tested different methods (especially Machine Learning based) to determine muscle activation onset offline, reporting promising results.
Conclusions
This study organized and classified the existing EMG onset detection methods to create consensus towards a possible standardized method for EMG onset detection, which would also allow more reproducibility across studies. The three most commonly used methods (ST, DT and AT) proved to be accurate, while ST and AT were faster in terms of EMG onset detection time, especially when applied on intramuscular EMG data. These are important features towards movement intention identification, especially in real-time applications. Machine Learning methods have received increased attention as an alternative to detect muscle activation onset. However, although several methods have shown their capability offline, more research is required to address their full potential towards real-time applications, namely to infer movement intention.
Similar content being viewed by others


Background
Electromyography (EMG) has been used as an interface tool for human-robot interaction and rehabilitation systems [1]. In fact, EMG is a relevant biological signal to inform on the motion onset of the user and can be applied in different applications such as the control of robotic devices in rehabilitation, kinesiology, biomechanics and motor control during several movements of the upper and lower extremities [2,3,4,5,6,7].
Muscle activation can be defined as the degree to which a muscle is excited, encompassing both the number of activated muscle fibers and the rate of their discharge [8]. Therefore, muscle activation onset, which is commonly estimated from EMG, is a physiological variable related to the beginning of contraction of a given muscle. As there is a latency between the onset time and the final movement that involves action on tendons and bones, there is a time window after detecting movement intention that allows actuation and control of wearable robots such as an exoskeleton. Therefore, accurate and fast detection of muscle onset time can potentially be used to identify movement intention [2, 9] and assist the user in real time.
The first method applied to detect muscle onset was the offline visual inspection by a trained user [10]. Although it is a subjective approach, visual inspection can be considered to provide accurate EMG onset detection values [10, 11]. On the other hand, visual inspection lacks reproducibility and can hardly be used in real-time applications [10]. In this context, computerized methods started to be developed and applied, and are currently the main solution to detect EMG onset in robotics and neurofeedback fields.
Due to the stochastic nature of the EMG signal, detecting onset of muscle activation is a challenging task, especially when EMG signals are weak [12]. Furthermore, despite the extensive literature devoted to detection of muscle contraction episodes, there is not a gold standard approach yet [13] and there is a degree of disparity across studies with regard to the definitions and parameters applied in each algorithm. This leads to similar EMG onset detection methods, with different nomenclatures, making it difficult to identify the most appropriated method for a specific application [10, 11, 13].
Given the lack of agreement on a standardized method for EMG onset detection and its importance towards intuitive and natural EMG-based control systems, it is timely to explore methods for automatic EMG onset detection in this review and to compare the performance of some of the most commonly used ones towards online applications. Therefore, the main goal of this study was to review the state-of-the-art on EMG onset detection algorithms. This can boost the development of novel algorithms and finally create consensus towards a possible standardized method for EMG onset detection, which would also allow more reproducibility across studies. In fact, a recent international initiative called ’Consensus for experimental design in electromyography’ (CEDE project), which aims to guide decision-making in recording, analysis, and interpretation of EMG data has been carried out. Results of our study can feed the CEDE project, as this initiate encompasses definitions for terms used in the EMG literature, basic principles for recording and analyzing EMG and electrode selection [8, 14].
The second goal of our study was to evaluate the performance of the most commonly used onset detection methods [three threshold-based algorithms—single (ST), double (DT) and adaptive threshold (AT)] to determine muscle onset on experimental EMG data. This allowed us to to evaluate the potential of these methods towards the real-time control of wearable robots (e.g., robotic exoskeletons).
Literature review
This review was based on the papers retrieved from the Scopus database using the following query strings:
TITLE-ABS-KEY ((emg OR electromyograph*) AND (onset AND detection))
and
TITLE((emg OR electromyograph*) AND (onset OR muscle OR movement) AND (detection OR activation)).
The first search returned a total of 245 papers and the second search 171, for a total of 416 possible publications. This research considered papers published until March 2022.
We applied the following exclusion criteria for our review:
-
papers aiming at detecting muscle fatigue;
-
use of additional sensors (e.g., inertial measurement units).
A total of 156 full-text journal articles were selected for analysis. The papers were analysed in terms of their application domain, pre-processing method and EMG onset detection method.
In the application domain, papers were classified as follows: Robotics, Clinical, Research, and Others. Specifically, papers that used EMG onset detection in the robotics domain (e.g., to control a robotic device) were classified as Robotics. Papers that presented results on the application of EMG onset techniques for clinical purposes or in the clinical setting were defined as Clinical. Research papers were those that proposed and/or tested a new technique of EMG onset detection. The remaining papers were classified as Others.
Pre-processing methods used to improve the quality of EMG before the application of the onset method itself were also analyzed in detail. Each EMG onset detection method was included in one of the following categories: Visual Inspection, Threshold-based, Statistical, Machine Learning or Others.
Regarding the EMG source type, from the total of 156 full-text journal articles selected for the analysis, 15 of them used intramuscular electromyography (iEMG) signals as the EMG source type where to test the performance of their algorithms at, whereas 145 articles used surface electromyography (sEMG) as the main EMG source type. This means that 4 articles tested onset detection algorithms in both sEMG and iEMG.
Literature review results
Figure 1 presents the number of publications on EMG onset detection methods along the years. After analyzing all papers selected, the pre-processing and EMG onset detection categories were defined according to the methods used and their relevance in terms of papers in the literature that applied each of them.

Number of publications on EMG onset detection methods per year reviewed in this study (period: 1978–2022; total articles: 156)
Pre-processing methods
Pre-processing methods, used to improve the quality of EMG signals towards the extraction of meaningful information, usually add more computational time, which means a delay in real-time implementations. The pre-processing methods evaluated in this review were classified in the following categories: EMG Envelope, Teager-Kaiser Energy Operator (TKEO), Wavelet Transform and Others, which included those that did not fit in none of these categories. Different pre-processing methods were applied 90 times in the papers reviewed. Calculating the EMG envelope was the method most frequently used, followed by the TKEO method.
EMG envelope
According to the CEDE project, EMG envelope is a smooth curve that tracks changes in the amplitude of an EMG signal over time [8]. Calculating the EMG envelope is a pre-processing method that can be obtained in several ways, as shown in Fig. 2.

Comparison of the most common approaches to obtain the EMG envelope from the raw EMG signal
To obtain the EMG envelope from raw signals, two main options are available: (1) low-pass filtering of the rectified signal; (2) root-mean-square (RMS) on raw EMG signal.
Low-pass filtering of the rectified signal One of the most common approaches to calculate the EMG envelope is to use a discrete version of traditional low-pass filters such as Butterworth or Chebyshev on the rectified EMG signal (obtained by computing the absolute value of the raw signal).. These filters can be considered as Infinite Impulse Response filters [15]. This approach was applied in: [16,17,18,19,20,21,22,23,24,25,26], with the Butterworth being the most predominant filter used.
Moving average (MA) According to the CEDE project, MA is defined as a method to smooth EMG data, that acts as a low-pass filter, reducing random fluctuations in the rectified or squared EMG signal [8].
This method was first used in the context of EMG onset detection by Maple-Horvart and Gilbey in 1992 [27]. After that, MA was applied to calculate EMG envelopes for EMG onset detection in several other papers: [13, 28,29,30,31,32,33,34,35,36,37,38,39,40,41].
The MA is calculated with a series of averages from successive segments, with or without overlap** windows. The consequence of its use is the attenuation of rapid variations through local averaging, but retention of slow variations [28], smoothing the signal and acquiring its envelope.
Root-mean-square (RMS) on raw EMG signal This approach ([28, 33, 42,43,44,45,46,47,48,49,50,51]) computes the RMS value of the signal within a window that “moves” across the raw EMG signal.
The RMS value measures the square root of the signal’s power. Therefore, it has a physical meaning. RMS is useful in many other applications [42]. EMG envelopes can be calculated from the RMS according to Eq. 1.
where \(x_{i}\) is the EMG value in the \(i^{th}\) sample and N is the number of samples.
Teager–Kaiser energy operator (TKEO)
The TKE operator method ([17, 25, 38,39,40, 48, 63,64,65,66,67]) was first proposed by Teager in 1982 [68,69,70]. The results obtained in these studies suggested that the production of speech involved nonlinear processes. As a result, Teager derived the TKE operator in the discrete-time domain to compute the energy of a sound. This method has been extended to cover other continuous signals such as EMG [53].
The discrete TKE operator \(\psi\) is defined in the time domain as:
where n is the sequence index and x the raw EMG signal. Considering a signal defined by Eq. 3:
where A is the amplitude, \(\omega _{0}(n)\) is the angular frequency, and \(\theta\) is the initial phase, the energy operator can be rewritten as defined in Eq. 4:
Equation 4 shows that the TKEO is proportional to the instantaneous amplitude (A) and frequency (\(\omega _{0}\)) of the input signal. Therefore, TKEO is usually applied on EMG signals to extract motor unit activity by making the action potential spikes sharper and narrower, enhancing the muscle activation points [53].
Several studies have demonstrated that pre-processing using TKEO can improve the EMG onset detection with respect to different pre-processing methods [17, 81,82], the Kalman filter [83], the Morphological Close Operator [38, 55], the Morphological Open Operator [38], the Multi Objective Optimization Genetic Algorithm [84], the Adaptative Linear Energy Detector [85], the use of an statistical criterion based on the amplitude distribution of EMG signal [86], the Constant False Alarm Rate method [87] and the Empirical Mode Decomposition [82].
EMG onset detection methods
EMG onset detection methods are those that, when applied to the EMG signal (raw or pre-processed signal), allow the identification of the beginning of muscle activation. In the pasts, the onset of muscle activation could be detected using mainly the following methods: Visual inspection, Threshold-based and Statistical. Recently, other studies have tested different methods (especially Machine Learning based) to determine muscle activation onset, reporting promising results. In our study, all EMG onset detection methods that do not fit into none of the previously mentioned categories were classified as ”Other EMG onset Detection Methods”. Figure 3 shows the number of papers that applied each of these categories within each different application domain (Robotics, Clinical, Research and Others). EMG onset detection has been applied in the application domain ’Research’ more than in all the other domains together.

Number of publications included in each of the different EMG onset detection categories (Visual inspection—black; Threshold—light gray; Statistical—dashed grey; Machine Learning—bold gray squares; and Others—dashed bold gray) within each different application domain. Application domains considered were Robotics, Clinical, Research and Others
Visual inspection
Visual inspection entails subjectivity and needs to be performed by an expert. There are no criteria established on how to carry out the visual inspection technique, although it is usually employed to detect the earliest rise in EMG activity above the steady-state (i.e., basal activity) [50, 88,89,90,91,92,93,94].
Despite being a subjective technique, visual inspection can be used to validate automatic EMG onset detection methods, serving as a gold-standard to develop computerized EMG onset detection methods. The visual detection of EMG onset has been widely referred in the literature: [11, 17, 21, 24,25,26, 32, 33, 36, 43, 49, 52, 57, 60, 60, 73, 95,96,97,98,99,100,101,102].
Threshold-based methods
The label ’THRESHOLD’ in Fig. 3 encompasses the use of one or more threshold-based methods, which are thoroughly described in this section, in each of the papers analyzed in this review. Threshold-based are the most common EMG onset detection methods found in the literature, being tested 253 times across the 156 papers analyzed (i.e., several papers tested and/or compared more than one different method based on EMG threshold).
In this approach, one attributes a threshold to discriminate between baseline activity and muscle activation. Thresholding is widely used due to its simplicity, speed and reliability. The simplicity of thresholding lies in its straightforward implementation. Additionally, thresholding is computationally efficient, making it suitable for real-time analysis of EMG signals and handling large datasets. Regarding its reliability, thresholding is a robust method that has been used in numerous studies in the literature. Although thresholding may not always provide the most accurate detection of EMG onset, it remains a popular choice in EMG signal processing. Nonetheless, there is lack of agreement among researchers on a standardized threshold method for EMG onset detection [46].
Cavanagh et al. were the first to propose the use of a threshold-based method [103]: authors investigated the dependence of electromechanical delay in the human elbow flexor group upon selected initial conditions at the time of muscle activation. Most common strategies followed to set threshold values are based on the baseline amplitude characteristics of the EMG signal, such as the mean or standard deviation. Some researchers name this strategy as the Shewhart protocol [16, 30, 104].
Some of the signal characteristics that can be considered to select the threshold are the following:
-
Standard Deviation (SD);
-
Period of time;
-
% Maximum Voluntary Contraction;
-
% Maximum EMG Amplitude.
Threshold-based methods can be classified in three different categories: Single Threshold (ST), Double Threshold (DT) and Adaptive Threshold (AT).
Single threshold (ST) ST method is the most predominant EMG onset detection method found in the literature: [2, 11, 13, 16,17,18,19, 22,23,24, 27, 29,30,31,32, 35,36,37,38,39,40,41, 43, 45,46,47,48, 51,63, 66, 67, 74, 77, 81,82,83,84, 86, 95, 96, 99, 103, 105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133].
ST compares the amplitude of the EMG signal (raw or EMG envelope) with a previously selected threshold. The onset is detected when the EMG amplitude is bigger than the threshold.
This method can be considered the most intuitive and standard computer-based method of time-locating the onset of muscle contraction activity [2].
ST can be useful to overcome some of the problems related to visual inspection. However, results of applying ST strongly depend on the choice of the threshold [134], which can lead to false positives in noisy signals. In theses cases, it is advisable to work on the EMG envelope, which smooths the signal and improves the onset detection.
Double threshold (DT): The DT method was applied in the following studies: [2, 10, 19,20,21, 24, 33, 34, 42, 51, 55, 65, 73, 82, 83, 87, 94, 95, 100, 115, 119,120,121, 123, 127, 128, 135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151].
To overcome some of the problems associated with ST, Lidierth et al. introduced the DT method in 1986 [135]. This method adds a second threshold to determine the muscle activation onset time, with the final goal of avoiding false positives and enhance EMG onset detection precision. A common strategy when applying DT method is to define an amplitude threshold, similar to what is done in ST. If the signal amplitude is higher than this threshold for a certain amount of time or samples (second threshold), then muscle activation is detected with DT. Due to the stochastic characteristics of the EMG signal, it is normally necessary to use a pre-processing method to obtain the signal envelope and then apply the second threshold.
Adaptive threshold (AT) The AT method can be applied directly on the raw EMG signal. AT segments the signal using the signal-to-noise (SNR) [61] or the energy value [85] to adapt the threshold of muscle activation by windows. As the SNR is the relative power of wanted EMG to unwanted signal components that are contained in the overall signal [8], this threshold method can be considered as an improvement of ST method, as it adapts its threshold value according to the EMG window being analyzed, which might enable a more precise EMG onset detection over time. AT was applied in the following works: [11, 52, 54, 55, 85, 97, 118, 121, 152,153,154,155,156].
Statistical methods
The onset of muscle activation can be detected by evaluating the statistical properties of the EMG signal before and after a possible change in model parameters [115]. Two main statistical approaches can be identified in the literature: the Approximated Generalized Likelihood Ratio (AGLR) and the Cumulative Sum (CUSUM).
Approximated generalized likelihood ratio (AGLR): The AGLR method was applied in the following publications: [10, 17, 37, 52, 57, 58, 67, 72, 77, 83, 93, 94, 100, 115, 121, 128, 157,158,159,160].
Sometimes also referred to as “Maximum Likelihood Estimator”, this method was first proposed as a change detection algorithm, with its first use in the context of muscle activity detection being presented in Hogan et al., in 1980 [157]. In short, the AGLR algorithm calculates an estimate of muscle activity as a function of the mean and variance of the activity level [121].
By using a log-likehood ratio test g(k) [66], the AGLR method detects if there is muscle contraction or not.
The log-likelihood ratio test is defined by the following equation:
where ln represents the natural logarithm, Y(n) represents the series of EMG samples, k the index of the product, r is the total length of the series, p1 and p0 represent the probability density function corresponding to the alternative hypothesis \(H_{1}\) (i.e., there are changes in the statistical properties of the EMG sequence) and the null hypothesis \(H_{0}\) (i.e., there are no changes in the statistical properties of the EMG sequence), respectively.
If the log-likelihood g(k) value is smaller than a pre-defined threshold, it indicates that the muscle is relaxed, whereas EMG onset is detected if g(k) value exceeds the threshold.
Cumulative sum (CUSUM): This method was used in: [67, 72, 95, 109]. CUSUM was first proposed by Ellaway in 1978 [161] with applications on the analysis of histograms.
The first study to propose the use of CUSUM to detect EMG onset was Chanaud et al., in 1991 [109], which used this method to determine how the different regions of the biceps femoris activated in a cat during a broad range of limb movements.
The CUSUM method works as follows [161]: a reference level (k), dependent on the task to be performed and selected in a previous training phase, is subtracted from each of the series of points on the signal (x1, x2, ..., xi, ..., Xn). The result of these subtractions, shown in Eq. 6, is a new series of points (Si) which are formed by adding up these differences consecutively.
The CUSUM chart is defined as the sequential plot of the values of Si, expressed by the Eq. 7:
The CUSUM technique has a smoothing action on the data [161] and the EMG onset detection is determined by a previous threshold, which can be defined by a training phase (see [72] for more details).
Other statistical methods Other statistical methods were also used in the following papers: [25, 49, 50, 60, 61, 75, 145, 147, 160, 162, 163].
Machine learning methods
Machine learning (ML), which is a discipline within the field of Artificial Intelligence, has recently gained increasing popularity due to the ability to extract patterns and information from complex and high-dimensional datasets. In the context of EMG onset detection, ML algorithms can automatically learn and adapt to the characteristics of the EMG signals, enabling the development of highly accurate and efficient detection methods. Machine learning-based algorithms were found in [33, 65, 164, 165].
Di Nardo et al. [165] evaluated a novel machine-learning-based approach (DEMANN) for detecting muscle activation onset/offset timing from sEMG signals. The study trained a neural network and evaluated DEMANN’s performance on simulated and real sEMG signals. DEMANN was validated against different reference algorithms, including the DT method. The study found that DEMANN provided a reliable prediction of muscle onset/offset and was minimally affected by SNR variability.
Trigili et al.[164] presented a ML-based algorithm able to detect users’ motion intention based on EMG signals and assessed its applicability towards the control of an upper-limb exoskeleton for people with severe arm disabilities. The algorithm was able to detect the onset of muscle activation before the actual movement, and its computational load was compatible with real-time applications. The study concluded that the proposed algorithm was promising for controlling upper-limb exoskeletons in real-time applications, and for assisting people with severe arm disabilities in performing functional tasks.
Dow et al. [33] presented the development of an algorithm to detect inspiratory events from EMG signals. A state-machine was utilized for classification and inspirations were detected with 98% accuracy in anesthetized and awake rats. The proposed algorithm can be explored in humans, as it may be useful for individuals requiring assisted ventilation.
Ghislieri et al. [65] introduced and validated a new approach to detect muscle activation intervals from sEMG signals using long short-term memory (LSTM) recurrent neural networks. The performance of the proposed LSTM-based muscle activity detector was compared with two other widely used approaches: TKEO and DT method. The study included simulated and real sEMG signals from healthy individuals, orthopedic patients, and neurological patients. Results showed that the LSTM outperformed the other approaches. The proposed algorithm overcomes the main limitations of other tested approaches and works directly on sEMG signals without the need for background-noise and SNR estimation.
Despite the growing interest in using ML techniques for EMG onset detection, there is currently no consensus on a reference method. As noted by Di Nardo et al. [165], a standardized approach for evaluating and comparing the performance of ML algorithms for EMG onset detection is still lacking. While several studies have proposed different ML approaches and achieved promising results, the absence of a reference method makes it challenging to classify these methods.
Other EMG onset detection methods
Other methods can be classified as: Energy-based methods [34, 85, 92], Entropy-based methods [12, 25, 38, 125, 146], Mathematical/numerical techniques [9, 16, 55, 166, 167], Computer Vision [127], Slope / discontinuities detectors [51, 62, 76] and External stimulation [168, 169].
Experimental protocol
The second goal of this study was to compare the performance of the three most commonly used methods for EMG onset detection, having in mind their potential towards online control of robotic exoskeletons for gait assistance or rehabilitation. As shown in Fig. 3, Threshold-based methods are the most commonly used in all application domains (Robotics, Clinical, Research and Others). For this reason, ST, DT and AT were tested on real data (iEMG and sEMG signals) obtained during motor tasks involving knee and ankle joints. This was done through simple tasks that could be used as a paradigm for comparison (such as knee and ankle flexion-extension), rather than gait, to minimize the influence of possible external factors (e.g., mechanical artifacts) on the evaluation of these methods. Furthermore, knee and ankle flexion-extension are important tasks during gait [170,171,172,173].
Participants
Three healthy subjects participated in this study. All procedures were approved by a local Ethics Committee (“Ethics Committee of Clinical Research with Medicines of the Hospital Complex of Toledo”), as well as by the Spanish Agency of Medicines and Medical Devices (AEMPS)—record 721/19/EC. All subjects volunteered to participate in the study, were informed about the procedures and possible adverse effects, and signed the informed consent to participate.
Data collection
EMG data were recorded while participants performed ankle dorsiflexion-plantarflexion and knee flexion-extension movements, using an EMG amplifier (Quattrocento, OT Bioelettronica, Torino, Italy) and a sampling frequency of 10,240 Hz. sEMG and iEMG were recorded from Tibialis Anterior (TA) and Vastus Lateralis (VL). For sEMG recordings, bipolar electrodes (Ag-AgCl, Ambu Neuroline 720, Ambu, Ballerup, Denmark) were used. For iEMG recordings, intramuscular thin wire electrodes (Fi-Wi2, Spes Medica, Genova, Italy) were used. More information on the protocol can be found in [174].
The selected number of muscles was kept to a minimum to simplify the procedure due to the invasiveness of the iEMG electrodes. On the other hand, testing the feasibility and performance of different threshold-based controllers can be carried out with such reduced number of EMG signals, as demonstrated in our previous study, where EMG-based controllers were used online to trigger the beginning of walking steps while healthy volunteers walked with an exoskeleton [175]. And, finally, these two muscles have an important role during gait [174].
Data processing
EMG onset was automatically detected offline using each of the three threshold-based methods (ST, DT and AT) on the EMG data recorded from each muscle (TA and VL) and participant, during knee and ankle flexion-extension trials. Threshold values were determined individually for each subject and task, and were based on the standard deviation (SD) of the baseline activity of each EMG recording through visual inspection.
Threshold values were defined between 1 and 3 times the SD of the EMG baseline, according to a training phase performed with each subject (see Table 1).
The DT method has to be performed on the EMG envelope due to the variation of the EMG amplitude over time (the second threshold). EMG envelopes were calculated using a Butterworth low-pass filter of second-order with a cut-off filter of 6 Hz [15]. The time required to ascertain muscle activation onset with DT method was 2.50 ms, i.e., EMG envelopes needed to stay above the first threshold for at least 2.5 ms in order for muscle activation to be detected offline.
The windows used in AT had a duration of 1/N of the total recording, where N is the number of movement cycles performed by the subject.
To analyze the performance of each method, the number of false/positive EMG onset detection events, the detection time and the processing time of each method were compared. The analysis of false positives/negatives was visually performed offline: any event labeled as the onset of EMG activation by a given method was considered as a false positive when an expert did not perceived it as a true onset of muscle activation; on the other hand, false negatives were those events labeled by an expert (offline, when assessing data visually) as an onset of muscle activation, but these were not detected by a given method. Furthermore, the difference between the onset timing calculated by each threshold-based method and the visual inspection (which was used as reference) was calculated for each cycle, task and subject. The mean difference was calculated for each method and subject. For this step, the first and last cycle of movement in both knee and ankle task performance were not considered, to exclude possible transients in the signal. Processing times required by each method were also calculated.
Results
The mean processing times needed by the computer (2,7 GHz Intel Core i7 processor) to compute the three threshold-based methods (ST, DT and AT), for each cycle of movement, are shown in Table 2.
DT method required more processing time (almost 10 times more) than the other two methods. The lengthy process required by DT to calculate EMG oset is due to the use of a pre-processing method (EMG envelope).
ST and DT methods obtained one false positive in a total of 124 cycles, which corresponds to 0.8% of detection error. AT obtained 9 false positives, which corresponds to a 7.3% of error detection. Table 3 represents the performance of the different threshold-based algorithms. This was done by assessing the mean time differences that each automatic method needed to detect muscle activation onset from both sEMG and iEMG signals, compared to the visual inspection.
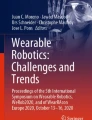
Considering the global performance of each threshold-based method, higher time precision was achieved using AT, which detected the onset of muscle activation, on average, 0.30 s after the visual inspection. ST and DT detected activation onset, on average, 0.33 s and 0.43 s after the visual inspection, respectively. Figure 4 shows an example of the detection timing for each of the three threshold-based methods assessed, which were applied on iEMG data from TA during one cycle of ankle dorsiflexion-plantarflexion task. Although the iEMG presented in Fig. 4 is very selective and presents clear individual action potentials, the iEMG signal was not always detected at the level of individual motor units, making a signal decomposition into individual motor unit action potentials not a viable option.

Individual example of EMG onset detection using four different methods (visual inspection (dashed line), ST (dotted line), DT (spaced dotted line) and AT (bold)) on iEMG recordings from Tibialis Anterior (TA) during ankle flexion-extension. Methods were applied offline. ST—Single Threshold. DT—Double Threshold. AT—Adaptive Threshold
Table 4 presents differences in terms of detection times when applying each of the threshold-based methods on sEMG and iEMG recordings. Muscle activation onset was detected before in iEMG signals for all subjects, using the three threshold-based methods, with the exception of DT in subject 02. On average, ST, DT and AT methods detected muscle activation 0.17, 0.02 and 0.16 s before in iEMG than in sEMG recordings, respectively.
Discussion
EMG has been increasingly applied in the research field as part of intuitive and natural control in human-robot interaction and rehabilitation systems for restoration of human movement and control of external devices from recordings of neural activity. One key component of these systems is the detection of movement intention (i.e., the onset of muscle activity). Given the lack of agreement on a standardized method for EMG onset detection and its importance towards intuitive and natural EMG-based control systems, it is timely to explore methods for automatic EMG onset detection. The first goal of our study was to review the state-of-the-art on EMG onset detection algorithms.
A total of 156 papers published until March 2022 were included in the review. The papers were analyzed in terms of application domain, pre-processing method and EMG onset detection method.
Regarding the application domain, EMG onset detection has been applied in the ’Research’ field more than in all the other domains together (i.e., Robotics, Clinical and others). This highlights the need of a standardized method for EMG onset detection, which may boost the translation from bench to bedside so that the onset of muscle activity could be used in more Clinical and Robotics applications, for example.
A total of 40% of all papers reviewed used a pre-processing technique before applying an onset detection method. Fast computational pre-processing methods are important to improve the quality of the EMG signal towards the extraction of information related with movement intention. EMG envelope was the most frequently applied pre-processing method across the reviewed papers. Although other authors have considered the EMG envelope and the TKEO as EMG onset detection methods [60], we have classified them as pre-processing methods, as previously done by others [53].
Threshold-based methods were found to be the most commonly used methods for EMG onset detection, for all application domains. Thresholding is a widely used method for detecting EMG onset due to its simplicity, speed and reliability. Recently, other studies have tested different methods (especially Machine Learning - ML - based) as an alternative to detect muscle activation onset, reporting promising results. One of the main advantages of ML-based methods is their ability to learn patterns from a dataset without the need for explicit feature extraction, which can otherwise be difficult and time-consuming. This can lead to more robust and generalizable models that can be applied to a wider range of datasets. Additionally, ML algorithms can adapt to changes in the data over time, allowing for the development of more adaptive and personalized systems. There are, on the other hand, some limitations of ML-based methods. One potential concern is the risk of overfitting, where the algorithm may learn the specific characteristics of the training data notably that it prevents it to generalize well to new data. This can, however, be mitigated through the use of appropriate validation methods and careful selection of training data. Additionally, ML-based methods can be computationally expensive and may require significant amounts of data to train. In this sense, more research is required to address the full potential of ML towards real-time applications, namely to infer movement intention.
We consider that our study fills a gap in the literature by providing a comprehensive classification framework for EMG onset detection methods. This framework not only enables a better understanding of the existing methods but also offers a practical tool for researchers and practitioners to easily navigate the field and select appropriate techniques for their specific requirements. This can also boost the development of novel algorithms and finally create consensus towards a possible standardized method, which would also allow more reproducibility across studies. Previously, 19 papers reviewed onset detection methods [10, 11, 19, 34, 36, 49, 53, 54, 57, 60, 71, 77, 83, 95, 96, 115, 119, 121, 128], although none of them has performed an extensive classification and definition of the available methods. From these 19 papers, only 3 of them had the review of onset detection methods as their main goal [10, 54, 115].
The second goal of our study was to evaluate the performance of the most commonly used onset detection methods (single (ST), double (DT) and adaptive threshold (AT)) to determine muscle onset on experimental EMG data (sEMG and iEMG). This allowed us to evaluate the potential of these methods towards the real-time control of wearable robots (e.g., robotic exoskeletons).
ST was the fastest of the three threshold-based methods to calculate EMG onset both in iEMG and sEMG data. This result can be explained by the low computational processing complexity required by ST, as well as the unnecessary employment of pre-processing methods, i.e., it can be applied on raw EMG data. On the other hand, ST is less precise than the other two threshold-based methods, as it uses a fixed threshold for the entire EMG signal. This can increase the number of false positives/negatives in terms of onset detection events. In that case, the use of TKEO as a pre-processing method can improve the accuracy of onset detection compared to ST alone [71]. Taking into account the advantages and disadvantages of ST, we consider that ST suits simple tasks (such as EMG-based static rehabilitation) best, where a fast response of the system is more important than its precision, and false negatives/positives do not mean security problems to the user.
DT was the slowest of the three methods to calculate EMG onset. This is due to the need of calculating EMG envelope (in addition to the second threshold), which adds more processing time and, thus, can compromise its use in real-time applications, especially when a fast detection is required. DT is more precise that ST to calculate EMG onset, as it uses two different thresholds (amplitude andd time) to detect the onset of the muscle activation. Therefore, it can be a robust solution to process EMG recordings offline [19].
Considering the global performance of each threshold-based method, higher time precision was achieved using AT, which detected the onset of muscle activation, on average, 0.30 s after the visual inspection. AT adapts the threshold of onset detection by segmenting the whole signal into small windows, allowing a more precise detection of muscle activation. AT can be a good option for real-time applications that need more precision and relatively fast processing times in terms of detection of muscle activation [153].
In summary, the choice of the most appropriate EMG onset detection method depends on the type of application and its requirements. A trade-off between processing speed, accuracy and time precision should be taken into account before defining which onset method best fits the application in question.
Muscle activation onset was detected before in iEMG signals for all subjects, using the three threshold-based methods, with the exception of DT in subject 02. Given that early detection of muscle contraction can be critical for real-time applications, iEMG signals should also be considered as an alternative to be used as input for human–machine interfaces [9], e.g., for the intuitive control of robotic exoskeletons, where timing is crucial for an efficient control strategy. Additionally, iEMG signals present higher SNR and less cross-talk, when compared with sEMG signals [174].
Conclusions
EMG can be used to infer movement intention and trigger exoskeletons and prostheses. However, determining the onset of muscle activation from EMG activity is not a trivial task. The first conclusion of this paper is that there is still no agreement on a standardized method for EMG onset detection (neither offline nor online), which hinders reproducibility across studies. Therefore, this study organized and classified the existing EMG onset detection methods in an attempt to bring additional interest to the field and create consensus towards a possible standardized method for EMG onset detection, which would also allow more reproducibility across studies. Despite the lack of standardized methods, the research interest has been growing along the years, with a soaring number of publications in the field.
A total of 156 papers published until March 2022 were analyzed in terms of application domain (Robotics, Clinical, Research and Others), pre-processing method and EMG onset detection method. Pre-processing methods are used to improve EMG quality towards the extraction of meaningful information, although this adds more computational time and might be a drawback towards real-time applications. EMG envelope, which represents the average activation of the EMG signal, was found to be the most used pre-processing method before applying algorithms aiming at detecting onset of muscle activity.
Threshold-based methods were found to be the most commonly used methods for EMG onset detection. On the other hand, Machine Learning (ML) methods have recently received increased attention as an alternative to detect muscle activation onset, reporting promising results. However, more research is required to address the full potential of ML towards real-time applications, namely to infer movement intention.
This study also evaluated the performance of the most commonly used onset detection detection methods (single (ST), double (DT) and adaptive threshold (AT)) to determine muscle onset on experimental EMG data. This allowed us to to evaluate the potential of these methods towards the real-time control of wearable robots. Results showed that DT required more processing time, which led to increased average onset timing detection compared to the other two methods, while ST and AT were faster in terms of EMG onset detection time, especially when applied on iEMG data. These are very important features towards movement intention identification. In that sense, this opens the window to further explore these methods in real-time applications such as the intuitive control of exoskeletons. In any case, the choice of the most appropriate EMG onset detection method depends on the type of application and its requirements. A trade-off between processing speed, accuracy and time precision should be taken into account before defining which onset method best fits the application in question.
One limitation of this study is its reduced sample size (n = 3 healthy subjects), which affects the likelihood of obtaining statistical differences and, thus, the generalizability of the results. However, data collected served the purpose of achieving the secondary goal of this study, allowing us to assess the advantages and limitation of each of the most used methods for EMG onset detection.
Availability of data and materials
The datasets used and/or analyzed in this study are available from the corresponding author upon reasonable request
Abbreviations
- AGLR:
-
Approximated generalized likehood ratio
- AT:
-
Adaptive threshold
- CUSUM:
-
Sumulative sum
- DT:
-
Double threshold
- EMG:
-
Electromyography
- iEMG:
-
Intramuscular electromyography
- LSTM:
-
Long short-term memory
- MA:
-
Moving average
- ML:
-
Machine learning
- RMS:
-
Root-mean-square
- SD:
-
Standard deviation
- sEMG:
-
Surface electromyography
- SNR:
-
Signal-to-noise
- ST:
-
Single threshold
- TA:
-
Tibialis anterior
- TKEO:
-
Teager–Kaiser energy operator
- VL:
-
Vastus lateralis
- WT:
-
Wavelet transform
References
Fukuda O, Tsuji T, Kaneko M, Otsuka A. A human-assisting manipulator teleoperated by EMG signals and arm motions. IEEE Trans Robot Autom. 2003;19(2):210–22.
Micera S, Vannozzi G. Improving detection of muscle activation intervals. IEEE Eng Med Biol Mag. 2001;20(6):38–46.
Kirchner EA, Tabie M, Seeland A. Multimodal movement prediction—towards an individual assistance of patients. PLoS ONE. 2014;9(1): e85060.
Cavallaro EE, Rosen J, Perry JC, Burns S. Real-time myoprocessors for a neural controlled powered exoskeleton arm. IEEE Trans Biomed Eng. 2006;53(11):2387–96.
Benitez LMV, Will N, Tabie M, Schmidt S, Kirchner E, Albiez J. An EMG-based Assistive Orthosis for Upper Limb Rehabilitation. Proceedings of the International Conference on Biomedical Electronics and Devices (MHGInterf-2013). 2013;p. 323–328.
Vaca Benitez LM, Tabie M, Will N, Schmidt S, Jordan M, Kirchner EA. Exoskeleton technology in rehabilitation: Towards an EMG-based orthosis system for upper limb neuromotor rehabilitation. Journal of Robotics. 2013;2013.
Kiguchi K, Imada Y, Liyanage M. EMG-based neuro-fuzzy control of a 4DOF upper-limb power-assist exoskeleton. Annual International Conference of the IEEE Engineering in Medicine and Biology—Proceedings. 2007;p. 3040–3043.
McManus L, Lowery M, Merletti R, Søgaard K, Besomi M, Clancy EA, et al. Consensus for experimental design in electromyography (CEDE) project: terminology matrix. J Electromyogr Kinesiol. 2021;59: 102565.
D’Anna C, Varrecchia T, Schmid M, Conforto S. Using the frequency signature to detect muscular activity in weak and noisy myoelectric signals. Biomed Signal Proc Control. 2019;52:69–76. https://doi.org/10.1016/j.bspc.2019.02.026.
Staude G, Wolf W. Objective motor response onset detection in surface myoelectric signals. Med Eng Phys. 1999;21(6–7):449–67.
Hodges PW, Bui BH. A comparison of computer-based methods for the determination of onset of muscle contraction using electromyography. Electroencephalogr Clin Neurophysiol. 1996;101:511–9.
Zhou P, Zhang X. A novel technique for muscle onset detection using surface EMG signals without removal of ECG artifacts. Physiol Meas. 2014;35(1):45–54.
Morantes G, Fernández G, Altuve M. A threshold-based approach for muscle contraction detection from surface EMG signals. IX Int Seminar Med Inf Proc Anal. 2013;8922:89220C.
Besomi M, Hodges PW, Van Dieën J, Carson RG, Clancy EA, Disselhorst-Klug C, et al. Consensus for experimental design in electromyography (CEDE) project: electrode selection matrix. J Electromyogr Kinesiol. 2019;10(48):128–44.
Rose W. Raw signal amplification-EMG analysis. Mathematics and Signal Processing for Biomechanics. 2014.
Allison GT. Trunk muscle onset detection technique for EMG signals with ECG artefact. J Electromyogr Kinesiol. 2003;13(3):209–16.
Solnik S, Rider P, Steinweg K, Devita P, Hortobágyi T. Teager-Kaiser energy operator signal conditioning improves EMG onset detection. Eur J Appl Physiol. 2010;110(3):489–98.
Sedlak J, Spulak D, Roman C, Kra B. Segmentation of Surface EMG Signals. In: International Conference on Applied Electronics. February 2016; 2013. p. 1–4.
Silva L, Marta S, Vaz J, Fernandes O, Castro MA, Pezarat-Correia P. Trunk muscle activation during golf swing: Baseline and threshold. J Electromyogr Kinesiol. 2013;23(5):1174–82.
Avila A, Chang JY. EMG onset detection and upper limb movements identification algorithm. Microsyst Technol. 2014;20(8–9):1635–40.
Begovic H, Zhou GQ, Li T, Wang Y, Zheng YP. Detection of the electromechanical delay and its components during voluntary isometric contraction of the quadriceps femoris muscle. Front Physiol. 2014;5:1–9.
Wentink EC, Schut VGH, Prinsen EC, Rietman JS, Veltink PH. Detection of the onset of gait initiation using kinematic sensors and EMG in transfemoral amputees. Gait Posture. 2014;39(1):391–6. https://doi.org/10.1016/j.gaitpost.2013.08.008.
Spulak D, Cmejla R, Bacakova R, Kracmar B, Satrapova L, Novotny P. Muscle activity detection in electromyograms recorded during periodic movements. Comput Biol Med. 2014;47(1):93–103.
Clair-Auger JM, Gan LS, Norton JA, Boliek CA. Simultaneous measurement of breathing kinematics and surface electromyography of chest wall muscles during maximum performance and speech tasks in children: methodological considerations. Folia Phoniatr Logop. 2016;67(4):202–11.
Tenan MS, Tweedell AJ, Haynes CA. Analysis of statistical and standard algorithms for detecting muscle onset with surface electromyography. J Appl Biomech. 2017;33(6):464–8.
Trinler U, Leboeuf F, Hollands K, Jones R, Baker R. Estimation of muscle activation during different walking speeds with two mathematical approaches compared to surface EMG. Gait Posture. 2018;64(July):266–73.
Marple-Horvat DE, Gilbey SL. A method for automatic identification of periods of muscular activity from EMG recordings. J Neurosci Methods. 1992;42(3):163–7.
Choi HG, Principe JC, Hutchison AA, Wozniak JA. Multiresolution segmentation of respiratory electromyographic signals. IEEE Trans Biomed Eng. 1994;41(3):257–66.
Leader JK, Boston JR, Moore CA. A data dependent computer algorithm for the detection of muscle activity onset and offset from EMG recordings. Electroencephalogr Clin Neurophysiol Electromyogr Motor Control. 1998;109(2):119–23.
Stokes IAF, Gardner-Morse M, Henry SM, Badger GJ. Decrease in trunk muscular response to perturbation with preactivation of lumbar spinal musculature. Spine. 2000;25(15):1957–64.
Kitsas IK, Hadjileontiadis LJ, Papakonstantinou IN, Kotzamanidis C. MYOS: an efficient multichannel EMG data acquisition and analysis system. In: Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No.03CH37439). IEEE; 2003. p. 3313–3316. Available from: http://ieeexplore.ieee.org/document/1280853/.
Biljan B, Potočanac Z, Cifrek M. Comparison of two muscle activity detection techniques from surface EMG signals applied to countermovement Jump. IFMBE Proc. 2011;37:834–7.
Dow DE, Petrilli AM, Mantilla CB, Zhan WZ, Sieck GC. Electromyogram-triggered inspiratory event detection algorithm. 6th International Conference on Soft Computing and Intelligent Systems, and 13th International Symposium on Advanced Intelligence Systems, SCIS/ISIS 2012. 2012;p. 789–794.
Rasool G, Iqbal K, White GA. Myoelectric activity detection during a Sit-to-Stand movement using threshold methods. Comput Math Appl. 2012;64(5):1473–83. https://doi.org/10.1016/j.camwa.2012.03.094.
Kanwade A, Bairagi VK. Classification of COPD and normal lung airways using feature extraction of electromyographic signals. J King Saud Univ Comput Inf Sci. 2016. https://doi.org/10.1016/j.jksuci.2017.05.006.
Tan ZX, Foong R, Ang KK. Determining mechanical and electromyographical reaction time in a BCI driving fatigue experiment. 2015 10th International Conference on Information, Communications and Signal Processing, ICICS 2015. 2016.
Hulsdunker T, Strüder HK, Mierau A. Neural correlates of expert visuomotor performance in badminton players. Med Sci Sports Exerc. 2016;48(11):2125–34.
Yang D, Zhang H, Gu Y, Liu H. Accurate EMG onset detection in pathological, weak and noisy myoelectric signals. Biomed Signal Proc Control. 2017;33:306–15. https://doi.org/10.1016/j.bspc.2016.12.014.
Zhang X, Li X, Samuel OW, Huang Z, Fang P, Li G. Improving the robustness of electromyogram-pattern recognition for prosthetic control by a postprocessing strategy. Front Neurorobotics. 2017;11:1–15.
Kanitz G, Cipriani C, Edin BB. Classification of transient myoelectric signals for the control of multi-grasp hand prostheses. IEEE Trans Neural Syst Rehabil Eng. 2018;26(9):1756–64.
Martinez IJR, Clemente F, Kanitz G, Mannini A, Sabatini AM, Cipriani C. Grasp Force Estimation from HD-EMG Recordings with Channel Selection Using Elastic Nets: Preliminary Study. Proceedings of the IEEE RAS and EMBS International Conference on Biomedical Robotics and Biomechatronics. 2018;2018:25–30.
Amon C, Marentakis G. Design and evaluation of an EMG-based recording and detection system. university of music and performing arts Graz; 2013.
Dieterich AV, Botter A, Vieira TM, Peolsson A, Petzke F, Davey P, et al. Spatial variation and inconsistency between estimates of onset of muscle activation from EMG and ultrasound. Sci Rep. 2017;7:1–11. https://doi.org/10.1038/srep42011.
El Falou W, Khalil M, Duchêne J. Adaptive approach for change detection in EMG recordings. Annu Int Conf IEEE Eng Med Biol-Proc. 2001;2:1875–8.
Fonda B, Panjan A, Markovic G, Sarabon N. Adjusted saddle position counteracts the modified muscle activation patterns during uphill cycling. J Electromyogr Kinesiol. 2011;21(5):854–60. https://doi.org/10.1016/j.jelekin.2011.05.010.
Ozgunen KT, Çelik U, Kurdak SS. Determination of an optimal threshold value for muscle activity detection in EMG analysis. J Sports Sci Med. 2010;9(4):620–8.
Pasinetti S, Lancini M, Bodini I, Docchio F. A novel algorithm for EMG signal processing and muscle timing measurement. IEEE Trans Instrum Meas. 2015;64(11):2995–3004.
Restrepo-Agudelo S, Roldan-Vasco S, Ramirez-Arbelaez L, Cadavid-Arboleda S, Perez-Giraldo E, Orozco-Duque A. Improving surface EMG burst detection in infrahyoid muscles during swallowing using digital filters and discrete wavelet analysis. J Electromyogr Kinesiol. 2017;35:1–8. https://doi.org/10.1016/j.jelekin.2017.05.001.
Soares SB, Coelho RR, Nadal J. The use of cross correlation function in onset detection of electromyographic signals. ISSNIP Biosignals and Biorobotics Conference, BRC. 2013.
Rodrigues A, Janssens L, Langer D, Matsumura U, Rozenberg D, Brochard L, et al. Semi-automated detection of the timing of respiratory muscle activity: validation and first application. Front Physiol. 2022. https://doi.org/10.3389/fphys.2021.794598/full.
Bairagi VK, Kanwade AB. Novel slope-based onset detection algorithm for electromyographical signals. Int J Biomed Eng Technol. 2021;36(4):311.
**aoyan Li, Aruin AS. Muscle Activity Onset Time Detection Using Teager-Kaiser Energy Operator. In: 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference. IEEE; 2005. p. 7549–7552. Available from: http://ieeexplore.ieee.org/document/1616259/.
Li X, Zhou P, Aruin AS. Teager-Kaiser energy operation of surface EMG improves muscle activity onset detection. Ann Biomed Eng. 2007;35(9):1532–8.
Tabie M, Kirchner EA. EMG Onset Detection—Comparison of Different Methods for a Movement Prediction Task based on EMG. In: In Proceedings of the 6th International Conference on Bio-inspired Systems and Signal Processing. August; 2013. p. 242–247.
Yang D, Huang Q, Yang W, Liu H. EMG Onset Detection Based on Teager–Kaiser Energy Operator and Morphological Close Operation. In: International Conference on Intelligent Robotics and Applications (ICIRA). vol. 8103; 2013. p. 257–268. Available from: http://springer.longhoe.net/10.1007/978-3-642-40849-6.
Bulea TC, Prasad S, Kilicarslan A, Contreras-Vidal JL. Sitting and standing intention can be decoded from scalp EEG recorded prior to movement execution. Front Neurosci. 2014;8:1–19.
Magda M, Carlsson B. EMG onset detection—development and comparison of algorithms. Blekinge Institute of Technology; 2015.
Krabben T, Prange GB, Kobus HJ, Rietman JS, Buurke JH. Application of the Teager–Kaiser energy operator in an autonomous burst detector to create onset and offset profiles of forearm muscles during reach-to-grasp movements. Acta Bioeng Biomech. 2016;18(4):135–44.
Roldan-vasco S, Perez-giraldo E, Orozco-Duque A. Continuous wavelet transform for muscle activity detection in surface EMG signals during swallowing. vol. 742. Springer International Publishing; 2017. Available from: http://springer.longhoe.net/10.1007/978-3-319-66963-2.
Tenan MS, Tweedell AJ, Haynes CA. Iterative assessment of statistically-oriented and standard algorithms for determining muscle onset with intramuscular electromyography. J Appl Biomech. 2017;33(6):464–8.
Bahadur R, Ur Rehman S, Rehman Su. A Robust and Adaptive Algorithm for Real-time Muscle Activity Interval Detection using EMG Signals. Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2018)—Volume 4: BIOSIGNALS. 2018;4(Biostec):89–96.
Bhardwaj S, Khan AA, Muzammil M. Onset difference between vastus lateralis and knee extension during sit to stand task. In: 1st international conference on manufacturing, material science and engineering (ICMMSE-2019); 2019. p. 020027.
Castillo-Escario Y, Rodriguez-Canon M, Garcia-Alias G, Jane R. Onset Detection to Study Muscle Activity in Reaching and Gras** Movements in Rats. In: 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). IEEE; 2019. p. 5113–5116. Available from: https://ieeexplore.ieee.org/document/8857200/.
Huang X, Wang H, **ao J, Automatic Zhao J, Detection of Muscle Mobilization Order in Sling Exercise Therapy. Proceedings, Chinese Automation Congress. CAC. 2018;2018(2019):810–4.
Ghislieri M, Cerone GL, Knaflitz M, Agostini V. Long short-term memory (LSTM) recurrent neural network for muscle activity detection. J NeuroEng Rehabil. 2021;18(1):153. https://doi.org/10.1186/s12984-021-00945-w.
Crotty ED, Furlong LAM, Hayes K, Harrison AJ. Onset detection in surface electromyographic signals across isometric explosive and ramped contractions: a comparison of computer-based methods. Physiol Meas. 2021;42(3).
Tigrini A, Mengarelli A, Cardarelli S, Fioretti S, Verdini F. Improving EMG signal change point detection for low SNR by using extended Teager-Kaiser energy operator. IEEE Trans Med Robot Bionics. 2020;2(4):661–9.
Teager H, Teager S. Phenomenological Model for Vowel Production. In: Speech Sciences: Recent Advances. College Hill Press; 1983. p. 73–109.
Teager HM, Teager SM. Evidence for Nonlinear Sound Production Mechanisms in the Vocal Tract. In: Speech Production and Speech Modelling. Dordrecht: Springer Netherlands; 1990. p. 241–261. Available from: http://springer.longhoe.net/10.1007/978-94-009-2037-8_10.
Kaiser JF. On a simple algorithm to calculate the ’energy’ of a signal. In: International Conference on Acoustics, Speech, and Signal Processing. IEEE; 1990. p. 381–384. Available from: http://ieeexplore.ieee.org/document/115702/.
Solnik S, DeVita P, Rider P, Long B, Hortobágyi T. Teager-Kaiser Operator improves the accuracy of EMG onset detection independent of signal-to-noise ratio. Acta Bioeng Biomech. 2008;10(2):65–8.
Khalil M, Duchêne J. Detection and classification of multiple events in piecewise stationary signals: comparison between autoregressive and multiscale approaches. Signal Process. 1999;75(3):239–51.
Lauer RT, Laughton CA, Orlin M, Smith BT. Wavelet decomposition for the identification of EMG activity in the gait cycle. Proceedings of the IEEE Annual Northeast Bioengineering Conference, NEBEC. 2003;2003:142–143.
Merlo A, Farina D, Merletti R. A fast and reliable technique for muscle activity detection from surface EMG signals. IEEE Trans Biomed Eng. 2003;50(3):316–23.
Journée HL, Postma AA, Sun M, Staal MJ. Detection of tremor bursts by a running second order moment function and analysis using interburst histograms. Med Eng Phys. 2008;30(1):75–83.
Vannozzi G, Conforto S, D’Alessio T. Automatic detection of surface EMG activation timing using a wavelet transform based method. J Electromyogr Kinesiol. 2010;20(4):767–72. https://doi.org/10.1016/j.jelekin.2010.02.007.
Santos BR, Larivière C, Delisle A, McFadden D, Plamondon A, Imbeau D. Sudden loading perturbation to determine the reflex response of different back muscles: a reliability study. Muscle Nerve. 2011;43(3):348–59.
Di Nardo F, Basili T, Meletani S, Scaradozzi D. Wavelet-based assessment of the muscle-activation frequency range by EMG analysis. IEEE Access. 2022;10:9793–805.
Phinyomark A, Limsakul C, Phukpattaranont P. Application of wavelet analysis in EMG feature extraction for pattern classification. Meas Sci Rev. 2011. https://doi.org/10.2478/v10048-011-0009-y.
Chen X, Wu Z, Huang NE. Detection technique of muscle activation intervals for sEMG signals based on the Empirical Mode Decomposition. Analysis. 2010;2(2):233–65.
Darvas F, Scherer R, Ojemann JG, Rao RP, Miller KJ, Sorensen LB. High gamma map** using EEG. NeuroImage. 2010;49(1):930–8. https://doi.org/10.1016/j.neuroimage.2009.08.041.
Junghoon Lee, Hyunchul Ko, Seunghwan Lee, Hyunsook Lee, Youngro Yoon. Detection technique of muscle activation intervals for sEMG signals based on the empirical mode decomposition. In: 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE; 2009. p. 336–339. Available from: http://ieeexplore.ieee.org/document/5333209/.
Lee AS, Cholewicki J, Peter RN. The effect of background muscle activity on computerized detection of sEMG onset and offset. J Biomech. 2007;40(15):3521–6.
Magda M, Martinez-Alvarez A, Cuenca-Asensi S. MOOGA Parameter Optimization for Onset Detection in EMG Signals. In: ICIAP Workshops. vol. 24. ICIAP Workshops; 2017. p. 171–180. https://doi.org/10.1007/978-3-319-70742-6_16.
Bengacemi H, Mesloub A, Ouldali A, Abed-Meraim K. Adaptive Linear Energy Detector based on onset and offset electromyography activity detection. 2017 6th International Conference on Systems and Control, ICSC 2017. 2017;p. 409–413.
Abbink JH, Van Der Bilt A, Van Der Glas HW. Detection of onset and termination of muscle activity in surface electromyograms. J Oral Rehabil. 1998;25(5):365–9.
Kontunen A, Rantanen V, Vehkaoja A, Ilves M, Lylykangas J, Mäkelä E, et al. Low-latency EMG Onset and Termination Detection for Facial Pacing. In: European Medical and Biological Engineering Conference Nordic-Baltic Conference on Biomedical Engineering and Medical Physics. vol. 65; 2018. p. 1016–1019.
Allum JHJ, Pfaltz CR. Visual and vestibular contributions to pitch sway stabilization in the ankle muscles of normals and patients with bilateral peripheral vestibular deficits. Exp Brain Res. 1985. https://doi.org/10.1007/BF00238956.
Crenna P, Frigo C, Massion J, Pedotti A. Forward and backward axial synergies in man. Exp Brain Res. 1987. https://doi.org/10.1007/BF00235977.
Woollacott MH, von Hosten C, Rösblad B. Relation between muscle response onset and body segmental movements during postural perturbations in humans. Exp Brain Res. 1988;72(3):593–604. https://doi.org/10.1007/BF00250604.
Inglis JT, Horak F, Shupert C, Jones-Rycewicz C. The importance of somatosensory information in triggering and scaling automatic postural responses in humans. Exp Brain Res. 1994. https://doi.org/10.1007/BF00243226.
Spasojevic S, Rodrigues A, Mahdaviani K, Reid WD, Mihailidis A, Khan SS. Onset and Offset Detection of Respiratory EMG Data Based on Energy Operator Signal. In: 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC). IEEE; 2021. p. 121–124. Available from: https://ieeexplore.ieee.org/document/9631101/.
Kowalski E, Catelli DS, Lamontagne M. Comparing the accuracy of visual and computerized onset detection methods on simulated electromyography signals with varying signal-to-noise ratios. J Funct Morphol Kinesiol. 2021;6(3):70.
Crotty ED, Furlong LAM, Hayes K, Harrison AJ. Onset detection in surface electromyographic signals across isometric explosive and ramped contractions: a comparison of computer-based methods. Physiol Meas. 2021;42(3): 035010. https://doi.org/10.1088/1361-6579/abef56.
Boxtel GJM, Geraats LHD, Berg-Lenssen MMC, Brunia CHM. Detection of EMG onset in ERP research. Psychophysiology. 1993;30(4):405–12. https://doi.org/10.1111/j.1469-8986.1993.tb02062.x.
Ym Wong. Recording the vastii muscle onset timing as a diagnostic parameter for patellofemoral pain syndrome: fact or fad? Phys Ther Sport. 2009;10(2):71–4. https://doi.org/10.1016/j.ptsp.2009.02.001.
Vaisman L, Zariffa J, Popovic MR. Application of singular spectrum-based change-point analysis to EMG-onset detection. J Electromyogr Kinesiol. 2010;20(4):750–60. https://doi.org/10.1016/j.jelekin.2010.02.010.
Klyne DM, Keays SL, Bullock-Saxton JE, Newcombe PA. The effect of anterior cruciate ligament rupture on the timing and amplitude of gastrocnemius muscle activation: a study of alterations in EMG measures and their relationship to knee joint stability. J Electromyogr Kinesiol. 2012;22(3):446–55. https://doi.org/10.1016/j.jelekin.2012.01.013.
Yaothak J, Phukpattaranont P, Wongkittisuksa B. Improvement in the algorithm for accurate detection of muscle activity from EMG. 5th 2012 Biomedical Engineering International Conference, BMEiCON 2012. 2012.
Jubany J, Angulo-Barroso R. An algorithm for detecting EMG onset/offset in trunk muscles during a reaction- stabilization test. J Back Musculoskelet Rehabil. 2016;29(2):219–30.
Williams SR, Chapman CE. Time course and magnitude of movement-related gating of tactile detection in humans. III. Effect of motor tasks. J Neurophysiol. 2017;88(4):1968–79.
Kusche R, Ryschka M. Combining bioimpedance and EMG measurements for reliable muscle contraction detection. IEEE Sens J. 2019;19(23):11687–96.
Cavanagh PR, Komi PV. Electromechanical delay in human skeletal muscle under concentric and eccentric contractions. Eur J Appl Physiol. 1979;42(3):159–63.
Vieira PM, Ferreira JF, Gomes PR, Lima CS. An adapted double threshold protocol for spastic muscles. In: 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). IEEE; 2016. p. 3630–3633. Available from: http://ieeexplore.ieee.org/document/7591514/.
Neafsey EJJ, Hull CDD, Buchwald NAA. Preparation for movement in the cat. II. Unit activity in the basal ganglia and thalamus. Electroencephalogr Clin Neurophysiol. 1978;44(6):714–23.
Nashner LM, Shumway-Cook A, Marin O. Stance posture control in select groups of children with cerebral palsy: deficits in sensory organization and muscular coordination. Exp Brain Res. 1983;49(3):393–409.
Greeley HP. Real-time detection of precise EMG onset for synchronisation of an EEG averager. Clin Phys Physiol Meas. 1984;5(1):13–9.
Haagh SAVM, Spijkers WAC, van den Boogaart B, van Boxtel A. Fractioned reaction time as a function of response force. Acta Physiol (Oxf). 1987;66(1):21–35.
Chanaud CM, Macpherson JM. Functionally complex muscles of the cat hindlimb—III. Differential activation within biceps femoris during postural perturbations. Exp Brain Res. 1991;85(2):271–80.
Bullock-Saxton JE. Local sensation changes and altered hip muscle function following severe ankle sprain. Phys Ther. 1994;74(1):17–28.
Latwesen A, Patterson PE. Identification of lower arm motions using the EMG signals of shoulder muscles. Med Eng Phys. 1994;16(2):113–21.
Thexton AJ. A randomisation method for discriminating between signal and noise in recordings of rhythmic electromyographic activity. J Neurosci Methods. 1996;66(2):93–8.
Hodges PW, Richardson CA. Delayed postural contraction of transversus abdominis in low back pain associated with movement of the lower limb. J Spinal Disord. 1998;11(1):46–56.
Radebold A, Cholewicki J, Panjabi MM, Patel TC. Muscle response pattern to sudden trunk loading in healthy individuals and in patients with chronic low back pain. Spine. 2000;25(8):947–54.
Staude G, Flachenecker C, Daumer M, Wolf W. Onset detection in surface electromyographic signals: a systematic comparison of methods. J Appl Signal Proc. 2001;2:67–81.
Skotte J, Hjortskov N, Essendrop M, Schibye B, Fallentin N. Short latency stretch reflex in human lumbar paraspinal muscles. J Neurosci Methods. 2005;145(1–2):145–50.
Belavý DL, Wilson SJ, Richardson CA. Quantification of the timing of continuous modulated muscle activity in a repetitive-movement task. Physiol Meas. 2006;27(11).
Zhang X, Wang X, Wang B, Sugi T, Nakamura M. Real-time control strategy for EMG-drive meal assistance robot — my spoon. In: 2008 International Conference on Control, Automation and Systems. 1. IEEE; 2008. p. 800–803. Available from: http://ieeexplore.ieee.org/document/4694607/.
Choi B, Kim M, Jeon HS. The effects of an isometric knee extension with hip adduction (KEWHA) exercise on selective VMO muscle strengthening. J Electromyogr Kinesiol. 2011;21(6):1011–6. https://doi.org/10.1016/j.jelekin.2011.08.008.
De Marchis C, Conforto S, Severini G, Schmid M, D’Alessio T. Detection of tremor bursts from the sEMG Signal: An optimization procedure for different detection methods. In: 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society. 1. IEEE; 2011. p. 7508–7511. Available from: http://ieeexplore.ieee.org/document/6091851/.
Navallas J, Ariz M, Villanueva A, San Agustn J, Cabeza R. Optimizing interoperability between video-oculographic and electromyographic systems. J Rehabil Res Dev. 2011;48(3):253.
Opisso E, Borau A, Rijkhoff NJM. Urethral sphincter EMG-controlled dorsal penile/clitoral nerve stimulation to treat neurogenic detrusor overactivity. J Neural Eng. 2011;8(3).
De Marchis C, Schmid M, Conforto S. An optimized method for tremor detection and temporal tracking through repeated second order moment calculations on the surface EMG signal. Med Eng Phys. 2012;34(9):1268–77. https://doi.org/10.1016/j.medengphy.2011.12.017.
Park SY, Lee SY, Kang HC, Kim SM. EMG analysis of lower limb muscle activation pattern during pedaling: experiments and computer simulations. Int J Precision Eng Manuf. 2012;13(4):601–8. https://doi.org/10.1007/s12541-012-0077-4.
Zhang X, Zhou P. Sample entropy analysis of surface EMG for improved muscle activity onset detection against spurious background spikes. J Electromyogr Kinesiol. 2012;22(6):901–7. https://doi.org/10.1016/j.jelekin.2012.06.005.
Jahanmiri-Nezhad F, Li X, Barkhaus PE, Rymer WZ, Zhou P. A clinically applicable approach for detecting spontaneous action potential spikes in amyotrophic lateral sclerosis with a linear electrode array. J Clin Neurophysiol. 2014;31(1):35–40.
McCool P, Chatlani N, Petropoulakis L, Soraghan JJ, Menon R, Lakany H. Lower arm electromyography (EMG) activity detection using local binary patterns. IEEE Trans Neural Syst Rehabil Eng. 2014;22(5):1003–12.
Kosaki T, Atsuumi K, Takahashi Y, Li S. A pneumatic arm power-assist system prototype with EMG-based muscle activity detection. 2017 IEEE International Conference on Mechatronics and Automation, ICMA 2017. 2017;p. 793–798.
Zibrandtsen IC, Kidmose P, Kjaer TW. Detection of generalized tonic-clonic seizures from ear-EEG based on EMG analysis. Seizure. 2018;59:54–9. https://doi.org/10.1016/j.seizure.2018.05.001.
Woods S, Dotan R, Jenicek N, Maynard J, Gabriel D, Tokuno C, et al. Isometric-based test improves EMG-threshold determination in boys vs. men. Eur J Appl Physiol. 2019;119(9):1971–9. https://doi.org/10.1007/s00421-019-04185-8.
Guerrero JA, Macías-Díaz JE. A threshold selection criterion based on the number of runs for the detection of bursts in EMG signals. Biomed Signal Proc Control. 2020;57: 101699.
Fernández García JM, Carvalho CR, Barroso FO, Moreno JC. Pseudo-online Muscle Onset Detection Algorithm with Threshold Auto-Adjustment for Lower Limb Exoskeleton Control. In: Wearable Robotics: Challenges and Trends. WeRob 2020. Biosystems & Biorobotics. Springer, Cham; 2022. p. 275–279. Available from: https://springer.longhoe.net/10.1007/978-3-030-69547-7_45.
Lee K. EMG-triggered pedaling training on muscle activation, gait, and motor function for stroke patients. Brain Sci. 2022;12(1):76.
Raez MBI, Hussain MS, Mohd-Yasin F. Techniques of EMG signal analysis: detection, processing, classification and applications. Biol Proc Online. 2006;8(1):11–35.
Lidierth M. A computer based method for automated measurement of the periods of muscular activity from an EMG and its application to locomotor EMGs. Electroencephalogr Clin Neurophysiol. 1986;64(4):378–80.
Di Fabio RP. Reliability of computerized surface electromyography for determining the onset of muscle activity. Phys Therapy. 1987;67(1):43–8.
Lee WA, Buchanan TS, Rogers MW. Effects of arm acceleration and behavioral conditions on the organization of postural adjustments during arm flexion. Exp Brain Res. 1987;66(2):257–70.
Studenski S, Duncan PW, Chandler J. Postural responses and effector factors in persons with unexplained falls: results and methodologic issues. J Am Geriatr Soc. 1991;39(3):229–34. https://doi.org/10.1111/j.1532-5415.1991.tb01642.x.
Bullock-Saxton JE, Janda V, Bullock MI. Reflex activation of gluteal muscles in walking. Spine. 1993;18(6):704–8.
Hudgins B, Parker P, Scott RN. A new strategy for multifunction myoelectric control. IEEE Trans Biomed Eng. 1993;40(1):82–94.
Thompson HW, McKinley PA. Landing from a jump: the role of vision when landing from known and unknown heights. NeuroReport. 1995;6(3):581–4.
Karst GM, Willett GM. Onset timing of electromyographic activity in the vastus medialis oblique and vastus lateralis muscles in subjects with and without patellofemoral pain syndrome. Phys Therapy. 1995;75(9):813–23.
Bonato P, D’Alessio T, Knaflitz M. A statistical method for the measurement of muscle activation intervals from surface myoelectric signal during gait. IEEE Trans Biomed Eng. 1998;45(3):287–99.
Lee JH, Shim H, Lee HS, Lee YH, Yoon YR. Detection of onset and offset time of muscle activity in surface EMGs using the Kalman smoother. IFMBE Proc. 2007;14(1):1103–6.
Rasool G, Bouaynaya N, Iqbal K. Muscle activity detection from myoelectric signals based on the ar-garch model. In: Statistical Signal Processing Workshop (SSP); 2012. p. 420–423.
Lyu M, **ong C, Zhang Q, He L. Fuzzy Entropy-Based Muscle Onset Detection Using Electromyography (EMG). In: International Conference on Intelligent Robotics and Applications; 2014. p. 89–98. Available from: http://springer.longhoe.net/10.1007/978-3-319-13966-1_9.
Liu J, Ying D, Rymer W, Zhou P. Robust muscle activity onset detection using an unsupervised electromyogram learning framework. PLoS ONE. 2015;10(6):1–15.
Ohta Y, Nakamoto H, Ishii Y, Ikudome S, Takahashi K, Shima N. Muscle activation characteristics of the front leg during baseball swings with timing correction for sudden velocity decrease. PLoS ONE. 2015;10(4):1–12.
Castagneri C, Agostini V, Rosati S, Balestra G, Knaflitz M. Longitudinal assessment of muscle function after Total Hip Arthroplasty: Use of clustering to extract principal activations from EMG signals. MeMeA 2018—2018 IEEE International Symposium on Medical Measurements and Applications, Proceedings. 2018;p. 1–5.
Di Nardo F, Strazza A, Palmieri MS, Mengarelli A, Burattini L, Orsini O, et al. Detection of surface-EMG activity from the extensor digitorum brevis muscle in healthy children walking. Physiol Meas. 2018;39(1).
Uthvag S, Vijay Sai P, Dheeraj Kumar S, Muthusamy H, Chanu OR, Karthik Raj V. Real-time EMG acquisition and feature extraction for rehabilitation and prosthesis. Biomed Eng Appl Basis Commun. 2019;31(05):1950037.
Happee R. Goal-directed arm movements: I. Analysis of EMG records in shoulder and elbow muscles. J Electromyogr Kinesiol. 1992;2(3):165–78.
Zhang X, Wang X, Wang B, Sugi T, Nakamura M. Automatic adaptive onset detection using an electromyogram with individual difference for control of a meal assistance robot. J Med Eng Technol. 2009;33(4):322–7.
Severini G, Conforto S, Schmid M, D’Alessio T. Novel formulation of a double threshold algorithm for the estimation of muscle activation intervals designed for variable SNR environments. J Electromyogr Kinesiol. 2012;22(6):878–85. https://doi.org/10.1016/j.jelekin.2012.04.010.
Xu Q, Quan Y, Yang L, He J. An adaptive algorithm for the determination of the onset and offset of muscle contraction by EMG signal processing. IEEE Trans Neural Syst Rehabil Eng. 2013;21(1):65–73.
Kachhwaha R, Vyas AP, Bhadada R. Adaptive Threshold-Based Approach for Facial Muscle Activity Detection in Silent Speech EMG Recording. In: Proceedings of 6th International Conference on Recent Trends in Computing. Lecture Notes in Networks and Systems. Springer, Singapore; 2021. p. 83–98. Available from: https://springer.longhoe.net/10.1007/978-981-33-4501-0_9.
Hogan N, Mann RW. Myoelectric signal processing: optimal estimation applied to electromyography-part i: derivation of the optimal myoprocessor. IEEE Trans Biomed Eng. 1980;BME–27(7):382–95.
Staude G, Wolf W, Appel U. Automatic event detection in surface EMG of rhythmically activated muscles. Annu Int Conf IEEE Eng Med Biol Proc. 1995;17(2):1351–2.
Micera S, Sabatini AM, Dario P. An algorithm for detecting the onset of muscle contraction by EMG signal processing. Med Eng Phys. 1998;20(3):211–5.
Magda M, Świątek J, Wyrostek P. Enhanced Sign Changes for SEMG Onset Detection. In: Proceedings of the 27th International Conference on Systems Engineering, ICSEng 2020. Lecture Notes in Networks and Systems. Springer, Cham.; 2021. p. 358–366. Available from: http://springer.longhoe.net/10.1007/978-3-030-65796-3_35.
Ellaway PH. Cumulative sum technique and its application to the analysis of peristimulus time histograms. Electroencephalogr Clin Neurophysiol. 1978;45(2):302–4. https://doi.org/10.1111/j.1532-5415.1991.tb01642.x.
Garavito F, Gonzalez J, Cabarcas J, Chaparro D, Portocarrero I, Vargas AEMG, signal analysis based on fractal dimension for muscle activation detection under exercice protocol. In. XXI Symposium on Signal Processing, Images and Artificial Vision (STSIVA). IEEE. 2016;2016:1–5.
Drapała J, Brzostowski K, Szpala A, Rutkowska-Kucharska A. Two stage EMG onset detection method. Arch Control Sci. 2012;22(4):427–40.
Trigili E, Grazi L, Crea S, Accogli A, Carpaneto J, Micera S, et al. Detection of movement onset using EMG signals for upper-limb exoskeletons in reaching tasks. J NeuroEng Rehabil. 2019;16(1):45. https://doi.org/10.1186/s12984-019-0512-1.
Di Nardo F, Nocera A, Cucchiarelli A, Fioretti S, Morbidoni C. Machine learning for detection of muscular activity from surface EMG signals. Sensors. 2022;22(9):3393.
Liu J, Liu Q. Use of the integrated profile for voluntary muscle activity detection using EMG signals with spurious background spikes: A study with incomplete spinal cord injury. Biomed Signal Proc Control. 2016;24:19–24. https://doi.org/10.1016/j.bspc.2015.09.004.
Santello M, McDonagh M. The control of timing and amplitude of EMG activity in landing movements in humans. Exp Physiol. 1998;83(6):857–74. https://doi.org/10.1113/expphysiol.1998.sp004165.
Allen GM, Gandevia SC, McKenzie DK. Reliability of measurements of muscle strength and voluntary activation using twitch interpolation. Muscle & Nerve. 1995;18(6):593–600.
Cannon J, Kay D, Tarpenning KM, Marino FE. Comparative effects of resistance training on peak isometric torque, muscle hypertrophy, voluntary activation and surface EMG between young and elderly women. Clin Physiol Funct Imaging. 2007;27(2):91–100. https://doi.org/10.1111/j.1475-097X.2007.00719.x.
Saito A, Akima H. Neuromuscular activation of the vastus intermedius muscle during isometric hip flexion. PLoS ONE. 2015;10(10):1–12.
Karimimehr S, Marateb HR, Muceli S, Mansourian M, Mañanas MA, Farina D. A real-time method for decoding the neural drive to muscles using single-channel intra-muscular EMG recordings. Int J Neural Syst. 2017;27(06):1750025. https://doi.org/10.1142/S0129065717500253.
Vila-Chã C, Falla D, Correia MV, Farina D. Adjustments in motor unit properties during fatiguing contractions after training. Med Sci Sports Exerc. 2012;44(4):616–24.
Ivanenko YP, Poppele RE, Lacquaniti F. Spinal cord maps of spatiotemporal alpha-motoneuron activation in humans walking at different speeds. J Neurophysiol. 2005;95(2):602–18. https://doi.org/10.1152/jn.00767.2005.
Rodrigues C, Fernandez M, Megia A, Comino N, Del-Ama A, Gil-Agudo A, et al. Comparison of Intramuscular and Surface Electromyography Recordings Towards the Control of Wearable Robots for Incomplete Spinal Cord Injury Rehabilitation. 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob). 2020 11;p. 564–569.
Rodrigues-Carvalho C, Fernández-García M, Pinto-Fernández D, Sanz-Morere C, Barroso FO, Borromeo S, et al. Benchmarking the effects on human-exoskeleton interaction of trajectory, admittance and EMG-triggered exoskeleton movement control. Sensors. 2023;23(2):791.
Acknowledgements
The authors would like to thank the participating volunteers for their valuable time and effort. We would also like to thank Dr. José L. Pons and Dr. Dario Farina for their insights on the conceptual design of this paper.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. This work was funded by the European Union’s Horizon 2020 research and innovation program (Project EXTEND - Biidirectional Hyper-Connected Neural System) under grant agreement No 779982. This work has been also partially funded by CSIC Interdisciplinary Thematic Platform (PTI+) NEURO-AGING+ (PTI-NEURO-AGING+) and by the Spanish Ministry of Science, Innovation and Universities, with grant agreement IJC2020-044467-I.
Author information
Authors and Affiliations
Contributions
CRC: main writing process for the manuscript. CRC, JMF, AJD-A, FOB and JCM: study design. CRC and JMF: data acquisition. CRC and JMF: data analysis. CRC, JMF, AJD-A, FOB and JCM: data interpretation. All authors: approval of final manuscript and agreement to be accountable for all aspects of the work while ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Participants were informed about the procedures and possible discomfort associated with the experiments. After that, they signed an informed consent to participate. All procedures were conducted in accordance with the Declaration of Helsinki and approved by a local ethics committee, as well as by the Spanish Agency of Medicines and Medical Devices (AEMPS)—record 721/19/EC.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Carvalho, C.R., Fernández, J.M., del-Ama, A.J. et al. Review of electromyography onset detection methods for real-time control of robotic exoskeletons. J NeuroEngineering Rehabil 20, 141 (2023). https://doi.org/10.1186/s12984-023-01268-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12984-023-01268-8