
Abstract
Backgrounds
To study the effects of supplementation of a marine omega-3 poly-unsaturated fatty acids (n3-PUFA) formulation (Omega3Q10) in older adults with hypertension and/or hypercholesterolemia.
Methods
A total of 97 people were enrolled to receive 12-week supplementation of either Omega3Q10 (n = 48) or soybean oil (n = 49). Total cholesterol (TC), low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), and hypertension-related symptoms were determined before and after the supplementation.
Results
There were no baseline differences between the two groups. Omega3Q10 supplementation significantly reduced diastolic blood pressure (DBP) (from 81.6 ± 5.3 mmHg to 79.3 ± 5.2 mmHg, P < 0.05). Blood concentrations of TC and LDL-C decreased significantly and blood HDL-C level increased significantly after 12 weeks of Omega3Q10 (5.5 ± 0.7 vs. 5.3 ± 0.5, P < 0.05; 3.7 ± 0.8 vs. 3.3 ± 0.6, P < 0.05; 1.2 ± 0.6 vs. 1.3 ± 0.5, P < 0.05, respectively) and soybean oil supplementation (5.7 ± 0.8 vs. 5.6 ± 0.7, P < 0.05; 3.6 ± 0.7 vs. 3.4 ± 0.8, P < 0.05; 1.0 ± 0.8 vs. 1.2 ± 0.7, P < 0.05, respectively) but no group differences were found. A significantly greater proportion of the people in the Omega3Q10 group became free from headache and palpitations & chest tightness symptoms after the 12-week supplementation compared to that of the soybean oil group (95.5% vs. 71.4%, P < 0.01; 95.8 vs. 75.5%, P < 0.01, respectively).
Conclusion
12-week supplementation of Fish oil-based PUFA appear to be more effective in improving DBP and hypertension-related symptoms than soybean oil in old adults with hypertension and hypercholesterolemia although both supplementation improved TC, LDL-C and HDL-C concentrations.
Similar content being viewed by others


Background
Elevated blood-pressure or blood cholesterol levels are major risk factors for cardiovascular events that are the major cause of death worldwide [1]. Hypertension that develops over time without a specific cause is considered benign hypertension. The common manifestations of hypertension include dizziness, headache, fatigue, tinnitus, palpitations & chest tightness, and lassitude in the loins and knees. It is estimated that more than one third of adults living in the US and China has hypertension or hypercholesterolemia, most of whom remain untreated [2, 3].
While modification of lifestyle, including low-sodium intake, high potassium diet, increasing physical activity, quitting smoking, reducing alcohol consumption, and maintaining a healthy weight can lower the risk of one’s progression of hypertension, many people experience difficulties to change their habits [4, 5]. Recent studies suggest that dietary supplementation of certain nature products, such as fish oil-derived Omega-3 polyunsaturated fatty acids (n-3 PUFA) [6,7,8,9,10] and/or plant derived-PUFA, phospholipids, sterols and stanols can be beneficial on blood cholesterol and blood pressure [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]. However, controversy still remains around the cardioprotective effects of fish oil-derived n3-PUFA [27,28,29] probably due to heterogeneous nature in the selection of different participants, formulation of different supplements, background diet, ratio of n3-PUFA: n6-PUFA and outcome measures [30,31,32].
The aim of this observational study was to evaluate the effects of supplementation of Omega3Q10, a fish oil-based Omega-3 n-3 PUFA formulation and soybean oil control in older adults with elevated blood pressure and blood cholesterol.
Methods
Study population
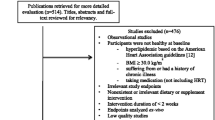
The recruitment of the participants into the study was started on September 2, 2013 and completed on October 12, 2013, and the last follow-up observation was completed on January 7, 2014, at Tang-Qiao Community Health Service Center in Pudong New District in Shanghai, China. Volunteers were recruited by self-referral in response to media coverage and word of mouth. All study procedures were conducted in accordance with the Helsinki Declaration of 1975 and were approved by the Shanghai Jiao Tong University School of Public Health Institutional Review Board. Written informed consent form was obtained from all participants prior to enrollment into the study.
Subjects who met the first and one of other three following criteria were eligible for the study:
Inclusion criteria:
-
1)
Healthy males or females at least 50 years of age;
-
2)
Having current symptoms of elevated blood pressure (systolic blood pressure 130–139 mmHg or diastolic blood pressure 85-89 mmHg);
-
3)
Having a history of elevated blood pressure (systolic blood pressure 140-159 mmHg or diastolic blood pressure 90-99 mmHg);
-
4)
Having a history of elevated blood cholesterol (total cholesterol (TC) concentrations higher than normal range: 2.8 to 5.7 mmol/L; HDL-C: 0.78 to 1.55 mmol/L; LDL-C: 1.68 to 4.53 mmol/L; glucose: 3.9 to 6.1 mmol/L).
Exclusion criteria:
-
1)
Having diagnosed with any severe medical conditions or complications of the liver, kidneys, heart, lungs, or any other organs, or malignant tumors;
-
2)
People who have much doubts of the study, unwilling to participate or unlikely to keep adherence of the study procedure were also excluded.
Randomization and blindness
Participants were randomly assigned to the Omega3Q10 treatment group or soybean oil control group. The randomization was performed using a predetermined randomization code which was generated by a random number generator.
Trial participants and community doctors were both blinded from the treatment (double-blind trial). Of the 100 enrolled participants, 97 participants completed the 12-week follow-up, including 48 subjects in the Omega3Q10 group and 49 subjects in the control group. Two subjects of the Omega3Q10 group and 1 subject of the soybean oil control group withdrew from the study due to objections by family members.
The participants received similar-looking capsules in color-coded bottles (white bottles for Omega3Q10 and yellow bottles for soybean oil control). Neither the subjects nor the medical doctors, including the study principal investigator (R.S.), knew the specific color code until the end of the study. Both the Omega3Q10 capsules and the control capsules (which was composed of soybean oil) were manufactured and supplied by GardaVita® Inc. (Costa Mesa, California, USA). Each participant was instructed to take 1 capsule with a meal, two times per day for 12 weeks and a new batch of supplements was dispensed every month during follow-up sessions.
The key active ingredients of Omega3Q10 formulation include Omega-3 fish oil (1000 mg/day) (including EPA (eicosapentaenoic acid, 312 mg), DHA (docosahexaeonic acid, 202 mg), Omega3Q10 complex (L-carnitine fumarate, Co-enzyme Q10, lycopene, 265 mg), vitamin E (alpha tocopherol acetate and natural tocopherol oil, 50 IU), Vitamin B6 (pyridoxine hydrochloride, 20 mg), B12 (methylcobalamin, 500 mcg) and folic acid (400 mcg). Each soybean oil capsule includes 910 mg soybean oil (saturated fatty acids 31.3 mg); monounsaturated fatty acids (45.57 mg); polyunsaturated fatty acids (229.48 mg); oleic acid (48 mg).
Evaluation of blood pressure, blood lipids/ cholesterols and quality of life
Blood concentrations of TC, LDL-C, HDL-C were evaluated before and after the 12-week treatment. Changes in blood pressure and in elevated blood pressure-related symptoms including headache, dizziness, tinnitus, palpitations, and chest tightness were evaluated before and after the 12-week intervention. Measurement of baseline blood pressure, and the measurement of the final blood pressure were both repeated twice with each repeat separated by a 1-week time interval. Elevated blood pressure-associated symptoms i.e. dizziness, headache, tinnitus, palpitations and chest tightness were scored using a self-administered 6-point scale (0 = no symptoms, 5 = most severe). All participants were followed up each month in order to check compliance and adverse effects.
Statistics analysis
EpiData 3.1 software was used for the data entry and SPSS 20 software was used for statistical analysis. Group data were presented as the mean ± standard deviation or median ± Quartile Range (QR). Differences between the Omega3Q10 and soybean oil groups were compared using Student’s t-test for quantitative variables with normal distribution and Mann-Whitney U test for variables with non-normal distribution, or Chi-square test for categorized variables. Ridit scoring test, which is a non-parameter test for comparing two or more sets of ordered qualitative data, was used for evaluating the changes in the symptom severity scores after the intervention. A multivariate regression analysis was also performed in order to evaluate the role of confounding factors on final results. The alpha level of P > 0.05 was chosen as being statistically significant. All p-values reported were 2-sided.
Results
Demographic characteristics
The baseline information of age, gender and histories of alcohol intake, disease and medication of the participants are shown in Table 1. There were 24 males (50%) and 24 females (50%) in the Omega3Q10 group, and 24 males (48.98%) and 25 females (51.02%) in the soybean oil group. The gender distribution between the two groups was not significantly different between the two groups (χ2 = 0.10, P = 0.920). The average age of all participants was 62.83 ± 10.16, and no significant difference for age was found between the Omega3Q10 group (63.26 ± 10.34 years) and the soybean oil group (62.41 ± 10.10 years) (t = 0.411, P = 0.682).
There were no significant differences between Omega3Q10 and soybean oil groups in the patterns of alcohol drinking (22.9% vs. 24.5%) (χ2 = 0.033, P = 0.855), smoking (22.9% vs. 20.4%) (χ2 = 0.09, P = 0.764), medical history of elevated blood pressure (39.6% vs. 46.9%) (χ2 = 0.534, P = 0.465), hypercholesterolemia (45.8% vs. 32.7%) (χ2 = 1.768, P = 0.184), coronary heart issues (6.2% vs. 16.3%) (χ2 = 2.449, P = 0.118), stroke (2.1% vs. 6.1%) (χ2 = 0.24, P = 0.624), diabetes (6.2% vs. 8.2%) (χ2 = 0.0, P = 1.00), and other health-related concerns (2.1% vs. 2.0%) (χ2 = 0.0, P = 1)(Table 1).
There were no significant differences between Omega3Q10 and soybean oil groups in the proportion of the participants who used anti-hypertensive medicine (35.4% vs. 46.9%,χ 2=1.328,P = 0.249, Renin-angiotensin system inhibitors (ACEI/ARB): 20.83% vs. 20.41%; calcium channel blockers: 10.42% vs. 16.33%; Diuretics: 2.08% vs. 4.8%; β-blockers: 2.04% vs. 1.03%% and other anti-hypertensive medicine: 2.04% vs. 4.08%), the number of years of anti-hypertensive medicine use (5.7 ± 4.0 vs. 5.8 ± 6.7,Z = 0.793,P = 0.428), the proportion of the participants who used cholesterol lowering drugs (6.7% vs. 11.6%, χ 2=0.192,P = 0.661) and the year of cholesterol lowering drug use (1.4 ± 1.4 vs. 2.5 ± 4.2,t = 0.426, P = 0.685).
Blood lipids/cholesterol levels
There are no significant differences between Omega3Q10 and soybean oil groups in baseline blood cholesterol (5.5 ± 0.7 mmol/L vs. 5.7 ± 0.8 mmol/L) (P > 0.05), HDL (1.3 ± 0.6 mmol/L vs. 1.0 ± 0.8 mmol/L) (P > 0.05), and LDL (3.7 ± 0.8 mmol/L vs. 3.6 ± 0.7 mmol/L), (P > 0.05), nor in post-treatment blood cholesterol (5.3 ± 0.5 mmol/L vs. 5.6 ± 0.7 mmol/L) (P > 0.05), HDL (1.3 ± 0.5 mmol/L vs. 1.2 ± 0.7 mmol/L) (P > 0.05), and LDL (3.3 ± 0.6 mmol/L vs. 3.4 ± 0.8 mmol/L) (P > 0.05) (Table 2). Both Omega3Q10 and soybean oil treatments, however, significantly reduced cholesterol and LDL-C and increased HDL-C (P < 0.05, each), with a relatively greater reduction of TC and LDL-C found in the Omega3Q10 group than in soybean oil group.
Blood pressure
The mean values of systolic blood pressure (SBP) and diastolic blood pressure (DBP) of the Omega3Q10 group and the soybean oil group before and after the 12-week treatment are shown in Table 3. There were no baseline differences between the Omega3Q10 and soybean oil groups in SBP (132.3 ± 5.5 vs.131.8 ± 9.3, P > 0.05) and DBP (81.6 ± 5.3 vs. 80.4 ± 6.1, P > 0.05) (Table 3), nor after the 12-week treatment in SBP (130.7 ± 7.3 vs. 129.7 ± 8.7 P > 0.05) and DBP (79.3 ± 5.2 vs. 79.1 ± 5.3, P > 0.05, respectively) (Tables 3). However, both SBP and DBP levels were reduced after either Omega3Q10 or soybean oil treatment, with a significant DBP reduction only found in the Omega3Q10 group. There are no baseline differences in the blood pressure equilibrium distribution (normal, high-normal (blood pressure), or level I hypertension (mild)) according to the Guidance for the prevention and management of elevated blood pressure (2010 Chinese Edition) between the two groups (χ 2=0.907, P = 0.341) (Table 4).
Hypertension-related symptoms
The results of Mann-Whitney U test showed no baseline differences between the Omega3Q10 and soybean oil groups in the self-reported hypertension-related symptom severity scores of headaches (Z = 1.585, P = 0.113), tinnitus (Z = 0.581, P = 0.561) and palpitations & chest tightness (Z = 0.92, P = 0.358) except a significant group difference in the distribution of dizziness scores (Z = 2.785, P = 0.005) (Table 5). After the 12-week intervention, however, more people in the Omega3Q10 group showed reduced symptom severities of headache (Z = 3.238, P = 0.001); tinnitus (Z = 1.732, P = 0.083) and; palpitations & chest tightness (Z = 2.852, P = 0.004) than the soybean oil group (Tables 6).
Discussion
Elevated blood lipid level and high-than-normal blood pressures are independent risk factors of increased cardiovascular dysfunction, chronic inflammation and stroke [33,34,35,36]. Despite the development of pharmaceutical therapies and the recommendations of life style modification, many people still fail to achieve therapeutic goals [37,38,39]. Dietary supplements of fish oil-derived n-3 PUFA or fish oil n-3 PUFA may reduce plasma cholesterol and LDL-C levels, and cardiovascular risk [18, 20].
In this study, both Omega3Q10 and soybean oil significantly reduced blood cholesterol and LDL-C levels and, to a less extend, reduced blood pressures by Omega3Q10. in old adults with elevated blood pressure and blood cholesterol levels. Omega3Q10 also reduced the symptom severities of headache and palpitations & chest tightness. These results are in agreement with the current knowledge that intake of n-3 polyunsaturated fatty acid (PUFA) especially that of fish oil can reduce the incidence of hypertension and cardiac mortality in certain subpopulation [40,41,42], and in line with the recent report that 12 months of omega 3 PUFA supplementation significantly decreased systolic blood pressure (SBP) (by 2.7 +/− 2.5 mmHg, p = 0.001) and diastolic blood pressure (DBP) (by 1.3 +/− 3.3 mmHg, p < 0.001), in 111 hypertriglyceridemic patients with untreated normal-high blood pressure and with or without metabolic syndrome [43].
Soybean oil was also effective in improving dyslipidemia probably because soybean oil contains n3-PUFA or other potent ingredients that have cholesterol relieving activities. Sterols, sterol esters and the sterol glycosides present in soybean oil [44], can inhibit cholesterol absorption and lower LDL-C levels [45].
In this study, the daily dose of Omega3Q10 contains 514 mg PUFA (312 mg EPA (n3-PUFA) and 202 mg DHA (n6-PUFA) whereas the daily dose of soybean oil contains 115.48 mg PUFA (14 mg linolenic acid (n3-PUFA), 100 mg linoleic acid (n6-PUFA) and 48 mg oleic acid all of which have different cholesterol and LDL-C lowering effects as well as cardioprotective effects albeit with the fish n-3 PUFA having better efficacy. Other studies showed that a 45-day supplement of high dose of fish oil-derived n-3 PUFA (3 g/day) significantly reduced systolic pressure [17]; high blood n-3 fatty acids levels are associated with reduced risk of death, [46] and dietary intake of linolenic acid is associated with a lower risk of cardiovascular disease mortality. [47]. Additionally, eating fish monthly can reduce the risk of ischemic stroke. [48]. Epidemiological studies also support a protective role of plant-derived n-3 fatty acid such as alpha-linolenic acid (ALA), which was inversely related to all-cause mortality in 5,452 participants without prior cardiovascular disease [49].
Genetic background may affect the efficacy of fish oil-derived n-3 PUFA. A recent longitudinal study shows that a higher omega-3 PUFA intake was associated with a more pronounced blood pressure decrease over time in subjects with the CYP4F2 433VV genotype [50]. Omega-3 PUFA may also reduce blood pressure by acting as a substrate of cytochrome P450 (CYP450), the enzymes involved in the production of vasoactive mediators. Functional polymorphisms (SNPs) in CYP450 genes are associated with elevated blood pressure and ischemic stroke [51,52,53,54,55,56]. Dietary fish oils have been shown to have different preventive effects on the development of elevated blood pressure and vascular response in different genetic strains of rat [57]. Depending on rat strains and fish oil composition, this was more pronounced for fish oils enriched with EPA and DHA and was more prominent in the SHR and SHR/WKY backcross than it was in the SHR-SP.
There is a possibility that ingredients such as vitamin B of the Omega3Q10 formulation may have interacted with n3- PUFA and n6-PUFA on cholesterol and LDL-C levels as supplementation of B vitamins had no beneficial effects on health-related quality of life in stroke and cardiovascular disease survivors [58].
Fish oil-derived n-3 PUFA may exert its cardioprotective effects by anti-inflammatory mechanisms [59]. Long-term n3-PUFA dietary supplementation prevents the development of intracranial atherosclerosis and macrophage infiltration into the vessel wall, therefore reducing inflammation and initial thickening in animals [60]. Omega-3 PUFAs may exert their multiple health-benefit effects partly by actions such as antagonizing arachidonic acid-induced proinflammatory prostaglandin E2 (PGE2) formation and by suppressing nuclear factor-κB, C-reactive proteins that are potent inducer of proinflammatory cytokines including interleukin-1beta, interleukin 6 and tumor necrosis factor-α, which are decreased by EPA and DHA [61,62,63,64,65,66,67] [68]. n-3 PUFAs can also repress lipogenesis and increase resolvins and protectin generation, thus reduced inflammation. EPA and DHA benefit insulin resistance by inducing adiponectin, an anti-inflammatory adipokine [67].
One study, however, showed that treatment with statin alone or statin plus fish oil, but not fish oil alone, reversed the increased plasma hs-CRP and IL-6 (a low-grade chronic inflammatory state) in in 48 obese individuals [69]. Marine omega-3 fatty acids also dose-dependently regulated apolipoproteins, apolipoprotein-defined lipoprotein subclasses, and Lp-PLA2 in individuals with moderate hypertriglyceridemia [70]. It is known that apolipoprotein (apo) distribution and lipoprotein (Lp)-associated markers of inflammation, such as lipoprotein-associated phospholipase A2 (Lp-PLA2), influence the atherogenicity of circulating lipids and lipoproteins.
Other multiple mechanisms may underlie the beneficial effect of Omega3O10. It has been reported that the antihypertensive effect of angiotensin converting enzyme (ACE) inhibitors can be augmented by supplementing fish oil [71]. Omega-3 PUFAs could regulate vasomotor tone and renal sodium excretion, through competing with omega-6 PUFAs for common metabolic enzymes and thereby decreasing the production of vasoconstrictor. PUFAs also reduce angiotensin-converting enzyme (ACE) activity, angiotensin II formation, tumor growth factor-beta (TGF-b) expression, enhance endothelial nitric oxide (NO) generation and activate the parasympathetic nervous system, resulting in improved vasodilation and arterial compliance of both small and large arteries [72]. Indeed, fish oil attenuated adrenergic overactivity without altering glucose metabolism during an oral glucose load [73]. Omega-3 fatty acids improved platelet redox balance in diabetic patients with hypertension [74]. Fish oil supplements increased the concentration of phospholipid, improved membrane fluidity, decreased the activity of HMG-CoA reductase in alloxan-induced diabetic mice [75]. n-3 PUFA is also involved in the regulation of mitochondrial 3-hydroxy-3-methylglutaryl-CoA (HMG-CoA) synthase (HMGCS2) that catalyzes the first step of ketogenesis and is critical in various metabolic conditions [76].
In this study, participants who received soybean oil capsule also showed improved cholesterol and LDL-C levels. Studies have shown that, soybean oil contains n-3 PUFA and other active ingredients such as proteins, phospholipids, lecithin, sterol and stanol, all of which can affect cholesterol metabolism. Supplement of soybean-derived lecithin for 2 years reduced serum cholesterol and triglycerides levels by 22% and 26%, respectively, in people on low fat diet. [77]. Replacement of dietary animal proteins with soy proteins for 4 weeks significantly reduced blood cholesterol by 18.6% and improved HDL-C, in 65 people with hyperlipidemia [78]. And novel soybean oils differing in linoleic acid (LA) and alpha-linolenic acid (ALA) ratio and n-6/n-3 ratio can alter immune functions. [79], and serum cholesterol and triglyceride levels, respectively [80].
Several meta-analyses reported that daily intake of up to 2 g of stanols or sterols can reduce blood LDL-C by 10% (or by 20% if on low fat/cholesterol diet or on statin medication) [81,82,83,84]. However, because sterol-enriched foods increase plasma sterol levels and the risk of atherosclerosis in patients with homozygous phytosterolemia [45, 85, 86], further studies are needed to determine the optimal dose range in different subpopulations.
Limitations
There are limitations of this pilot study. The number of the participants, the selection of the dosage of Omega3Q10 supplement and the control group (soy oil) were not optimized for detecting potential effects of Omega3Q10 on the studied parameters. For example, the originally calculated sample size (N = 45 per group, with 10% drop rate) was based on the assumption of a baseline value of 3.7 ± 0.7 mmol/L of LDL-C in the Omega3Q10 and soybean oil group that would be decreased to 3.3.0 ± 0.6 mmol/L after 12-week Omega3Q10 intervention and no change after soybean oil intervention. But the results show that soy oil tended to produce similar effects as that of Omega3Q10 probably due to the presence of plant sterols and other active PUFA ingredients in soy oil.
The concurrent use of different anti-hypertension and anti-dyslipidemia drugs by a significant portion of the participants in the Omega3Q10 group (42.1%) and in the Soy Oil group (58.5%) would also make it difficult to discern the true effects of the Omega3Q10 and Soy oil on blood pressure and blood lipid profile.
Previous studies showed that both statin therapy (simvastatin (40 mg/d) and co-supplements of red yeast rice (a natural source of statins) and fish oil for 12 weeks significantly reduced LDL-C levels (−39.6% vs. −42.4%, P < .001 and P < .001) [87]. And co-administration of omega-3 fatty acids (4.2 g/d) with statin for 8-weeks significantly increased LDL particle size and decreased TG level in dyslipidemic patients with type 2 diabetes and without causing significant adverse effects [88]. Furthermore, co-administration of omega-3 (EPA 465 mg; DHA, 375 mg; othern-3 FA, 60 mg) and statins (simvastatin 20 mg /d) for 6 weeks produced greater reduction in TG than statin monotherapy (41% reduction vs 13.9% reduction, P < 0.01) [89].
Other studies show that statin alone or co-treatment with fish oil, but not fish oil alone, reversed increased plasma hs-CRP and IL-6 and, hence reduced chronic inflammatory state in visceral obesity [69]. In addition, the triglyceride-lowering effect of atorvastatin, but not fish oils, is associated with increased VLDL apo C-III fractional catabolism and hence lower VLDL apo C-III concentrations. Co-treatment provided no significant additional improvement in VLDL apo C-III metabolism compared with atorvastatin alone [90].
Recent studies have also showed that 16-week of co-administration of plant sterols esters (1300 mg), fish oil (1000 mg EPA and DHA) and vitamins B12 (50 mug), B6 (2.5 mg), folic acid (800 mug) and coenzyme Q10 (3 mg) significantly reduced total cholesterol, LDL- cholesterol, VLDL-cholesterol, subfractions LDL-2, IDL-1, IDL-2 and plasma homocysteine levels and decreased triacylglycerols levels at a trend level (by 17.6%) in hypercholesterolemic children and adolescents [91]. Fish-oil esters of plant sterols improve the lipid profile of dyslipidemic subjects more than do fish-oil or sunflower oil esters of plant sterols [92]. Low doses of fish oil-derived EPA and DHA plus plant sterols also dose-dependently decreased serum triglyceride concentrations in hypercholesterolemic men and women [93]. These studies together with our current findings suggest potential additive benefits of co-administration of n-3 PUFAs and plant sterols for people with increased risk of cardiovascular conditions and that should be evaluated in future better-controlled, large-scale studies.
In this study, we also conducted multivariate regression analysis, with intervention groups as the primary variable of interest. The covariates were baseline smoking status (yes/no), current medicine use (yes/no), baseline DBP (mmHg), and baseline cholesterol level (baseline TC/baseline HDL/baseline LDL). No significant differences were found between the Omega3Q10 and soybean oil in blood pressures (SBP/DBP) or in cholesterol (LDL/TC/HDL) after the potential confounders were controlled, suggesting that both Omega3Q10 and soybean oil supplementation had similar effects on blood cholesterol and blood pressure. We did notice, however, that after controlling the current medicine use (taken by 42.1% of the Omega3Q10 group and by 58.5% of the Soy Oil group), the LDL-C results showed a trend difference (P < 0.18) between the Omega3Q10 and Soybean oil group. Because the number of people is very small and the medicine varied greatly (anti-hypertension or lipid-lowering etc.), further studies should determine if Omega3Q10 and soybean oil could interact differently with different anti-hypertension and anti-dyslipidemia drugs.
Conclusions
Dietary supplementation of Fish oil-based Omega3Q10 were safe and effective in reducing blood pressure and blood cholesterol and LDL-C levels in old adults with hypertension and hypercholesterolemia. Omega3Q1 also appears to be more effective than soybean oil in improving DBP and hypertension-related symptoms in old adults with hypertension and hypercholesterolemia although both supplementation improved TC, LDL-C and HDL-C concentrations.
Abbreviations
- ALA:
-
alpha-linolenic acid
- CYP450:
-
cytochrome P450
- DBP:
-
diastolic blood pressure
- DHA:
-
docosahexaeonic acid,
- EPA:
-
eicosapentaenoic acid
- HDL-C:
-
high density lipoprotein cholesterol
- LA:
-
linoleic acid
- LDL-C:
-
low density lipoprotein cholesterol
- n3-PUFA:
-
omega-3 poly-unsaturated fatty acids
- Omega3Q10:
-
dietary supplement formulation based on marine n3-PUFA
- SBP:
-
systolic blood pressure
- SHR:
-
spontaneously hypertensive rat
- SHR/WKY:
-
a backcross of SHR and WKY rats
- SHR-SP:
-
stroke-prone spontaneously blood pressure symptoms rats
- SNPs:
-
single nucleotide polymorphisms
- TC:
-
total cholesterol
- WKY:
-
Wistar-Kyoto rat, a normotensive and the closest genetic control for the SHR rats
References
Nwankwo T, Yoon S, Burt V, Gu Q: Hypertension among adults in the US: National Health and Nutrition Examination Survey, 2011–2012[777 KB]. NCHS Data Brief, No. 133. Hyattsville, MD: : National Center for Health Statistics, Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2013.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, et al. Executive summary: heart disease and stroke statistics--2016 update: a report from the American Heart Association. Circulation. 2016;133:447–54.
Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, et al. Heart disease and stroke Statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133:e38–60.
Zomer E, Leach R, Trimmer C, Lobstein T, Morris S, James WP, Finer N. Effectiveness and cost-effectiveness of interventions that cause weight loss and reduce the risk of cardiovascular disease. Diabetes Obes Metab. 2017;19:118–24.
Ritz E. Total cardiovascular risk management. Am J Cardiol. 2007;100:53J–60J.
Merino J, Sala-Vila A, Kones R, Ferre R, Plana N, Girona J, Ibarretxe D, Heras M, Ros E, Masana L. Increasing long-chain n-3PUFA consumption improves small peripheral artery function in patients at intermediate-high cardiovascular risk. J Nutr Biochem. 2014;25(6):642–6.
Investigators of the GISSI Prevension trial. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto miocardico. Lancet. 1999;354:447–55.
Lee TH. Go fish: a good choice for preventing strokes. Harv Heart Lett. 2001;12:1–2.
Omega-3 fatty acids offer heart protection in multiple ways. These healthy essential fats provide benefits whether consumed as supplements or from dietary sources. Heart Advis. 2011;14:5.
Tokede OA, Onabanjo TA, Yansane A, Gaziano JM, Djousse L. Soya products and serum lipids: a meta-analysis of randomised controlled trials. Br J Nutr. 2015;114:831–43.
Ho XL, Liu JJ, Loke WM. Plant sterol-enriched soy milk consumption modulates 5-lipoxygenase, 12-lipoxygenase, and myeloperoxidase activities in healthy adults - a randomized-controlled trial. Free Radic Res. 2016;50:1396–407.
Fukunaga K, Hosomi R, Fukao M, Miyauchi K, Kanda S, Nishiyama T, Yoshida M. Hypolipidemic effects of phospholipids (PL) containing n-3 polyunsaturated fatty acids (PUFA) are not dependent on esterification of n-3 PUFA to PL. Lipids. 2016;51:279–89.
Wanezaki S, Tachibana N, Nagata M, Saito S, Nagao K, Yanagita T, Kohno M. Soy beta-conglycinin improves obesity-induced metabolic abnormalities in a rat model of nonalcoholic fatty liver disease. Obes Res Clin Pract. 2015;9:168–74.
Lammi C, Zanoni C, Arnoldi A, Vistoli G. Two peptides from soy beta-Conglycinin induce a Hypocholesterolemic effect in HepG2 cells by a statin-like mechanism: comparative in vitro and in silico modeling studies. J Agric Food Chem. 2015;63:7945–51.
Huth PJ, Fulgoni VL 3rd, Larson BT. A systematic review of high-oleic vegetable oil substitutions for other fats and oils on cardiovascular disease risk factors: implications for novel high-oleic soybean oils. Adv Nutr. 2015;6:674–93.
Tong LT, Zhong K, Liu L, Guo L, Cao L, Zhou S. Oat oil lowers the plasma and liver cholesterol concentrations by promoting the excretion of faecal lipids in hypercholesterolemic rats. Food Chem. 2014;142:129–34.
Simao AN, Lozovoy MA, Simao TN, Dichi JB, Matsuo T, Dichi I. Nitric oxide enhancement and blood pressure decrease in patients with metabolic syndrome using soy protein or fish oil. Arq Bras Endocrinol Metabol. 2010;54:540–5.
Chen ZY, Peng C, Jiao R, Wong YM, Yang N, Huang Y. Anti-hypertensive nutraceuticals and functional foods. J Agric Food Chem. 2009;57:4485–99.
Teres S, Barcelo-Coblijn G, Benet M, Alvarez R, Bressani R, Halver JE, Escriba PV. Oleic acid content is responsible for the reduction in blood pressure induced by olive oil. Proc Natl Acad Sci U S A. 2008;105:13811–6.
Aguila MB, Pinheiro AR, Aquino JC, Gomes AP, Mandarim-de-Lacerda CA. Different edible oil beneficial effects (canola oil, fish oil, palm oil, olive oil, and soybean oil) on spontaneously hypertensive rat glomerular enlargement and glomeruli number. Prostaglandins Other Lipid Mediat. 2005;76:74–85.
Merritt JC. Metabolic syndrome: soybean foods and serum lipids. J Natl Med Assoc. 2004;96:1032–41.
Aguila MB, Sa Silva SP, Pinheiro AR, Mandarim-de-Lacerda CA. Effects of long-term intake of edible oils on hypertension and myocardial and aortic remodelling in spontaneously hypertensive rats. J Hypertens. 2004;22:921–9.
Ogawa H, Yamamoto K, Kamisako T, Meguro T. Phytosterol additives increase blood pressure and promote stroke onset in salt-loaded stroke-prone spontaneously hypertensive rats. Clin Exp Pharmacol Physiol. 2003;30:919–24.
Ratnayake WM, Plouffe L, Hollywood R, L'Abbe MR, Hidiroglou N, Sarwar G, Mueller R. Influence of sources of dietary oils on the life span of stroke-prone spontaneously hypertensive rats. Lipids. 2000;35:409–20.
Nevala R, Vaskonen T, Vehniainen J, Korpela R, Vapaatalo H. Soy based diet attenuates the development of hypertension when compared to casein based diet in spontaneously hypertensive rat. Life Sci. 2000;66:115–24.
Samsonov MA, Pogozhaeva AV, Vasilev AV, Bogdanova SN, Pokrovskaia GR, Varsanovich EA, Orlova LA. Effect of anti-arteriosclerosis diet, containing soya protein isolate and omega-3 polyunsaturated fatty acids on the activity of mononuclear and platelet lysosomal hydrolases in patients with hypertension and ischemic heart disease. Vopr Pitan. 1993:14–8.
n-3 fatty acids in patients with multiple cardiovascular risk factors. N Engl J Med. 2013;368:1800–8.
Fish, not fish oil, prevents stroke. Harv Mens Health Watch. 2013;17:8.
Rhee JJ, Kim E, Buring JE, Kurth T. Fish consumption, Omega-3 fatty acids, and risk of cardiovascular disease. Am J Prev Med. 2017;52:10–9.
Zock PL, Blom WA, Nettleton JA, Hornstra G. Progressing insights into the role of dietary fats in the prevention of cardiovascular disease. Curr Cardiol Rep. 2016;18:111.
Yuan F, Wang H, Tian Y, Li Q, He L, Li N, Liu Z. Fish oil alleviated high-fat diet-induced non-alcoholic fatty liver disease via regulating hepatic lipids metabolism and metaflammation: a transcriptomic study. Lipids Health Dis. 2016;15:20.
Yang LG, Song ZX, Yin H, Wang YY, Shu GF, HX L, Wang SK, Sun GJ. Low n-6/n-3 PUFA ratio improves lipid metabolism, inflammation, oxidative stress and endothelial function in rats using plant oils as n-3 fatty acid source. Lipids. 2016;51:49–59.
Sturgeon JD, Folsom AR, Longstreth WT, Jr., Shahar E, Rosamond WD, Cushman M: Risk factors for intracerebral hemorrhage in a pooled prospective study. Stroke 2007, 38:2718–2725.
Nilsson PM, Engstrom G, Hedblad B. The metabolic syndrome and incidence of cardiovascular disease in non-diabetic subjects--a population-based study comparing three different definitions. Diabet Med. 2007;24:464–72.
Reeder BA, Angel A, Ledoux M, Rabkin SW, Young TK, Sweet LE. Obesity and its relation to cardiovascular disease risk factors in Canadian adults. Canadian heart health surveys research group. CMAJ. 1992;146:2009–19.
Reeder BA, Senthilselvan A, Despres JP, Angel A, Liu L, Wang H, Rabkin SW. The association of cardiovascular disease risk factors with abdominal obesity in Canada. Canadian heart health surveys research group. CMAJ. 1997;157(Suppl 1):S39–45.
Alagona P Jr, Ahmad TA. Cardiovascular disease risk assessment and prevention: current guidelines and limitations. Med Clin North Am. 2015;99:711–31.
De Vera MA, Bhole V, Burns LC, Lacaille D. Impact of statin adherence on cardiovascular disease and mortality outcomes: a systematic review. Br J Clin Pharmacol. 2014;78:684–98.
Teng M, Lin L, Zhao YJ, Khoo AL, Davis BR, Yong QW, Yeo TC, Lim BP. Statins for primary prevention of cardiovascular disease in elderly patients: systematic review and meta-analysis. Drugs Aging. 2015;32:649–61.
Yang B, Shi MQ, Li ZH, Yang JJ, Li D. Fish, long-chain n-3 PUFA and incidence of elevated blood pressure: a meta-analysis of prospective cohort studies. Nutrients. 2016;8
Song TJ, Cho HJ, Chang Y, Choi K, Jung AR, Youn M, Shin MJ, Kim YJ. Low plasma proportion of omega 3-polyunsaturated fatty acids predicts poor outcome in acute non-cardiogenic ischemic stroke patients. J Stroke. 2015;17:168–76.
Leon H, Shibata MC, Sivakumaran S, Dorgan M, Chatterley T, Tsuyuki RT. Effect of fish oil on arrhythmias and mortality: systematic review. BMJ. 2008;337:a2931.
Cicero AF, Derosa G, Di Gregori V, Bove M, Gaddi AV, Borghi C. Omega 3 polyunsaturated fatty acids supplementation and blood pressure levels in hypertriglyceridemic patients with untreated normal-high blood pressure and with or without metabolic syndrome: a retrospective study. Clin Exp Hypertens. 2010;32:137–44.
Milkova T, Popov A, Selva A, Vettori U. Sterol composition of Bulgarian soya and corn oils. Nahrung. 1977;21:7–12.
Gylling H, Plat J, Turley S, Ginsberg HN, Ellegard L, Jessup W, Jones PJ, Lutjohann D, Maerz W, Masana L, et al. Plant sterols and plant stanols in the management of dyslipidaemia and prevention of cardiovascular disease. Atherosclerosis. 2014;232:346–60.
Erkkila AT, Lehto S, Pyorala K, Uusitupa MI. N-3 fatty acids and 5-y risks of death and cardiovascular disease events in patients with coronary artery disease. Am J Clin Nutr. 2003;78:65–71.
Djousse L, Folsom AR, Province MA, Hunt SC, Ellison RC. Dietary linolenic acid and carotid atherosclerosis: the National Heart, Lung, and Blood Institute family heart study. Am J Clin Nutr. 2003;77:819–25.
He K, Rimm EB, Merchant A, Rosner BA, Stampfer MJ, Willett WC, Ascherio A. Fish consumption and risk of stroke in men. JAMA. 2002;288:3130–6.
Sala-Vila A, Guasch-Ferre M, Hu FB, Sanchez-Tainta A, Bullo M, Serra-Mir M, Lopez-Sabater C, Sorli JV, Aros F, Fiol M, et al. Dietary alpha-linolenic acid, marine omega-3 fatty acids, and mortality in a population with high fish consumption: findings from the PREvencion con DIeta MEDiterranea (PREDIMED) study. J Am Heart Assoc. 2016;5
Tagetti A, Ericson U, Montagnana M, Danese E, Almgren P, Nilsson P, Engstrom G, Hedblad B, Minuz P, Orho-Melander M, et al. Intakes of omega-3 polyunsaturated fatty acids and blood pressure change over time: possible interaction with genes involved in 20-HETE and EETs metabolism. Prostaglandins Other Lipid Mediat. 2015;120:126–33.
Yi X, Zhang B, Wang C, Liao D, Lin J, Chi L. CYP2C8 rs17110453 and EPHX2 rs751141 two-locus interaction increases susceptibility to ischemic stroke. Gene. 2015;565:85–9.
Yan G, Wang Y. Association of CYP11B2 gene polymorphism with ischemic stroke in the north Chinese Han population. Neurol India. 2012;60:504–9.
Demirdogen BC, Adali AC, Bek S, Demirkaya S, Adali O. Cytochrome P4501A1 genotypes and smoking- and hypertension-related ischemic stroke risk. Hum Exp Toxicol. 2013;32:483–91.
Munshi A, Sharma V, Kaul S, Al-Hazzani A, Alshatwi AA, Shafi G, Koppula R, Mallemoggala SB, Jyothy A. Association of 1347 G/a cytochrome P450 4F2 (CYP4F2) gene variant with hypertension and stroke. Mol Biol Rep. 2012;39:1677–82.
Wang SY, **ng PF, Zhang CY, Deng BQ. Association of CYP2J2 gene polymorphisms with ischemic stroke and stroke subtypes in Chinese population. Medicine (Baltimore). 2017;96:e6266.
Marginean A, Banescu C, Moldovan V, Scridon A, Marginean M, Balasa R, Maier S, Tarusi M, Dobreanu M. The impact of CYP2C19 loss-of-function polymorphisms, clinical, and demographic variables on platelet response to Clopidogrel evaluated using impedance Aggregometry. Clin Appl Thromb Hemost. 2017;23:255–65.
Mano MT, Bexis S, Abeywardena MY, McMurchie EJ, King RA, Smith RM, Head RJ. Fish oils modulate blood pressure and vascular contractility in the rat and vascular contractility in the primate. Blood Press. 1995;4:177–86.
Andreeva VA, Latarche C, Hercberg S, Briancon S, Galan P, Kesse-Guyot E. B vitamin and/or n-3 fatty acid supplementation and health-related quality of life: ancillary findings from the SU.FOL.OM3 randomized trial. PLoS One. 2014;9:e84844.
Bazan HA, Lu Y, Thoppil D, Fitzgerald TN, Hong S, Dardik A. Diminished omega-3 fatty acids are associated with carotid plaques from neurologically symptomatic patients: implications for carotid interventions. Vasc Pharmacol. 2009;51:331–6.
Cao Z, Zhang P, He Z, Yang J, Liang C, Ren Y, Wu Z. Obstructive sleep apnea combined dyslipidemia render additive effect on increasing atherosclerotic cardiovascular diseases prevalence. Lipids Health Dis. 2016;15:98.
Mocellin MC, SilvaJde a P e, Camargo Cde Q, Fabre ME, Gevaerd S, Naliwaiko K, Moreno YM, Nunes EA, Trindade EB. Fish oil decreases C-reactive protein/albumin ratio improving nutritional prognosis and plasma fatty acid profile in colorectal cancer patients. Lipids. 2013;48:879–88.
Adler N, Schoeniger A, Fuhrmann H. Polyunsaturated fatty acids influence inflammatory markers in a cellular model for canine osteoarthritis. J Anim Physiol Anim Nutr (Berl). 2017;
Weylandt KH, Chiu CY, Gomolka B, Waechter SF, Wiedenmann B. Omega-3 fatty acids and their lipid mediators: towards an understanding of resolvin and protectin formation. Prostaglandins Other Lipid Mediat. 2012;97:73–82.
Ramirez-Ramirez V, Macias-Islas MA, Ortiz GG, Pacheco-Moises F, Torres-Sanchez ED, Sorto-Gomez TE, Cruz-Ramos JA, Orozco-Avina G, de la Rosa AJ C. Efficacy of fish oil on serum of TNF alpha, IL-1 beta, and IL-6 oxidative stress markers in multiple sclerosis treated with interferon beta-1b. Oxidative Med Cell Longev. 2013;2013:709493.
Faber J, Berkhout M, Fiedler U, Avlar M, Witteman BJ, Vos AP, Henke M, Garssen J, van Helvoort A, Otten MH, Arends J. Rapid EPA and DHA incorporation and reduced PGE2 levels after one week intervention with a medical food in cancer patients receiving radiotherapy, a randomized trial. Clin Nutr. 2013;32:338–45.
Langerhuus SN, Tonnesen EK, Jensen KH, Damgaard BM, Halekoh U, Lauridsen C. Effects of dietary n-3 and n-6 fatty acids on clinical outcome in a porcine model on post-operative infection. Br J Nutr. 2012;107:735–43.
Siriwardhana N, Kalupahana NS, Fletcher S, **n W, Claycombe KJ, Quignard-Boulange A, Zhao L, Saxton AM, Moustaid-Moussa N. N-3 and n-6 polyunsaturated fatty acids differentially regulate adipose angiotensinogen and other inflammatory adipokines in part via NF-kappaB-dependent mechanisms. J Nutr Biochem. 2012;23:1661–7.
Takase O, Hishikawa K, Kamiura N, Nakakuki M, Kawano H, Mizuguchi K, Fujita T. Eicosapentaenoic acid regulates IkappaBalpha and prevents tubulointerstitial injury in kidney. Eur J Pharmacol. 2011;669:128–35.
Chan DC, Watts GF, Barrett PH, Beilin LJ, Mori TA. Effect of atorvastatin and fish oil on plasma high-sensitivity C-reactive protein concentrations in individuals with visceral obesity. Clin Chem. 2002;48:877–83.
Skulas-Ray AC, Alaupovic P, Kris-Etherton PM, West SG. Dose-response effects of marine omega-3 fatty acids on apolipoproteins, apolipoprotein-defined lipoprotein subclasses, and Lp-PLA2 in individuals with moderate hypertriglyceridemia. J Clin Lipidol. 2015;9:360–7.
Howe PR, Lungershausen YK, Cobiac L, Dandy G, Nestel PJ. Effect of sodium restriction and fish oil supplementation on BP and thrombotic risk factors in patients treated with ACE inhibitors. J Hum Hypertens. 1994;8:43–9.
Cicero AF, Ertek S, Borghi C. Omega-3 polyunsaturated fatty acids: their potential role in blood pressure prevention and management. Curr Vasc Pharmacol. 2009;7:330–7.
Delarue J, Guillodo MP, Guillerm S, Elbaz A, Marty Y, Cledes J. Fish oil attenuates adrenergic overactivity without altering glucose metabolism during an oral glucose load in haemodialysis patients. Br J Nutr. 2008;99:1041–7.
McDonald DM, O'Kane F, McConville M, Devine AB, McVeigh GE. Platelet redox balance in diabetic patients with hypertension improved by n-3 fatty acids. Diabetes Care. 2013;36:998–1005.
Kamat SG, Roy R. Evaluation of the effect of n-3 PUFA-rich dietary fish oils on lipid profile and membrane fluidity in alloxan-induced diabetic mice (Mus Musculus). Mol Cell Biochem. 2016;416:117–29.
Rescigno T, Capasso A, Tecce MF. Involvement of nutrients and nutritional mediators in mitochondrial 3-hydroxy-3-methylglutaryl-CoA synthase gene expression. J Cell Physiol. 2017;
Tompkins RK, Parkin LG. Effects of long-term ingestion of soya phospholipids on serum lipids in humans. Am J Surg. 1980;140:360–4.
Sirtori CR, Zucchi-Dentone C, Sirtori M, Gatti E, Descovich GC, Gaddi A, Cattin L, Da Col PG, Senin U, Mannarino E, et al. Cholesterol-lowering and HDL-raising properties of lecithinated soy proteins in type II hyperlipidemic patients. Ann Nutr Metab. 1985;29:348–57.
Han SN, Lichtenstein AH, Ausman LM, Meydani SN. Novel soybean oils differing in fatty acid composition alter immune functions of moderately hypercholesterolemic older adults. J Nutr. 2012;142:2182–7.
Lee JH, Fukumoto M, Nishida H, Ikeda I, Sugano M. The interrelated effects of n-6/n-3 and polyunsaturated/saturated ratios of dietary fats on the regulation of lipid metabolism in rats. J Nutr. 1989;119:1893–9.
Amir Shaghaghi M, Abumweis SS, Jones PJ. Cholesterol-lowering efficacy of plant sterols/stanols provided in capsule and tablet formats: results of a systematic review and meta-analysis. J Acad Nutr Diet. 2013;113:1494–503.
Han S, Jiao J, Xu J, Zimmermann D, Actis-Goretta L, Guan L, Zhao Y, Qin L. Effects of plant stanol or sterol-enriched diets on lipid profiles in patients treated with statins: systematic review and meta-analysis. Sci Rep. 2016;6:31337.
Rocha VZ, Ras RT, Gagliardi AC, Mangili LC, Trautwein EA, Santos RD. Effects of phytosterols on markers of inflammation: a systematic review and meta-analysis. Atherosclerosis. 2016;248:76–83.
Ras RT, Geleijnse JM, Trautwein EA. LDL-cholesterol-lowering effect of plant sterols and stanols across different dose ranges: a meta-analysis of randomised controlled studies. Br J Nutr. 2014;112:214–9.
Katan MB, Grundy SM, Jones P, Law M, Miettinen T, Paoletti R. Efficacy and safety of plant stanols and sterols in the management of blood cholesterol levels. Mayo Clin Proc. 2003;78:965–78.
Hallikainen M, Simonen P, Gylling H. Cholesterol metabolism and serum non-cholesterol sterols: summary of 13 plant stanol ester interventions. Lipids Health Dis. 2014;13:72.
Becker DJ, Gordon RY, Morris PB, Yorko J, Gordon YJ, Li M, Iqbal N. Simvastatin vs therapeutic lifestyle changes and supplements: randomized primary prevention trial. Mayo Clin Proc. 2008;83:758–64.
Lee MW, Park JK, Hong JW, Kim KJ, Shin DY, Ahn CW, Song YD, Cho HK, Park SW, Lee EJ. Beneficial effects of Omega-3 fatty acids on low density lipoprotein particle size in patients with type 2 diabetes already under statin therapy. Diabetes Metab J. 2013;37:207–11.
Kim SH, Kim MK, Lee HY, Kang HJ, Kim YJ, Kim HS. Prospective randomized comparison between omega-3 fatty acid supplements plus simvastatin versus simvastatin alone in Korean patients with mixed dyslipidemia: lipoprotein profiles and heart rate variability. Eur J Clin Nutr. 2011;65:110–6.
Chan DC, Nguyen MN, Watts GF, Ooi EM, Barrett PH. Effects of atorvastatin and n-3 fatty acid supplementation on VLDL apolipoprotein C-III kinetics in men with abdominal obesity. Am J Clin Nutr. 2010;91:900–6.
Garaiova I, Muchova J, Nagyova Z, Mislanova C, Oravec S, Dukat A, Wang D, Plummer SF, Durackova Z. Effect of a plant sterol, fish oil and B vitamin combination on cardiovascular risk factors in hypercholesterolemic children and adolescents: a pilot study. Nutr J. 2013;12:7.
Demonty I, Chan YM, Pelled D, Jones PJ. Fish-oil esters of plant sterols improve the lipid profile of dyslipidemic subjects more than do fish-oil or sunflower oil esters of plant sterols. Am J Clin Nutr. 2006;84:1534–42.
Ras RT, Demonty I, Zebregs YE, Quadt JF, Olsson J, Trautwein EA. Low doses of eicosapentaenoic acid and docosahexaenoic acid from fish oil dose-dependently decrease serum triglyceride concentrations in the presence of plant sterols in hypercholesterolemic men and women. J Nutr. 2014;144:1564–70.
Funding
This study was funded, in part, by DRM Resources (Costa Mesa, California, USA), National Natural Science Foundation of China (7163187), the Social Cognitive and Behavioral Sciences Program of Shanghai Jiao Tong University (14JCRY03), Shanghai Key Discipline Construction Project in Public Health (15GWZK1002). The funders had no role in the collection, analysis or interpretation of the data, nor the drafting of the manuscript.
Availability of data and materials
Not applicable
Data sharing statement
No additional data are available.
Author information
Authors and Affiliations
Contributions
JR and RS conceived experiments; TS, Gang Xu and YC designed the experiments; TS, Gang Xu, YC, JZ and DL recruited and followed the participants; TS, JZ, YC and Guoqiang **ng analyzed the data; Guoqiang **ng wrote the paper; EX reviewed the paper. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Shanghai Jiao Tong University School of Public Health Institutional Review Board and conducted in agreement with the Declaration of Helsinki.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Shen, T., **ng, G., Zhu, J. et al. Effects of 12-week supplementation of marine Omega-3 PUFA-based formulation Omega3Q10 in older adults with prehypertension and/or elevated blood cholesterol. Lipids Health Dis 16, 253 (2017). https://doi.org/10.1186/s12944-017-0617-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12944-017-0617-0