
Abstract
Background
As a means of establishing a sustained and fair health care financing system, Ethiopia has planned and ratified a legal framework to introduce a social health insurance program for employees of the formal sector to protect them against financial and health burdens. However, the implementation has been delayed due to the resistance of public servants to pay the proposed premium. The aim of this study was to estimate the magnitude of willingness to pay the proposed amount of premium set by the government for the social health insurance program and the factors associated with it among public servants in Addis Ababa, Ethiopia.
Methods
An institution-based cross-sectional study design was used to conduct the study. Multistage sampling was employed to select a total of 503 from 12 randomly selected public sectors. Data were collected using pretested, interviewer-administered structured questionnaires. A contingent valuation method with an iterative bidding game was used to elicit willingness to pay. Finally, logistic regression analysis was used to identify independent predictors of willingness to pay. Statistical significance was considered at P < 0.05 with adjusted odds ratios calculated at 95% CIs.
Results
Only 35.4% were willing to pay the proposed premium (3% of their monthly salary). Those who had children from 6–18 years old (AOR = 3.252; 95% CI: 1.15, 9.22), had a history of unaffordable health service costs during the last 12 months (AOR = 9.631; 95% CI: 4.12, 22.52), and had prior information about the social health insurance program (AOR = 11.011, 95% CI. 3.735–32.462) were more likely to pay for the proposed social health insurance program compared to their counterparts.
Conclusion
The willingness to pay the proposed amount premium for social health insurance among public servants in Addis Ababa was very low that implies the implementation will be challenging. Thus, the government of Ethiopia should consider reviewing the amount of premium contributions expected from employees before implementing the social health insurance scheme.
Similar content being viewed by others
Introduction
Revenue raising, pooling and purchasing of health services are the key functions of the health financing system [1]. The health system should have a good health financing system that ensures that people use health services without financial catastrophe or impoverishment [2, 3]. This can be done by designing insurance systems [4]. The social health insurance (SHI) scheme is one of the possible organizational mechanisms for raising and pooling funds to finance health services, along with tax financing, private health insurance, community-based health insurance, and others [4, 5].
Pooling of prepaid funds has received due attention in the health financing mechanisms of the health system framework designed by the World Health Organization (WHO) [6]. The system pools both the health risks of the people on the one hand and the contributions of employees, employers and the government on the other [7]. Thus, it protects people against financial and health burdens and is a relatively fair method of financing health care [8, 9]. To achieve universal health coverage (UHC), social health insurance plays a crucial role without incurring financial hardship [8, 10, 11].
Developed countries often use SHI to mobilize funds and pool risks, but low- and middle-income countries rarely use this approach [11]. In Ethiopia, the strategic health care financing system is a recent practice that began in the 1990s [12], following the 1993 health policy [13]. Health insurance was one of the financing mechanisms of the 1998 health care financing strategy (HCFS) and received more attention in the 2017 revised strategy [14]. According to the 2018 Ethiopian Ministry of Health annual report, only 38% of the eligible population joined the Community health insurance program [15]. Similarly, although legal frameworks were developed and many preparatory activities have been made to implement the Social Health insurance scheme [16, 17] in which government employees shall contribute 3% of their gross salary [17], Ethiopia is still at the introduction stage of SHI [16,17,18,19]. One of the main reasons for repeatedly postponing the implementation of the SHI scheme in Ethiopia was public servant’s resistance to pay the proposed amount of premium [12, 20].
Despite the fact that there is no national study on Willingness to pay (WTP) for SHI in Ethiopia, and most of them were conducted in some parts of the country on few type of public servants that made it to generalized, evidence from those studies indicated that public servants willing to pay for SHI varied from place to place [2, 21,22,23]. For example, according to a study done on public servants in St. Paul’s hospital, Addis Ababa, showed that only 17% were willing to pay the proposed amount of premium [2]. In contrast to this, a study in Northeast Ethiopia showed that 85.3% of public servants were willing to pay and join SHI. However, a focused group discussion in this similar study showed that public servants were agreed to contribute approximately 2% of their gross salary by giving their reasons of low salary, very high cost of living, and burden of other deductions from their salary that implied the need to reduce the proposed premium [22].
The government of Ethiopia has implemented many awareness and demand creation activities for SHI in the country including Addis Ababa. However, the current status of willingness to pay the proposed amount of premium was not well known in Addis Ababa, central Ethiopia. Therefore, this study was conducted to assess the current status of willingness to pay for the proposed SHI scheme and its associated factors among the general public servants in Addis Ababa, Ethiopia.
Methods
Study design and setting
This study employed an institution-based cross-sectional design and was conducted from February 24-June 17/2020. The study was conducted among public servants in Addis Ababa, which is the capital city of Ethiopia and has a population of approximately 4.8 million [24]. Administratively, the city has 11 sub Cities and 116 Districts. According to the 2019 report, there were approximately 85 registered types of public institutions that might have its own lower level organizational structures, and 115,398 public servants who were permanently employed at different levels of the city administration [25].
Population
All employees working in 85 registered public institutions in the Addis Ababa city administration were considered as the source population. The study participants were randomly selected public servants from the sampled public institutions. Public servants who were permanently employed and present during the study period were included in the study. Public servants who were severely ill or could not listen and speak were excluded from the study.
Sample size and sampling procedures
The required sample size for the first objective of this study was determined by using a single population proportion formula with the following assumptions: 95% confidence level, 5% margin of error and 53% proportion public servants willing to willingness to pay for the proposed SHI, taken from a previous study done in South Ethiopia [26].
Accordingly, this yields a maximum sample size of 383. Adding a 10% nonresponse rate and a design effect of 1.2, the final sample size required for the study was 506.
Sample size for the second objective was calculated by using EPI Info version 7, and using factors associated with WTP. Studies in Ethiopia found that WTP for social health insurance were associated with income, educational status, information status on SHI, health status, quality of health service and affordability of health service. The sample size was calculated by using each listed factors, and unfortunately the sample size we found in each of them was less compared to the sample size calculated for the first objective.
A multistage sampling system was used to select study participants. Initially, 12 public sectors were randomly selected from all 85 public sectors identified in Addis Ababa. In the next stage, offices, directorates or units were selected randomly from the selected public institutions. Finally, lists of public servants were obtained from the human resource department, and participants were selected from each office, directorate or unit proportionally depending on the size of the public institutions using a systematic random sampling technique.
Variables
Dependent variables
Willingness to pay the proposed amount premium for the SHI.
Independent variables
Socio-demographic variables (age, sex, educational status, income, marital status, family size, presence of under five children, presence of children from 6–18 years old), level of awareness of social health insurance, health status and affordability of health service costs.
Data collection tool and quality control
Data were collected using an interviewer-administered structured questionnaire adapted from previous studies. The questionnaire was first prepared in English and then translated to Amharic. A pretest was performed among 5% of the sample size among public servants working in public institutions that were not included in the study. Data were collected by six BSc health science professionals and supervised by two experienced public health specialists. Data collectors and supervisors were trained for two days on procedures and made familiar with the questionnaire.
Data collection procedure
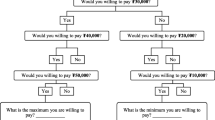
In measuring WTP using contingent valuation and bidding games, first, the hypothetical market was described to respondents, and a series of questions were asked. In this study, a social health insurance scheme proposed by the government of Ethiopia was taken as a case scenario. First, information was provided on general concepts of health insurance, particularly about the proposed social health insurance scheme. Then, participants were asked for their willingness to pay 3% of their monthly salary for the proposed SHI scheme. The amount of the first bid was purposively selected to assess participants’ willingness to pay for the proposed amount of premium (3% of gross salary) for the planned SHI scheme in Ethiopia. Depending upon the response, the respondents were then asked if they would be willing to pay the next higher or lower amount. If a participant responded ‘yes’ for 3%, the next higher bid (4%) was offered, and if a participant responded “No” for 3%, the next lower bid (2%) was offered. This bidding game was continued until a participant switched his or her response from inclusion or exclusion.
Operational definitions
-
Public institution: All types registered institutions that are directly responsible to report to Addis Ababa City administration that might also have organizational structures to the lower administration level
-
Proposed amount of premium: 3% of public servants’ gross salary.
-
Willingness to pay for the proposed premium: Willingness to pay 3% of gross monthly salary that was set by the government for the proposed SHI Scheme in Ethiopia
Data management and analysis
Data was coded and entered into Epi Info version 7 and transferred into SPSS version 21 for analysis. Descriptive statistics, such as frequency tables, were used to present the results. Associations between independent variables and willingness to pay were assessed using both bivariate and multivariable logistic regression analyses. Independent variables with p values < 0.25 were entered into multivariable logistic regression to assess the effect of each independent variable when controlling for all other potential confounders. Adjusted odds ratios (AORs) and 95% confidence intervals were estimated, and a p value < 0.05 was considered significant.
Results
Socio-demographic characteristics of respondents
Of the 506 randomly selected respondents, 503 (99.4%) agreed to participate. Among the participants, more than half (56.3%) were males. The mean age of the respondents was 33.22 (SD ± 7.724), with a range between 21 and 56 years. More than half (53.1%) of the respondents were married, and the average family size of study participants was 2.89 (SD ± 1.690). The majority (74.2%) of respondents had a first degree or above educational level (See Table 1).
Health and health care-related characteristics of respondents
Among the study participants, 103 (20.5%) had chronic disease, and 208 (41.4%) experienced at least one episode of any other acute illness in the last 12 months. Among participants who had experienced illness, 93.8% sought treatment for their recent episodes. Out-of-pocket health expenditure (86.7%) was the main means of paying at a point of getting health service. More than half (51.8%) experienced unaffordable health service costs. About one third (36.9%) received their health service from public health facilities, and only 15.9% of them were satisfied with the service quality (See Table 2).
Awareness of social health insurance
The study revealed that 70% of the respondents had ever heard about SHI, and mass media was the main source of information for more than half (54.5%) of them. Among those participants who had ever heard about social health insurance, 94% believed that social health insurance has benefits (See Table 3).
Willingness to pay the proposed premium
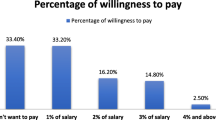
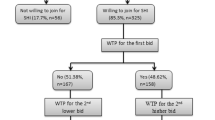
The present study indicated that only 178 (35.4%) study participants had a willingness to pay for the proposed SHI premium (3% of their gross monthly salary). Out of those who were willing to pay the starting bid, 69 (38.8%) respondents also had a willingness to pay for the next higher bid. Out of the 325 (64.6%) participants who responded did not have a willingness to pay the starting bid, 79 (24.3%) had a willingness to pay for the next lower bid. The overall estimated mean WTP for the proposed SHI was 2.5% (95% CI 2.4–2.6) of their gross monthly salary. More than half (53.4%) were willing to pay less than 3% of their gross salary (See Table 4).
Factors associated with willingness to pay for the proposed SHI scheme
After multivariable logistic regression analysis, presence of children from 6–18 years old, who experienced unaffordable health service costs, and who had ever heard of the social health insurance scheme were significantly associated with WTP for SHI.
Participants who had family members from 6–18 years of age were 3 times more likely to be willing to pay for the proposed SHI scheme compared to those who had not (AOR = 3.252, 95% CI. 1.147–9.219).
It was also found that participants who experienced unaffordable health service costs were 9 times more willing to pay for the proposed SHI scheme than those who experienced affordable health service costs (AOR = 9.631, 95% CI. 4.118–22.525). In addition, participants who had ever heard about the health insurance scheme were 11 times more likely to be willing to pay than those who had never heard (AOR = 11.011, 95% CI. 3.735–32.462 (See Table 5).
Discussion
The establishment and implementation of a fair and resilient health care financing system requires local context studies and recommendations. As part of future evidence, this study aimed to assess the willingness to pay the amount of premium for the proposed social health insurance and the factors associated with it among public servants working in Addis Ababa, Ethiopia.
In the present study, only 35.4% of respondents were WTP the amount of premium for the proposed SHI which is much higher than the findings of a study performed in St. Pauls’ Hospital Millennium Medical College, Addis Ababa Ethiopia, which found that 17% of public servants were WTP for the proposed SHI scheme [2]. This difference may be due to the difference in the study population. Participants in the St. Paul’s Hospital Millennium Medical College study included only health care professionals (HCPs). The main explanation for the lower prevalence of WTP for SHI among HCP in this study is that all government hospitals in Addis Ababa provide free health services for their employees. As a result, HCPs rely on the free health service rather than using SHI. Health professionals have an interest in obtaining free health services. The reason behind this interest was that health workers believe that they should not pay for health services that they are providing for others or that the government should cover their expenses for health care.
In contrast to this, there were also evidences indicating that public servants could be willing to pay more than a premium set by the government. A study conducted in North East Ethiopia, Mekele, in 2017 revealed that WTP for SHI scheme was 3.6% [27]. This showed that WTP in Mekele was higher than both of the proposed premium and the WTP in the current study. Another study in Iran in 2014 also showed that more than half (56.6%) with willing to pay the proposed premium and the average WTP for SHI per person per month was more than the premium for the SHI in Iran which consistently showed that public servants also can be willing to pay more than the premium set by the government [28]. This difference might be due to the difference in socio demographic characteristics, and methodology. Mekele and Addis Ababa are two different cities with different characteristics. Addis Ababa is the capital city of the country with higher cost of living. In addition, the study in Mekele did not used the actual proposed premium(3%) as a first bid while our study used the proposed premium as the first bid for their willingness to pay. This showed that the difference might be due to methodology.
The current study result shows that the overall estimated mean of WTP for SHI was 2.5% of participants’ gross monthly salary, which is less than the amount of premium declared by the Ethiopian government [18]. This is higher than the figure obtained from a previous study performed at the initial stage of SHI introduction among public servants in Addis Ababa which showed that the average willingness of contribution was 1.52% of their gross monthly salary [23]. This improvement may be due to awareness and demand creation efforts made by the government, differences in time of study and/or changes in socioeconomic characteristics of the study participants. However, the finding of this study is lower than the finding of a study conducted in northeastern Ethiopia, Mekele, in 2017, which found a 3.6% WTP for the SHI scheme [27].
Our study found that out-of-pocket (OOP) health expenditure was participants’ main means (86.7%) of payment for their health service costs. This finding is supported by a previous study performed in the southern part of Ethiopia in 2014, which found that 87.7% of the respondents used OOP expenditures [26]. This is also consistent with the report from the Ethiopian Health Account (EHA) in 2016/17. The report of the EHA shows that OOP health expenditure was one of the dominant sources of health care finance in Ethiopia [29]. Depending on a health system dominated by OOP health expenditure contradicts the goal of universal health coverage (UHC). To achieve the goals of UHC, a health system requires financing systems that enable health services without incurring financial hardship at a time of obtaining health services [10].
Participants who had family members aged 6–18 years were more likely to have WTP for the proposed SHI scheme than those who had not. The possible reason might be that those participants who had children from 6–18 years old may believe that the proposed SHI scheme is favoring them over the others. In the current Ethiopian SHI scheme, children above 18 years are not entitled to their parent’s health insurance benefits. The finding of this study is supported by a previous study performed in Mekele in 2017 that reported participants were resisting that eligibility should not be based on age alone but also on their capacity to generate income [27].
Study participants who had ever heard about health insurance schemes prior to this study were more willing to pay than those who had never heard. This finding is consistent with a study performed in South Ethiopia [26] and Vietnam in 2014 [30]. This could be explained by employees who ever heard about SHI being more likely to be aware of the benefits of having health insurance.
Regarding awareness and demand creation, the government of Ethiopia reported that many efforts have been made [15]. However, this study revealed that nearly one-third of public servants (30%) were not ever heard about SHI. As a country that is going to implement SHI, having such a significant portion of public servants who had not heard about SHI will have a negative effect on the implementation of the SHI scheme.
Study participants who had experienced unaffordable health service costs were more willing to pay for the proposed SHI scheme than those who did not experience unaffordable health service costs. This finding is similar to a previous study performed in Wolaita Sodo Town, South Ethiopia [26].
Strength and limitations of the study
This study was one of the few studies done on the proposed SHI scheme, characterizing the public servants in Addis Ababa, covering more public institutions, employing random sampling, pretesting tools, making statistical adjustments of design effect may ensure validity and reliability of the data.
Study participants were asked their willingness to pay without having previous experiences with SHI. Due to this, they may have ambitious expectations or may not take it as a serious plan going to be realized soon. Due to this, their decision may deviate from the decision they made if they were put themselves in the real situation. Moreover, the starting point for the biding game was decided to be 3% of gross salary (proposed by the government), which might affect participants’ first bid choice decision. This first choice bias may influence participants’ last bid of WTP for SHI.
Conclusions
The willingness to pay the proposed amount premium for social health insurance among public servants in Addis Ababa was very low that implies the implementation will be challenging. Willingness to pay for SHI was more likely among those participants who had children from 6–18 years old, had a history of unaffordable health service costs and had prior information about the SHI scheme, which were significant determinants of WTP. The government of Ethiopia should consider the current level of WTP and address all related factors prior to implementing SHI in the country. All policy makers and implementers under the government of Ethiopia can use the identified associated factors as potential areas of intervention to introduce accepted and sustainable SHI in the country. Further efforts should be made to create awareness and increase demand for SHI. A comprehensive national assessment should be conducted to understand the overall images of the country on employees’ WTP for SHI schemes.
Availability of data and materials
Most of the datasets generated and analyzed during the current study are included in the manuscript, hence, for those who need the underling row data, they can get from corresponding author on reasonable request.
Abbreviations
- CBHI:
-
Community-Based Health Insurance
- CVM:
-
Contingent Valuation Method
- EHA:
-
Ethiopian Health Account
- HCFS:
-
Health Care Financing Strategy
- OOP:
-
Out of Pocket
- REC:
-
Research and Ethics Committee
- SHI:
-
Social Health Insurance
- SPSS:
-
Statistical Package for Social Science
- UHC:
-
Universal Health Coverage
- WHO:
-
World Health Organization
- WTP:
-
Willingness to Pay
References
WHO. Health Systems Governance & Financing. Health Financing Guidline No 1:Health financing country diagnostic: a foundation for national strategy development. Vol 200, Autonomic Neuroscience: Basic and Clinical. 2016. Report No.: 1. https://www.who.int/health_financing/documents/country-diagnostic/en/. [Last accessed on 2022 Jan 2].
Lasebew Y, Mamuye Y, Abdelmenan S. Willingness to Pay for the Newly Proposed Social Health Insurance among Health Workers at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. Int J Heal Econ Policy. 2017;2(4):159–66.
Kofoworola Y, Id O, Akomolafe B, Ohiri K. Factors influencing willingness and ability to pay for social health insurance in Nigeria. PLoS ONE. 2019;14(8):e0220558.
WHO. The world health report. Health systems improving performance. 2000. https://www.who.int/whr/2010/en/. [Last accessed on 2021 Jan 15].
Ole Doetinchem GC and DE. Thinking of introducing social health insurance ? Ten questions health system financing. the pathto universal coverage. Geneva; 2010. https://www.who.int/healthsystems/topics/financing/healthreport/26_10Q.pdf?ua=1.[Last accessed on 2021 Feb 02].
WHO. Everybody’s business: strengthening health systems to improve health outcomes: WHO’s Framwork for Action. Geneva: WHO press; 2007. https://www.who.int/healthsystems/strategy/everybodys_business.pdf. [Last accessed on 2021 Dec 15].
Le Gall-Ely M. Definition, Measurement and Determinants of the Consumer’s Willingness to Pay: A Critical Synthesis and Directions for Further Research. Rech Appl en Mark (English Ed. 2009;24(2):91–112.
WHO. Social Health Insurance:Report of a Regional Expert Group Meeting. New Delhi; 2003. https://apps.who.int/iris/handle/10665/206364. [Last accessed on 2021 Dec 11].
Chiwire P, Evers SM, Mahomed H, Hiligsmann M. Willingness to pay for primary health care at public facilities in the Western Cape Province, Cape Town. South Africa J Med Econ. 2021;24(1):162–72.
WHO. The World Health Report. Health System Financing. 2010. https://www.who.int/whr/2010/en/. [Last accessed on 2021 Dec 15].
Hsiao WC, Shaw RP, Fraker A, Jowett M. Social Health Insurance for Develo** Nations - World Bank Institute development studies. Washington, D. C; 2007. 1–184 bl. https://openknowledge.worldbank.org/handle/10986/6860. [Last accessed on 2022 Feb 04]
Alebachew A, Yusuf Y, Mann C, Berman P. Ethiopia ’ s Progress in Health Financing and the Contribution of the 1998. Health Care and Financing Strategy in Ethiopia.Resource Tracking and Management Project. Boston, Massachusetts and Addis Ababa, Ethiopia; 2015.https://fpfinancingroadmap.org/data/files/resource-documents/hcfs_review_final_report_september_2015_0.pdf. [Last accessed on 2022 Feb 04]
Transitional Government of Ethiopia. Health Policy of the Transitional Government of Ethiopia. Addis Ababa; 1993. https://www.mindbank.info/item/721. [Last accessed on 2021 Dec 2].
FMoH. Health Care Financing Strategy 2017 – 2025. Addis Ababa, Ethiopia; 2017. Report No.: 2.
FMoH. Annual Health Sector Performance Report 211EFY(2018/19). Addis Ababa, Ethiopia; 2018. https://www.thepalladiumgroup.com/downloads/c442edbcdc749cd6dba609ada08a257b. [Last accessed on 2021 Dec 2].
FDRE. Social Health Insurance proclamation No.690/2010. Addis Ababa: 16th ye ar No.50. 19th August 2010. Federal Negarit Gazeta of the Federal Democratic Republic of Ethiopia. 2010. https://www.ilo.org/dyn/travail/docs/269/Social%20Health%20Insurance%20Proclamation%202010.pdf. [Last accessed on 2021 April 11].
Federal Democratic Republic of Ethiopia. Social Health Insurance scheme Council of Ministers Regulation No. 271/2012. Addis Ababa: 19th year No.3. Addis Ababa: Federal Negarit Gazeta of the Federal Democratic Republic of Ethiopia; 2012. http://ilo.org/dyn/natlex/natlex4.detail?p_lang=en&p_isn=89591&p_country=ETH&p_count=141&p_classification=15&p_classcount=5. [Last accessed on 2021 Dec 11].
Federal Democratic Republic of Ethiopia. Ethiopian Health Insurance Agency establishment Council of Ministers Regulation No. 191/2010. Addis Ababa; 2010. https://chilot.me/wp-content/uploads/2011/12/reg-no-191-2010-the-ethiopian-health-insurance-agency.pdf. [Last accessed on 2021 Dec 11].
EFMoH. Health Sector Transformation Plan (2015/16–2019/20). Vol 20. Addis Ababa, Ethiopia; 2015. https://www.globalfinancingfacility.org/ethiopia-health-sector-transformation-plan-201516-201920. [Last accessed on 2021 Dec 2].
Lavers T. Towards Universal Health Coverage in Ethiopia’s ‘developmental state’? The political drivers of health insurance. Soc Sci Med. 2019;228:60–7.
Tadele W, Aklilu M, Getaneh Y, Defar A, Acham Y. Willingness to pay for social health insurance among staffs in Ethiopian Public Health Institute, Addis Ababa. Ethiop j public Heal nutr. 2015;2(2):1–6.
Gidey MT, Gebretekle GB, Hogan ME, Fenta TG. Willingness to pay for social health insurance and its determinants among public servants in Mekelle City , Northern Ethiopia : a mixed methods study. Cost Eff Resour Alloc. 2019;17(2)1–12. Available at: https://doi.org/10.1186/s12962-019-0171-x
Obse A, Ryan M, Heidenreich S, Normand C, Hailemariam D. Eliciting preferences for social health insurance in Ethiopia: A discrete choice experiment. Health Policy Plan. 2016;31(10):1423–32.
United Nations - World Population Prospects. Addis Ababa, Ethiopia Metro Area Population 1950–2021. https://worldpopulationreview.com/en/world-cities/addis-ababa-population. [Last accessed on 2021 Dec 2].
Addis Ababa City adminstration Human resource management and development Bureau Annual report. 2019. http://www.addisababa.gov.et/ar/web/guest/civil-service-agency. [Last accessed on 2021 Dec 26].
Agago TA, Woldie M, Ololo S. Willingness to join and pay for the newly proposed social health insurance among teachers in Wolaita Sodo Town. South Ethiopia Ethiop J Health Sci. 2014;24(3):195–202.
Gidey MT, Gebretekle GB, Hogan ME, Fenta TG. Willingness to pay for social health insurance and its determinants among public servants in Mekelle City, Northern Ethiopia: A mixed methods study. Cost Eff Resour Alloc. 2019;17(1):1–11.
Nosratnejad S, Rashidian A, Mehrara M, Akbari Sari A, Mahdavi G, Moeini M. Willingness to pay for the social health insurance in Iran. Glob J Health Sci. 2014;6(5):154–63.
FMoH. Ethiopian Health Accounts,2016/17. Addis Ababa; 2019. http://www.moh.gov.et/ejcc/sites/default/files/2020.01/Ethiopia%207th%20Health%20Accounts%20Report_2016-17.pdf. [Last accessed on 2021 May 26].
Nguyen LH, Hoang ATD. Willingness to pay for social health insurance in central Vietnam. Front Public Heal. 2017;5(89):1–7.
Acknowledgements
The authors would like to express their sincere gratitude to St. Paul’s Millennium Medical College and Ethiopian Health Insurance Agency for their support for the accomplishment of this study. We would also like to thank the supervisors and data collectors for taking their precious time to collect the data. We are grateful to all respondents who participated in this study and took their time to provide information.
Funding
The funding source for each per diem of data collectors and supervisors of this research was Saint Paul’s Hospital Millennium Medical College. The funding body has no role in the design of the study, and collection, analysis and interpretation of data, and in writing this manuscript.
Author information
Authors and Affiliations
Contributions
MAK conceived and designed the study, performed the data collection and the statistical analysis, served as the lead author and revised the manuscript. ZAA assisted in data analysis and primarily wrote the manuscript. SM & BL designed and supervised the study, contributed to the local implementation of the study, assisted in the analysis and interpretation of the data and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was obtained from the Institutional Review Board (IRB) approval letter of St. Paul’s Hospital Millennium Medical College (reference number PM73/522 and date 29/02/2020). A formal letter obtained from the Addis Ababa city administration was provided to the respective administrative levels of the city. All of the study participants was informed about the purpose of the study, about their right to participate or to with draw at any time if they don’t want and their confidentiality. Informed consent was obtained from all study participants after explaining the purpose of the study. All methods were performed in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kokebie, M.A., Abdo, Z.A., Mohamed, S. et al. Willingness to pay for social health insurance and its associated factors among public servants in Addis Ababa, Ethiopia: a cross-sectional study. BMC Health Serv Res 22, 909 (2022). https://doi.org/10.1186/s12913-022-08304-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-022-08304-8