
Abstract
Objectives
To assess the characteristics of patients with unilateral and bilateral tubo-ovarian abscess (TOA).
Methods
Women diagnosed with TOA during 2003–2017 were included in this retrospective cohort study. TOA was diagnosed using sonography or computerized tomography and clinical criteria, or by surgical diagnosis. Demographics, sonographic data, clinical treatment, surgical treatment, and post-operative information were retrieved.
Results
The study cohort included 144 women who met the inclusion criteria, of whom 78 (54.2%) had unilateral TOA and 66 (45.8%) had bilateral TOA. Baseline characteristics were not different between the groups. There was a statistical trend that women with fewer events of previous PID were less likely to have with bilateral TOA (75.3% vs. 64.1%, respectively; p = 0.074). Women diagnosed with bilateral TOA were more likely to undergo surgical treratment for bilateral sal**o-oophorectomy compared to unilateral TOA (61.5% vs. 42.3%, respectively; p = 0.04). There was no difference in maximum TOA size between groups.
Conclusions
This study detected a trend toward increased need for surgical treatment in women diagnosed with bilateral TOA. These findings may contribute to determining the optimal medical or surgical treatment, potentially leading to a decrease in the duration of hospitalization, antibiotic exposure, and resistance. However, it is important to acknowledge that the results of the current study are limited, and further research is warranted to validate these potential outcomes.
Similar content being viewed by others
Introduction
Pelvic inflammatory disease (PID) is an ascending infection of the upper genital tract (uterus, fallopian tubes, and ovaries) that is caused by sexually transmitted organisms [1]. When left untreated, PID can worsen and lead to the formation of an abscess, known clinically as a tubo-ovarian abscess (TOA) [2, 3]. TOA is a serious complication of PID, as it can spread beyond the borders of the upper genital tract to involve adjacent pelvic organs [4].
Among women undergoing treatment for confirmed PID, 15–35% will receive a diagnosis of TOA [5, 6]. PID with progression to TOA is most common during the reproductive years, when sexual activity is usually at its peak and sexually transmitted infections are spread more widely [7,8,9,10].
The clinical presentation of this condition includes lower abdominal pain, purulent vaginal discharge, abnormal uterine bleeding, and elevated body temperature. Pelvic examination often reveals cervical, uterine, and adnexal motion tenderness [11]. Ultrasound scan or computed tomography (CT) is the preferred diagnostic imaging used to visualize and characterize a TOA [12, 13]. Diagnosis is usually based on both clinical and imaging parameters [14, 15].
The first-line treatment for TOA is broad-spectrum antibiotics, which successfully eliminate the infection in 70–87% of cases, depending on several factors, including the size of the abscess, patient’s age, and serum levels of inflammatory markers. Failure to respond to pharmacological treatment requires surgical intervention [4, 16,17,18,19]. Definitive information on the preferred procedure for TOA is lacking. The choice of surgical intervention depends on factors such as patient fertility planning and the severity of the disease [19, 20]. Options for surgical intervention include drainage, and most often unilateral or bilateral sal**ectomy. Unilateral or bilateral oophorectomy and hysterectomy can be an option in selected cases. A laparoscopic approach is preferred to laparotomy in centers with adequate experience [21]. Untreated PID or TOA can lead to long-term complications, such as infertility, ectopic pregnancies, abdominal adhesions, and chronic pelvic pain [22].
Extensive research has been invested in trying to identify the characteristics associated with TOA that were treated surgically versus those that responded well to antibiotics [23,24,25]. The findings suggested that bilateral as compared to unilateral abscesses were more likely to require surgical intervention [20]. TOAs that measured 6–7 cm or more were managed surgically more often than those 5 cm or smaller, which were managed conservatively with antibiotics [26]. Older women were more likely to fail antibiotic treatment [27]. Moreover, elevated inflammatory markers such as white blood cell count > 16,000/µL, C-reactive protein, and erythrocyte sedimentation rate levels, in addition to higher body temperature, were shown to be major determinants for drainage or surgical treatment [28, 29].
This study focused on the effect of unilateral or bilateral cases of TOA to determine whether the course of treatment, could be predicted based on this identifying feature.
Methods
This was a retrospective, cohort study. Data were retrieved from hospital electronic medical records from 2003 to 2017 of women admitted to the Gynecology Department of a tertiary level university-affiliated medical center.
Ethics
This study was performed in accordance with the principles of the Declaration of Helsinki. All methods were carried out in accordance with relevant guidelines and regulations. All experimental protocols were approved by the Meir Medical Center Ethics Committee, approval number MMC-082-17. Due to the retrospective nature of the study, Meir Medical Center Ethics Committee has waived need for informed consent statement.
Patients diagnosed with either unilateral or bilateral TOA were included in the study. Criteria for diagnosis included a positive computerized tomography (CT) or ultrasound scan revealing adnexal infiltration and at least one of the following criteria: temperature > 38 °C, leukocytosis > 15,000 mm3, or surgically proven TOA. Excluded from the study were patients who did not meet the strict criteria or those with insufficient data in the electronic medical record.
Hemodynamically stable women were treated conservatively with broad-spectrum parenteral antibiotics according to the protocol followed by the hospital gynecology department and based on CDC guidelines [30]. All women admitted to the gynecology ward receive treatment comprised of intravenous amoxicillin/clavulanic acid 1 g, three times daily, along with oral doxycycline 100 mg twice daily and oral metronidazole 500 mg three times a day. Cervical swabs are used to collect material for polymerase chain reaction (PCR) tests for sexually transmitted diseases and bacterial infections. The continuation of doxycycline treatment is contingent on the identification of chlamydia infection in the PCR results. Antibiotic treatment is then modified based on the outcome of the swab results. Surgery was indicated for unstable women or in cases of failed antibiotic therapy after 72 h. Signs of continuous abdominal pain, elevated temperature, or persistently high levels of inflammatory markers while receiving parenteral antibiotic treatment were considered failure to respond to antibiotic treatment. Surgical interventions included subcutaneous drainage guided by ultrasound or CT, laparoscopic unilateral or bilateral sal**ectomy, and in some cases, bilateral or unilateral sal**o-oophorectomy, with or without hysterectomy.
Demographic data, sonographic results, pre-operative, intraoperative, and post-operative findings were retrieved from the hospital electronic medical records to assess the differences between the two groups. No direct human involvement was needed.
Outcomes were compared between patients with unilateral TOA or bilateral TOA.
Statistical analysis
Patient characteristics were compared between the groups, using student t-test for continuous variables, and the chi-square or Fisher’s Exact Test for categorical variables. Results were considered significant when the p-value was ≤ 0.05. Data are presented as number and percentage for categorical variables and as mean and standard deviation (SD) for continuous variables. All statistical analyses were performed using IBM SPSS for Windows, version 29.
A logistic regression was conducted, in which the type of treatment served as the dependent variable, while maternal age, parity, history of TOA, and bilateral or unilateral TOA, served as independent variables.
Results
The research was based on data from 873 women diagnosed with PID. During this period, 208 (23.82%) were diagnosed with TOA. The final study cohort included 144 (69.23%) women who met the strict inclusion criteria, of whom, 78 (54.2%) were treated for unilateral TOA and 66 (45.8%) for bilateral TOA (Fig. 1).

Study flow diagram. Flow diagram demonstrating the cohort included for analysis. We included 873 women for analysis who were admitted with PID, 208 of whom were diagnosed with TOA. Only 144 who met the strict criteria were included in the final cohort. Among them, 78 (54.2%) were diagnosed with unilateral TOA and 66 (45.8%) with bilateral TOA.
Baseline demographics of age, marital status, gravity, parity, or comorbidities did not differ significantly between groups (Table 1).
Table 2 shows the prevalence of several risk factors in the groups, including history of abdominal surgery, smoking, contraception, history of PID, and number of PID episodes. Neither unilateral nor bilateral TOA had a significantly increased association with prior abdominal surgery, smoking, or contraception use. However, the results revealed a trend that those with bilateral TOA were more likely to have a history of PID than those with unilateral TOA (35.9% vs. 24.7%, respectively; p = 0.074).
Table 3 shows that women who were diagnosed with bilateral TOA were more likely to undergo surgical treatment than those diagnosed with unilateral TOA (56.9% vs. 42.3%, respectively; p = 0.04). There was no difference in of the size of the TOA between groups.
Multivariant logistic regression analysis found bilateral TOA was independently associated with surgical intervention(OR 2.5 (95% CI 1.17–5.29), p < 0.017).
Discussion
Many efforts to characterize the predictive factors of whether to treat TOA with surgery as opposed to antibiotics alone, are underway. Markers of the TOA such as unilateral or bilateral involvement and size, as well as information about the patient, such as age and severity of inflammation, have traditionally been used as a guide for treatment. In this study, we evaluated the implications of one parameter in particular: unilateral or bilateral involvement, to observe its potential role in determining treatment and its correlation to certain risk factors.
We found a trend that showed a greater need for surgical treatment in women diagnosed with bilateral TOA in comparison to unilateral TOA, similar to the findings reported in previous research [20].
We did not observe a difference in the size of the abscess between those treated for unilateral compared to bilateral abscesses. This finding differs from several previous studies that reported a positive correlation between abscess size and need for surgical intervention [20, 25, 26, 31]. In fact, a study conducted by Levin et al., which attempted to build a novel risk assessment score to identify surgical indications for TOA, went as far as to suggest that abscess diameter was one of the strongest predictors of failed antibiotic treatment. Characteristics applied towards calculating the score included age, leukocyte count, abscess diameter, and presence of a bilateral abscess. Data revealed that age > 36 years at admission was associated with an odds ratio (OR) of 2.1, mean leukocytosis at admission > 16,000 mm3 with an OR of 2.2, and presence of a bilateral abscess with an OR 2.2. In comparison, ultrasonographic measurement of abscess diameter > 7 cm was associated with an OR of 3.6 [24]. In our study, however, unilateral or bilateral involvement was noted to be a better predictor of the type of intervention than the size of the TOA because size did not seem to differ between groups, whereas treatment methods did. It is important to note that the sample sizes in these studies were similar to those in the current study.
This information should be considered in clinical scenarios, as it could help physicians determine the most appropriate treatment for TOA and prevent unnecessary delays.
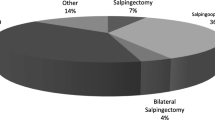
Despite the accepted practice of tailoring the surgical approach to the woman’s reproductive status, or unstable patients [32], there is a lack of understanding and consensus regarding the preferred procedure according to whether the abscess is unilateral or bilateral. The literature lacks clear guidance on the selection of a surgical approach, especially in the context of unilateral or bilateral TOA. While hysterectomy and bilateral sal**o-oophorectomy are recognized as definitive treatments, there is a knowledge gap regarding the extent of surgery needed for each case based on the surgical findings. There are various surgical interventions for treating TOA following failure of broad-spectrum antibiotics, as detailed in the Methods section. Drainage interventions can be guided by ultrasound or CT, while surgical procedures may involve unilateral or bilateral sal**ectomy, unilateral or bilateral sal**o-oophorectomy, and in some cases, hysterectomy but there are no specific guidelines [33] Our data show that drainage was more successful for unilateral TOA, while surgical procedures of all kinds required more often for patients with bilateral TOA. It is important to note that this study did not delve into determining a preferred surgical treatment method. Instead, it highlighted a correlation between whether the disease was unilateral or bilateral and the choice of surgical intervention.
There are several strengths to the current study. First, to the best of our knowledge it is the first study to investigate the differences between bilateral and unilateral TOA. In addition, we used strict diagnostic criteria, only selecting cases with a white blood cell count above 15,000 mm3, a formal CT or US scan showing TOA, and a documented body temperature above 38 °C. Moreover, the study was conducted at a single medical institution. Therefore, decisions for each case were based on the same protocols, which did not change over the study period.
The study is not without limitations. Some are inherent to the retrospective study design. The data were based on medical records, which implies that some data could have been erroneously input by physicians or overlooked during review. Additionally, previously documented risk factors for TOA and blood samples could not be measured as those data were missing from the electronic medical records. Moreover, the relatively small sample size limited us from fully studying and understanding the effects of bilateral TOA.
Conclusion
This retrospective study detected a trend toward more need for surgical treatment in women diagnosed with bilateral TOA and more successful outcomes with antibiotic treatment only among women with unilateral TOA.
It is plausible to consider that these findings may contribute to optimizing treatment decisions for TOA, potentially leading to a reduction in the duration of hospitalization, antibiotic exposure, and resistance. However, it is important to acknowledge that the results of the current study have limitations and further research is warranted to validate these potential outcomes.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CT:
-
Computed tomography
- OR:
-
Odds ratio
- PID:
-
Pelvic inflammatory disease
- PCR:
-
Polymerase Chain Reaction
- TOA:
-
Tubo-ovarian abscess
References
Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory Disease. N Engl J Med. 2015;372:2039–48.
Kim HY, Yang JI, Moon C. Comparison of severe pelvic inflammatory Disease, pyosalpinx and tubo-ovarian abscess. J Obstet Gynecol Res. 2015;41.
Beigi RH. Epidemiology, clinical manifestations, and diagnosis of tubo-ovarian abscess. Up to date. 2017.
Chappell CA, Wiesenfeld HC. Pathogenesis, diagnosis, and management of severe pelvic inflammatory Disease and tuboovarian abscess. Clin Obstet Gynecol. 2012;55.
Sordia-Hernández LH, Serrano Castro LG, Sordia-Piñeyro MO, Morales Martinez A, Sepulveda Orozco MC, Guerrero-Gonzalez G. Comparative study of the clinical features of patients with a tubo-ovarian abscess and patients with severe pelvic inflammatory Disease. Int J Gynecol Obstet. 2016;132.
Munro K, Gharaibeh A, Nagabushanam S, Martin C. Diagnosis and management of tubo-ovarian abscesses. Volume 20. The Obstetrician & Gynaecologist; 2018.
Ginsburg DS, Stern JL, Hamod KA, Genadry R, Spence MR. Tubo-ovarian abscess: a retrospective review. YMOB. 1980;138(7 Pt 2):1055–8.
Unemo M, Bradshaw CS, Hocking JS, de Vries HJC, Francis SC, Mabey D et al. Sexually transmitted Infections: challenges ahead. Lancet Infect Dis. 2017.
Global incidence and prevalence of selected curable sexually transmitted infections. 2008. Reprod Health Matters. 2012. https://doi.org/10.1016/s0968-8080(12)40660-7.
Centers for Disease Control. Sexually Transmitted Disease Surveillance. 2017. Centre of Disease Control and Prevention. 2017. https://doi.org/10.1016/j.molmet.2013.04.004.
Ross J, Guaschino S, Cusini M, Jensen J. 2017 European guideline for the management of pelvic inflammatory Disease. Int J STD AIDS. 2018. https://doi.org/10.1177/0956462417744099.
Romosan G, Valentin L. The sensitivity and specificity of transvaginal ultrasound with regard to acute pelvic inflammatory Disease: a review of the literature. Arch Gynecol Obstet. 2014;289.
Revzin Mv, Mathur M, Dave HB, Macer ML, Spektor M. Pelvic inflammatory Disease: multimodality imaging approach with clinical-pathologic correlation. Radiographics. 2016;36.
Curry A, Williams T, Penny ML. Pelvic inflammatory Disease: diagnosis, management, and prevention. Am Fam Physician. 2019;100.
Wiesenfeld HC, Hillier SL, Meyn LA, Amortegui AJ, Sweet RL. Subclinical pelvic inflammatory Disease and infertility. Obstet Gynecol. 2012;120.
McNeeley SG, Hendrix SL, Mazzoni MM, Kmak DC, Ransom SB, Levine E et al. Medically sound, cost-effective treatment for pelvic inflammatory Disease and tuboovarian abscess. In: Am J Obstet Gynecol. 1998. p. 1272–8.
Gjelland K, Ekerhovd E, Granberg S. Transvaginal ultrasound-guided aspiration for treatment of tubo-ovarian abscess: a study of 302 cases. Am J Obstet Gynecol. 2005;193:1323–30.
Granberg S, Gjelland K, Ekerhovd E. The management of pelvic abscess. Best Pract Res Clin Obstet Gynaecol. 2009;23:667–78.
Rosen M, Breitkopf D, Waud K. Tubo-ovarian abscess management options for women who desire fertility. Obstet Gynecol Surv. 2009;64.
Akselim B, Karaşin SS, Demirci A, Üstünyurt E. Can antibiotic treatment failure in tubo-ovarian abscess be predictable? Eur J Obstet Gynecol Reproductive Biology. 2021;258.
Yang CC, Chen P, Tseng JY, Wang PH. Advantages of open laparoscopic Surgery over exploratory laparotomy in patients with tubo-ovarian abscess. J Am Association Gynecologic Laparoscopists. 2002;9.
Bugg CW, Taira T. Pelvic inflammatory Disease: diagnosis and treatment in the Emergency Department. Emerg Med Pract. 2016;18.
Greenstein Y, Shah AJ, Vragovic O, Cabral H, Soto-Wright V, Borgatta L et al. Tuboovarian abscess: factors associated with operative intervention after failed antibiotic therapy. J Reprod Med. 2013;58.
Fouks Y, Cohen A, Shapira U, Solomon N, Almog B, Levin I. Surgical intervention in patients with tubo-ovarian abscess: clinical predictors and a simple risk score. J Minim Invasive Gynecol. 2019;26.
Hwang JH, Kim BW, Kim SR, Kim JH. The prediction of surgical intervention in patients with tubo-ovarian abscess. J Obstet Gynaecol (Lahore). 2022;42.
Chan GMF, Fong YF, Ng KL. Tubo-Ovarian Abscesses: Epidemiology and Predictors for Failed Response to Medical Management in an Asian Population. Infect Dis Obstet Gynecol. 2019;2019.
Halperin R, Levinson O, Yaron M, Bukovsky I, Schneider D. Tubo-ovarian abscess in older women: is the woman’s age a risk factor for failed response to Conservative treatment? Gynecol Obstet Invest. 2003;55:211–5. https://doi.org/10.1159/000072076.
Demirtas O, Akman L, Demirtas GS, Hursitoglu BS, Yilmaz H. The role of the serum inflammatory markers for predicting the tubo-ovarian abscess in acute pelvic inflammatory Disease: a single-center 5-year experience. Arch Gynecol Obstet. 2013;287.
Zhu S, Ballard E, Khalil A, Baartz D, Amoako A, Tanaka K. Impact of early surgical management on tubo-ovarian abscesses. J Obstet Gynaecol (Lahore). 2021;41.
Workowski KA. Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines. Clin Infect Dis. 2015;61.
Tugrul Ersak D, Ersak B, Kokanalı MK. The effect of intrauterine device presence and other factors in medical treatment success of tuboovarian abscess. J Gynecol Obstet Hum Reprod. 2021;50.
Landers DV, Sweet RL. Tubo-ovarian abscess: contemporary approach to management. Rev Infect Dis. 1983;5.
Lareau SM, Beigi RH. Pelvic inflammatory Disease and tubo-ovarian abscess. Infect Dis Clin N Am. 2008;22:693–708.
Acknowledgements
Not applicable.
Funding
The authors declare no funding.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Y.Y.: Conceptualized the project, Data collection, Project development, Data analysis, Manuscript writing. O.W.: Data analysis, manuscript editing. R.S.: manuscript editing. G.M.-E.: Data collection. Y.K.: Manuscript editing. Z.K.: Data analysis, Manuscript editing. Y.D.: Data analysis, Manuscript writing. R.S.: Data analysis, Manuscript editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in accordance with the principles of the Declaration of Helsinki. All methods were carried out in accordance with relevant guidelines and regulations. All experimental protocols were approved by the Meir Medical Center Ethics Committee, approval number MMC-082-17. Due to the retrospective nature of the study, Meir Medical Center Ethics Committee has waived need for informed consent statement.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yagur, Y., Weitzner, O., Shams, R. et al. Bilateral or unilateral tubo-ovarian abscess: exploring its clinical significance. BMC Women's Health 23, 678 (2023). https://doi.org/10.1186/s12905-023-02826-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12905-023-02826-x