
Abstract
Background
Knowledge on oral health-related quality of life (OHRQoL) in children and adolescents with juvenile idiopathic arthritis (JIA) is limited, and longitudinal studies are lacking. We aimed to describe OHRQoL in children and adolescents with JIA compared to controls, and to explore the validity and internal consistency of the Early Childhood Oral Health Impact Scale (ECOHIS) and the Child Oral Impact on Daily Performance (Child-OIDP). Furthermore, we wanted to investigate associations between OHRQoL and orofacial pain, physical health, disease activity, and temporomandibular joint (TMJ) involvement in JIA.
Methods
The Norwegian prospective, multicenter cohort study recruited participants with JIA between 4 and 16 years of age and corresponding controls from three pediatric university hospital departments and public dental health services. In the present study, we analyzed OHRQoL in all children < 12 years with the ECOHIS and adolescents ≥ 12 years with the Child-OIDP at the first visit and the two-year follow-up. Associations between OHRQoL and JIA characteristics, collected in clinical exam and questionnaires, were analyzed in logistic regressions.
Results
The same OHRQoL questionnaire was completed both at first visit and two-year follow-up in 101 children < 12 years (47 JIA, 54 controls) and 213 adolescents ≥ 12 years (111 JIA, 102 controls). The frequency of OHRQoL impacts in children was similar at the first visit and the two-year follow-up (ECOHIS > 0: JIA group 81% and 85%, p = 0.791; control group 65% and 69%, p = 0.815), while adolescents with JIA reported fewer impacts at the two-year follow-up (Child OIDP > 0: JIA group 27% and 15%, p = 0.004; control group 21% and 14%, p = 0.230). The internal consistency of the OHRQoL instruments was overall acceptable and the criterion validity indicated that the instruments were valid at both visits. Orofacial pain was more frequent in children and adolescents with JIA than in controls. We found associations between OHRQoL impacts and orofacial pain, impaired physical health, disease activity, and TMJ involvement.
Conclusions
Children and adolescents with orofacial pain or impaired physical health were more likely to report impacts on daily life activities than those without. Pediatric rheumatologists and dentists should be aware of impaired OHRQoL in individuals with JIA with active disease or temporomandibular joint involvement.
Trial registration
Registered on clinicaltrials.gov (NCT03904459, 05/04/2019).
Similar content being viewed by others


Background
Children and adolescents with juvenile idiopathic arthritis (JIA) have a chronic rheumatic disease with onset before the age of 16 years and several different characteristics and symptoms due to joint inflammation [1]. In Norway the annual incidence rate is between 14 and 23 per 100,000 under 16 years of age, which is somewhat higher than corresponding rates from other geographical regions, but comparable to other Scandinavian countries [2,3,4,5]. Despite the increasing availability of biologic disease-modifying antirheumatic drugs in recent decades, there is still a substantial proportion of patients with active disease in long-term follow-up of JIA cohorts [6, 7]. Children and adolescents with JIA report a significant impairment of health-related quality of life (HRQoL) with impacts on daily functioning both at home and in school settings [8, 9].
Oral health is not only the absence of pathological findings in the oral cavity but should incorporate the patient’s perceptions, such as “the ability to speak, smile, smell, taste, touch, chew, swallow, and convey a range of emotions through facial expressions with confidence and without pain, discomfort, and disease of the craniofacial complex” [10], in other words, the patient’s oral health-related quality of life (OHRQoL). Research regarding OHRQoL in children and adolescents with JIA is limited and needs further exploration [11]. A small study on oral health and OHRQoL reported no differences in OHRQoL in children and adolescents with JIA, compared to controls [12], while three recent studies on orofacial symptoms [13, 14] and TMJ arthritis [15] found that self-reported orofacial symptoms and TMJ arthritis have a negative impact on OHRQoL [13, 15]. One study found that 22% of the children and adolescents were severely impacted by orofacial symptoms and dysfunction [14]. To our knowledge there is no longitudinal study on OHRQoL in JIA.
Temporomandibular joint (TMJ) arthritis is a common finding in children and adolescents with JIA that can occur throughout the disease course [9, 16, 17]. Arthritis in the TMJ may lead to severe craniofacial growth disturbances, functional problems, and pain in the orofacial region, which may impact overall oral health [18, 19]. There is limited research on oral health in children and adolescents with JIA, and the findings are divergent [11]. Dental plaque and gingival bleeding, as an indicator of gingival inflammation, are more commonly reported clinical findings in children and adolescents with JIA than in controls [11, 20, 21]. Caries prevalence does not significantly differ in children with and without JIA, according to recent reports [11, 22].
In order to improve the OHRQoL in children and adolescents with JIA, it is important that both dental and medical practitioners are aware of the implications of JIA on both OHRQoL and the family dynamics [23, 24]. Thus, the overall aim of this study was to gain further knowledge on such implications.
In detail, the aims of this study were first to describe oral health-related conditions and OHRQoL in a cohort of children and adolescents with JIA compared to controls without JIA at the time of inclusion (the first visit) and after two years (the two-year follow-up). Secondly, to explore the internal consistency and validity of the Early Childhood Oral Health Impact Scale (ECOHIS) and the Child Oral Impact on Daily Performance (Child-OIDP) in our JIA cohort. Thirdly, to investigate associations between OHRQoL and orofacial pain and impaired physical health among children and adolescents with and without JIA; and fourthly, to investigate associations between OHRQoL and disease activity and TMJ involvement in the JIA cohort.
Methods
Study design and population
This study is part of the Norwegian JIA study (NorJIA, www.norjia.com). NorJIA is a prospective, longitudinal multicenter cohort study with a comparative design. We collected data at the first visit and after two years in 224 children and adolescents with JIA and a corresponding control group without JIA between April 2015 and October 2020. At the university hospitals in Bergen, Trondheim, and Tromsø, pediatric rheumatologists invited participants diagnosed with JIA according to the International League of Associations for Rheumatology (ILAR) criteria [25]. The control group, children and adolescents without JIA listed for routine examination in public dental health service care, were recruited from both rural and urban areas; the University Dental Clinic in Bergen, Public Dental Health Clinics in and around Bergen (Western Norway), the Public Dental Health Clinic in Stjørdal (Central Norway) and the University Dental Clinic in Tromsø (Northern Norway). They were matched 1:1 at each center to the participants with JIA, according to age and gender. Both at the time of inclusion (the first visit) and after two years (the two-year follow-up) the participants underwent the same examinations and answered the age-appropriate questionnaires. All questionnaires were completed either before the oral examination or closely after the examination with a maximum of two reminders. This report includes the children and adolescents who answered the same OHRQoL instrument at both visits. The sample size calculation for our cohort was based on caries estimates described by Gil et al. [22].
Oral health questionnaire
Adolescents ≥ 12 years of age and parental proxies of children younger than 12 years completed a questionnaire including sociodemographic data and oral health information. For this report, we dichotomized the educational level of caregivers (university/college = 0, primary school/high school = 1), the number of caregivers (two caregivers = 0, one caregiver = 1), the frequency of toothbrushing (twice a day or more = 0, less than twice a day = 1) and use of dental floss (several times weekly or more = 0, less than several times weekly = 1), self-reported clinical signs such as gingival bleeding during toothbrushing (never = 0, sometimes or more = 1), pain or discomfort during tooth brushing (no = 0, yes = 1), and the frequency of intraoral ulcerations (less than once a year = 0, several times yearly = 1). The original and new codes are presented in the supplemental material (Supplemental, Additional file S1, Table 1).
Oral examinations
The oral examinations were carried out by six experienced dentists, who underwent training and calibration exercises both before and during the study period, as described by Gil et al. [20, 22]. Caries, at both the enamel and dentin levels (d1-5f /D1-5F), was diagnosed on all five surfaces of the second primary or the first permanent molars by visual inspection and on bitewing radiographs as described elsewhere [22] and were dichotomized as 0 = absent (d1-5f/D1-5F = 0) or 1 = present (d1-5f /D1-5F > 0). The missing component was not included in the d1-5f /D1-5F- index due to only a few missing teeth. For adolescents, supragingival debris and calculus were measured according to the Simplified Oral Hygiene Index (OHI-S) by Greene and Vermillion [26] and gingival bleeding was assessed according to the Gingival Bleeding Index (GBI) by Ainamo and Bay [27] modified as described elsewhere [20]. The OHI-S was dichotomized to 0 = good oral hygiene, representing approximately 33% of the participants with the lowest plaque and calculus scores (OHI-S cut off 0.5) and 1 = moderate to poor oral hygiene with OHI-S ≥ 0.5. The GBI was dichotomized with a cutoff of 10% bleeding: 0 = no or less than 10% bleeding points and 1 = 10% or more bleeding points.
Early childhood oral health impact scale (ECOHIS)
To assess the impacts of oral health problems on quality of life in children (defined as participants < 12 years of age in this report), we used the ECOHIS, a questionnaire with 13 items answered by a parental proxy [28], previously validated in a general local population of Norwegian children [29]. The response options were recoded on a Likert scale with scores from 0 = never to 4 = very often (Supplemental, Additional file S1, Table 2), where missing single items were replaced by the mean score of the section. Questionnaires with more than two missing items in the child section or more than one missing item in the family section were excluded as described elsewhere [28, 30, 31]. The scores on the 13 items were added to the total ECOHIS additive (ADD) score (range 0—52). To calculate changes in OHRQoL over time, the two-year follow-up score was subtracted from the first visit score, forming the ECOHIS change ADD score, where negative values indicated worsened and positive values improved precepted oral health at the two-year follow-up [32]. Additionally, the score from the first visit and the two-year follow-up was dichotomized to 0 = no impacts and 1 = ADD score > 0 when at least one ECOHIS item was affected.
Child oral impact on daily performance index (Child OIDP)
For adolescents (defined as participants ≥ 12 years of age in this report), OHRQoL was assessed using the Child-OIDP [33], an eight-item instrument adapted from the adult OIDP inventory [34] and validated in a general local population of Norwegian adolescents [29]. The adolescent was asked by the dentist, prior to the oral examination, whether each of the eight daily activities was affected by problems with their teeth or mouth during the last three months. The response options were coded on a Likert scale with the original scores never = 0, once or twice a month = 1, once or twice a week = 2, and every day/almost every day = 3. The eight scores were added to the Child-OIDP ADD score (range 0—24). The ADD score was dichotomized to 0 = no impacts and 1 = at least one impact in the last three months. A Child-OIDP change ADD score was calculated as described for the ECOHIS.
Global oral health outcomes as reported by adolescents and parental proxies
Adolescents and parental proxies of children were asked to rate their/their child’s dental health and tooth appearance. They were asked, “How would you rate your dental health?”. The response options were coded on a five-point Likert scale and dichotomized into good = 0 including the original responses very good and good (scores 1 and 2) and poor = 1 including neither nor, poor, and very poor (scores 3–5). Second, they were asked, “How satisfied are you with the appearance of your teeth?”. The five response options were dichotomized into satisfied = 0 including very satisfied and satisfied (scores 1 and 2) and unsatisfied = 1 including neither nor, unsatisfied, and very unsatisfied (scores 3–5).
Orofacial pain
In accordance with the international consensus-based recommendations for orofacial assessment in patients with JIA [35], all participants were asked during the orofacial examination visits, if they ever had pain in their jaw, temple, ear, or in front of the ear on at least one side. Those answering “yes” were also asked, which of the three alternatives best described a possible pain in one of the regions during the last 30 days. The three answer options were dichotomized to no pain = 0 (the original answer no pain) and pain = 1 including pain comes and goes and pain all the time.
Child health questionnaire
The parent-administered Norwegian version of the child health questionnaire (CHQ-PF50) [36] is a generic measure of the physical and psychosocial health of children and adolescents [37]. The CHQ physical summary score (PhS) ranges from 0–100 (mean 50, SD ± 10), with higher scores indicating a better status and health [37, 38]. The PhS was dichotomized as 0 = normal with scores ≥ 40 and 1 = impaired with scores < 40, accordingly more than one SD lower than the mean of the US norm population [37].
JIA characteristics
The pediatric rheumatologists collected clinical characteristics, including age at disease onset, disease duration, JIA category according to the ILAR criteria, the number of active joints, the cumulative number of affected joints, and previous and current disease-modifying antirheumatic drugs (DMARDs). Additionally, the pediatric rheumatologists rated the JIA disease activity on a visual analog scale (VAS) from 0–10 (MDgloVAS: 0 = “no activity”, 10 = “high activity”). The patients (children ≥ 9 years) or proxies (children < 9 years) reported functional ability in the Childhood Health Assessment Questionnaire (CHAQ), as well as the disease impact on overall wellbeing (PRgloVAS) and pain during the last week on a VAS (range 0–10, 0 = “no influence”/”no pain” and 10 = “severely influenced”/ “severe pain”). MDgloVAS, PRgloVAS, and global pain reports were dichotomized to “0″ for those with a rating of 0 and “1″ for ratings > 0 on the VAS scale. We analyzed C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). The juvenile arthritis disease activity score (JADAS71) was calculated based on the MDgloVAS, the PRgloVAS, the active joint count, and the ESR (CRP with missing ESR), as appropriate [39]. For analysis, we dichotomized to 0 = JADAS < 1 and 1 = JADAS ≥ 1 as an indicator for active disease for all JIA categories. Former clinical TMJ involvement and clinical TMJ involvement at the study visits were registered by the pediatric rheumatologists based on the best judgment of all available information, including symptoms, clinical examination, and radiologic evaluation up to the study visit [40].
Statistical methods
All statistical analyses were conducted using STATA version 17 software (STATA Corp., College Station, Texas, USA). Means, 95% confidence intervals, medians, interquartile ranges, and frequencies were reported for descriptive data. Chi-squared- and Fisher’s exact-test were applied, to evaluate differences in frequencies of OHRQoL impacts between groups at one timepoint. Mann–Whitney U-tests were applied, to evaluate differences of OHRQoL mean ADD scores between groups. McNemar’s test and Wilcoxon signed-rank test were used, to assess change within the frequencies of OHRQoL impacts and OHRQoL mean ADD scores in the respective group over time. Effect sizes for the OHRQoL mean ADD scorers were calculated for differences between JIA and control group at one timepoint by Cohen’s d for two independent samples using groups (JIA/Controls):
For differences between first visit and two-year follow-up within one group Cohen’s d was calculated according to the following formula:
Effect sizes of ≤ 0.2 were considered small, > 0,2 and ≤ 0.5 medium and ≥ 0.8 large [41].To assess the internal consistency reliability of the two OHRQoL instruments, we used Cronbach’s alpha, and to assess the validity, we compared the mean OHRQoL ADD scores according to the two categories of global oral health outcomes (“good” vs. “poor oral health” and “satisfied” vs. “unsatisfied with tooth appearance”, Mann–Whitney U-test). To assess the longitudinal validity of the OHRQoL instruments, we evaluated the association between OHRQoL change ADD scores and change in the category of the reference variables, in terms of the global oral health outcomes and self-reported clinical signs, using one-way ANOVA and Bonferroni post hoc test. To analyze associations between OHRQoL and orofacial pain, impaired overall physical health, JIA disease activity, and TMJ involvement, we applied logistic regression both unadjusted and adjusted for age, gender, parental educational level, and group affiliation (JIA/Controls).
Results
Study population
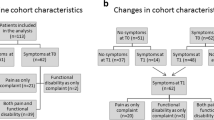
Of the 360 invited patients with JIA and 294 controls, the 47 children and 111 adolescents with JIA and 54 children and 102 adolescents without JIA, who completed the same OHRQoL instrument at both visits, were included in this study (Fig. 1). The distribution of sociobehavioral characteristics, parent/patient-reported oral symptoms, and clinical oral findings among children (< 12 years of age) and adolescents (≥ 12 years of age) are presented in Tables 1 and 2, respectively, together with JIA disease characteristics for the JIA group only.

Flow diagram of participating children and adolescents with juvenile idiopathic arthritis (JIA) and controls
Dropout analyses, performed separately for children and adolescents with and without JIA, are presented in the supplementary files (Supplemental, Additional file S2, Tables 1 and 2). Children, included in this study, were significantly younger than those, who were lost to follow-up or excluded. For adolescents, this age difference was only significant in the JIA group. Additionally, adolescents with JIA, who were lost to follow-up, had significantly more caries at the D1-5F-level than those who participated in the two-year follow-up.
We found similar sociodemographic and behavioral characteristics in both the JIA and control group, except for lower paternal educational levels in adolescents with JIA than in controls (university/college education in 39.6% vs. 63.2%, p < 0.001). When controlling the association between OHRQoL impacts > 0 and JIA group affiliation (JIA/no JIA) for the parental educational level, we did not find significant changes in the results (ordinal logistic regression, results not shown).
Oral health related conditions and OHRQoL
Compared to controls, more children with JIA reported oral ulcerations at least several times a year at the first visit, and pain or discomfort during toothbrushing at the two-year follow-up (Table 1). In the clinical examination, we found significantly more adolescents with JIA who had moderate to poor oral hygiene than controls at the first visit, and significantly more adolescents with JIA than controls who presented with gingival bleeding at the two-year follow-up (Table 2).
More than 80% of the children with JIA and more than 60% of the controls reported negative OHRQoL impacts (ECOHIS > 0), as shown together with the mean ECOHIS ADD scores for the JIA and control group in Table 3. We found higher mean ECOHIS ADD scores for children with JIA both at the first visit and the two-year follow-up with moderate effect sizes (ES 0.48 and 0.53, Table 3). The ECOHIS ADD scores for the first visit and the two-year follow-up did not differ significantly either in the JIA group or in the control group (Table 3). We did not find gender differences in frequencies or mean ADD scores for children with or without JIA (results not shown). When analyzing and comparing each separate item, more children with JIA reported difficulty eating some foods compared to the children in the control group at the first visit (31.9% vs. 13.0%, p = 0.021, results not shown). At the two-year follow-up, more children with JIA reported having pain in their teeth, mouth, or jaw compared to children in the control group (74.5% vs. 51.9%, p = 0.019). Additionally, more children with JIA reported having missed preschool or school because of dental problems or treatments (38.3% vs. 11.1%, p = 0.001).
The frequencies for Child OIDP > 0 and the mean ADD scores are presented in Table 3. More adolescents with JIA reported negative impacts on daily performance at the first visit than at the two-year follow-up (27.0% and 15.3%, respectively, p = 0.004). Stratified by gender, we found that girls with JIA more commonly reported Child OIDP > 0 than boys with JIA (42% and 9% respectively, p < 0.001) and girls without JIA (21%, p = 0.018) at the first visit but not at the two-year follow-up (results not shown). Adolescent girls with JIA had a higher mean Child OIDP ADD score than adolescent boys with JIA (first visit: 1.76 and 0.46, respectively, p < 0.001, two-year follow-up: 0.81 and 0.21, p = 0.032) and girls without JIA at the first visit (first visit: 0.52, p = 0.008, two-year follow-up: 0.38, p = 0.444). We did not find this difference when comparing boys with and without JIA. The mean Child OIDP ADD scores for both the JIA and control group were significantly lower at the two-year follow-up, with a low effect size (Table 3). When analyzing and comparing each separate item, problems with eating were reported by more adolescents with JIA than by adolescents in the control group (19.8% and 9.8% respectively, p = 0.041) at the first visit (results not shown). There was no significant difference between adolescents in the JIA and the control group according to any other item at either of the study visits.
Internal consistency and validity of the ECOHIS and Child OIDP
The total ECOHIS scale showed good internal consistency for the JIA group (Cronbach’s alpha = 0.82 at both visits) and acceptable internal consistency for the control group (Cronbach’s alpha = 0.77 at the first visit and 0.74 at the two-year follow-up) (Supplemental, Additional file S3, Table 1). At both visits we found lower mean ECOHIS ADD scores for participants with ratings of “good” oral health and satisfaction with tooth appearance, and correspondingly higher scores when ratings of oral health were poor and there was dissatisfaction with tooth appearance (Table 4). The ECOHIS change ADD scores were small in both the JIA and control group and only correlated with changes in the global oral health outcomes for children with JIA (Supplemental, Additional file S3, Table 2).
The internal consistency reliability (Cronbach’s alpha) of the Child OIDP inventory was 0.77 for the JIA group and 0.73 for the control group at the first visit and 0.69 and 0.65, respectively, at follow-up (Supplemental, Additional file S3, Table 1). The first visit and two-year follow-up mean Child OIDP ADD scores were lower for those rating oral health as good and were satisfied with their tooth appearance, while the scores were higher for those rating oral health as poor or were unsatisfied with their tooth appearance (Table 4). The Child OIDP change ADD scores were small and did not correlate with changes in the patient-rated overall oral health and tooth appearance (Supplemental, additional file S3, Table 2).
Associations between OHRQoL and orofacial pain, and impaired physical health,
Significantly more children and adolescents with JIA reported orofacial pain than controls at both visits (Tables 1 and 2).In the group of children under 12 years of age, all children who reported orofacial pain also reported at least one negative impact on OHRQoL at follow-up (Table 5). Independent of group affiliation, adolescents with orofacial pain were more likely to report negative OHRQoL impacts than those without orofacial pain (Table 6). Children and adolescents reporting orofacial pain had higher mean OHRQoL ADD scores (Supplemental, additional file S4, Table 1). These results were significant for children with and without JIA at the two-year follow-up and for adolescents with JIA both at the first visit and at the two-year follow-up.
There were no significant associations between negative OHRQoL impacts and impaired physical health in children with JIA. Adolescents with JIA and impaired physical health had significantly higher odds of having at least one negative OHRQoL impact at the two-year follow-up (adjusted logistic regression, OR 5.1, 95% CI 1.2–20.8), as shown in Table 6. The mean Child OIDP ADD scores for adolescents with JIA and impaired physical health were higher both at the first visit and the two-year follow-up (Supplemental, additional file S4, Table 2).
Associations between OHRQoL and JIA disease activity and TMJ involvement
The mean OHRQoL ADD scores were higher for children and adolescents with active disease (JADAS71 ≥ 1). The differences in ECOHIS and Child OIDP add scores according to disease activity were significant only at the first visit (Supplemental, additional file S4, Table 3). Among adolescents, we found significantly higher odds for negative OHRQoL impacts in individuals with active disease (OR 5.1, 95% CI 1.3–19.6) at the first visit, as presented in Table 6.
All children with JIA and clinical TMJ involvement had at least one negative impact on OHRQoL (ECOHIS > 0) at the first visit (Table 5). Adolescents with JIA and TMJ involvement had significantly higher odds of reporting negative impacts on OHRQoL at the first visit (OR 8.5 95% CI 2.0–37.0), but this association was not found at the two-year follow-up (Table 6).
Discussion
In this longitudinal multicenter study focusing on children and adolescents with JIA, we found that there are differences in oral health and OHRQoL between participants with and without JIA. Children with JIA reported pain or discomfort during toothbrushing and ulcerations more often than controls. Orofacial pain was also most frequent in children and adolescents with JIA. Furthermore, moderate to poor oral hygiene and gingival bleeding were more common among adolescents with JIA than among those without JIA. Children with JIA had higher OHRQoL mean ADD scores than children without JIA. There were no significant differences in frequencies of negative OHRQoL impacts or in OHRQoL mean ADD scores in adolescents with and without JIA. Testing for longitudinal validity, the OHRQoL change ADD scores were small in both the JIA and control group, and correlated only with changes in the global oral health outcomes for children with JIA. We found associations between negative OHRQoL impacts and orofacial pain, impaired physical health, active JIA disease, and TMJ involvement.
A strength of this study is the longitudinal study design and the included age- and gender-matched control group. It is difficult, to define the right interval for a longitudinal study on children and adolescents with such a wide age span, since changes in children can appear quickly in certain time periods of cognitive development and growth. Rahimi et al. [13] reported persistency of orofacial symptoms in a two-year follow-up of adolescents with JIA, and we found this interval sufficient for the NorJIA study. An additional strength of the study is the use of standardized and validated protocols and age-appropriate questionnaires. Furthermore, we conducted calibration exercises among the dental examiners both before and during the study period. Another strength of the NorJIA study is the multidisciplinary collaboration of the medical and dental specialists, that increases the knowledge beyond the individual specialists’ fields and hopefully lead to a more comprehensive understanding of the disease and a better treatment.
A limitation of this study is the small number of participants in the group of children < 12 years. Approximately half of the children could not be included since they changed age group and reported OHRQoL in the Child OIDP instead of the ECOHIS at the two-year follow-up. Hence, the sample size is low for some analyses for subgroups of our study population. An additional limitation regarding the ECOHIS questionnaire is the different timing of completion; some parents completed the questionnaire after the examination. Another limitation of this report is the assessment of TMJ involvement, that was based on the best judgment of the pediatric rheumatologist without MRI scoring available.
To our knowledge, NorJIA is the first study that applied the ECOHIS and the Child OIDP inventory in a follow-up study of children and adolescents with JIA. While most of the children reported negative impacts on OHRQoL (ECOHIS > 0), less than one-third of adolescents reported oral impacts on daily life activities (Child OIDP > 0). A higher frequency of negative OHRQoL impacts in children than in adolescents was also found in a previous Norwegian study, where ECOHIS and Child OIDP inventories were used in a general local population of children and adolescents [29]. Importantly, the ECOHIS and Child OIDP instruments are not directly comparable since the Child OIDP addresses impacts experienced during the last three months, while ECOHIS items are reported with no time limit. To be able to compare our results with prior publications, we chose to use the same methods of dichotomization of the ECOHIS instrument as previous Norwegian studies. Thus, the severity of the impacts on the child’s quality of life can be discussed if the impact occurred “hardly ever”. This must be taken into account, when evaluating the high number of children with impacts.
We found no differences in the number of participants that reported negative impacts on OHRQoL in the JIA group compared to controls, but we found a significantly higher mean ECOHIS ADD score for children with JIA with a moderate effect size at both visits. These findings may indicate, that children with JIA have several negative impacts or have impacts more often than children without JIA. In contrast, Santos et al. [12] reported no difference in mean OHRQoL scores in a study on 17 children and adolescents with JIA and 15 controls using the short form of the Brazilian Parental-Caregiver Perception Questionnaire. While we found, that the OHRQoL in children was stable over time, fewer adolescents had negative impacts on daily performance at the two-year follow-up compared to the first visit. In a review, Alvarez et al. [42] found lower Child OIDP scores in studies carried out in groups of older adolescents compared to studies with younger cohorts. The lower frequency of reported negative impacts in adolescents at the two-year follow-up in our study may thus be related to increased age. There were no significant changes in oral health in terms of other reported orofacial symptoms or clinical findings such as caries or gingival bleeding. However continuous medical treatment and multidisciplinary follow up may have contributed to less negative OHRQoL impacts.
The reliability in terms of internal consistency for the total ECOHIS scale was good at the first visit and acceptable at the two-year follow-up. For the Child OIDP scale, the internal consistency was acceptable at the first visit but somewhat lower than the accepted range for the two-year follow-up [43]. The Child OIDP inventory has only eight items. The low number of items in a scale can affect Cronbach’s alpha and lead to an underestimation of the reliability in short scales [43]. A recent reliability generalization meta-analysis of the Child OIDP questionnaire showed that a majority of publications reported a Cronbach’s alpha of ≥ 0.7, and they found that age and gender have a significant effect on the overall estimate [44].
Testing for criterion validity, we found higher mean ECOHIS and Child OIDP ADD scores in relation to the global reference outcomes “poor oral health” and “unsatisfied with tooth appearance”, indicating that both OHRQoL instruments are valid at both visits. Assessing the longitudinal validity of the ECOHIS and Child OIDP in our study cohort, most of the children and adolescents were stable in their category for the global oral health outcomes, and the mean change ADD scores for ECOHIS and Child OIDP were low. Only a few participants had a worsened or improved global rating of oral health and tooth appearance, and in both groups were as well participants that had negative and positive change scores. The same problem was described by Locker et al., testing the responsiveness of the oral health impact profile [32]. Intervention studies on early childhood caries that applied the ECOHIS instrument found mild to moderate changes in the ADD scores after treatment [30, 31, 45]. As the present NorJIA study is an observational study without major interventions on oral health, significant changes were not expected. Mashoto et al. [46] used the Child OIDP instrument in a study on Tanzanian children that underwent caries treatment. They described flooring effects where 63% of the total group and 50% of the treated participants had a zero score at baseline [46]. In our study, the frequency of adolescents without negative oral impacts on daily activities was even higher with approximately 70% of the adolescents with JIA and 80% of controls. This flooring effect may additionally limit the sensitivity of the Child OIDP to changes in the global oral health categories.
We found higher OHRQoL ADD scores for children and adolescents with orofacial pain, impaired physical health, or active JIA disease. Leksell et al. concluded in a study of 41 patients with JIA and 41 controls that symptoms from the orofacial area were more common in the JIA group and impacted daily life to a high extent [14]. Comparable results were found in a more recent two-year prospective observational study of 157 Danish children with JIA. Rahimi et al. applied the Child Perceptions Questionnaire (a 31-item questionnaire on OHRQoL) at the two-year follow-up and found that orofacial pain and functional disability significantly reduced OHRQoL [13]. Although these studies are not directly comparable due to different study designs, they support our results that orofacial pain correlates with increasing negative impacts on OHRQoL in children and adolescents.
Adolescents with JIA and impaired physical health had significantly more negative impacts on OHRQoL than those with normal physical health. Two cross-sectional studies on associations between OHRQoL and general HRQoL in mainly adult populations indicate that OHRQoL has some impact on HRQoL and that low HRQoL can be an indicator of impaired oral health [47, 48]. We found no comparable studies of associations between OHRQoL and HRQoL in children and adolescents. Analyzing the whole first-visit JIA cohort of the NorJIA study (JIA, n = 221), Gil et al. reported a higher risk for negative impacts on daily activities in adolescents with JIA and continued disease activity or flare [49]. In our report which included 111 of the 125 adolescents with JIA and 47 of the 96 children with JIA, we analyzed the associations between the OHRQoL ADD scores and the JADAS71 score, a composite measure for disease activity. We found similar associations as Gil et al. with significantly higher mean ECOHIS and Child OIDP scores in the participants with active disease (JADAS ≥ 1) at the first visit. However, the mean OHRQoL scores for participants with and without active disease did not differ significantly at the two-year follow-up.
At the first visit children and adolescents with JIA and TMJ involvement had higher odds for negative OHRQoL impacts than those without TMJ involvement. Clinical findings as active TMJ arthritis orofacial pain or dysfunction were treated according to the clinical protocols between first visit and two-year follow-up. The treatment could involve adjustment of the systemic medication in cases of active TMJ arthritis, information and physical exercises or splint therapy in cases of orofacial pain or dysfunction. The individually tailored multidisciplinary treatment may explain, that we did not find significantly higher odds for negative OHRQoL impacts in participants with TMJ involvement and JADAS > 1 at the two year follow up (24).
Conclusions
Our cohort study found differences in the oral health and OHRQoL of children and adolescents with JIA compared to controls. Children and adolescents with orofacial pain were more likely to report negative oral health-related impacts on daily life activities than those without pain. We found an association between impaired OHRQoL and active disease (JADAS ≥ 1), impaired physical health, and TMJ involvement. Adolescent girls with JIA reported negative OHRQoL impacts more often than both boys with JIA and girls without JIA. Future research should identify and explore OHRQoL instruments that may better capture the OHRQoL impacts in children and adolescents with JIA. Pediatric rheumatologists and dental specialists should give attention to children and adolescents reporting impaired physical health, high disease activity, orofacial pain, and TMJ involvement in JIA and cooperate closely to optimize normal daily life activities and functioning.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- ADD:
-
Additive
- Child-OIDP:
-
Child oral impact on daily performance
- CHQ-PF50:
-
50 Items parent administered version of the child health questionnaire
- CI:
-
Confidence interval
- CRP:
-
C-reactive protein
- d1-5f/ D1-5F:
-
Caries on enamel and dentin level in primary/permanent teeth
- ECOHIS:
-
Early childhood oral health impact scale
- ES:
-
Effect size
- ESR:
-
Erythrocyte sedimentation rate
- GBI:
-
Gingival Bleeding index
- HRQoL:
-
Health related quality of life
- ILAR:
-
The International League of Associations for Rheumatology
- JADAS:
-
Juvenile arthritis disease activity score
- JIA:
-
Juvenile idiopathic arthritis
- MDgloVAS:
-
The pediatric rheumatologist’s global assessment of disease activity
- NorJIA:
-
Norwegian JIA Study
- OHI-S:
-
Simplified Oral Hygiene Index
- OHRQoL:
-
Oral health related quality of life
- OR:
-
Odds ratio
- PhS:
-
Physical score of the CHQ-PF50
- PRgloVAS:
-
Patients/parents global rating of the diseases influence on wellbeing
- SD:
-
Standard deviation
- TMJ:
-
Temporomandibular joint
- VAS:
-
Visual analog scale
References
Månsson B. Etiologi og patogenes vid juvenil idiopatisk artrit. In: Hagelberg S, Andersson-Gaere B, Fasth A, Månsson B, Enman Y, editors. Barnreumatologi 2008. p. 35–7.
Moe N, Rygg M. Epidemiology of juvenile chronic arthritis in northern Norway: a ten-year retrospective study. Clin Exp Rheumatol. 1998;16(1):99–101.
Riise OR, Handeland KS, Cvancarova M, Wathne KO, Nakstad B, Abrahamsen TG, et al. Incidence and characteristics of arthritis in Norwegian children: a population-based study. Pediatrics. 2008;121(2):e299–306.
Berntson L, Andersson Gare B, Fasth A, Herlin T, Kristinsson J, Lahdenne P, et al. Incidence of juvenile idiopathic arthritis in the Nordic countries. A population based study with special reference to the validity of the ILAR and EULAR criteria. J Rheumatol. 2003;30(10):2275–82.
Thierry S, Fautrel B, Lemelle I, Guillemin F. Prevalence and incidence of juvenile idiopathic arthritis: a systematic review. Joint Bone Spine: revue du rhumatisme. 2014;81(2):112–7.
Glerup M, Herlin T, Twilt M. Clinical outcome and long-term remission in JIA. Curr Rheumatol Rep. 2017;19(12):75.
Guzman J, Oen K, Tucker LB, Huber AM, Shiff N, Boire G, et al. The outcomes of juvenile idiopathic arthritis in children managed with contemporary treatments: results from the ReACCh-out cohort. Ann Rheum Dis. 2015;74(10):1854–60.
Moorthy LN, Peterson MG, Hassett AL, Lehman TJ. Burden of childhood-onset arthritis. Pediatr Rheumatol Online J. 2010;8:20.
Frid P, Nordal E, Bovis F, Giancane G, Larheim TA, Rygg M, et al. Temporomandibular joint involvement in association with quality of life, disability, and high disease activity in Juvenile idiopathic arthritis. Arthritis Care Res. 2017;69(5):677–86.
Glick M, Williams DM, Kleinman DV, Vujicic M, Watt RG, Weyant RJ. A new definition for oral health developed by the FDI world dental federation opens the door to a universal definition of oral health. Br Dent J. 2016;221(12):792–3.
Skeie MS, Gil EG, Cetrelli L, Rosén A, Fischer J, Åstrøm AN, et al. Oral health in children and adolescents with juvenile idiopathic arthritis - a systematic review and meta-analysis. BMC Oral Health. 2019;19(1):285.
Santos D, Silva C, Silva M. Oral health and quality of life of children and adolescents with juvenile idiopathic arthritis according to their caregivers’ perceptions. Special Care Dent. 2015;35(6):272–8.
Rahimi H, Twilt M, Herlin T, Spiegel L, Pedersen TK, Küseler A, et al. Orofacial symptoms and oral health-related quality of life in juvenile idiopathic arthritis: a two-year prospective observational study. Pediatr Rheumatol. 2018;16(1):47.
Leksell E, Ernberg M, Magnusson B, Hedenberg-Magnusson B. Orofacial pain and dysfunction in children with juvenile idiopathic arthritis: a case-control study. Scand J Rheumatol. 2012;41(5):375–8.
Isola G, Perillo L, Migliorati M, Matarese M, Dalessandri D, Grassia V, et al. The impact of temporomandibular joint arthritis on functional disability and global health in patients with juvenile idiopathic arthritis. Eur J Orthod. 2019;41(2):117–24.
Twilt M, Schulten AJ, Verschure F, Wisse L, Prahl-Andersen B, van Suijlekom-Smit LW. Long-term followup of temporomandibular joint involvement in juvenile idiopathic arthritis. Arthritis Rheum. 2008;59(4):546–52.
Rönning O, Väliaho ML, Laaksonen AL. The involvement of the temporomandibular joint in juvenile rheumatoid arthritis. Scand J Rheumatol. 1974;3(2):89–96.
Kjellberg H. Juvenile chronic arthritis. Dentofacial morphology, growth, mandibular function and orthodontic treatment. Swedish Dent J Suppl. 1995;109:1–56.
Peltomäki T, Kreiborg S, Pedersen TK, Ogaard B. Craniofacial growth and dento-alveolar development in juvenile idiopathic arthritis patients. Sem Orthodont. 2015;21(2):84–93.
Gil EG, Åstrøm AN, Lie SA, Rygg M, Fischer J, Rosén A, et al. Dental plaque and gingival bleeding in adolescents with juvenile idiopathic arthritis and controls: a multilevel analysis. Acta Odontol Scand. 2023;81(1):50–65.
Grevich S, Lee P, Leroux B, Ringold S, Darveau R, Henstorf G, et al. Oral health and plaque microbial profile in juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2019;17(1):81.
Gil EG, Åstrøm AN, Lie SA, Rygg M, Fischer J, Rosén A, et al. Dental caries in children and adolescents with juvenile idiopathic arthritis and controls: a multilevel analysis. BMC Oral Health. 2021;21(1):417.
Leksell E, Eriksson C, Ernberg M, Hedenberg-Magnusson B. Facilitating care of children with Juvenile idiopathic arthritis, orofacial pain, and dysfunction: an interview study of specialized health professionals. J Oral Facial Pain Headache. 2021;35(4):278–87.
Leksell E, Hallberg U, Horne A, Ernberg M, Hedenberg-Magnusson B. Parenting a child with Juvenile idiopathic arthritis, orofacial pain, and dysfunction: a qualitative study. J Oral Facial Pain Headache. 2017;31(4):353–61.
Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–2.
Greene JC, Vermillion JR. THE simplified oral hygiene index. J Am Dent Assoc. 1939;1964(68):7–13.
Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque. Int Dent J. 1975;25(4):229–35.
Pahel BT, Rozier RG, Slade GD. Parental perceptions of children’s Oral health: the early childhood Oral health impact scale (ECOHIS). Health Qual Life Outcomes. 2007;5:6.
Skeie M, Skaare A, Sande M, Sirevåg L, Åstrøm A. Oral health related quality of life among children and adolescents in Bergen, Norway. Validity and reliability of two measuring instruments. Nor Tannlegeforen Tid. 2017;127(7):592–8.
Boukhobza S, Stamm T, Glatthor J, Meißner N, Bekes K. Changes in oral health-related quality of life among Austrian preschool children following dental treatment under general anaesthesia. Clin Oral Invest. 2021;25(5):2821–6.
Arrow P. Responsiveness and sensitivity of the early childhood oral health impact scale to primary dental care for early childhood caries. Commun Dent Oral Epidemiol. 2016;44(1):1–10.
Locker D, Jokovic A, Clarke M. Assessing the responsiveness of measures of oral health-related quality of life. Commun Dent Oral Epidemiol. 2004;32(1):10–8.
Gherunpong S, Tsakos G, Sheiham A. Develo** and evaluating an oral health-related quality of life index for children; the CHILD-OIDP. Community Dent Health. 2004;21(2):161–9.
Adulyanon S, Sheiham A. Oral Impacts on Daily Performances. In: Slade GD, editor. Measuring Oral Health and Quality of Life; June 13-14, 1996; University of North Carolina-Chapel Hill, North Carolina: Department of Dental Ecology, School of Dentistry, University of North Carolina; 1997. p. 151-60
Stoustrup P, Twilt M, Spiegel L, Kristensen KD, Koos B, Pedersen TK, et al. Clinical orofacial examination in juvenile idiopathic arthritis: international consensus-based recommendations for monitoring patients in clinical practice and research studies. J Rheumatol. 2017;44(3):326–33.
Selvaag AM, Ruperto N, Asplin L, Rygg M, Landgraf JM, Forre Ø, et al. The Norwegian version of the Childhood Health Assessment Questionnaire (CHAQ) and the Child Health Questionnaire (CHQ). Clin Exp Rheumatol. 2001;19(4 Suppl 23):S116–20.
Landgraf J, Abetz L, Ware J. Child Health Questionnaire (CHQ): A User’s Manual. Boston: Health Institute, New England Medical Center; 1996.
Ruperto N, Ravelli A, Pistorio A, Malattia C, Cavuto S, Gado-West L, et al. Cross-cultural adaptation and psychometric evaluation of the Childhood Health Assessment Questionnaire (CHAQ) and the Child Health Questionnaire (CHQ) in 32 countries. Review of the general methodology. Clin Exper Rheumatol. 2001;19(4 Suppl 23):S1–9.
Consolaro A, Ruperto N, Bazso A, Pistorio A, Magni-Manzoni S, Filocamo G, et al. Development and validation of a composite disease activity score for juvenile idiopathic arthritis. Arthritis Rheum. 2009;61(5):658–66.
Stoustrup P, Resnick CM, Pedersen TK, Abramowicz S, Michelotti A, Küseler A, et al. Standardizing terminology and assessment for orofacial conditions in Juvenile idiopathic arthritis: international, multidisciplinary consensus-based recommendations. J Rheumatol. 2019;46(5):518–22.
Cohen J. A power primer. Psychol Bull. 1992;112(1):155–9.
Alvarez-Azaustre MP, Greco R, Llena C. Oral health-related quality of life in adolescents as measured with the child-OIDP questionnaire: a systematic review. Int J Environ Res Public Health. 2022;19(19):12450.
Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–5.
Pentapati KC, Yeturu SK, Siddiq H. A reliability generalization meta-analysis of Child Oral Impacts on Daily Performances (C - OIDP) questionnaire. J Oral Biol Craniofac Res. 2020;10(4):776–81.
Guney SE, Araz C, Tirali RE, Cehreli SB. Dental anxiety and oral health-related quality of life in children following dental rehabilitation under general anesthesia or intravenous sedation: a prospective cross-sectional study. Niger J Clin Pract. 2018;21(10):1304–10.
Mashoto KO, Astrøm AN, Skeie MS, Masalu JR. Changes in the quality of life of Tanzanian school children after treatment interventions using the child-OIDP. Eur J Oral Sci. 2010;118(6):626–34.
Zimmer S, Bergmann N, Gabrun E, Barthel C, Raab W, Rüffer JU. Association between oral health-related and general health-related quality of life in subjects attending dental offices in Germany. J Public Health Dent. 2010;70(2):167–70.
Sekulic S, John MT, Davey C, Rener-Sitar K. Association between Oral health-related and health-related quality of life. Zdr Varst. 2020;59(2):65–74.
Gil EG, Skeie MS, Halbig J, Jönsson B, Lie SA, Rygg M, et al. Oral health-related quality of life in 4–16-year-olds with and without juvenile idiopathic arthritis. BMC Oral Health. 2022;22(1):387.
Acknowledgements
This study is part of the multicenter NorJIA Study (The Norwegian JIA Study – Temporomandibular Involvement, Oral Health, Uveitis, Bone Health and Quality of Life in Children with Juvenile Idiopathic Arthritis (JIA)). NorJIA is a collaboration among universities (The University of Bergen, The Norwegian University of Science and Technology, The Arctic University of Norway), university hospitals (Haukeland University Hospital, St. Olav’s Hospital, University Hospital of North Norway) and oral health centers (Oral Health Center of Expertise in Western Norway- Vestland, Center for Oral Health Services and Research, Trondheim, Public Dental Health Service Competence Centre of Northern Norway) in Bergen, Trondheim and Tromsø. Represented by Karen Rosendahl MD PhD (PI), Marit Slåttelid Skeie DDS PhD, Marite Rygg MD PhD, Ellen Nordal MD PhD, Anne N. Åstrøm DDS PhD, Karin Tylleskär MD, Annika Rosén DDS PhD, Elisabeth G. Gil DDS PhD, Johannes Fischer DDS PhD, **eqi Shi DDS PhD, Oskar Angenete MD PhD, Lena Cetrelli DDS, Gunnar Lyngstad DDS, Marie Sager DDS, Astrid J Feuerheim PhD, Anette Lundestad MD, Thomas A. Augdal MD, Paula Frid DDS PhD, Veronika Rypdal MD PhD, Josefine M. Halbig DDS, Athanasia Bletsa DDS PhD, Marit Midtbø DDS PhD, Larissa von Wangenheim Marti DDS, Mats Säll DDS and Keijo Luukko DDS PhD. We are indebted to radiographers Marianne Lothe Vollan and Erik Haro and the study nurses Tone Kvinnsland Amdal, Susanne Irene Tobiesen Eidset, Line Rapp Simonsen, Marte Grimsmo Teige, Brita Lena Hansen, Lisbeth Aune and Tonje Løvli. Finally, we are thankful to all the children and their caregivers who participated in the study.
Funding
Open access funding provided by UiT The Arctic University of Norway (incl University Hospital of North Norway) The current study is supported by universities (The Arctic University of Norway, University of Bergen, Norwegian University of Science and Technology), university hospitals (University Hospital of North Norway, Haukeland University Hospital, St. Olav’s Hospital), and oral health centers (Public Dental Health Service Competence Centre of Northern Norway, Oral Health Centre of Expertise in Western Norway-Vestland, Center for Oral Health Services and Research, Trondheim) in Tromsø, Bergen, and Trondheim. We are grateful to “Norsk Revmatikerforbund” and the Grete Harbitz Foundation (Norway) for funding parts of the data collection. The first author’s PhD program is financed by the Public Dental Health Service Competence Centre of Northern Norway. The funding organizations did not play a role in the design of the study, collection, analysis, interpretation of data, or in writing the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
JMH contributed to the design, data collection, and data analysis of this substudy, performed the statistical analysis, and wrote the manuscript in consultation with EN, BJ, ANÅ, and EGG. EN, BJ, ANÅ and EGG contributed to the design of the study. EGG, VR, PF, JF, MR, AL, KT, EN, LC, and TAA contributed to data collection or adaptation of data and provided valuable comments. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Regional Committees for Medical and Health Research Ethics (2012/542/REK), Rogaland, Vestland (West). Written informed consent was obtained from the caregivers and adolescents, as appropriate. The study was registered at ClinicalTrials.gov (No: NCT03904459, 5/4/2019). All procedures were performed in accordance with relevant guidelines.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Original codes and recoded variables. S1 Table 1. Categories for socio-behavioral characteristics, as originally coded and as recoded for analyses. S1 Table 2. ECOHIS answering categories as originally coded and recoded for analysis.
Additional file 2:
Dropout analysis. S2 Table 1. First visit characteristics for children <12 years in JIA and control group for dropout analysis. S2 Table 2. First visit characteristics for adolescents ≥12 years in JIA and control group for dropout analysis.
Additional file 3:
Reliability and validity of OHRQoL instruments. S3 Table 1. Internal consistency reliability of the OHRQoL instruments. S3 Table 2. Mean OHRQoL change ADD scores by change categories of reference variables in children and adolescents.
Additional file 4:
Mean OHRQoL ADD scores according to orofacial pain, CHQ physical scores, and disease activity (JADAS71). S4 Table 1. Mean OHRQoL ADD scores according to orofacial pain. S4 Table 2. Mean OHRQoL ADD scores according to CHQ physical scores. S4 Table 3. Mean OHRQoL ADD scores according to JADAS71.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Halbig, J.M., Jönsson, B., Gil, E.G. et al. Oral health-related quality of life, impaired physical health and orofacial pain in children and adolescents with juvenile idiopathic arthritis – a prospective multicenter cohort study. BMC Oral Health 23, 895 (2023). https://doi.org/10.1186/s12903-023-03510-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12903-023-03510-0