
Abstract
Objective
The aim was to study associations between chronic widespread pain, widespread pain sensitivity, leptin, and metabolic factors in individuals with knee pain. A secondary aim was to study these associations in a subgroup of individuals with normal BMI.
Method
This cross-sectional study included 265 individuals. The participants were categorised into three different pain groups: Chronic widespread pain (CWP), chronic regional pain (ChRP), or no chronic pain (NCP). The pressure pain thresholds (PPTs) were assessed using computerised pressure algometry. Low PPTs were defined as having PPTs in the lowest third of all tender points. Leptin and metabolic factors such as BMI, visceral fat area (VFA), lipids, and glucose were also assessed.
Result
Sixteen per cent reported CWP, 15% had low PPTs, and 4% fulfilled both criteria. Those who fulfilled the criteria for CWP were more often women, more obese, and had increased leptin levels. In logistic regression, adjusted for age and gender, leptin was associated with fulfilling criteria for CWP, OR 1.015 (95% CI 1.004–1.027, p = 0.008). In logistic regression, adjusted for age and gender, leptin was associated with low PPTs, OR 1.016 (95% CI 1.004–1.029, p = 0.012). Leptin was also associated with fulfilling both criteria, adjusted for age, sex, and visceral fat area (VFA), OR 1.030 (95% CI 1.001–1.060), p = 0.040.
Conclusion
Leptin was associated with fulfilling the combined criteria for chronic widespread pain and low PPTs, even after adjusting for the visceral fat area (VFA). Longitudinal studies are needed to study the causal relationships between leptin and the development of widespread pain.
Trial registration
clinicalTrials.gov Identifier: NCT04928170.
Similar content being viewed by others


Introduction
Knee pain is an early feature of knee OA, which precedes structural changes within the joint [1]. In individuals with knee pain, it is relatively common to have a more widespread pain, affecting not only the knee joint but the whole body—about one-third of individuals with knee pain report chronic widespread pain [2, 3].
Obesity is reported to be associated not only with OA but also with chronic widespread pain and fibromyalgia [3,4,5]. Studies have also reported associations between obesity and higher levels of pain intensity and disease activity in patients with low back pain, psoriatic arthritis (PsoA), rheumatoid arthritis (RA), ankylosing spondylitis (AS) and systemic lupus erythematosus (SLE) [6,7,8,9].
Adipose tissue synthesises hormones (adipokines), cytokines, and growth factors [10]. The adipokine leptin was identified in 1994 and is synthesised by mature adipocytes [11, 12]. Leptin regulates hunger and appetite but has other functions, such as glucose tolerance, insulin sensitivity, and immune cell functions [13, 14]. Leptin has recently been reported to be able to act via the sympathetic nervous system (SNS), and leptin receptors have been identified on dorsal root ganglia neurons in the SNS [15]. The SNS regulates leptin synthesis and secretion and modulates leptin levels independent of adiposity [16,17,18]. The SNS also suppresses pain by descending inhibition of nociceptive transmission in the spinal cord [19,20,21].
Leptin is increased in individuals with OA, and women have higher levels than men [22,23,24]. It is associated with OA and symptoms such as pain; however, the mechanisms are not yet known in detail [25, 26]. Leptin has further been suggested to be involved in the pathogenesis of OA, up-regulating matrix metalloproteinases (MMPs), and contribute to the low-grade inflammation seen in OA [22, 24].
Pain and allodynia are significant symptoms in patients with lipedema, and they have increased levels of leptin and achieve pain relief after liposuction [27]. Some studies also report improvement in pain intensity and sensitisation after weight loss in the general population as well as in individuals with musculoskeletal diseases [28,29,30,31]. Increased metabolic risk factors have been reported also in individuals with normal BMI [32, 33]. However, knowledge of the pathophysiological mechanisms involved in pain sensitisation and widespread pain is still scarce.
The aim was to study associations between chronic widespread pain, widespread pain sensitivity, leptin, and metabolic factors in individuals with knee pain. A secondary aim was to study the associations also in a subgroup of individuals with normal BMI.
Method
Participants
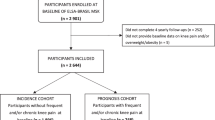
In total, 265 individuals with complete assessment for pressure pain thresholds (PPTs) from the Halland osteoarthritis cohort (HALLOA), ClinicalTrials.gov NCT04928170, were included in this cross-sectional study. HALLOA is a longitudinal cohort study including individuals with knee pain at baseline [34]. The inclusion criteria for the HALLOA cohort were current knee pain, with no former known radiographic knee OA and no cruciate ligament rupture or rheumatological disorder, with a preferable age of 30–65 years. The mean age and standard deviation (SD) were 51.6 (8.8), and 71% were women.
Outcome measures
Chronic pain assessment and classifications
Participants marked their painful areas, if they had any, on a pain figure that showed 18 predefined regions [35]. They were categorised into three different pain groups by the modified WP2019 definition [36]: Chronic widespread pain (CWP), chronic regional pain (ChRP) if criteria for CWP were not met, or no chronic pain (NCP). The definition of WP2019, where the knees were excluded, was used due to higher goodness of fit.
The pressure pain thresholds (PPTs) were measured on eight of the 18 predefined tender points by the definition of fibromyalgia [37]. The locations of the eight tender points were: trapezius (bilateral, midpoint of the upper border); second rib (right side, at the second costochondral junctions, just lateral to the junctions on the upper surfaces); lateral epicondyle (right side, 2 cm distal to the epicondyles); knees (bilateral, at the medial fat pad proximal to the joint line); and gluteus (bilateral, in upper outer quadrants of the buttocks in the anterior fold of the gluteus maximus muscle). A hand-held pressure algometer with a 1 cm2 rubber probe and a computer interface with an assistant linear response to force application (AlgoMed, Medoc, Ramat Yishai, Israel) were used. A description of the pressure pain threshold assessment has been published previously [3]. Individuals with a PPT value in the lowest third in all separate tender points were included in the group with low PPTs to study those with a more widespread pain sensitivity.
Clinical assessments of metabolic factors
The participant’s height and weight were measured, and BMI was calculated. Visceral fat area (VFA) was assessed by bioimpedance measurement, Inbody 770 (Biospace South Korea).
Fasting plasma glucose (mmol/L), triglycerides (TG) (mmol/L), total cholesterol (mmol/L), high-density lipoprotein (HDL)-cholesterol and low-density lipoprotein (LDL)-cholesterol (mmol/L), haemoglobin A1c (HbA1c) (mmol/mol) and C-reactive protein (CRP) > 1.0 mg/L were measured from venous blood, by the current laboratory standards at Halland County Hospital in Halmstad, Sweden, accredited according to SS-EN ISO 15,189. Glucose, TG, total cholesterol, HDL- and LDL-cholesterol were analysed with photometry (Cobas 8000, Roche). HbA1c was analysed with liquid chromatography (TOSOH G8), and CRP was analysed with turbidimetry (Cobas 8000, Roche). CRP below 1.0 mg/L was further explored by applying a sensitive CRP ELISA method (Abnova). Fasting serum leptin was analysed with an enzyme-linked immunosorbent Assay (ELISA) method (Alpco). The leptin analyses were performed as duplicates. Raised glucose was classified as fasting plasma glucose ≥ 5.6 mmol/L or previously diagnosed type II diabetes [38]. Raised triglycerides were classified as triglycerides ≥ 1.7 mmol/L or having specific treatment for this lipid abnormality [38]. Reduced HDL-cholesterol was classified as HDL-cholesterol < 1.03 mmol/L in males and 1.29 mmol/L in females, or specific treatment for this lipid abnormality [38].
Statistics
To test the differences between groups, the Mann-Whitney U test and the chi-squared tests were used, where appropriate. If comparisons of more than two groups were performed, the Kruskall-Wallis test was used, and if p < 0.05, pairwise comparisons were performed. The missing data were not replaced. All missing data were addressed in the tables. In the analysis of self-reported pain distribution, the three pain groups, NCP, ChRP, and CWP, were compared. In the logistic regression models, CWP was compared to not having CWP as the dependent variable. In the analysis of bilateral PPTs (trapezius, knees, and gluteus), the mean of the two bilateral PPTs on each tender point was used [39]. To study those with more widespread pain sensitivity, those with a PPT value in the lowest third in all separate tender points were included in the group with low PPTs. Low PPTs were compared to not having low PPTs as the dependent variable in the logistic regression models. Variables associated with reporting CWP or having low PPTs, respectively, with a significance level of p ≤ 0.25, were introduced into a multivariate model [40], controlling for age and sex. Separate logistic regression models were also performed between leptin, CWP and low PPT,s adjusting for age, sex and VFA. Dichotomised variables of glucose, triglycerides, and HDL-cholesterol, according to the International Diabetes Federation, were chosen, taking medical treatment into account [38].
Analyses of subgroups were performed by selecting individuals with a normal BMI (BMI < 25) and comparing the groups NCP, ChRP, and CWP and the groups with or without Low PPTs, respectively. Analyses of the combined groups, which fulfilled either or both criteria (CWP and/or low PPTs), were also performed. The logistic regression analysis was performed using the group fulfilling both criteria (Low PPTs and CWP) compared to not doing so as the dependent variable. This group was seen as the most fibromyalgia-like group.
The significance tests were two-tailed and conducted at the 0.05 level of significance. Statistical analyses were performed using SPSS version 21.0 statistical software (IBM Corp., Armonk, NY, USA).
Results
Chronic widespread pain and associations with metabolic factors
Out of 265 included individuals, 250 individuals answered the questionnaire, the mean (sd) age was 51.6 (8.8) years, and 71% were women. There were no significant differences between those who answered the questionnaire and those who did not in age, sex, BMI, VFA, and leptin. Of those who answered the questionnaire, 16% reported CWP. They were more often women and had increased BMI compared to NCP (p = 0.014) and higher VFA compared to both NCP (p = 0.001) and ChRP (p = 0.009). Those reporting CWP had more often raised triglycerides (standard residual 2.5) and higher leptin levels compared to both NCP (p = 0.002) and ChRP (p = 0.001), Table 1.
Both univariate and multivariate regression models, adjusted for age and sex, showed associations between female sex, obesity (BMI and VFA), raised triglycerides, increased leptin, and CWP, Table 2. The correlation between VFA and leptin was r = 0.74, p < 0.001. When adjusting for age, sex, and VFA, leptin and CWP showed no significant association with OR 1.007 (95% CI 0.989–1.025, p = 0.461).
In a subgroup with BMI < 25 (n = 115), 12% reported CWP, Table 3. Also, in this subgroup, both VFA and leptin, adjusted for age and sex, were associated with CWP (VFA OR 1.021, 95% CI 1.001–1.040, p = 0.035 and leptin OR 1.036, 95% CI 1.002–1.072, p = 0.038), supplement Table 1. The correlation between VFA and leptin in this subgroup was r = 0.68, p < 0.001. Leptin and CWP were not significantly associated when adjusted for age, sex, and VFA, OR 1.019(95% CI 0.970–1.070, p = 0.449).
Pain pressure thresholds and associations with metabolic factors
Fifteen per cent of the included individuals had low PPTs. The individuals with low PPTs were younger, had higher VFA, more often reduced HDL-cholesterol, and increased leptin Table 4.
Univariate and multivariate logistic regressions, adjusted for age and sex, showed associations between low PPTs and younger age, increased VFA, reduced HDL-cholesterol, and increased leptin, Table 5. The correlation between VFA and leptin was r = 0.75, p < 0.001. There was no significant association between leptin and CWP when adjusted for age, sex, and VFA, OR 1.010 (95% CI 0.992–1.029, p = 0.267).
In a subgroup with BMI < 25 (n = 119), 11% had low PPTs, Table 6. In this subgroup, leptin, adjusted for age and sex, was associated with low PPTs (OR 1.030 (95% CI 0.997–1.065), p = 0.073), supplement Table 2. The correlation in this subgroup between VFA and leptin was r = 0.68, p < 0.001. When adjusting for age, sex, and VFA, the association between leptin and low PPT was non-significant, OR 1.010 (95% CI 0.960–1.062, p = 0.669).
Leptin levels in those who did or did not fulfil the combined pain criteria
The individuals that fulfilled both criteria (for CWP and low PPTs) were younger than those reporting CWP (p = 0.047). Those fulfilling both criteria had higher VFA and leptin levels than those that did not fulfil the criteria (no pain) (p = 0.028 and p = 0.012), supplement Table 3. Younger age, increased VFA, raised TG, reduced HDL-cholesterol, and leptin was associated with fulfilling both criteria, supplement Table 4. Leptin was associated with fulfilling both criteria, adjusted for age, sex, and VFA, OR 1.030 (95% CI 1.001–1.060), p = 0.040.
Discussion
This study found that more than every fourth individual with knee pain reported CWP and/or low PPTs and that 4% fulfilled both criteria. Obesity, leptin, and metabolic factors were associated with both CWP and low PPTs.
The link between chronic pain and OA is not fully known. There are studies suggesting mechanical load could induce chronic pain due to compression and aberrant loading [41,42,43]. In the present study, 11–12% of those with normal BMI (BMI < 25 kg/m2) reported CWP and/or had low PPTs, and in those individuals, the mechanical load should not have a significant impact. There are studies suggesting that inflammation due to obesity could cause chronic pain [42, 44]. However, in the current study, there was no association between reported CWP or having low PPTs with inflammation assessed with CRP. Although, it could be a limitation that the low-grade inflammation in the present study was assessed by CRP and not IL-6, which could be a better biomarker for low-grade inflammation [14].
In the present study, leptin level was increased and associated with CWP and having low PPTs. However, in the sub-studies of normal BMI, there were no significant differences in leptin levels between pain groups (NCP, ChRP and CWP; not low PPTs and low PPTs), but still an association between leptin and CWP. Interestingly, there was an increasing level of leptin, with the lowest level in the no pain group and the highest level in the group that met both criteria. There was an association between fulfilling both criteria and leptin, adjusted for age, sex, and VFA. This study does not reveal if increased leptin is a marker for obesity or has a more active role within the pathophysiological mechanism of chronic widespread pain. There is a high correlation between VFA and leptin, and when adjusting for VFA, an actual association may be removed. In a previous longitudinal study of the transition between pain groups in patients with rheumatoid arthritis, a transition from CWP to NCP was associated with a normal BMI and a transition from NCR/ChRP to CWP was associated with central obesity [45]. In mice, it has been shown that when injecting leptin, the pain behaviour increases and this was reversed with the administration of a leptin agonist [46, 47].
In those with normal BMI, leptin was also increased and/or associated with reporting CWP. There are reports of a new concept of normal-weight obesity or metabolically obese normal-weight individuals. It is defined by normal weight and BMI but with a cluster of metabolic characteristics, such as increased insulin sensitivity, triglycerides, and VFA [33, 48]. In another study within the HALLOA cohort, associations between metabolic factors and OA have also been reported in individuals with normal BMI [32]. A group of individuals within the study could have a metabolic condition, including increased leptin levels despite normal BMI. It was thus essential to test the hypothesis also in the subgroup with normal BMI to reveal if leptin could be associated with CWP and low PPTs also in this subgroup. In a clinical setting, a normal BMI may not be a guarantee that there are no metabolic issues.
Other studies have reported increased leptin levels in migraine [49], pelvic pain in endometriosis [50], lipedema [27], low back pain [51], and multisomatoform disorder (MSD) [52]. Leptin levels have been reported to be reduced when weight is lost [53]. Studies also report symptom and pain reduction in relation to losing weight, not only in OA but also in chronic pain conditions, such as fibromyalgia [4]. In rodents, leptin has been shown to decrease pain thresholds and contribute to neuropathic pain [46, 47]. One study showed that low leptin levels were associated with clinical improvement, assessed by Ankylosing Spondylitis Disease Activity Score (ASDAS) in axSpA patients treated with anti-tumor necrosing factor injections (TNFi) [54]. ASDAS includes pain scores; an improvement in pain scores decreases the total score. The study concluded that obese patients should be encouraged to lose weight.
Leptin is shown to reduce norepinephrine (noradrenaline) concentrations in the paraventricular nucleus, arcuate nucleus, and ventromedial hypothalamus in mice [55]. Noradrenaline is the main neurotransmitter released by the SNS and is involved in the intrinsic control of pain [56, 57]. There is a possibility that leptin could influence the descending control of pain, as the descending control of pain involves norepinephrine [16, 56, 57]. Leptin concentration is associated with the amount of white fat mass, and weight reduction is shown to reduce leptin levels and symptoms such as pain [16, 28, 29, 31, 53, 58,59,60].
There were also increased levels and associations of other metabolic factors. The patients who reported CWP had higher levels of triglycerides, and triglycerides were associated with reporting CWP, also in the subgroup with normal BMI. Triglycerides were also associated with having low PPTs. The current study found associations between having low PPTs and reduced HDL-cholesterol. Other studies have reported associations between hyperlipidemia, chronic pain, and pain sensitisation [61, 62].
Weight loss is not a high-priority recommendation in treatment recommendations for OA and chronic pain/fibromyalgia [63,64,65]. Given that obesity and/or increased VFA is a risk factor for both OA and chronic pain/fibromyalgia, weight reduction should have a more prominent position as a treatment option in OA to prevent pain sensitisation and treat chronic pain/fibromyalgia.
The limitation of the current study is its cross-sectional design and not longitudinal; studies of casual relationships are needed. However, as this study is part of a longitudinal cohort study within the HALLOA cohort, causal relationships could be studied in the future. CWP was self-reported, which could be a limitation. The pain figure used for reporting CWP has been used in several studies [2, 35, 66, 67]. The lack of a control group could be a limitation. However, the comparisons between pain groups are valid within this context of individuals with knee pain, giving a possible risk marker for widespread pain. The PPTs assessment was performed by more than one test leader, which could be a limitation, but all the test leaders had previous experience and had undergone training. A previous study shows that at least one hour of training improved reliability [68]. The study’s strength is that it is a population-based cohort with knee pain at baseline and is part of a longitudinal cohort study. Many of the included individuals (76%) have no radiographic knee OA and are considered individuals in the early disease course [32].
In conclusion, leptin and metabolic factors were associated with both CWP and low PPTs in this study. The pathophysiological mechanism causing widespread pain and pain sensitivity is probably multifactorial, involving biological and physical factors. The adipokine leptin could be involved in some of these mechanisms, but longitudinal studies are needed to explore causal relationships and pathophysiological mechanisms. There is also a need to study leptin in other diseases with a risk of develo** chronic widespread pain.
Data Availability
The dataset used and analysed during the current study is available from the corresponding author upon reasonable request.
Abbreviations
- ADL:
-
Function in daily living
- AS:
-
Ankylosing spondylitis
- BMI:
-
Body mass index
- ChRP:
-
Chronic regional pain
- CRP:
-
C-reactive protein
- CWP:
-
Chronic widespread pain
- ELISA:
-
Enzyme-linked immunosorbent assay
- HALLOA:
-
Halland osteoarthritis cohort
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- NCP:
-
No chronic pain
- OA:
-
Osteoarthritis
- PsoA:
-
Psoriatic arthritis
- PPTs:
-
Pressure pain thresholds
- RA:
-
Rheumatoid arthritis
- SLE:
-
Systemic lupus erythematosus
- SNS:
-
Sympathetic nervous system
- VFA:
-
Visceral fat area
References
Mahmoudian A, Lohmander LS, Mobasheri A, Englund M, Luyten FP. Early-stage symptomatic osteoarthritis of the knee - time for action. Nat Rev Rheumatol. 2021;17:621–32.
Bergman S, Thorstensson C, Andersson MLE. Chronic widespread pain and its associations with quality of life and function at a 20- year follow-up of individuals with chronic knee pain at inclusion. BMC Musculoskelet Disord. 2019;20:592.
Sylwander C, Larsson I, Haglund E, Bergman S, Andersson MLE. Pressure pain thresholds in individuals with knee pain: a cross-sectional study. BMC Musculoskelet Disord. 2021;22:516.
Ursini F, Naty S, Grembiale RD. Fibromyalgia and obesity: the hidden link. Rheumatol Int. 2011;31:1403–8.
Wright LJ, Schur E, Noonan C, Ahumada S, Buchwald D, Afari N. Chronic pain, overweight, and obesity: findings from a community-based twin registry. J pain: official J Am Pain Soc. 2010;11:628–35.
Ajeganova S, Andersson ML, Hafstrom I, Group BS. Association of obesity with worse disease severity in rheumatoid arthritis as well as with comorbidities: a long-term followup from disease onset. Arthritis Care Res. 2013;65:78–87.
Eder L, Thavaneswaran A, Chandran V, Cook RJ, Gladman DD. Obesity is associated with a lower probability of achieving sustained minimal disease activity state among patients with psoriatic arthritis. Ann Rheum Dis. 2015;74:813–7.
Maguire S, Wilson F, Gallagher P, O’Shea F. Central obesity in Axial Spondyloarthritis: the missing link to understanding worse outcomes in women? J Rhuematol. 2022;49:577–84.
Oeser A, Chung CP, Asanuma Y, Avalos I, Stein CM. Obesity is an independent contributor to functional capacity and inflammation in systemic lupus erythematosus. Arthritis Rheum. 2005;52:3651–9.
Galic S, Oakhill JS, Steinberg GR. Adipose tissue as an endocrine organ. Mol Cell Endocrinol. 2010;316:129–39.
Zhang F, Basinski MB, Beals JM, Briggs SL, Churgay LM, Clawson DK, et al. Crystal structure of the obese protein leptin-E100. Nature. 1997;387:206–9.
Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM. Positional cloning of the mouse obese gene and its human homologue. Nature. 1994;372:425–32.
Funcke JB, Scherer PE. Beyond adiponectin and leptin: adipose tissue-derived mediators of inter-organ communication. J Lipid Res. 2019;60:1648–84.
Kinfe TM, Buchfelder M, Chaudhry SR, Chakravarthy KV, Deer TR, Russo M et al. Leptin and Associated Mediators of Immunometabolic Signaling: Novel Molecular Outcome Measures for Neurostimulation to treat Chronic Pain. Int J Mol Sci. 2019;20.
Chen HP, Fan J, Cui S. Detection and estrogen regulation of leptin receptor expression in rat dorsal root ganglion. Histochem Cell Biol. 2006;126:363–9.
Caron A, Lee S, Elmquist JK, Gautron L. Leptin and brain-adipose crosstalks. Nat Rev Neurosci. 2018;19:153–65.
Fried SK, Ricci MR, Russell CD, Laferrere B. Regulation of leptin production in humans. J Nutr. 2000;130:3127S–31S.
Wajchenberg BL. Subcutaneous and visceral adipose tissue: their relation to the metabolic syndrome. Endocr Rev. 2000;21:697–738.
Millan MJ. Descending control of pain. Progress in Neurology. 2002;66:355–474.
Schlereth T, Birklein F. The sympathetic nervous system and pain. Neuromolecular Med. 2008;10:141–7.
Yam MF, Loh YC, Tan CS, Khadijah Adam S, Abdul Manan N, Basir R. General Pathways of Pain Sensation and the major neurotransmitters involved in Pain Regulation. Int J Mol Sci. 2018;19.
Ait Eldjoudi D, Cordero Barreal A, Gonzalez-Rodriguez M, Ruiz-Fernandez C, Farrag Y, Farrag M et al. Leptin in Osteoarthritis and Rheumatoid Arthritis: player or bystander? Int J Mol Sci. 2022;23.
Kroon FPB, Veenbrink AI, de Mutsert R, Visser AW, van Dijk KW, le Cessie S et al. The role of leptin and adiponectin as mediators in the relationship between adiposity and hand and knee osteoarthritis. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society. 2019;27:1761-7.
Yan M, Zhang J, Yang H, Sun Y. The role of leptin in osteoarthritis. Med (Baltim). 2018;97:e0257.
Sellam J, Rat AC, Fellahi S, Bastard JP, Ngueyon Sime W, Ea HK, et al. Pain in women with knee and/or hip osteoarthritis is related to systemic inflammation and to adipose tissue dysfunction: cross-sectional results of the KHOALA cohort. Semin Arthritis Rheum. 2021;51:129–36.
Achenbach J, Rhein M, Glahn A, Frieling H, Karst M. Leptin promoter methylation in female patients with painful multisomatoform disorder and chronic widespread pain. Clin Epigenetics. 2022;14:13.
Aksoy H, Karadag AS, Wollina U. Cause and management of lipedema-associated pain. Dermatol Ther. 2021;34:e14364.
Atukorala I, Makovey J, Lawler L, Messier SP, Bennell K, Hunter DJ. Is there a dose-response relationship between weight loss and symptom improvement in persons with knee osteoarthritis? Arthritis Care Res. 2016;68:1106–14.
Kerver GA, Bond DS, Crosby RD, Cao L, Engel SG, Mitchell JE, et al. Pain is adversely related to weight loss maintenance following bariatric surgery. Surg Obes Relat Dis. 2021;17:2026–32.
Klingberg E, Bilberg A, Bjorkman S, Hedberg M, Jacobsson L, Forsblad-d’Elia H, et al. Weight loss improves disease activity in patients with psoriatic arthritis and obesity: an interventional study. Arthritis Res therapy. 2019;21:17.
Stefanik JJ, Felson DT, Apovian CM, Niu J, Margaret Clancy M, LaValley MP, et al. Changes in Pain Sensitization after bariatric surgery. Arthritis Care Res. 2018;70:1525–8.
Andersson M, Haglund E, Aili K, Bremander A, Bergman S. Associations between metabolic factors and radiographic knee osteoarthritis in early disease - a cross-sectional study of individuals with knee pain. BMC Musculoskelet Disord. 2022;23:938.
Oliveros E, Somers VK, Sochor O, Goel K, Lopez-Jimenez F. The concept of normal weight obesity. Prog Cardiovasc Dis. 2014;56:426–33.
Andersson MLE, Haglund E, Aili K, Bremander A, Bergman S. Cohort profile: the Halland osteoarthritis (HALLOA) cohort-from knee pain to osteoarthritis: a longitudinal observational study in Sweden. BMJ open. 2022;12:e057086.
Bergman S, Herrstrom P, Hogstrom K, Petersson IF, Svensson B, Jacobsson LT. Chronic musculoskeletal pain, prevalence rates, and sociodemographic associations in a swedish population study. J Rhuematol. 2001;28:1369–77.
Wolfe F, Butler SH, Fitzcharles M, Hauser W, Katz RL, Mease PJ, et al. Revised chronic widespread pain criteria: development from and integration with fibromyalgia criteria. Scand J Pain. 2019;20:77–86.
Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American College of Rheumatology 1990 Criteria for the classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33:160–72.
International Diabetes Federation (IDF). The IDF consensus worldwide definition of the metabolic Syndrome. 2006.
Lacourt TE, Houtveen JH, van Doornen LJP. Experimental pressure-pain assessments: test-retest reliability, convergence and dimensionality. Scand J Pain. 2012;3:31–7.
Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:17.
Dieppe PA, Lohmander LS. Pathogenesis and management of pain in osteoarthritis. Lancet. 2005;365:965–73.
Okifuji A, Hare BD. The association between chronic pain and obesity. J pain Res. 2015;8:399–408.
Zdziarski LA, Wasser JG, Vincent HK. Chronic pain management in the obese patient: a focused review of key challenges and potential exercise solutions. J pain Res. 2015;8:63–77.
Lee YC, Lu B, Bathon JM, Haythornthwaite JA, Smith MT, Page GG, et al. Pain sensitivity and pain reactivity in osteoarthritis. Arthritis Care Res. 2011;63:320–7.
Andersson M, Svensson B, Bergman S. Pain in rheumatoid arthritis: a seven-year follow-up study of pain distribution and factors associated with transition from and to chronic widespread pain. Scand J Rheumatol. 2022;51:345–54.
Kutlu S, Canpolat S, Sandal S, Ozcan M, Sarsilmaz M, Kelestimur H. Effects of central and peripheral administration of leptin on pain threshold in rats and mice. Neuro Endocrinol Lett. 2003;24:193–6.
Lim G, Wang S, Zhang Y, Tian Y, Mao J. Spinal leptin contributes to the pathogenesis of neuropathic pain in rodents. J Clin Invest. 2009;119:295–304.
De Lorenzo A, Soldati L, Sarlo F, Calvani M, Di Lorenzo N, Di Renzo L. New obesity classification criteria as a tool for bariatric surgery indication. World J gastroenterology: WJG. 2016;22:681–703.
Peterlin BL. The role of the adipocytokines adiponectin and leptin in migraine. J Am Osteopath Assoc. 2009;109:314–7.
Bedaiwy MA, Falcone T, Goldberg JM, Sharma RK, Nelson DR, Agarwal A. Peritoneal fluid leptin is associated with chronic pelvic pain but not infertility in endometriosis patients. Hum Reprod. 2006;21:788–91.
Segar AH, Fairbank JCT, Urban J. Leptin and the intervertebral disc: a biochemical link exists between obesity, intervertebral disc degeneration and low back pain-an in vitro study in a bovine model. Eur Spine J. 2019;28:214–23.
Achenbach J, Volkmann L, Tran AT, Jager B, Rhein M, Glahn A, et al. Neurohumoral profiles and Childhood Adversity of Patients with Multisomatoform Disorder and Pain as the leading Bodily Symptom. Dis Markers. 2022;2022:7958375.
Maffei M, Giordano A. Leptin, the brain and energy homeostasis: from an apparently simple to a highly complex neuronal system. Rev Endocr Metab Disord. 2022;23:87–101.
Hernandez-Breijo B, Novella-Navarro M, Genre F, Navarro-Compan V, Martinez-Feito A, Remuzgo-Martinez S et al. Serum leptin concentration is associated with the attainment of clinical outcomes in patients with axial spondyloarthritis treated with TNF inhibitors. Clinical and experimental rheumatology. 2022.
Clark KA, Shin AC, Sirivelu MP, Mohankumar SM, Mohankumar PS. Systemic administration of leptin decreases plasma corticosterone levels: role of hypothalamic norepinephrine. Brain Res. 2008;1195:89–95.
Ossipov MH, Morimura K, Porreca F. Descending pain modulation and chronification of pain. Curr Opin Support Palliat Care. 2014;8:143–51.
Pertovaara A. Noradrenergic pain modulation. Prog Neurobiol. 2006;80:53–83.
Guven S, El-Bershawi A, Sonnenberg GE, Wilson CR, Hoffmann RG, Krakower GR, et al. Plasma leptin and insulin levels in weight-reduced obese women with normal body mass index: relationships with body composition and insulin. Diabetes. 1999;48:347–52.
Kotowski SE, Davis KG. Influence of weight loss on musculoskeletal pain: potential short-term relevance. Work. 2010;36:295–304.
Maffei M, Halaas J, Ravussin E, Pratley RE, Lee GH, Zhang Y, et al. Leptin levels in human and rodent: measurement of plasma leptin and ob RNA in obese and weight-reduced subjects. Nat Med. 1995;1:1155–61.
Cordero MD, Alcocer-Gomez E, Cano-Garcia FJ, Sanchez-Dominguez B, Fernandez-Riejo P, Moreno Fernandez AM, et al. Clinical symptoms in fibromyalgia are associated to overweight and lipid profile. Rheumatol Int. 2014;34:419–22.
Gurer G, Sendur OF, Ay C. Serum lipid profile in fibromyalgia women. Clin Rheumatol. 2006;25:300–3.
Fernandes L, Hagen KB, Bijlsma JW, Andreassen O, Christensen P, Conaghan PG, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72:1125–35.
Geenen R, Overman CL, Christensen R, Asenlof P, Capela S, Huisinga KL, et al. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Ann Rheum Dis. 2018;77:797–807.
Macfarlane GJ, Kronisch C, Dean LE, Atzeni F, Hauser W, Fluss E, et al. EULAR revised recommendations for the management of fibromyalgia. Ann Rheum Dis. 2017;76:318–28.
Andersson ML, Svensson B, Bergman S. Chronic widespread pain in patients with rheumatoid arthritis and the relation between pain and disease activity measures over the first 5 years. J Rhuematol. 2013;40:1977–85.
Aronsson M, Bergman S, Lindqvist E, Andersson MLE. Comparison of chronic widespread pain prevalence with different criteria in two cohorts of rheumatoid arthritis. Clin Rheumatol. 2022;41:1023–32.
Walton DM, Macdermid JC, Nielson W, Teasell RW, Chiasson M, Brown L. Reliability, standard error, and minimum detectable change of clinical pressure pain threshold testing in people with and without acute neck pain. J Orthop Sports Phys Ther. 2011;41:644–50.
Acknowledgements
The authors thank the participants for taking the time to participate in the study. A special thanks to Jan Bagge, who participated in the study’s development and design as a patient research partner.
Funding
Open access funding provided by Lund University. The study was funded by the Swedish Rheumatism Association, grant numbers R-531621, R-635431, R-939824, and R-967899; targeted investment from the Swedish Rheumatism Association – Osteoarthritis from 2014 to 2019, and the Crafoord Foundation. The funders have not influenced the study design, collection, analysis, or interpretation of data, nor the writing of the manuscript or the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
All authors contributed equally to the conception and design of the study and interpretation of data, obtained the funding, and read and approved the final version. MA took part in the collection and assembly of data, analysed the data, and drafted the article. CS took part in the collection and assembly of data, and critically revised the manuscript. CS and SB read it critically for important intellectual content. MA (maria.andersson@fou-spenshult.se) and SB (stefan.bergman@fou-spenshult.se) took responsibility for the integrity of the work, from inception to the finished article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants gave informed consent to participate in the study, obtained by the Helsinki Declaration (World Medical Association, 1964). The Regional Ethical Review Board, Faculty of Medicine, University of Lund, Sweden (2016 − 229 and 2017/253) approved the study.
Consent for publication
Not applicable.
Competing interests
The authors have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
Cite this article
Andersson, M.L., Thorén, E., Sylwander, C. et al. Associations between chronic widespread pain, pressure pain thresholds, leptin, and metabolic factors in individuals with knee pain. BMC Musculoskelet Disord 24, 639 (2023). https://doi.org/10.1186/s12891-023-06773-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-023-06773-4