
Abstract
Background
Loneliness is a significant public health concern due to its detrimental impact on health and wellbeing. Despite people with disability reporting higher levels of loneliness than the general population, there has been little research into how this is affecting their health and wellbeing. In light of this, the aim of our study was to scope both the existing evidence about the health and wellbeing outcomes associated with loneliness for people with disability, as well as the conceptual frameworks and measures utilised in this field of research.
Methods
To conduct this sco** review, we followed the methodology outlined by JBI and searched MEDLINE, Scopus, Informit, Embase, and Web of Science for peer-reviewed, English-language articles published between 1 January 2000 and 8 February 2023. Two independent reviewers completed screening, full-text review and data extraction, with consensus sought at each stage. Data were analysed using content analysis and presented both numerically and narratively.
Results
Out of the initial 1602 publications identified in the sco** review, only nine were included after duplicate removal, title and abstract screening, and full-text review. This limited number of studies, with the earliest study one published in 2015, represents a key finding. Eight of the nine studies were quantitative, and all were conducted in high income countries. Most of these studies utilised a version of the University of Los Angles Loneliness Scale to measure loneliness and addressed specific impairment groups. Notably, most of the studies identified associations between loneliness and health and wellbeing outcomes for people with disability.
Conclusions
This sco** review highlights the current scarcity of studies examining the effect that loneliness has on the health and wellbeing outcomes of people with disability. As most of the reviewed studies relied on loneliness measures designed for individuals without disability, they potentially overlook the unique life experiences of people with disability. Given that loneliness is an international public health concern, it is imperative that people with disability are not left behind or overlooked in efforts to address the impact of loneliness on health and wellbeing.
Similar content being viewed by others


Background
Meaningful social connections are essential for humans to thrive. Loneliness, defined as a “a subjective unpleasant or distressing feeling of a lack of connection to other people, along with a desire for more, or more satisfying, social relationships” [1], is closely linked to the quality of social connections as opposed to the quantity [2]. Globally, there is a growing concern about the rates and health consequences of loneliness [1, 3,4,5,6], with it now considered a public health priority [7, 8].
As noted in the editorial associated with this loneliness special issue, people with the greatest social disadvantage and marginalisation may have the highest rates of loneliness [8]. People with disability are one such vulnerable group. We know from previous research that they are more likely to report being lonely compared to those without disability [9,10,11]. For instance, analysis of data collected between 2016 and 2019 from the English Community Life survey, a nationally representative sample of approximately 17,000 adults, found that people with disability were over three times more likely to report feelings of loneliness than their peers without disability [9]. In a further study, Emerson and colleagues (2021) drew on the 2016–2019 waves of the United Kingdom (UK) Understanding Society survey, a nationally representative sample of approximately 35,000 adults, and found that adults with persistent disability (not just disability at some point in time) were over five times more likely to report ‘substantial’ loneliness than those without disability [10]. In both studies, disability is identified in the surveys by an affirmative response to two questions: the first asking about physical or mental health conditions or illnesses lasting or expected to last for 12 months or more and the second asking about whether the condition or illness result in difficulties carrying out day-to-day activities [9, 10].
People with disability are not a homogeneous group, for example it is likely that loneliness may be experienced quite differently by someone with severe intellectual disability and someone with a physical impairment associated with spinal cord injury. Some studies have suggested the degree of loneliness may be related to impairment. For example, an Australian study using data from the 2019 Household, Income and Labour Dynamics in Australia (HILDA) Survey found that working age people with psychosocial disability (47%) were most likely to experience loneliness while people with sensory disability (27%) were least likely to experience loneliness [12]. Stancliffe and colleagues (2010) in a study of over 13,000 users of intellectual and developmental disability services from 26 states in America found loneliness to be a widespread issue with 46% of all respondents reporting feeling lonely sometimes or often [13].
General population studies have shown that loneliness is associated with multiple adverse health outcomes, including a negative impact on mental health [6, 14,15,16,17], morbidity [17,18,19] and mortality [20, 21]. Given that people with disability are more likely to be at risk of loneliness, there is a high likelihood that they may also experience associated adverse health and wellbeing outcomes similar to or different from the general population. To the best of our knowledge there is no synthesis of the literature regarding the health and wellbeing outcomes associated with loneliness for people with disability.
Our primary aim was to scope the peer-reviewed published evidence about health and wellbeing outcomes associated with loneliness for ‘working age’ adults with disability (aged 15 – 64 years). Our second aim was to establish the conceptual frameworks and loneliness measures used by researchers studying this topic. Our third and final aim was to report the strengths, limitations, and gaps in the published literature.
Methods
We employed a sco** review methodology guided by the work of JBI [22, 23] and Levac and colleagues [24] in this area. The review was conducted in accordance with an a priori protocol that has been published [25]. Reporting was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Sco** Reviews (PRISMA-ScR) checklist [26]. Critical appraisal and risk of bias assessment of identified publications were not conducted, consistent with JBI methodology for sco** reviews.
Stage 1: research question
The sco** review research questions were as follows:
-
(1)
What, if any, health and wellbeing outcomes are associated with loneliness for people with disability of working age?
-
(2)
What conceptual frameworks and measures are being used to examine health and wellbeing outcomes associated with loneliness for people with disability?
-
(3)
What are the strengths, limitations and gaps in the published literature?
Stage 2: relevant literature identification
An initial search of MEDLINE and Google Scholar was conducted in January 2023 by the first author (JB) to identify relevant studies and generate a list of search terms. A full search strategy was developed for MEDLINE in consultation with an academic librarian (KE), and the senior author (GL) who has content expertise in the field of disability and loneliness (Table 1). To further ensure inclusivity we mapped our search results with references in recent publications about loneliness and disability. Embase, Informit, MEDLINE, Scopus and Web of Science were searched on 10 February 2023 (Additional file 1). The search was filtered to include peer-reviewed journal articles published in English between 1 January 2000 and 8 February 2023. The study also included hand searches of cited publications within eligible studies.
Stage 3: study selection
Inclusion criteria were identified and refined by the review team, according to the schema set out by JBI as follows.
Population
People with disability, aged 15–64 years, defined as having a long-term impairment or health condition lasting more than six months (including episodic conditions such as mental illness) that is associated with an activity limitation or participation restriction. We excluded studies in which the age of the participants was not given, or in which a sub-group of adults up to the age of 64 years could not be differentiated. The population of interest was those of school leaving age and prior to retirement to focus attention on adults of working age with lifelong or acquired disability and to exclude disability associated with the ageing process.
Concepts
Our focus was on studies examining the association between loneliness and health and wellbeing outcomes, including both the physical and psychological aspects. Studies that focused on social exclusion or social isolation, rather than loneliness, were excluded as these terms are considered conceptually different in the loneliness literature. We also excluded studies where the primary purpose was to examine, at a point in time, the impact of the COVID-19 pandemic on aspects of life for people with disability.
Context
All countries and settings.
Types of evidence sources
Original empirical research including quantitative, qualitative, mixed-methods study designs, and reviews (sco**, narrative, systematic and meta-analytical) published in English in a peer-reviewed journal. The index year of 2000 was selected to capture more than 20 years of publications. If the full-text version of a publication was not available, we contacted the corresponding authors to request one; if it was still not forthcoming, the publication was excluded.
The search results were exported to Endnote v.X9 [27], and duplicates removed before importing to Covidence (Veritas Health Innovation, Melbourne) [28] for screening. Following a pilot test, two independent reviewers (JB, GL) conducted title and abstract screening using the pre-defined inclusion and exclusion criteria. The same two reviewers independently completed full-text screening of abstracts and, subsequently, full-text review of included articles. Any discrepancies were then able to be resolved through discussion.
Stage 4: data extraction (data charting)
A data-charting tool aligned with the review questions, developed by JB and GL and inserted into Covidence, was used to extract information from eligible publications. The tool was developed a priori and piloted on four randomly selected studies, then refined through discussion and updated accordingly. No further changes were made to the data-extraction tool after piloting. Two reviewers (JB and GL) independently extracted data, then discussed and cross-checked their data extraction. In cases where extracted data differed between reviewers, consensus was reached through discussion.
Stage 5: data analysis and synthesis
Following JBI guidance, we conducted a qualitative content analysis [23, 29] on the extracted data using our first two research questions as the organising frame. Both reviewers (JB and GL) read and re-read the charted data plus revisited the source publications to review context as we independently worked through our analysis.
Deviations from the protocol
We note several deviations from the study protocol. Firstly, two independent reviewers screened all the titles and abstracts, as opposed to only 20 per cent of them as outlined in the protocol. Secondly, we excluded studies that were undertaken during the COVID-19 pandemic following the lead of Taylor et al. (2023) [8] in this special edition. In their editorial they rightly point out that loneliness is a phenomenon that is worthy of study in and of itself, irrespective of unusual social circumstances such as those experienced during the pandemic.
Results
Search results and study selection
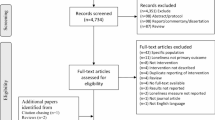
The literature search identified 1602 publications. After duplicate removal, title and abstract screening, and full text review, nine publications were included for review (Fig. 1).

Preferred Reporting of Items for Systematic Reviews and Meta-Analysis Extension for Sco** Reviews (PRISMA-ScR) selection of sources of evidence flow diagram
Study country and year of publication
All of the studies in the nine reviewed publications were undertaken in high-income countries [30], with the number of publications from each of the five countries listed here in descending order: UK (n = 4), United States of America (n = 2), Canada (n = 1), Taiwan (n = 1) and Switzerland (n = 1). These nine publications were all published between 2015 and 2022, with none published between 2000–2014. Table 2 presents a summary of the nine articles.
Study purpose
The stated aims or objectives of six of the nine studies focused on investigating the health and wellbeing outcomes associated with loneliness for people with disability [9, 10, 31, 42, 45, 48] (Additional file 2). The remaining three studies reported on health and wellbeing outcomes associated with loneliness in the context of other study aims or objectives [36, 50, 51].
Study methods and data sources
All nine studies (eight quantitative and one qualitative) used a type of cross-sectional study design. Seven of the nine utilised pre-existing data sources, which included population-level data from three separate national surveys conducted in the UK [9, 10, 42]: the English Adult Psychiatric Morbidity Survey, Understanding Society, and the Community Life Survey, (Understanding Society is a longitudinal cohort study; Emerson et al. 2021 [10] utilised cross-sectional analysis of 2 waves only). Additionally, data from existing longitudinal cohort studies for people with specific impairments / health conditions were used in two studies [45, 51], while in the remaining two studies data were collected as part of larger projects [31, 48].
Primary data collection methods – semi-structured life story interviews [50], and a self-administered paper-based questionnaire [36] – were employed in two of the nine studies.
Five of the nine studies drew comparisons between the health and wellbeing outcomes of people with disability and those without [9, 10, 36, 42, 51].
Disability study population
All studies addressed community-dwelling adults, with one exception: Smith and Caddick (2015) focused on those individuals living or who had lived in a care home within the previous six months.
The nine studies employed various ways to describe people with disability. Seven focused on specific impairment or diagnostic groups, including those with spinal cord injury [45, 48, 50, 51], autism spectrum disorder [36], multiple sclerosis [31], and borderline intellectual impairment [42]. In contrast, two studies focused on people with disability as a group without differentiating by impairment or disability type [9, 10].
Six different approaches to determining disability status were taken. Three studies relied on positive responses to one or more disability-related questions in a survey [9, 10, 42]. Two relied on self-reporting of disability along with either a confirmed diagnosis by a registered psychiatrist [36] or being officially registered as disabled by a government authority [50]. Of the remaining four studies, two confirmed disability status by registration on a disability research register [31, 51], while the other two used patient attendance at a clinic or rehabilitation centre [45, 48].
Loneliness conceptual framework
Seven studies based their understanding of loneliness on one of two well-known conceptual frameworks about loneliness, with the remaining two publications not providing a conceptualisation of loneliness [36, 50]. The most frequently used conceptual framework was that developed by Perlman and Peplau [31, 32, 42, 45, 48]. This approach defines loneliness as the discrepancy between a person’s desired and actual social relationships. According to Perlman and colleagues, loneliness is characterised as “the unpleasant experience that occurs when a person’s network of social relations is deficient in some important way, either quantitatively or qualitatively” [32]. This conceptualisation emphasises the objective (and therefore potentially measurable) features of an individual’s social network that may contribute to feelings of loneliness. The remaining three studies [9, 10, 51] drew on the conceptual framework proposed by Hawkley and Cacioppo [38]. This framework, in contrast to the objective features approach by Perlman and colleagues, emphasises the subjective experience of loneliness. According to this perspective, loneliness exists when an individual perceives a lack of desired social connections, regardless of the quantity or quality of their social network.
Loneliness measures
Six of the eight quantitative studies used a version of the University of California Los Angeles Loneliness Scale (UCLA-LS) (Table 3) as the measure of loneliness: four employed the UCLA-LS 3-Item version [9, 45, 48, 51], one the original UCLA-LS 20-Item version, [31] and the remaining study used the UCLA-LS 8-Item Chinese version [36].
The two studies, conducted by Emerson and colleagues (2021) [9, 10], were dependent on the loneliness measure incorporated in national surveys designed by the Office of National Statistics, which asks the question, “How often do you feel lonely?” [57]. The first study used the UCLA-LS 3-Item in addition to the single Office of National Statistics item [9], while the second study only used the single Office of National Statistics loneliness item found in the English Community Life Survey [10].
One study used a single item from the Social Functioning Questionnaire: “I feel lonely and isolated from other people” [42]. In their qualitative study, Smith and Caddick (2015) [50] posed a range of open-ended questions, including, “Can you tell me about your life in the care home”, “Can you describe how it feels to be living in a care home”. The impact of loneliness on health and wellbeing outcomes were identified by thematic analysis of the qualitative responses.
Health and wellbeing measures
There were 16 different approaches to assessing health and wellbeing outcomes in the eight quantitative studies (Table 2). Mental health and wellbeing outcomes measured included the followingFootnote 1 (i) anxiety [9, 31, 36, 42]; (ii) depression [31, 45]; (iii) suicidal ideation [42]; (iv) wellbeing [42]; (v) life satisfaction [9, 45, 48]; (vi) vitality [51]; (vii) worth [9]; and (viii) happiness [9]. Physical health outcomes reported included functional limitations as a result of fatigue [31], self-reporting of health status [42], and identification of a chronic disease in the past 12 months [42]. The qualitative study used an inductive thematic analysis approach to identify the themes related to the health and wellbeing outcomes caused by loneliness for people with disability [50].
Association between loneliness and health and wellbeing for people with disability
In Table 4 we present a summary of the identified associations between loneliness and health and wellbeing outcomes for people with disability, according to the measures used in each study. Additional file 3 provides extracts from studies on health and wellbeing outcomes.
Discussion
Main findings of this study
In this sco** review covering more than two decades of literature, we only identified nine articles that examined the association between loneliness and health and wellbeing outcomes for people with disability. Key findings from this sco** review suggest that research on this topic is just beginning to emerge, with the earliest study only published in 2015. Our findings demonstrate that: (i) relatively few studies have examined whether loneliness is associated with health and wellbeing (including adverse outcomes) for people with disability; (ii) even fewer studies use a comparison group of people without disability; (iii) the studies examine a wide range of health and wellbeing outcomes, which limits the conclusions that can be drawn from them; (iv) most studies continue to focus on people from specific impairment groups rather than from the broader population of people with disability; and (v) the studies predominantly rely on self-reported items about loneliness and a small suite of loneliness measures that, to the best of our knowledge, have not been evaluated for their validity in assessing the loneliness experienced by people with disability. Of note, all the studies came from high-income countries.
That said, our findings suggest that loneliness for people with disability is associated with poorer health and wellbeing, specifically mental health, but also poorer physical health in the studies where it has been possible to examine this outcome. These findings provide the impetus to develop our program of research further, with the aim of extending it beyond prevalence and correlational studies to incorporate study designs that examine the directionality of the association between poorer health and wellbeing outcomes and loneliness, and possible causality. Fried et al. (2020) [4] have also drawn attention to the need for more research into the impacts of loneliness on health and wellbeing outcomes for the general population.
All the studies reviewed used cross-sectional study designs. This highlights the need for longitudinal studies that examine this relationship between loneliness and health and wellbeing outcomes for people with disability and whether the association has persisted over time. As no low and middle-income country studies were included in this review there is a need for disability, loneliness and health and wellbeing research in these contexts.
The extant literature on loneliness and health and wellbeing outcomes for people with disability is currently limited to the two major conceptual approaches found for the general population and associated instruments to measure loneliness. This leaves a significant gap in understanding loneliness for people with disability and association with or impact on their health and wellbeing. There are two major concerns: the first relates to the loneliness measures used; and the second to the possible interactions between loneliness and health and wellbeing for people with disability.
Firstly, understanding the lived experience of loneliness for people with disability needs attention. As with other reviews that have examined loneliness measures, we found the UCLA-LS to be by far the most frequently used [59, 60]. It may be the case, as in other life areas, that the loneliness people with disability experience differs somewhat from those of their peers without disability, e.g., in the frequently experienced discrimination in public places [61]. If this is the case, it may be that the UCLA-LS and other measures currently used, although capable of uncovering significant differences in the prevalence of loneliness between people with disability and those without, may need to be revised or expanded to capture the nature and full extent of the loneliness experienced by people with disability. Similar to Gomez-Zuniga and colleagues (2023), we identified a lack of qualitative studies that explore the subjective experience of loneliness for people with disability. This is a major shortcoming given that loneliness is typically defined as a subjective unpleasant or distressing feeling [60].
Secondly, the loneliness literature for the general population suggests that loneliness and health have a bi-directional and cyclical relationship, meaning that each can influence the other [62, 63]. While this may also be the case for people with disability, there may be other factors at play. It is well established that people with disability experience inequalities in health care, resulting in poorer physical and mental health outcomes than people without disability [64,65,66]. This is especially important when considering associations between loneliness and health and wellbeing outcomes given that the increased prevalence of both issues could simply be due to the experience of disability, rather than loneliness promoting certain health and wellbeing outcomes or that certain health and wellbeing outcomes promote loneliness. It could be, for example, as the Emerson et al. 2021 [10] study included in this review demonstrated, that the association between loneliness and poorer health and wellbeing outcomes occurs only with persistent disability, potentially suggesting a cyclical relationship. It is still unclear from the literature whether this is the case for people with disability, but given the higher prevalence of loneliness for people with disability it does warrant further examination in the interests of promoting better health and wellbeing outcomes.
Strengths and limitations
The strengths of our sco** review are: 1) a published a priori protocol [25] that improves the transparency and reproducibility of the sco** review; 2) the rigorous process of two reviewers independently conducting title and abstract screening, full text review and data extraction, and engaging in robust discussions to reach consensus at every stage; and 3) a search strategy designed with both an experienced academic librarian (KE) and a well-qualified research team.
Review limitations include: 1) the risk of language bias as only publications in English were included; 2) potentially missing relevant evidence as we excluded grey literature, including theses.; and 3) potentially missing relevant studies if they focused on specific impairment groups and did not use the terms ‘disability’ or ‘impairment’.
Conclusions
This sco** review highlights the nascent state of research on the health and wellbeing outcomes associated with loneliness for people with disability. The scarcity of studies, the lack of comparison groups of people without disability, the reliance on measures designed for individuals without disability, and the narrow focus on specific impairments pose challenges to a comprehensive understanding of the topic. This is regrettable given the rise in loneliness reported in many countries and the ongoing impact of the isolation from their fellows that many people experienced during the COVID-19 pandemic. Work in several countries including Australia is attempting to understand the drivers of loneliness as COVID-19 and post-COVID 19 population data becomes available. It will be important that this work includes consideration of people with disability to understand the nature and extent of the impact of loneliness on their health and wellbeing and to ensure that they are not overlooked or left behind in any public health interventions for loneliness for the general population.
Availability of data and materials
All data and materials generated or analysed are included in this article.
Notes
The wellbeing measure used in the study by Emerson et al. (2021) has four components that are measured separately – satisfaction, anxiety, happiness and worth. We report these separately to align with the study publication.
References
Badcock JC, Holt-Lunstad J, Garcia,E, Bombaci P, & Lim MH. Position Statement: Addressing Social Isolation and Loneliness and the Power of Human Connection. Global Initiative on Loneliness and Connection (GILC). 2022. Available at: <https://www.gilc.global/general-6Accessed 5 Sept 2023.
Masi CM, Chen HY, Hawkley LC, Cacioppo JT. A meta-analysis of interventions to reduce loneliness. Pers Soc Psychol Rev. 2011;15(3):219–66. https://doi.org/10.1177/1088868310377394.
Lim MH, Eres R, Vasan S. Understanding loneliness in the twenty-first century: an update on correlates, risk factors, and potential solutions. Soc Psychiatry Psychiatr Epidemiol. 2020;55(7):793–810. https://doi.org/10.1007/s00127-020-01889-7.
Fried L, Prohaska T, Burholt V, et al. A unified approach to loneliness. Lancet. 2020;395(10218):114. https://doi.org/10.1016/S0140-6736(19)32533-4.
Surkalim DL, Luo M, Eres R, et al. The prevalence of loneliness across 113 countries: systematic review and meta-analysis. BMJ. 2022;376:e067068. https://doi.org/10.1136/bmj-2021-067068. Published 2022 Feb 9.
Cacioppo JT, Cacioppo S. The growing problem of loneliness. Lancet. 2018;391(10119):426. https://doi.org/10.1016/S0140-6736(18)30142-9.
O’Sullivan R, Leavey G, Lawlor B. We need a public health approach to loneliness. BMJ. 2022;376:o280. https://doi.org/10.1136/bmj.o280. Published 2022 Feb 9.
Taylor HO, Cudjoe TKM, Bu F, Lim MH. The state of loneliness and social isolation research: current knowledge and future directions. BMC Public Health. 2023;23(1):1049. https://doi.org/10.1186/s12889-023-15967-3. Published 2023 Jun 1.
Emerson E, Fortune N, Llewellyn G, Stancliffe R. Loneliness, social support, social isolation and wellbeing among working age adults with and without disability: Cross-sectional study. Disabil Health J. 2021;14(1):100965. https://doi.org/10.1016/j.dhjo.2020.100965.
Emerson E, Stancliffe R, Fortune N, Llewellyn G. Disability, Loneliness and Health in the UK: cross-sectional survey. Eur J Public Health. 2021;31(3):533–8. https://doi.org/10.1093/eurpub/ckab018.
McGlone M, Long E. Are young adults with long-standing illness or disability at increased risk of loneliness? Evidence from the UK Longitudinal Household Study. J Public Health Res. 2020;9(4):1861. https://doi.org/10.4081/jphr.2020.1861. Published 2020 Dec 21.
DSS (Department of Social Services) and MIAESR (Melbourne Institute of Applied Economic Social Research). The Household, Income and Labour Dynamics in Australia (HILDA) Survey, General Release 18 (Wave 17). Available at https://dataverse.ada.edu.au/dataset.xhtml?persistentId=doi:10.26193/IYBXHM. Accessed 5 Sept 2023.
Stancliffe RJ, Larson S, Auerbach K, Engler J, Taub S, Lakin KC. Individuals with Intellectual disabilities and augmentative and alternative communication: Analysis of survey data on uptake of aided AAC, and loneliness experiences. Augment Altern Commun. 2010;26(2):87–96.
Wang J, Mann F, Lloyd-Evans B, Ma R, Johnson S. Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatry. 2018;18(1):156. https://doi.org/10.1186/s12888-018-1736-5. Published 2018 May 29.
Mann F, Wang J, Pearce E, et al. Correction to: Loneliness and the onset of new mental health problems in the general population. Soc Psychiatry Psychiatr Epidemiol. 2022;57(11):2179. https://doi.org/10.1007/s00127-022-02337-4.
Lee SL, Pearce E, Ajnakina O, et al. The association between loneliness and depressive symptoms among adults aged 50 years and older: a 12-year population-based cohort study. Lancet Psychiatry. 2021;8(1):48–57. https://doi.org/10.1016/S2215-0366(20)30383-7.
Park C, Majeed A, Gill H, et al. The Effect of Loneliness on Distinct Health Outcomes: A Comprehensive Review and Meta-Analysis. Psychiatry Res. 2020;294:113514. https://doi.org/10.1016/j.psychres.2020.113514.
Petitte T, Mallow J, Barnes E, Petrone A, Barr T, Theeke L. A Systematic Review of Loneliness and Common Chronic Physical Conditions in Adults. Open Psychol J. 2015;8(Suppl 2):113–32. https://doi.org/10.2174/1874350101508010113.
Valtorta NK, Kanaan M, Gilbody S, Ronzi S, Hanratty B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: systematic review and meta-analysis of longitudinal observational studies. Heart. 2016;102(13):1009–16. https://doi.org/10.1136/heartjnl-2015-308790.
Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci. 2015;10(2):227–37. https://doi.org/10.1177/1745691614568352.
Rico-Uribe LA, Caballero FF, Martín-María N, Cabello M, Ayuso-Mateos JL, Miret M. Association of loneliness with all-cause mortality: A meta-analysis. PLoS One. 2018;13(1):e0190033. https://doi.org/10.1371/journal.pone.0190033. Published 2018 Jan 4.
Munn Z, Pollock D, Khalil H, et al. What are sco** reviews? Providing a formal definition of sco** reviews as a type of evidence synthesis. JBI Evid Synth. 2022;20(4):950–2. https://doi.org/10.11124/JBIES-21-00483. Published 2022 Apr 1.
Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of sco** reviews. JBI Evid Synth. 2020;18(10):2119–26. https://doi.org/10.11124/JBIES-20-00167.
Levac D, Colquhoun H, O’Brien KK. Sco** studies: advancing the methodology. Implement Sci. 2010;5:69. https://doi.org/10.1186/1748-5908-5-69. Published 2010 Sep 20.
Bailie J, Ekanayake K, Llewellyn G. Health and wellbeing consequences of loneliness for people with disability: sco** review protocol. Open Science Framework. 2023. Available at: <https://osf.io/vguj8/Accessed 5 Sept 2023.
Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Sco** Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–73. https://doi.org/10.7326/M18-0850.
The EndNote Team, EndNote Version X9. Clarivate Analytics, Philadelphia.
Covidence Systematic Review Software. Melbourne, Australia: Veritas Health Innovation. Available at: < https://www.covidence.orgAccessed 9 Jul 2023.
Pollock D, Peters MDJ, Khalil H, et al. Recommendations for the extraction, analysis, and presentation of results in sco** reviews. JBI Evid Synth. 2023;21(3):520–32. https://doi.org/10.11124/JBIES-22-00123. Published 2023 Mar 1.
The World Bank. The World by Income and Region. World Bank. 2022. Available at: <https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.htmlAccessed 5 Sept 2023.
Balto JM, Pilutti LA, Motl RW. Loneliness in Multiple Sclerosis: Possible Antecedents and Correlates. Rehabil Nurs. 2019;44(1):52–9. https://doi.org/10.1097/rnj.0000000000000128.
Perlman D. Toward a social psychology of loneliness. In: Duck S, Gimour R, editors. Personal Relationships in Disorder, vol. 3. London, UK: Academic Press; 1981. p. 31–56.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–70.
Fisk JD, Ritvo PG, Ross L, Haase DA, Marrie TJ, Schlech WF. Measuring the functional impact of fatigue: initial validation of the fatigue impact scale. Clin Infect Dis. 1994;18(Suppl 1):S79–83. https://doi.org/10.1093/clinids/18.supplement_1.s79.
McGuigan C, Hutchinson M. The multiple sclerosis impact scale (MSIS-29) is a reliable and sensitive measure. J Neurol Neurosurg Psychiatry. 2004;75(2):266–9.
Chang YC, Chen CH, Huang PC, Lin LY. Understanding the characteristics of friendship quality, activity participation, and emotional well-being in Taiwanese adolescents with autism spectrum disorder. Scand J Occup Ther. 2019;26(6):452–62. https://doi.org/10.1080/11038128.2018.1449887.
Che H-H, Lu M-L, Chen H-C, Chang S-W, Lee Y-J. Validation of the Chinese version of the Beck Anxiety Inventory. Formos J Med. 2006;10(4):451–2.
Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. 2010;40(2):218–27. https://doi.org/10.1007/s12160-010-9210-8.
Office for National Statistics. Measuring Loneliness: Guidance for use of the National Indicators on Surveys. United Kingdom. 2018. Available at: <https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/methodologies/measuringlonelinessguidanceforuseofthenationalindicatorsonsurveysAccessed 5 Sept 2023.
Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–33. https://doi.org/10.1097/00005650-199603000-00003.
Goldberg D, Williams P. A User's Guide to the General Health Questionnaire. Windsor. 1988.
Papagavriel K, Jones R, Sheehan R, Hassiotis A, Ali A. The association between loneliness and common mental disorders in adults with borderline intellectual impairment. J Affect Disord. 2020;277:954–61. https://doi.org/10.1016/j.jad.2020.09.005.
Stewart-Brown SL, Platt S, Tennant A, Maheswaran H, Parkinson J, Weich S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): a valid and reliable tool for measuring mental well-being in diverse populations and projects. J Epidemiol Community Health. 2011;65(Suppl 2):A38–9.
Lewis G, Pelosi AJ, Araya R, Dunn G. Measuring psychiatric disorder in the community: a standardized assessment for use by lay interviewers. Psychol Med. 1992;22(2):465–86. https://doi.org/10.1017/s0033291700030415.
Robinson-Whelen S, Taylor HB, Feltz M, Whelen M. Loneliness Among People With Spinal Cord Injury: Exploring the Psychometric Properties of the 3-Item Loneliness Scale. Arch Phys Med Rehabil. 2016;97(10):1728–34. https://doi.org/10.1016/j.apmr.2016.04.008.
Whiteneck GG, Charlifue SW, Gerhart KA, Overholser JD, Richardson GN. Quantifying handicap: a new measure of long-term rehabilitation outcomes. Arch Phys Med Rehabil. 1992;73(6):519–26.
Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49(1):71–5.
Santino N, Larocca V, Hitzig SL, Guilcher SJT, Craven BC, Bassett-Gunter RL. Physical activity and life satisfaction among individuals with spinal cord injury: Exploring loneliness as a possible mediator. J Spinal Cord Med. 2022;45(2):173–9. https://doi.org/10.1080/10790268.2020.1754651.
Fugl-Meyer AR, Melin R, Fugl-Meyer KS. Life satisfaction in 18- to 64-year-old Swedes: in relation to gender, age, partner and immigrant status. J Rehabil Med. 2002;34(5):239–46. https://doi.org/10.1080/165019702760279242.
Smith B, Caddick N. The impact of living in a care home on the health and wellbeing of spinal cord injured people. Int J Environ Res Public Health. 2015;12(4):4185–202. https://doi.org/10.3390/ijerph120404185. Published 2015 Apr 15.
Tough H, Fekete C, Brinkhof MWG, Siegrist J. Vitality and mental health in disability: Associations with social relationships in persons with spinal cord injury and their partners. Disabil Health J. 2017;10(2):294–302. https://doi.org/10.1016/j.dhjo.2016.12.008.
Ware JE. SF-36 Health Survey. Manual and Interpretation Guide. The Health Institute. 1993:6: 1–6: 22.
Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–72. https://doi.org/10.1177/0164027504268574.
Tough H, Gross-Hemmi M, Eriks-Hoogland I, Fekete C. Pathways to loneliness: a mediation analysis investigating the social gradient of loneliness in persons with disabilities in Switzerland. Int J Equity Health. 2021;20(1):261. https://doi.org/10.1186/s12939-021-01600-5. Published 2021 Dec 20.
Russell D, Peplau LA, Ferguson ML. Develo** a measure of loneliness. J Pers Assess. 1978;42(3):290–4. https://doi.org/10.1207/s15327752jpa4203_11.
Wu C-h, Yao G. Psychometric analysis of the short-form UCLA Loneliness Scale (ULS-8) in Taiwanese undergraduate students. Pers Individ Differ. 2008;44(8):1762–71.
Office for National Statistics. Measuring Loneliness: Guidance for Use of the National Indicators on Surveys. 2018. Available: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/methodologies/measuringlonelinessguidanceforuseofthenationalindicatorsonsurveys, Accessed 5 Sept 2023.
Tyrer P, Nur U, Crawford M, et al. The Social Functioning Questionnaire: a rapid and robust measure of perceived functioning. Int J Soc Psychiatry. 2005;51(3):265–75.
Maes M, Qualter P, Lodder GMA, Mund M. How (Not) to Measure Loneliness: A Review of the Eight Most Commonly Used Scales. Int J Environ Res Public Health. 2022;19(17):10816. https://doi.org/10.3390/ijerph191710816. Published 2022 Aug 30.
Gómez-Zúñiga B, Pousada M, Armayones M. Loneliness and disability: A systematic review of loneliness conceptualization and intervention strategies. Front Psychol. 2023;13:1040651. https://doi.org/10.3389/fpsyg.2022.1040651. Published 2023 Jan 25.
Wayland S, Newland J, Gill-Atkinson L, Vaughan C, Emerson E, Llewellyn G. I had every right to be there: discriminatory acts towards young people with disabilities on public transport. Disabil Soc. 2022;37(2):296–319.
Nuyen J, Tuithof M, de Graaf R, van Dorsselaer S, Kleinjan M, Have MT. The bidirectional relationship between loneliness and common mental disorders in adults: findings from a longitudinal population-based cohort study. Soc Psychiatry Psychiatr Epidemiol. 2020;55(10):1297–310. https://doi.org/10.1007/s00127-019-01778-8.
Phillips DM, Finkel D, Petkus AJ, et al. Longitudinal analyses indicate bidirectional associations between loneliness and health. Aging Ment Health. 2023;27(6):1217–25. https://doi.org/10.1080/13607863.2022.2087210.
Krahn GL, Walker DK, Correa-De-Araujo R. Persons with disabilities as an unrecognized health disparity population. Am J Public Health. 2015;105(Suppl 2):S198–206. https://doi.org/10.2105/AJPH.2014.302182.
Emerson E, Madden R, Graham H, Llewellyn G, Hatton C, Robertson J. The health of disabled people and the social determinants of health. Public Health. 2011;125(3):145–7. https://doi.org/10.1016/j.puhe.2010.11.003.
Shea B, Bailie J, Dykgraaf SH, Fortune N, Lennox N, Bailie R. Access to general practice for people with intellectual disability in Australia: a systematic sco** review. BMC Prim Care. 2022;23(1):306. https://doi.org/10.1186/s12875-022-01917-2. Published 2022 Nov 29.
Funding
This research is supported by the NHMRC Centre for Research Excellence in Disability Health, grant #1116385 and NHMRC Synergy Grant ‘Develo** interventions for better life-time mental health for young Australians (aged 15 to 24 years) with disability’, grant #2010290. HB is supported by an RMIT Vice-Chancellor’s Senior Research Fellowship.
Author information
Authors and Affiliations
Contributions
JB and GL designed the study; KE, an academic librarian, assisted JB and GL in the development of search terms and extraction of publications from library databases; JB and GL screened the papers and undertook data extraction. JB led the analysis and writing of the manuscript, in collaboration with GL. All authors critically reviewed draft versions of the manuscript, revisions were made in response to their input, and all authors gave final approval of the version to be published.
Author note
Within the author team, one researcher identified as having a disability (GB) and two researchers JB and GL (first and senior authors) identified as having close family members with disability. All authors are deeply committed to improving the health outcomes of people with disability.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
No ethics approval was required and consent to participate is not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search terms.
Additional file 2.
Aims and objectives of included studies.
Additional file 3.
Health and wellbeing associations with loneliness identified in studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bailie, J., Bishop, G.M., Badland, H. et al. Health and wellbeing outcomes associated with loneliness for people with disability: a sco** review. BMC Public Health 23, 2361 (2023). https://doi.org/10.1186/s12889-023-17101-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-17101-9