
Abstract
Background
Children and adolescents have suboptimal physical activity and eating habits during summer breaks. Unlike the school setting, there is little evidence on interventions to promote healthy lifestyle behaviors in Summer Day Camps (SDCs).
Methods
The aim of this sco** review was to examine physical activity, healthy eating, and sedentary behavior interventions in the SDCs. A systematic search on four platforms (EBSCOhost, MEDLINE, EMBASE, and Web of Science) was performed in May 2021 and was updated in June 2022. Studies related to promoting healthy behaviors, physical activity, sedentary behaviors and/or healthy eating among campers aged 6 to 16 in Summer Day Camps were retained. The protocol and writing of the sco** review were done according to the guidelines of the “Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for sco** reviews (PRISMA-ScR)”.
Results
Most interventions had a positive effect on the behavioral determinants or the behaviors themselves (i.e., physical activity, sedentary behaviors, or healthy eating). Involving counsellors and parents, setting camp goals, gardening, and education are all relevant strategies in promoting healthy lifestyle behaviors in SDCs.
Conclusions
Since only one intervention directly targeted sedentary behaviors, it should strongly be considered for inclusion in future studies. In addition, more long-term and experimental studies are needed to establish cause-and-effect relationships between healthy behavior interventions in SDCs and behaviors of children and young adolescents.
Similar content being viewed by others


Introduction
The promotion of healthy lifestyle behaviors such as physical activity and healthy eating is a priority among children and adolescents, especially since the healthy behaviors developed early in life persist into adulthood [1]. Regular physical activity and healthy eating habits can improve musculoskeletal health, decrease symptoms of anxiety, depression, and risk of chronic disease, and promote academic performance [2]. While there appears to be difficulty meeting recommendations for both physical activity and nutrition during school [3], one would expect children and young adolescents to be more active during summer breaks and have better eating habits given the increased supply of fresh fruits and vegetables. However, physical activity during this period is rather marked by weight gain and a decline in fitness [4, 5] partially explained by a lack of organization of activities and support by adults regularly offered through institutions such as school or extracurricular programs [6]. Summer can also present an open and autonomous environment for children that can negatively influence their eating habits [7]. Indeed, during summer breaks, many children and adolescents do not accumulate 60 min of moderate-to-vigorous physical activity (MVPA) per day [8] as recommended by the most recent 24-h guidelines [9]. They also have low consumption of vegetables, and high consumption of sugar-sweetened beverages (SSB) [8] contrary to what is recommended by the 2019 Canada's Food Guide [10].
Considered a setting for organized activities for children during summer breaks, Summer Day Camps (SDCs) appear to be a good solution to the problem of organization and supervision of activities. However, even if SDCs address the lack of organization and support, they do not necessarily offer opportunities for children and young adolescents to be physically active for at least 60 min per day. Observation tools in SDCs showed that only 38% of weekly plans were devoted to physical activity and that only 19% and 18% of children and adolescents participating in physical activities organized by the camps were engaged in moderate or vigorous physical activity, respectively [11]. In addition, an observational study among campers showed that only 20% and 4% of lunch boxes contained a fruit and a vegetable, respectively [12]. This study also concluded that 47% of campers had brought non-100% juice and 4% had soft drinks in their lunch boxes, indicating a large intake of SSB [12]. The fluid intake of campers also seems inadequate considering that many of them drank no beverages at all at any of the meals across the entire day [13]. Children and adolescents, therefore, have suboptimal physical activity and eating habits, especially during summer breaks. To date, there is little evidence on interventions to promote healthy lifestyle behaviors in SDCs to improve physical activity, sedentary behaviors, and eating habits of campers. The overall aim of this sco** review is to describe the interventions promoting healthy lifestyle behaviors in children and adolescents, particularly those that involve physical activity, sedentary behaviors, and healthy eating in SDCs settings in order to guide further interventions.
Methods
Design
This study used the sco** literature review design described by Arksey and O’Malley [14] to explore the available literature, guide future interventions, and pave the way for further systematic reviews based on gaps in this research area. According to this design, the quality of the studies was not assessed and does not constitute a condition for rejection [14]. This sco** review conforms to the “Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for sco** reviews (PRISMA-ScR)” [15].
Research questions
The purpose of this sco** review is 1) to map the interventions promoting healthy lifestyle behaviors, particularly those that involve physical activity, sedentary behaviors, and healthy eating in SDC settings, and 2) to describe the effects on campers and identify gaps and promising strategies for future interventions.
Identifying relevant studies
A literature search was performed with the support of an experienced librarian (Marie Denise Lavoie) in May 2021 and was updated in June 2022 to capture the studies. The following platforms were accessed: SPORTDiscus, CHILD DEVELOPMENT & ADOLESCENT STUDIES, ERIC, EDUCATION SOURCE, MEDLINE, EMBASE, and Web of Science [See Additional file 1 for detailed search methodology].
A targeted search based on the concepts "promotion of healthy lifestyles and/or health" OR "physical activity" OR "eating habits" AND "Summer Day Camp" was carried out, with variants adapted for each database, if applicable. To be included in the review, studies must a) be related to the promotion of healthy behaviors; b) be related to physical activity, sport, exercise, outdoor games, sedentary behavior and/or diet, eating habits, nutrition, and healthy eating; c) be in Summer Day Camps of varying lengths to which access is public and not private; and d) include a sample of children and young adolescents aged 6 to 16 years. The following items have been excluded: a) studies related to a setting that includes cam**; b) studies related to a framework specific to public holidays; c) studies related to a framework that includes school environments; d) studies related to a framework that includes specific food consumption; e) studies related to a framework that includes eating disorders; f) studies in which the sample includes specific conditions (e.g., weight loss camp, those diagnosed with severe mental illness or physical disability); g) unpublished studies or non-intervention studies; and h) articles that were not in English or French.
Study selection
All references were imported into EndNote 20 software (Clarivate Analytics, Philadelphia, United States) and duplicates were removed using Covidence (i.e., a screening and data extraction tool). The remaining titles and abstracts were screened by two independent reviewers (DL, MCSC) using predetermined inclusion/exclusion criteria. Full texts were independently reviewed against inclusion/exclusion criteria. Discrepancies were resolved by a third independent reviewer (SP). Consensus was reached for all included articles.
Data charting
A data extraction table was created in Microsoft Excel by the research team by identifying different variables consistent with the objective of the sco** review. Then, two reviewers independently extracted information from relevant articles and charted the data using the same extraction table. The key variables included citation, research question, framework, sample population (i.e., the number of participants who were considered for the statistical analysis, not the complete sample), research design, data collection methods and measures, counsellors’ implication, intervention, and main results based on campers and environment (i.e., counsellors, parents, SDCs setting).
Collecting, summarizing, and reporting the results
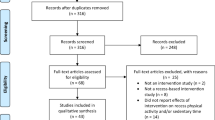
The PRISMA diagram was used to illustrate the review process and specifies the number of articles rejected for each of the main reasons for exclusion (Fig. 1). The data from the approved articles were synthesized and classified according to the variables previously presented in an excel document.

PRISMA flow diagram of study selection process
Results
Study characteristics
A total of 1941 articles were initially identified and imported into the Endnote and then Covidence software. After removing duplicates (n = 541), a total of 1400 articles were screened by title and abstract, 171 articles were full text filtered, and 28 studies met our eligibility criteria. The main reasons for exclusion were study design (e.g., there was no intervention), article availability (e.g., some were impossible to find while many were only abstracts of published conferences), participants (e.g., children had specific health problems such as diabetes or vision problems), study outcomes were not relevant (e.g., weight or waist circumference) or the language (i.e., the article was not in English or French). Of the articles selected, eight interventions specifically targeted the promotion of physical activity, fourteen interventions focused on healthy eating, five targeted both physical activity and healthy eating, and one intervention was specific to physical activity, sedentary behaviors, and healthy eating. Among all these interventions, only five are not based on precise theoretical frameworks [16,17,18,19,20]. To measure the effects of these interventions, seven studies used an experimental design, eighteen studies used a quasi-experimental design, two studies used a mixed methods design, and one study used a qualitative design. Sixteen of the studies using a quasi-experimental design did not have a control group and seventeen did not randomize their sample. Most of these studies used a pre- and post-intervention design and seven studies had a follow-up. All the studies were cross-sectional, except for four longitudinal studies. Three of the cross-sectional studies measured the effects of the intervention over several years (i.e., more than one year), but with different groups of campers (Table 1).
Measurement of physical activity, sedentary behaviors, and healthy eating
Of the fourteen studies that assessed physical activity, twelve of them measured the effects of promoting physical activity on the physical activity of children and young adolescents [17,18,19, 21, 24, 25, 34, 38,39,40,41, 43], while the other two only measured the effects of the interventions on determinants of physical activity. Physical activity (PA) was measured using accelerometers/pedometers in five studies [21, 24, 25, 40, 43], using questionnaires (i.e., self-reported data) in six studies [17,18,19, 21, 34, 41], and using a validated time-sampling observation tool (SOPLAY) in three studies [25, 38, 39]. For the evaluation of the determinants of physical activity using questionnaires, one study measured intention and self-efficacy [16], one study measured physical literacy and barriers towards physical activity [37], two studies measured knowledge and attitudes towards physical activity [17, 41], and one study measured enjoyment [43].
Among the twenty articles that evaluated interventions targeting the promotion of healthy eating, twelve studies measured eating habits [19, 21, 23, 24, 26, 28, 30,31,32, 34, 36, 41]. Eight studies used questionnaires [19, 26, 28, 30,31,32, 34, 41], three used observations [23, 30, 36], and two of them used 24-h dietary recalls [21, 24]. The main determinants of healthy eating measured were food preferences, liking, knowledge, self-efficacy, motivation, environment, exposure, availability, cooking skills, cooking behavior, involvement in family meals, and attitudes [17, 20,21,22, 26,27,28,29, 31,32,33,34,35, 41, 42].
A few studies have measured the sedentary behaviors of campers, either with accelerometers/pedometers [24], observations (SOPLAY) [38, 39] or with questionnaires (i.e., screen time) [19, 41]. Nonetheless, only one intervention targeted sedentary behaviors [41].
Effect of Summer Day Camp interventions targeting physical activity or sedentary behaviors
Eight of the twelve studies that measured physical activity observed increases across different measures. Studies by Bohnert et al. [24], Gachupin et al. [17], Weaver, Beets, Saunders et al. [38], Weaver, Beets, Turner-McGrievy et al. [39], and Weaver et al. [40] measured increases in moderate-to-vigorous physical activity using different tools (i.e., accelerometer/pedometer, questionnaire, and SOPLAY). Kimiecik et al. [18] observed differences in how campers perceived their behaviors to be healthier after the summer. Reverter-Masia et al. [19] observed an increase in short- and long-term physical activity after the intervention and Wilson et al. [43] measured a greater number of steps taken by campers during the SDCs (Table 2).
The five studies that measured the determinants of physical activity observed increases following the interventions. Specifically, Gachupin et al. [17], Seal & Seal [34], and Werner et al. [41] measured increases in knowledge (e.g., how long they should be active each day and places where they can be active), Anderson-Butcher et al. [16], Seal & Seal [34], and Werner et al. [41] measured increases in perception of control (i.e., self-efficacy or self-perception of competence) while Gachupin et al. [17] and Wilson et al. [43] measured increases in positive attitude and enjoyment, respectively.
Only one intervention directly targeted sedentary behaviors, but a few studies whose intervention targeted physical activity still measured sedentary behaviors. Although few studies have ultimately measured sedentary behaviors, all those that have measured them have observed positive changes. In all cases, screen-time or television time [19, 24, 41] and sedentary time [38, 39] decreased during the summer or following the intervention.
Effects of Summer Day Camp interventions targeting healthy eating
Nine of the twelve studies that measured eating habits observed positive changes. Studies by Baranowski et al. [21], Beets et al. [23], Bohnert et al. [24], Mabary-Olsen et al. [31], Reverter-Masia et al. [19], Seal & Seal [34], Tilley et al. [36], and Werner et al. [41] measured increases in fruit and/or vegetable (FV) consumption and Baranowski et al. [21], Lawman et al. [30], and Tilley et al. [36] measured an increase in water consumption. These same studies measured a decrease in the consumption of sugary drinks among campers and counsellors [21, 30, 36]. Some studies such as Beets et al. [23], Reverter-Masia et al. [19], and Tilley et al. [36] also measured decreases in unhealthy behaviors (e.g., soda/pop, non-100% juice, chips, and fast food). Finally, some isolated studies measured a decrease in energy intake from lipids [21] or a decrease in the consumption of dairy products [19, 24].
Thirteen of the fifteen studies that measured the determinants of healthy eating observed increases following the interventions. Specifically, Beets et al. [22], Condrasky et al. [26], Gachupin et al. [17], Jacob et al. [20], Mabary-Olsen et al. [31], Seal & Seal [34], and Werner et al. [41] measured an increase in food-related knowledge. Beets et al. [22], Condrasky et al. [26], Harmon et al. [28], Mabary-Olsen et al. [31], Murad et al. [33], and Seal & Seal [34] measured increases in perceived control (i.e., self-efficacy or self-perception of competence towards cooking or healthy eating) while Beets et al. [22], Gachupin et al. [17], and Harmon et al. [28] measured favorable changes in attitudes towards healthy foods. Finally, Ehrenberg et al. [27], Heim et al. [29], Mabary-Olsen et al. [31], Tauriello et al. [35], and Maxwell et al. [32] measured increases in preferences towards fruits or vegetables, and Werner et al. [41] measured increases in label reading.
Discussion
Children and young adolescents must meet the recommendations for physical activity, sedentary behavior, and healthy eating throughout the year for optimal health. SDCs have the potential to replace the organization of school settings during summer breaks, but few interventions have been conducted in SDCs. In this review, we synthesized and summarized interventions that have integrated physical activity, sedentary behaviors, and healthy eating promotion in SDCs to identify some key lessons for future programs on healthy lifestyles targeting children and young adolescents. Our results showed that the number of studies targeting physical activity and healthy eating in SDCs was relatively low. We found that eight of the twenty-eight studies meeting eligibility criteria were limited to promoting physical activity, fourteen were limited to healthy eating promotion and five included both. Additionally, only one intervention targeted sedentary behaviors.
Physical activity, sedentary behaviors, and healthy eating are behaviors influenced by individual and environmental factors. The articles in this review are primarily focused on the behaviors themselves or their determinants. Fourteen studies included the promotion of physical activity in their intervention and most of them indicated positive changes in physical activity (i.e., MVPA, perceived behaviors, and number of steps) and/or their determinants (i.e., knowledge, perception of control, and attitude) [16,17,18,19, 24, 34, 38,39,40,41, 43]. Positive effects of physical activity promotion on sedentary behaviors (i.e., screen-time, television time, and sedentary time) were also observed in five studies [19, 24, 38, 39, 41]. For interventions that promoted healthy eating, most of them reported positive changes (i.e., FV, water, and SSB consumption) and/or their determinants (i.e., food-related knowledge, control perception, attitudes, and preferences) [17, 19,20,21,22,23,24, 26,27,28,29,30,31,32,33,34,35,36, 41]. Overall, only three of fourteen studies that measured physical activity [21, 25, 37] and one of twenty studies [42] that measured healthy eating did not observe changes in the target behavior or their determinants. Several methodological factors may explain these results, such as the specific content of the intervention, and the involvement of counsellors and/or parents.
Among all the factors that can explain success in intervention, the use of a theoretical frame to build the intervention represents an important aspect. Indeed, the use of a theory, often a theory of behavior change, is associated with a greater rate of success when it comes to promoting healthy lifestyle behaviors [44]. Most interventions targeting physical activity, except for four studies [16,17,18,19], were based on theories and all except three interventions targeting healthy eating [17, 19, 20] relied on a theoretical framework. The concepts of social cognitive theory and the ecological model of human development were the main elements used in the design of the interventions. Surprisingly, the results of the studies in this review do not differ according to the use of a theory.
Our results highlight a variety of different types of strategies that influenced physical activity, sedentary behaviors, and healthy eating. The most efficient strategies identified were goal setting or point systems, modifications of physical environments, physical activity education activities, promotion of physical activity with counsellors, cooking workshops or specific healthy eating education, and activities on overall healthy lifestyle behaviors including sedentary behaviors. The interventions could contain several strategies, but the majority had only one. Among those strategies, using goal setting seems promising. For instance, Wilson et al. [43] show that an intervention focusing primarily on goal setting to promote physical activity generally increases the number of steps taken and enjoyment of physical activity in SDCs. After a week, setting individual and camp-wide goals increased the number of steps. Conversely, group goal setting (vs. individual) did not affect step count but still had a positive influence on camper enjoyment. As for healthy eating, Baranowski et al. [21] and Heim et al. [29] used goal setting as a secondary component of the intervention. Even if both interventions had positive effects on the behavior, it is difficult to conclude if this specific strategy is responsible for the changes. Similarly, an intervention evaluated by Beets et al. [23] and Tilley et al. [36] used a point system to encourage healthy eating among campers. In both cases, the authors observed increases in FV consumption and a decrease in unhealthy behaviors in both campers and counsellors. Adding goal setting or point system, therefore, seems to be a very interesting component for interventions promoting physical activity and healthy eating in SDCs, mainly when it comes to individual and camp-wide goals.
Although physical environments are very important in the adoption of healthy behaviors [45], only three studies changed the physical environment in the camp to influence eating habits [29,30,31]. Accordingly, Lawman et al. [30] replaced old and unappealing water fountains (i.e., one or two per site) and distributed reusable water bottles to campers and some staff [30]. In addition, they ran a campaign to promote the acceptability of tap water, including a brief training for staff based on behavioral and social strategies which aimed to discourage SSB consumption and encourage water consumption [30]. Results indicate that at the end of the camp, campers consumed more water, there were more reusable bottles on the sites and the staff consumption of sugar-sweetened beverages over the last 30 days decreased. The other two studies changed physical environments by creating gardens and this had positive effects on young people. Indeed, Heim et al. [29] measured an increase in preference for vegetables, and Mabary-Olsen et al. [31] measured tendencies towards an increase in knowledge and self-efficacy towards vegetables. Thus, modification of the physical environments in the camps combined with a social campaign represents another interesting strategy to promote healthy behaviors.
The most common strategy used in physical activity interventions is education implemented using direct or indirect strategies. Some interventions included physical activity education directly to campers [16, 18, 37] and while others, rather included physical activity education through counsellors [25, 38,39,40]. Anderson-Butcher et al. [16], Kimiecik et al. [18], and Warner et al. [37] have all respectively evaluated positive changes following direct education on either self-efficacy, girls' healthy behaviors, or physical literacy. In the case of the intervention evaluated by Brazendale et al. [25] and Weaver et al. [40], based on the theory of expanded, extended, and enhanced opportunities which include indirect education through counsellors as the main strategy, the authors report an increase in the number of campers meeting the recommendations of 60 min of PA per day after the first year [40]. The results after four years also show that there is no difference between one year and two years of intervention. However, even though campers are ultimately no more likely to meet the recommendations of 60 min of PA per day at the end of the study, girls and boys were still 3.5 and 3.7 times more likely to meet the 60 min/d guidelines during intervention summers versus follow-up, respectively [25]. As for the intervention evaluated by Weaver, Beets, Saunders et al. [38] and Weaver, Beets, Turner-McGrievy et al. [39], it is rather based on the Let Us Play theory which also aimed to use an indirect education strategy. These studies have both measured increases in MVPA and a decrease in sedentary behavior in some campers. Interventions including education, therefore, have positive effects on physical activity of campers both when it is addressed directly to them or when it is implemented indirectly via the counsellors. Moreover, targeting counsellors makes it possible not only to target campers but also young adolescents.
The promotion of healthy eating is also essentially done through education with culinary workshops [20, 22, 26,27,28, 31, 33, 42]. Culinary workshops in SDCs improve the determinants of healthy eating, such as knowledge [20, 22, 26] preference [27], and the perception of control [22, 28, 33]. However, they have less effect on healthy eating whereas only one study observed an effect on campers' eating habits [31] and one study reported that campers replicated recipes learned in the workshops [28]. Other interventions have instead used repeated exposure to influence healthy eating among campers [32, 35]. Both studies improved campers' preferences/liking for vegetables, yet it is not known if this influenced their eating habits. Although it is difficult to conclude that cooking workshops in SDCs influence the eating habits of children and young adolescents, it has been shown that few cooking workshop opportunities are enough to improve the determinants of behavior change towards healthy eating [26].
While some interventions targeted a single behavior, some interventions targeted multiple behaviors (i.e., physical activity, sedentary behaviors, and healthy eating) altogether [17, 19, 21, 24, 34, 41]. Although the six interventions used education to improve campers' lifestyle behaviors, certain particularities such as the use of a web program in addition to the camp experience [21], six hours of totally structured activity [24], the use of the traditional food guide pyramid adapted to children's and adolescents to create discussions [19], and the inclusion of sedentary behaviors [41] distinguish them. The six studies all reported positive changes in behaviors or determinants, but they did not necessarily impact all the behaviors. For instance, the study of Baranowski et al. [21] influenced the eating habits of campers, but it did not modify the physical activity of the girls in the program. One of the reasons that may explain the lack of change is the low connection rate of participants to the web program. Similarly, Seal & Seal [34] also measured changes in participants' eating habits following the intervention, but there was no change in physical activity per se despite an increase in knowledge and self-perception. In sum, interventions that simultaneously target several lifestyle behaviors have reported positive effects on one or more behaviors and determinants of all the targeted behaviors.
The involvement of counsellors in the implementation of the interventions represents an interesting resource for promoting healthy lifestyle behaviors as they are in contact with campers daily. A total of eight interventions presented in eleven studies included counsellors in different ways to promote physical activity or healthy eating [18, 23, 25, 29, 30, 34, 36, 38,39,40, 43] but the implementation is not always well described. Three interventions presented in six studies put more emphasis on the role of counsellors; these interventions mainly consisted of personalized training and supporting counsellors and camps with booster sessions (i.e., visits or communications with the camp to ensure the proper implementation of the intervention) [23, 25, 36, 38,39,40]. The major difference between these interventions, in addition to the behavior promoted, is the content of the interventions and the number of booster sessions The intervention by Weaver, Beets, Turner-McGrievy et al. [39] and Weaver, Beets, Saunders et al. [38] contains additional elements for counsellors such as training to help use template schedules and six booster sessions. These sessions were in the camps where the program staff provided oral feedback based on weekly assessments. Beets et al. [23] and Tilley et al. [36] also include personalized training to counsellors and booster sessions (i.e., weekly communications and site visits) by the program staff to ensure that the program was properly implemented. Brazendale et al. [25] and Weaver et al. [40] include personalized training to counsellors based on the theory to expand, extend, and enhance PA opportunities and two on-site booster sessions for counsellors during the summer. Results from the review indicate that the two of these interventions had a positive effect on physical activity and eating habits. Overall, it seems that the intervention with individualized training to counsellors and more support for the camps in the implementation (i.e., booster sessions) have a better impact on the promotion of healthy lifestyle behaviors and ultimately on the behaviors of campers and counsellors.
Several interventions involved the parents of participating campers in physical activity [17, 19] and healthy eating promotion [19, 21, 23, 28, 30, 36]. All interventions that included parents did so by educating them to sustain behaviors promoted in camps at home, but two interventions were also asking parents to help campers in activities that had to be done at home [21, 28], and two interventions also used a point system at camp and campers’ rewards to further incentivize parents to modify camper lunch boxes [23, 36]. Concretely, it is difficult to say whether the inclusion of parents is effective since only one measured their commitment and it was rather weak. However, Anderson-Butcher et al. [16] aimed to assess the influence of parental support on physical activity determinants and found that parental support was a predictor of self-efficacy and intention toward healthy behaviors [16]. Additionally, the authors observed that parental support increased the beneficial effect of support from staff on self-efficacy and intention toward healthy behaviors. The inclusion of parents, therefore, seems interesting for campers’ behaviors, but also to increase the influence and support of counsellors on them.
Strengths and limitations
The main strength of this review is the extensive article search strategies with syntax that made it possible to include as many articles as possible on several platforms. Another strength is the inclusion of interventions targeting sedentary behaviors as most of the reviews on healthy lifestyle interventions in after-school programs included physical activity and healthy eating but not sedentary behaviors. As day camps represent an important setting that can contribute to reduce sedentary behaviors, the identification of strategies that may contribute reducing sedentary behaviors represents an important step forward in this context. The use of PRISMA-ScR, is also a strength of this sco** review. This review is, however, also subject to some limitations. In line with sco** review objectives (i.e., more descriptive review compared to systematic reviews), the quality of the articles was not evaluated. Even if the quality of the articles had not been assessed, the present scoo** review highlighted that most studies were cross-sectional and had a quasi-experimental design, mainly because they did not include a control group, which can both have effects on the capacity to infer causation. Also, gray literature was not included in this review. Moreover, the lack of details on training and the degree of intervention implementation compromises comparisons between programs and influences the conclusions of this review. Finally, the length of the evaluation was short, one summer for most interventions, and the studies that made several evaluations did not necessarily assess the same campers across the years.
Conclusion
This sco** review revealed that the targeted behaviors such as physical activity, sedentary behaviors, eating habits, and their determinants significantly improved in most intervention studies. Considering that physical activity, sedentary behaviors, and eating habits are not optimal in children and young adolescents during the summer and even in the SDCs, promoting healthy behaviors during this specific period is needed. This review highlights that strategies such as goal setting or a point system, modification of the physical environments (e.g., garden) combined with a social campaign, the inclusion of counsellors, comprehensive and individualized counsellor training, multiple booster sessions, and parents’ support are key elements for the success of an intervention promoting healthy lifestyle behaviors in SDCs. Future research should include more long-term intervention studies including a control group to better assess the causality between the promotion of healthy behaviors in SDCs and the effects on camper’s behavior. Finally, the most important recommendation of this review is to make interventions that will not only target physical activity and healthy eating but also sedentary behaviors to develop more global lifestyle interventions.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SDCs:
-
Summer day camps
- MVPA:
-
Moderate-to-vigorous physical activity
- SSB:
-
Sugar-sweetened beverages
- FV:
-
Fruit and vegetable
- PA:
-
Physical activity
- BCT:
-
Behavioral choice theory
- SCT:
-
Social cognitive theory
- STEPs:
-
Strategies to enhance practices
- TEO:
-
Theory of expanded, extended, and enhanced opportunities
References
Movassagh EZ, Baxter-Jones ADG, Kontulainen S, Whiting SJ, Vatanparast H. Tracking Dietary Patterns over 20 Years from Childhood through Adolescence into Young Adulthood: The Saskatchewan Pediatric Bone Mineral Accrual Study. Nutrients. 2017;9(9):900.
Strong WB, Malina RM, Blimkie CJ, Daniels SR, Dishman RK, Gutin B, et al. Evidence based physical activity for school-age youth. J Pediatr. 2005;146(6):732–7.
Craig WM, King M, Pickett W. The Health of Canadian Youth: Findings from the Health Behaviour in School-aged Children Study. 2020.
Carrel AL, Clark RR, Peterson S, Eickhoff J, Allen DB. School-Based Fitness Changes Are Lost During the Summer Vacation. Arch Pediatr Adolesc Med. 2007;161(6):561–4.
Baranowski T, O’Connor T, Johnston C, Hughes S, Moreno J, Chen TA, et al. School year versus summer differences in child weight gain: a narrative review. Child Obes. 2014;10(1):18–24.
Brazendale K, Beets MW, Weaver RG, Chandler JL, Randel AB, Turner-McGrievy GM, et al. Children’s Moderate to Vigorous Physical Activity Attending Summer Day Camps. Am J Prev Med. 2017;53(1):78–84.
Brazendale K, Beets MW, Weaver RG , Pate RR, Turner-McGrievy GM, Kaczynski AT, et al. Understanding differences between summer vs. school obesogenic behaviors of children: the structured days hypothesis. Int J Behav Nutr Phys Act. 2017;14(1):100.
Wang YC, Vine S, Hsiao A, Rundle A, Goldsmith J. Weight-related behaviors when children are in school versus on summer breaks: does income matter? J Sch Health. 2015;85(7):458–66.
Tremblay MS, Warburton DE, Janssen I, Paterson DH, Latimer AE, Rhodes RE, et al. New Canadian physical activity guidelines. Appl Physiol Nutr Metab. 2011;36(1):36–46; 7–58.
Canada H. Canada’s dietary guidelines for health professionals and policy makers. 2019.
Beets MW, Weaver RG, Beighle A, Webster C, Pate RR. How Physically Active Are Children Attending Summer Day Camps? J Phys Act Health. 2013;10(6):850–5.
Tilley F, Beets MW, Jones S, Turner-McGrievy G. Evaluation of compliance to national nutrition policies in summer day camps. Public Health Nutr. 2015;18(9):1620–5.
Kenney EL, Lee RM, Brooks CJ, Cradock AL, Gortmaker SL. What Do Children Eat in the Summer? A Direct Observation of Summer Day Camps That Serve Meals. J Acad Nutr Diet. 2017;117(7):1097–103.
Arksey H, O’Malley L. Sco** studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Sco** Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467–73.
Anderson-Butcher D, Amorose AJ, Bates S, Newman TJ, Okamoto K, Volek A. Exploring the Influence of Program Staff and Parental Support on Changes in Physical Health Outcomes of Vulnerable Youth Participating in a Sport-based Positive Youth Development Summer Camp. J Sport Behav. 2019;42(4):394–414.
Gachupin FC, Morehouse L, Bergier N, Thomson C. Describing a Public-health Summer Camp for Underserved Children: Healthy 2B Me. J Phys Educ Recreation Dance. 2019;90(4):39–51.
Kimiecik C, Bates S, Anderson-Butcher D. Examining the impact of a sport-based positive youth development program for adolescent girls of color: A Mixed methods study. Journal of Sport for Development. 2021;9(1):48–64.
Reverter-Masia J, Legaz-Arrese A, Jove-Deltell MC, Pi MCM, Salvo CV. EDUCATIONAL INTERVENTION ON NUTRITIONAL, HYGIENE AND HEALTH HABITS OF ELEMENTARY STUDENTS. Revista Internacional De Medicina Y Ciencias De La Actividad Fisica Y Del Deporte. 2012;12(48):611–23.
Jacob R, Motard-Belanger A, Provencher V, Fernandez MA, Gayraud H, Drapeau V. Influence of Cooking Workshops on Cooking Skills and Knowledge among Children Attending Summer Day Camps. Can J Diet Pract Res. 2020;81(2):86–90.
Baranowski T, Baranowski JC, Cullen KW, Thompson DI, Nicklas T, Zakeri IF, et al. The Fun, Food, and Fitness Project (FFFP): The Baylor GEMS pilot study. Ethn Dis. 2003;13(1 SUPPL. 1):S1-30.
Beets MW, Swanger K, Wilcox DR, Cardinal BJ. Using Hands-on Demonstrations to Promote Cooking Behaviors with Young Adolescents: The Culinary Camp Summer Cooking Program. J Nutr Educ Behav. 2007;39(5):288–9.
Beets MW, Tilley F, Weaver RG, Turner-McGrievy GM, Moore JB. Increasing fruit, vegetable and water consumption in summer day camps—3-year findings of the healthy lunchbox challenge. Health Educ Res. 2014;29(5):812–21.
Bohnert AM, Bates CR, Heard AM, Burdette KA, Ward AK, Silton RL, et al. Improving Urban Minority Girls’ Health Via Community Summer Programming. J Racial Ethn Health Disparities. 2017;4(6):1237–45.
Brazendale K, Beets MW, Weaver RG, Turner-McGrievy GM, Moore JB, Huberty JL, et al. Turn up the healthy eating and activity time (HEAT): Physical activity outcomes from a 4-year non-randomized controlled trial in summer day camps. Prev Med Rep. 2020;17:101053.
Condrasky MD, Johnson G, Corr A, Sharp JL. Cook Like a Chef 1- and 4-Week Camp Models. Journal of Extension. 2015;53(2), Article 26.
Ehrenberg S, Leone LA, Sharpe B, Reardon K, Anzman-Frasca S. Using repeated exposure through hands-on cooking to increase children’s preferences for fruits and vegetables. Appetite. 2019;142: 104347.
Harmon BE, Smith N, Pirkey P, Beets MW, Blake CE. The Impact of Culinary Skills Training on the Dietary Attitudes and Behaviors of Children and Parents. Am J Health Educ. 2015;46(5):283–92.
Heim S, Stang J, Ireland M. A garden pilot project enhances fruit and vegetable consumption among children. J Am Diet Assoc. 2009;109(7):1220–6.
Lawman HG, Lofton X, Grossman S, Root M, Perez M, Tasian G, et al. A randomized trial of a multi-level intervention to increase water access and appeal in community recreation centers. Contemp Clin Trials. 2019;79:14–20.
Mabary-Olsen EA, Litchfield RE, Foster R, Lanningham-Foster L, Campbell C. Can an Immersion in Wellness Camp Influence Youth Health Behaviors? J Ext. 2015;53(2):2.
Maxwell AE, Castillo L, Arce AA, De Anda T, Martins D, McCarthy WJ. Eating Veggies Is Fun! An Implementation Pilot Study in Partnership With a YMCA in South Los Angeles. Prev Chronic Dis. 2018;15:E132.
Murad M, Alford A-M, Davis K. Farm to Future: A Virtual Summer Nutrition Culinary Camp for Kids. J Nutr Educ Behav. 2021;53(5):445–8.
Seal N, Seal J. Develo** healthy childhood behaviour: outcomes of a summer camp experience. Int J Nurs Pract. 2011;17(4):428–34.
Tauriello S, Bowker J, Wilding G, Epstein L, Anzman-Frasca S. Examining associative conditioning with a positive peer context as a strategy to increase children’s vegetable acceptance. Pediatr Obes. 2020;15(10): e12660.
Tilley F, Weaver RG, Beets MW, Turner-McGrievy G. Healthy Eating in Summer Day Camps: The Healthy Lunchbox Challenge. J Nutr Educ Behav. 2014;46(2):134–41.
Warner M, Robinson J, Heal B, Lloyd J, Mandigo J, Lennox B, et al. Increasing Physical Literacy in Youth: A Two-Week Sport for Development Program for Children Aged 6–10. Prospects: Quarterly Review of Comparative Education. 2021;50:165–82.
Weaver RG, Beets MW, Saunders RP, Beighle A. A coordinated comprehensive professional development training’s effect on summer day camp staff healthy eating and physical activity promoting behaviors. J Phys Act Health. 2014;11(6):1170–8.
Weaver RG, Beets MW, Turner-McGrievy G, Webster CA, Moore J. Effects of a competency-based professional development training on children’s physical activity and staff physical activity promotion in summer day camps. New Dir Youth Dev. 2014;143:57–78.
Weaver RG, Brazendale K, Chandler JL, Turner-McGrievy GM, Moore JB, Huberty JL, et al. First year physical activity findings from turn up the HEAT (Healthy Eating and Activity Time) in summer day camps. PLoS One. 2017;12(3):e0173791.
Werner D, Teufel J, Holtgrave PL, Brown SL. Active Generations: An Intergenerational Approach to Preventing Childhood Obesity. J Sch Health. 2012;82(8):380–6.
Williams L, Magee A, Kilby C, Maxey K, Skelton JA. A pilot summer day camp cooking curriculum to influence family meals. Pilot Feasibility Stud. 2019;5:147.
Wilson C, Sibthorp J, Brusseau TA. Increasing Physical Activity and Enjoyment Through Goal-Setting at Summer Camp. J Park Recreat Adm. 2017;35(4):24–36.
Barley E, Lawson V. Using health psychology to help patients: theories of behaviour change. Br J Nurs. 2016;25(16):924–7.
Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health. 2010;31:399–418.
Acknowledgements
The authors particularly thank Marie Denise Lavoie, librarian at Université Laval, for her expert advice and help with research strategies.
Funding
David Larose is the recipient of a doctoral scholarship from the Centre NUTRISS.
Author information
Authors and Affiliations
Contributions
The study was designed by DL and VD and supervised by JY and VD. Articles were read and sorted by DL, MCSC, and SP. Data interpretation and the first draft of the manuscript were done by DL. All authors have read, critically revised the manuscript, and approved the final version (DL: 50%, MCSC: 25%, SP: 5%, JY: 5%, AT: 5%, VD: 10%).
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Larose, D., Chih-Shing Chen, M., Panahi, S. et al. Interventions to promote healthy lifestyle behaviors in children and adolescents in summer day camps: a sco** review. BMC Public Health 23, 773 (2023). https://doi.org/10.1186/s12889-023-15521-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15521-1