
Abstract
Background
Non-suicidal self-injury (NSSI) has exhibited an increasing trend in recent years and is now globally recognized as a major public health problem among adolescents and young adults. Negative life events (NLEs) are positively associated with NSSI. We sought to explore (1) whether sex plays a role in the risk of NLEs leading to NSSI and (2) the role played by mental health (MH).
Methods
We adopted a multi-stage cluster sampling method to select college students across four grades from May to June 2022. Generalized linear models were used to evaluate the relationships between NLEs, sex, MH and NSSI, presented as incidence-rate ratios (RRs) with 95% confidence intervals (CIs). We examined the complex relationship between these variables using the PROCESS method for moderation analysis.
Results
Following the exclusion of data that did not meet the study requirements, data from 3,578 students (mean age: 20.53 [± 1.65] years) were included. Poisson regression results indicate that high-level NLEs (RR = 0.110, 95%CI: 0.047–0.173) are associated with increased NSSI. Furthermore, interaction effects were observed among sex, NLEs and NSSI. MH and sex moderated the relationship between NLEs and NSSI.
Conclusion
Identifying risk factors for NSSI is also important when exploring the interaction between NLEs and MH given the potential for NSSI to significantly increase the risk of later psychopathological symptoms and substance abuse problems. In addition, the significance of sex differences in risk factors for NSSI should be determined. This study evaluated how the impact of NLEs on NSSI can be reduced among adolescents from multiple perspectives.
Similar content being viewed by others


Background
In recent years, economic losses caused by mental illness have been gradually increasing. Compared with symptoms such as depression and anxiety, non-suicidal self-injury (NSSI) has not received sufficient attention. NSSI refers to inflicting physical harm upon oneself without suicidal intention, and is considered a socially unacceptable behavior [1]. NSSI includes various behavioral patterns, such as cutting, burns, beating, scratching, and hair pulling. While distinct from suicidal behavior, it is also a strong predictor of suicide. NSSI continues to cause indelible harm and remains a significant mental health (MH) concern among adolescents worldwide. The Diagnostic and Statistical Manual of Mental Disorders also identifies NSSI as a separate behavioral category and lists it as an “item for further study.” A meta-study revealed that the reporting rate of NSSI (including individual NSSI) among adolescents was 17.2% [2]. Lim et al. estimate the reporting rate to be approximately 19.5% (95% CI = 13.3–27.6% from global literature data) [3]. Another adverse effect of NSSI is that it maintains a “trajectory” into adulthood and increases psycho-behavioral problems during this period [4, 5]. One study estimated the lifetime prevalence rate of NSSI to be 4.86% [6]. In general, the current epidemic of NSSI worldwide is a serious concern [7]. NSSI has evolved into a major public health problem that has endangered the physical and MH of Chinese adolescents. Moreover, NSSI is also linked to suicide, an ongoing social health problem that can lead to further fatal behavior.
If the continued development of NSSI is to be promptly controlled, key questions such as the factors influencing NSSI, its duration, and measures to safeguard those affected by it should be addressed. The factors influencing NSSI in children and adolescents are complex and it is associated with many risk factors. Adolescent’s NSSI is a social phenomenon influenced by various factors that can promote, maintain, or inhibit its occurrence. Therefore, what causes the occurrence of NSSI is worthy of in-depth investigation. As a comprehensive variable encapsulating multiple social factors, negative life events (NLEs) can promote physiological and psychological changes by precipitating shifts in chronic stress states [9]. While the independent effects of sex and NLEs on depression have been reported [26], further correlations require clarification. MH remains an important factor that cannot be disregarded, with research indicating certain biological and behavioral markers meeting the criteria for potential endophenotypes of suicidal behaviors, including early-onset depression [27].
The aforementioned studies affirm the moderating role of NSSI in the relationship between NLEs and MH; however, the potential for sex differences to moderate the relationship between NLEs and NSSI is not yet clarified. The psychological mechanism underlying these associations remains unclear. Moreover, the relationship between NLE exposure and sex differences in the short-term outcomes of NSSI during adolescence has received limited research attention. A more comprehensive understanding of these complex relationships may help in better controlling the occurrence of NSSI. Therefore, this line of research within the specific context of college students needs to be reinforced. The present study investigates the prevalence rate of NSSI among college students and observes the influence of some potential factors on NSSI caused by NLEs. Additionally, it provides empirical evidence for research into the roles of sex, MH, and their impact on NSSI. By integrating the findings of previous research, this study proposes a systematic and comprehensive adolescent MH screening and prevention program, which can serve as a strong basis for establishing relevant guidelines on adolescent MH prevention techniques or expert consensus. Therefore, this study (1) examines the correlations between MH, sex, NLEs and NSSI and (2) investigates the moderating effects of sex and MH in the relationship between NLEs and NSSI among Chinese college students.
Methods
Study design
This cross-sectional study was conducted among a population of college students, following the methodology described in previous studies [28, 29]. The surveyed schools adopted cluster sampling, and students of all grades and majors were included. A total of 3,600 college students aged 15–26 years were recruited through an electronic questionnaire survey. Participants were then asked to complete an anonymous questionnaire, which was submitted through mobile phones upon completion. Furthermore, a supervisor was present at the survey site to ensure quality control. The survey was conducted between May and June 2022, and 22 participants were excluded after the survey because they were unwilling to answer the questionnaire or were absent from class. In other cases, missing data (missing values greater than 5%) or obvious errors led to exclusions [30,31,32]. The design and data collection procedures were approved by the Ethics Committee of Anhui Medical University, and all methods were performed in accordance with the relevant guidelines.
Exposure
Negative life events
In this study, NLEs were assessed using the Adolescent Life Events Scale (ASLEC) developed and revised by Liu et al. The ASLEC consists of 27 items [33], each rated on a scale from 1 to 5 (1 = no impact, 2 = mild, 3 = moderate, 4 = severe, 5 = very severe). Higher total scores mean a greater impact of NLEs risk.
Mental health
The Depression Anxiety Stress Scales – 21 (DASS-21) was used to evaluate students’ psychological problems. This is a valid and reliable tool that accurately measures depression, anxiety, stress, and other symptoms. The DASS-21 comprises three subscales, each with seven items. Each item has four response options to reflect the severity of psychological problems (0 = No match, 3 = always). Both clinical and non-clinical samples have been used to assess the reliability of the DASS-21 subscale, with favorable results [34].
Outcome: NSSI
“Have you intentionally hurt yourself in the past 12 months, but not for suicide?” The questionnaire lists several methods of self-injury: hitting with a fist or palm, pulling hair, hitting a hard object with head or fist, pinching or scratching, biting, cutting, and stabbing. Participants who reported engaging in NSSI were further asked about the frequency and the number of NSSI was taken as the total number, with “five kinds” or more defined as NSSI [35].
Statistics analysis
Mean, standard deviation, and one-way analysis of variance (ANOVA) were used to describe the distribution of continuous variables, and frequency and percentage of Chi-square tests were adopted to characterize categorical variables. We adopted a generalized linear model to assess the relationship between NLEs, sex, MH and NSSI, expressed in terms of incidence ratio (RRs) and 95% confidence interval (CIs). Moderation analysis was conducted by PROCESS method to explore the relationship between NLEs, sex, MH, and NSSI [30, 36]. The bootstrap method was used to re-sample 1,000 samples, and 95% CI was calculated. All data were analyzed using SPSS (Windows Version 23.0). Following preliminary data sorting, missing data were processed via multiple imputation using SPSS 23.0.
Results
General demographic characteristics
After data validation and removal of entries that did not meet the study criteria, the final dataset comprised 3,578 students. The general distribution of the variables concerning depression, anxiety, and NSSI is presented in Tables 1, 2 and 3. Among the participants, 1,745 (48.8%) were women; with an average age of 20.53 (± 1.65) years. Regarding residential areas, 1,130 (31.6%) lived in urban areas, 783 (21.9%) in towns, and 1,665 (46.5%) in rural areas. The prevalence rates of NSSI was 8.5%. NSSI was correlated with having fewer than two friends, while depression and anxiety symptoms were correlated with both a worse family economic status and having fewer than two friends. Additional results are detailed in Table 1.
Association between independent variables and adolescents’ psychological and behavioral problems
Among adolescent participants at risk for NSSI, 0.152 times as many had depressive symptoms as did not (95%CI: 0.075 ~ 0.229; P < 0.001), 0.135 times more with anxiety symptoms than those without (95%CI: 0.064 ~ 0.206; P < 0.001), those with stress were 0.220 times higher than those without (95%CI: 0.098 ~ 0.343; P < 0.001), and 0.110 times more with anxiety symptoms than those without (95%CI: 0.047 ~ 0.173; P < 0.001). These results are reported in Table 2.
Moderation analyses of the relationship between NLEs and MH, sex, and adolescent NSSI
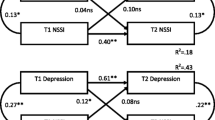
Moderation analyses were performed with NLEs, MH, sex, and NSSI and the results are presented in Tables 3, 4 and 5. The findings reveal a positive association between exposure to NLEs and anxiety, alongside a significant association between sex and anxiety. Moreover, the interaction between NLEs and sex significantly predicted the severity of anxiety. However, concerning NSSIs, the interaction between NLEs and sex did not significantly predict the severity of NSSI. Furthermore, the anxiety × sex interaction was correlated with NSSI. After controlling for educational level, consistent patterns were observed across marital status, total annual household income, ethnicity, and age.
Discussion
Main findings
The prevalence rates of NSSI in our sample of college students was 8.5%. In our generalized linear model, NLEs were positively correlated with the development of NSSI, which suggests that higher exposure to NLEs is related to increased NSSI. Second, we combined NLEs, sex, and MH and established an interaction effect between NLEs, sex, and NSSI. Consistent with our hypothesis, our findings suggest that MH moderates the relationship between NLEs and NSSI; this relationship is also moderated by sex. The relationship between NLEs, MH problems, and NSSI is complex and may involve the moderating role of sex differences. Our findings also provide a new perspective for preventing NSSI among college students [37]. Therefore, we developed and evaluated a moderation model to clarify the role of multilevel factors, including NLEs, MH, and sex, on NSSI [16]. A more comprehensive understanding of NSSI and its associated factors may be helpful in develo** programs and interventions to reduce the occurrence of NSSI.
Comparison with other studies
NSSI is a common MH problem in adolescents [38]. Attention to NSSI is crucial, as it not only has a high incidence but also serves as a major predisposing factor for suicide and even death. The harm of NSSI is that not only can it affect the lives of teenagers, but that it can also further lead to suicidal behavior. A review of 1,094 articles found that NSSI rates have increased globally from 11.5% to as high as 33.8% [39]. Other studies have documented that NLEs have a significant triggering effect on the day and month of a suicide attempt [12]. Importantly, NSSI is associated with, is a specific risk factor for, and can somewhat increase the risk of suicidal behavior. In addition to imposing a personal burden, self-harm, including NSSI and self-harm with suicidal intent, entails significant costs owing to increased morbidity and mortality. This emphasizes the need to investigate the causes and management of NSSI [17]. Despite the high incidence rate, studies on NSSI seem to be insufficient, thereby suggesting the need to pay more attention to the contributing factors. Several factors have been identified, including NLEs, SLEs, negative co** style, problematic Internet use, sleep disturbance, traumatic experiences, problematic parent–child relationships, and MH problems [10, 40,41,42]. Observing the interactions between variables in more detail requires us to understand the linkages between them.
Variations in NSSI were observed based on sex [10, 35]. A meta-analysis of 18 case-control and seven cohort studies with a total sample size of more than 55,596 individuals reported that NSSI in adolescents was associated with sex differences and mental disorders [35]. Akin to early exposure to environmental endocrine disruptors, NLEs are considered one of the major psychosocial environmental risks that pose a serious and imminent threat to public health and are identified with the increased risk of adult MH difficulties in the future [43]. Exposure to childhood trauma or multiple accumulations of SLEs may lead to an adaptive overload of the biological stress response, thereby dysregulating its development and/or homeostasis [44]. Since the seminal research on cumulative risk, various social and cognitive domains have also presented support for this concept [45]. Using concepts such as the diathesis-stress model and cumulative risk, research has reported that childhood abuse and neglect can significantly increase the risk of psychopathological symptoms in young people [46]. Previous research has recognized these two factors, and the current work also provides answers that complement previous research. Such studies shed light on how NLEs interact with sex factors with regard to NSSI in MH.
We explored the association between MH, sex, NLEs, and NSSI and derived the following observations. First, patients with major depressive disorder and NSSI had experienced ACEs [35, 37, 47]. The present study clarifies the relationship between NLEs and NSSI and provides insights into how therapeutic interventions targeting NLEs can prevent the occurrence of NSSI [37]. Second, previous studies have established that NLEs and MH are associated with higher NSSI [14, 17], and we observed an association between the two in our study. Our analysis is based on the hypothesis of psychopathological development resulting from the interplay between NLEs and behavioral and MH issues [16]. These findings offer a theoretical foundation for a comprehensive investigation of its role in understanding the relationships between NLEs, MH, and NSSI. Third, the interaction between higher-risk NLEs and higher depression was correlated with NSSI [14]. This finding indicates that exposure to low-risk social environments among adolescents with depression can exacerbate MH problems, including common mood and anxiety disorders, self-harm, and suicidal ideation [14]. These results are similar to those of socio-ecological psychology research, which is a process study and can indicate that specific features of the environment lead to a psychological state that can stimulate the target’s behavior through some mechanism (in the current study, psychological problems). These results are also similar to those of previous studies [48, 49]. Finally, we explore the reasons for the association in terms of its underlying mechanisms. Research has highlighted the importance of considering the possible role of chronic inflammatory states by investigating them as mediating mechanisms in the relationship between NLE and NSSI [50]. In terms of biological mechanisms, the hypothalamic–pituitary–adrenal (HPA) axis and circulating inflammatory cytokines may be involved in part of the process [51]. By constructing a gene–environment interaction model, Ben-Efraim et al. explored the effect of interaction between HPA axis regulatory genes (i.e., candidate genes associated with suicide and its endophenotype) and SLEs on suicidal behavior [44]. Furthermore, NSSI self-efficacy may buffer the effect of NLEs and recent NLEs on NSSI [52]; this finding verifies the associations between NLEs, MH, and sex, and NSSI [49]. NLEs are a more complex etiological marker among the factors that cause NSSI, and its effects appear to vary by type, time, and severity, and are also influenced by gender-related factors [53].
Additionally, we explored the moderating effects of MH and sex [49] and identified an association between MH and NSSI [43, 54]. The potential mechanism at play may involve the cumulative and interacting physiological responses to psychosocial stress (including altered neuroendocrine hormone levels, toxic stress, and allostatic load). These processes can lead to nervous system impairments, such as depression and thoughts of suicide/self-harm [55]. In a conceptual model, negative emotions are proposed as an important factor that causes HRBs [56]. We investigated the relationship between sex, MH, and NSSI from a social environment perspective (specifically considering the influence of NLEs) and established that high NLE is associated with high MH and NSSI. Similarly, NSSI and MH issues increased, depending on sex, among adolescents who experienced a poor social environment. The key mechanisms by which stressors such as NLEs lead to behavioral changes such as NSSI include epigenetic changes [57,58,59]. A series of animal experiments revealed that early adverse life experiences are more important for the change of apparent inheritance pattern; the same is true of population studies. Moreover, ACEs induce changes in MicroRNAs (miRNAs) function through complex interactions of genes associated with the HPA axis and other neuroendocrine signaling systems, further leading to the development of NSSI [60]. Kang et al. explored the association between BDNF methylation, depression, and suicide; they found that a higher BDNF-promoting methylation status was significantly associated with a history of prior suicide attempts, suicidal ideation during treatment, suicidal ideation at final evaluation, higher suicidal ideation scores, and adverse outcomes of suicidal ideation treatment [61].
The aforementioned findings provide empirical evidence for the relationship between NSSI and MH; further, some theoretical models can support our results [17], such as the empirical avoidance model [54], the emotional cascade model [62], and Nock’s integration model [63]. The latter proposes that NSSI combines two motivations (personal, interpersonal, or social) and may in turn be associated with positive or negative reinforcement events [43]. According to Bandura’s social cognitive theory, the potential social factor influence of MH and resulting NSSI may be impacted by resilience [64]; in other words, the relationship between NSSI and sex provides a new perspective into specific NSSI-related cognitions. Our results corroborate and extend those of previous research. Moreover, to explore the mediating role of MH in NSSI and further verify the moderating role of sex, we adopted multiple social environments to portray adolescents’ social interactions, together with their mediating conditions. We also provide perspectives to investigate the association of NSSI with MH and sex, rather than only NLEs (including failure at school, failure to achieve something important, drug use, and bullying), which have been associated with suicidal ideation [65]. The premise of putting forward this complex relationship is that mediating and regulating effects are crucial in psychological research for exploring psychological behavior problems, and the potential mechanisms can be further discovered. This study starts with NLEs, and after observing its association with NSSI, introduces MH, a mediating variable, and sex, a regulating variable. Different positions and roles of these variables in the model will produce different outcomes. A mediating regulating model is a common model that includes both the regulating and the mediating variable. This indicates that the effect of NLEs on NSSI is influenced by sex, and that sex acts (at least in part) through MH.
Strengths and limitations
The advantages of this study lie in its multilevel design and a large number of adolescent participants. It also explored the associations between complex variables—including moderating effects—that were designed to examine variables influencing the strength and direction of the prediction–outcome relationship and covariates. The use of recommendation in this study could help identify the interdependence between NLEs and NSSI.
However, the following potential limitations should be noted. The cross-sectional design of this study was unable to observe causal inferences of the association between NLEs and NSSI. Future longitudinal studies are needed to assess potential correlations between variables. In addition, the data were obtained using self-recall reports, which can lead to some degree of recall bias. In addition, a key conceptual question in the current literature on NLEs is how researchers conceptualize and measure NLEs; we did not address these aspects (e.g., heterogeneity of NLEs) in our study. In addition, this study only investigated social and psychological factors and did not explore the influence of other biological factors such as inflammation and methylation. Future research should conduct a critical methodological examination of the underlying mechanisms. Finally, as only some variables were included, future research should consider more psychosocial variables [18].
Conclusion
We found that exposure to NLEs among college students is universal and occurs during a potentially sensitive developmental period. Poisson regression also revealed that NLE, psychological problems, and NSSI are closely related, which has important implications regarding the etiology of NSSI and MH. An interactive positive association was also observed between cumulative NLEs and sex. Finally, moderation analysis should also focus on the MH of adolescents and explore the differences between genders.
Data availability
The datasets generated for this study are available on request to the corresponding author.
Data availability
The data used and analyzed during the study are available from the corresponding author on reasonable request.
Abbreviations
- ASLEC:
-
Adolescent Life Events Scale
- ACE:
-
Adverse childhood experiences
- CI:
-
Confidence intervals
- DASS-21:
-
Depression Anxiety Stress Scales – 21
- HRB:
-
Health risk behaviors
- HPA:
-
Hypothalamic–pituitary–adrenal
- MicroRNAs:
-
miRNAs
- MH:
-
Mental health
- NLE:
-
Negative life events
- NSSI:
-
Non-suicidal self-injury
- RR:
-
Rate ratios
- SLE:
-
Stressful life events
References
Nock MK. Self-injury. Annu Rev Clin Psychol. 2010;6:339–63.
Liu RT, Walsh RFL, Sheehan AE, et al. Prevalence and correlates of suicide and nonsuicidal self-injury in children: a systematic review and meta-analysis. JAMA Psychiatry. 2022;79(7):718–26.
Lim KS, Wong CH, McIntyre RS, et al. Global lifetime and 12-month prevalence of suicidal behavior, deliberate self-harm and non-suicidal self-injury in children and adolescents between 1989 and 2018: a meta-analysis. Int J Environ Res Public Health. 2019;16(22):4581.
Tilton-Weaver L, Latina D, Marshall SK. Trajectories of nonsuicidal self-injury during adolescence. J Adolesc. 2022. https://doi.org/10.1002/jad.12126.
Adrian M, Zeman J, Erdley C, et al. Trajectories of non-suicidal self-injury in adolescent girls following inpatient hospitalization. Clin Child Psychol Psychiatry. 2019;24(4):831–46.
Liu RT. The epidemiology of non-suicidal self-injury: lifetime prevalence, sociodemographic and clinical correlates, and treatment use in a nationally representative sample of adults in England. Psychol Med. 2023;53(1):274–82. https://doi.org/10.1017/S003329172100146X.
Ribeiro JD, Franklin JC, Fox KR, et al. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: a meta-analysis of longitudinal studies. Psychol Med. 2016;46(2):225–36.
**a H, Han X, et al. Effects of negative life events on depression in middle school students: the chain-mediating roles of rumination and perceived social support. Front Psychol. 2022;13:781274. https://doi.org/10.3389/fpsyg.2022.781274.
Jiang Z, Wang Z, Diao Q, et al. The relationship between negative life events and non-suicidal self-injury (NSSI) among Chinese junior high school students: the mediating role of emotions. Ann Gen Psychiatry. 2022;21(1):45. https://doi.org/10.1186/s12991-022-00423-0. Published 2022 Nov 19.
Wang YJ, Li X, Ng CH, Xu DW, Hu S, Yuan TF. Risk factors for non-suicidal self-injury (NSSI) in adolescents: a meta-analysis. EClinicalMedicine. 2022;46:101350. https://doi.org/10.1016/j.eclinm.2022.101350.
Ernst M, Brähler E, Kampling H, et al. Is the end in the beginning? Child maltreatment increases the risk of non-suicidal self-injury and suicide attempts through impaired personality functioning. Child Abuse Negl. 2022;133:105870.
Liu BP, Zhang J, Chu J, Qiu HM, Jia CX, Hennessy DA. Negative life events as triggers on suicide attempt in rural China: a case-crossover study. Psychiatry Res. 2019;276:100–6. https://doi.org/10.1016/j.psychres.2019.04.008.
Shao C, Wang X, Ma Q, et al. Analysis of risk factors of non-suicidal self-harm behavior in adolescents with depression. Ann Palliat Med. 2021;10(9):9607–13.
Wei C, Li Z, Ma T, Jiang X, Yu C, Xu Q. Stressful life events and non-suicidal self-injury among Chinese adolescents: a moderated mediation model of depression and resilience. Front Public Health. 2022;10:944726. https://doi.org/10.3389/fpubh.2022.944726. Published 2022 Aug 4.
Gu H, Lu Y, Cheng Y. Negative life events and nonsuicidal self-injury in prisoners: the mediating role of hopelessness and moderating role of belief in a just world. J Clin Psychol. 2021;77(1):145–55. https://doi.org/10.1002/jclp.23015.
Zhang Y, Suo X, Zhang Y, Zhang S, Yang M, Qian L, Shang L, Zhang D, Xu F, Li W. The relationship between negative life events and Nonsuicidal Self-Injury among Chinese adolescents: a moderated-mediation model. Neuropsychiatr Dis Treat. 2022;18:2881–90. PMID: 36540672; PMCID: PMC9760044.
Hepp J, Carpenter RW, Störkel LM, Schmitz SE, Schmahl C, Niedtfeld I. A systematic review of daily life studies on non-suicidal self-injury based on the four-function model. Clin Psychol Rev. 2020;82:101888. https://doi.org/10.1016/j.cpr.2020.101888. Epub 2020 Jul 6. PMID: 32949907; PMCID: PMC7680364.
Panagou C, MacBeth A. Deconstructing pathways to resilience: a systematic review of associations between psychosocial mechanisms and transdiagnostic adult mental health outcomes in the context of adverse childhood experiences. Clin Psychol Psychother. 2022;29(5):1626–54. https://doi.org/10.1002/cpp.2732.
McGue M, Bouchard TJ. Adjustment of twin data for the effects of age and sex. Behav Genet. 1984;14(4):325–43. https://doi.org/10.1007/bf01080045.
Lee RD, Chen J. Adverse childhood experiences, mental health, and excessive alcohol use: examination of race/ethnicity and sex differences. Child Abuse Negl. 2017;69:40–8. https://doi.org/10.1016/j.chiabu.2017.04.004.
Kessler RC. The effects of stressful life events on depression. Annu Rev Psychol. 1997;48:191–214. https://doi.org/10.1146/annurev.psych.48.1.191.
Plener PL, Kaess M, Schmahl C, Pollak S, Fegert JM, Brown RC. Nonsuicidal Self-Injury in adolescents. Dtsch Arztebl Int. 2018;115(3):23–30. https://doi.org/10.3238/arztebl.2018.0023.
Stikkelbroek Y, Bodden DH, Kleinjan M, Reijnders M, van Baar AL. Adolescent Depression and Negative Life Events, the Mediating Role of Cognitive Emotion Regulation [published correction appears in PLoS One. 2018;13(1):e0192300]. PLoS One. 2016;11(8):e0161062. Published 2016 Aug 29. https://doi.org/10.1371/journal.pone.0161062.
Peng L, Zhang J, Li M, et al. Negative life events and mental health of Chinese medical students: the effect of resilience, personality and social support. Psychiatry Res. 2012;196(1):138–41. https://doi.org/10.1016/j.psychres.2011.12.006.
Sokratous S, Merkouris A, Middleton N, Karanikola M. The association between stressful life events and depressive symptoms among Cypriot university students: a cross-sectional descriptive correlational study. BMC Public Health. 2013;13:1121. https://doi.org/10.1186/1471-2458-13-1121.
Sun XJ, Niu GF, You ZQ, Zhou ZK, Tang Y. sex, negative life events and co** on different stages of depression severity: A cross-sectional study among Chinese university students [published correction appears in J Affect Disord. 2017;215:102]. J Affect Disord. 2017;209:177–181. https://doi.org/10.1016/j.jad.2016.11.025.
Mann JJ, Arango VA, Avenevoli S, et al. Candidate endophenotypes for genetic studies of suicidal behavior. Biol Psychiatry. 2009;65(7):556–63. https://doi.org/10.1016/j.biopsych.2008.11.021.
Li S, Wang R, Thomas E, et al. Patterns of adverse childhood experiences and depressive symptom trajectories in young adults: a longitudinal study of college students in China. Front Psychiatry. 2022;13:918092. https://doi.org/10.3389/fpsyt.2022.918092.
Song X, Wang S, Wang R, et al. Mediating effects of specific types of co** styles on the relationship between Childhood Maltreatment and depressive symptoms among Chinese undergraduates: the role of sex. Int J Environ Res Public Health. 2020;17(9):3120. https://doi.org/10.3390/ijerph17093120.
Jiang Z, Xu H, Wang S, et al. Parent-child relationship quality, childhood maltreatment, and psychological symptoms in Chinese adolescent. J Interpers Violence. 2022;37(19–20):NP18130–51. https://doi.org/10.1177/08862605211035869.
Li S, Wang S, Gao X, et al. Patterns of adverse childhood experiences and suicidal behaviors in adolescents: a four-province study in China. J Affect Disord. 2021;285:69–76. https://doi.org/10.1016/j.jad.2021.02.045.
Wang S, Xu H, Li S, Jiang Z, Wan Y. Sex differences in the determinants of suicide attempt among adolescents in China. Asian J Psychiatr. 2020;49:101961. https://doi.org/10.1016/j.ajp.2020.101961.
Liu X, Liu LQ, et al. Reliability and validity of the adolescents self-rating life events checklist. Chin J Clin Psychol. 1997;5(1):34–6.
Crawford JR, Henry JD. The Depression anxiety stress scales (DASS): normative data and latent structure in a large non-clinical sample. Br J Clin Psychol. 2003;42(Pt 2):111–31. https://doi.org/10.1348/014466503321903544.
Wan Y, Chen R, Ma S, et al. Associations of adverse childhood experiences and social support with self-injurious behaviour and suicidality in adolescents. Br J Psychiatry. 2019;214(3):146–52. https://doi.org/10.1192/bjp.2018.263.
Jiang T, Zhang Y, Dai F, Liu C, Hu H, Zhang Q. Advanced glycation end products and diabetes and other metabolic indicators. Diabetol Metab Syndr. 2022;14(1):104. https://doi.org/10.1186/s13098-022-00873-2.
Chen Z, Li J, Liu J, Liu X. Adverse childhood experiences, recent negative life events, and non-suicidal self-injury among Chinese college students: the protective role of self-efficacy. Child Adolesc Psychiatry Ment Health. 2022;16(1):97. https://doi.org/10.1186/s13034-022-00535-1. Published 2022 Dec 3.
Brown RC, Plener PL. Non-suicidal Self-Injury in Adolescence. Curr Psychiatry Rep. 2017;19(3):20. https://doi.org/10.1007/s11920-017-0767-9.
Mannekote Thippaiah S, Shankarapura Nanjappa M, Gude JG, et al. Non-suicidal self-injury in develo** countries: a review. Int J Soc Psychiatry. 2021;67(5):472–82. https://doi.org/10.1177/0020764020943627.
Yang F, Jiang L, Miao J, et al. The association between non-suicidal self-injury and negative life events in children and adolescents in underdeveloped regions of south-western China. PeerJ. 2022;10:e12665. https://doi.org/10.7717/peerj.12665. Published 2022 Mar 9.
Baetens I, Greene D, Van Hove L, et al. Predictors and consequences of non-suicidal self-injury in relation to life, peer, and school factors. J Adolesc. 2021;90:100–8. https://doi.org/10.1016/j.adolescence.2021.06.005.
Fan YY, Liu J, Zeng YY, Conrad R, Tang YL. Factors Associated with Non-suicidal Self-Injury in Chinese adolescents: a Meta-analysis. Front Psychiatry. 2021;12:747031. https://doi.org/10.3389/fpsyt.2021.747031. PMID: 34916971; PMCID: PMC8669619.
Vega D, Sintes A, Fernández M, et al. Review and update on non-suicidal self-injury: who, how and why? Actas Esp Psiquiatr. 2018;46(4):146–55.
Ben-Efraim YJ, Wasserman D, Wasserman J, Sokolowski M. Gene-environment interactions between CRHR1 variants and physical assault in suicide attempts. Genes Brain Behav. 2011;10(6):663–72. https://doi.org/10.1111/j.1601-183X.2011.00703.x.
Mackenzie MJ, Kotch JB, Lee LC, et al. A cumulative ecological–transactional risk model of child maltreatment and behavioral outcomes: reconceptualizing early maltreatment report as risk factor. Child Youth Serv Rev. 2011;33(11):2392–8. https://doi.org/10.1016/j.childyouth.2011.08.030.
Karatekin C. Adverse childhood experiences (ACEs), Stress and Mental Health in College Students. Stress Health. 2018;34(1):36–45. https://doi.org/10.1002/smi.2761.
Qian H, Shu C, Feng L, **ang J, Guo Y, Wang G, Childhood Maltreatment SL, Events. Cognitive emotion regulation strategies, and non-suicidal Self-Injury in adolescents and Young adults with First-Episode Depressive Disorder: direct and indirect pathways. Front Psychiatry. 2022;13:838693. https://doi.org/10.3389/fpsyt.2022.838693. Published 2022 Apr 12.
Taylor BJ, Hasler BP. Chronotype and Mental Health: Recent Advances. Curr Psychiatry Rep. 2018;20(8):59. Published 2018 Jul 23. https://doi.org/10.1007/s11920-018-0925-8.
Zhang Y, Li Y, Jiang T, Zhang Q. Role of body mass index in the relationship between adverse childhood experiences, resilience, and mental health: a multivariate analysis. BMC Psychiatry. 2023;23(1):460. https://doi.org/10.1186/s12888-023-04869-8. Published 2023 Jun 23.
Su YA, Lin JY, Liu Q, et al. Associations among serum markers of inflammation, life stress and suicide risk in patients with major depressive disorder. J Psychiatr Res. 2020;129:53–60. https://doi.org/10.1016/j.jpsychires.2020.06.008.
Kuhlman KR, Geiss EG, Vargas I, Lopez-Duran NL. Differential associations between childhood trauma subtypes and adolescent HPA-axis functioning. Psychoneuroendocrinology. 2015;54:103–14.
Chen Y, Huang CC, Yang M, Wang J. Relationship between adverse childhood experiences and resilience in college students in China [published online ahead of print, 2022 Mar 29]. J Fam Violence. 2022;1–10. https://doi.org/10.1007/s10896-022-00388-4.
Herzog JI, Schmahl C. Adverse childhood experiences and the consequences on Neurobiological, Psychosocial, and somatic conditions across the Lifespan. Front Psychiatry. 2018;9:420. https://doi.org/10.3389/fpsyt.2018.00420.
Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: the experiential avoidance model. Behav Res Ther. 2006;44:371–94.
McNair FD, Havens J, Surko M, et al. Post-traumatic stress and related symptoms among juvenile detention residents: results from intake screening. Child Abuse Negl. 2019;92:22–31. https://doi.org/10.1016/j.chiabu.2019.03.011.
Duffy KA, McLaughlin KA, Green PA. Early life adversity and health-risk behaviors: proposed psychological and neural mechanisms. Ann N Y Acad Sci. 2018;1428(1):151–69. https://doi.org/10.1111/nyas.13928.
Park C, Rosenblat JD, Brietzke E, et al. Stress, epigenetics and depression: a systematic review. Neurosci Biobehav Rev. 2019;102:139–52. https://doi.org/10.1016/j.neubiorev.2019.04.010.
Lutz PE, Turecki G. DNA methylation and childhood maltreatment: from animal models to human studies. Neuroscience. 2014;264:142–56. https://doi.org/10.1016/j.neuroscience.2013.07.069.
Jaworska-Andryszewska P, Rybakowski JK. Childhood trauma in mood disorders: neurobiological mechanisms and implications for treatment. Pharmacol Rep. 2019;71(1):112–20. https://doi.org/10.1016/j.pharep.2018.10.004.
Allen L, Dwivedi Y. MicroRNA mediators of early life stress vulnerability to depression and suicidal behavior. Mol Psychiatry. 2020;25(2):308–20. https://doi.org/10.1038/s41380-019-0597-8.
Kang HJ, Kim JM, Lee JY, et al. BDNF promoter methylation and suicidal behavior in depressive patients. J Affect Disord. 2013;151(2):679–85. https://doi.org/10.1016/j.jad.2013.08.001.
Klonsky ED. The functions of deliberate self-injury: a review of the evidence. Clin Psychol Rev. 2007;27:226–39.
Selby EA, Joiner TE. Cascades of emotion: the emergence of Borderline personality disorder from emotional and behavioral dysregulation. Rev Gen Psychol. 2009;13:219.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. https://doi.org/10.1037/0033-295X.84.2.191.
Lannoy S, Mars B, Heron J, Edwards AC. Suicidal ideation during adolescence: the roles of aggregate genetic liability for suicide attempts and negative life events in the past year. J Child Psychol Psychiatry. 2022;63(10):1164–73. https://doi.org/10.1111/jcpp.13653.
Acknowledgements
We would like to acknowledge all hospital action teams, the staff and participants from the participating hospitals, and our cooperators, for their assistance in data collection.
Funding
This research was funded by Anhui Institute of Translational Medicine (2023 hyx-C33), China Postdoctoral Science Foundation (2023M740022), National Natural Science Foundation of China (82073578), Anhui University Humanities and Social Science Research Key Project (2022AH050614), Anhui Medical University Research Fund Project Youth Science Fund (2022xkj307), the National Natural Science Foundation of China Youth Science 2018 Fund Training Program, The First Affiliated Hospital of Anhui Medical University (2018kj20), Hunan Sanuo Diabetes Charity Foundation “Sweet Doctor Cultivation” project (2021SD08), and National Natural Science Foundation of China (82370836).
Author information
Authors and Affiliations
Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Anhui Medical University. All focus group participants provided signed informed consent forms prior to the start of the focus groups. Written informed consent was obtained from the parents or guardians of all the students.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, Y., Gong, L., Feng, Q. et al. Association between negative life events through mental health and non-suicidal self-injury with young adults: evidence for sex moderate correlation. BMC Psychiatry 24, 466 (2024). https://doi.org/10.1186/s12888-024-05880-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-024-05880-3