
Abstract
Introduction
Much confusion exists between health-related QoL (HRQoL) scales and subjective QoL (SQoL) scales. One method to avoid confusion is use of a single question that asks What is your quality of life? or similar. This study explored the relationship between biopsychosocial factors and high SQoL, SQoL stability, and factors associated with improving SQoL.
Method
We conducted a large cohort study of community-dwelling Chinese adults with schizophrenia, with two data points (2015–2016 (N = 742), 2017–2018 (N = 491)). Demographic and clinically related items and a comprehensive suite of published measures were collected. Direct logistic regressions were used to explore links between biopsychosocial factors and high SQoL and Improvement in SQoL across time.
Results
Sample at Baseline: Male = 62.3%; Med age = 38.5 years; Med Age at illness onset = 24 years; SQoL Mode = neither poor nor good. Three independent variables predicted high SQoL at T1. Contemporary age and the presence of clinically relevant symptoms had a negative relationship with high SQoL; insight had a positive relationship with high SQoL. SQoL changed significantly across time with a modest effect size. Age at illness onset was the single independent variable linked to improving SQoL favoring being older at the time of illness onset.
Discussion/Conclusions
SQoL can be high and changeable. While symptomology and illness insight may affect SQoL self-appraisals at single points in time, only age of illness onset was connected with improving SQoL. Thus, public health measures to delay illness onset are important. In addition, care about the distinction between HRQoL and SQoL in study design and choice of measures is necessary and will depend on the purpose and context.
Similar content being viewed by others


Introduction
Given the range and severity of symptomology experienced by individuals diagnosed with schizophrenia, symptoms and service use are prominent treatment and research interests [e.g., 1, 2,3,4]. Symptom mitigation and/or resolution is important but not at the expense of an individual’s life expectancy and quality of life both of which can be impacted by various medical treatments [5].
Health-related quality of life (HRQoL), a specialised-type of quality of life (QoL) measure, is increasingly accepted as an important outcome in health studies [6]. HRQoL measures are designed to examine the relative impact that health (or a health condition) has on an individual’s life qualities [7] and often used to monitor outcomes in clinical practice, clinical trials and population studies, especially for diseases with relapsing and remitting courses such as rheumatoid arthritis [8] and schizophrenia [9,10,11]. Encouraged by the WHO’s Constitutional principle of health being more than the absence of disease or infirmity [12] interest in more general QoL has also grown in health-related research including into persisting schizophrenia [e.g., 13, 14, 15].
While definitions of QoL abound, it is generally accepted that QoL consists of objective and subjective dimensions [16,17,18,19]. Typically, objective QoL is measured with indicators that you can count such as the size of one’s pay cheque or the size of one’s house. In contrast subjective QoL (SQoL) is a self-reported personal reflection and generally thought to come from an amalgamation of cognition and affect [20, 21]. Objective and subjective indicators are ordinarily poorly correlated [16, 19]. For instance, the average SQoL of waste pickers in South Africa was found to be higher than the national average [22] and the SQoL in individuals living with persisting serious disability such as tetraplegia can report living good or excellent lives [23] – as maintained by the disability paradox [24] whereby objective QoL is often low in individuals living with disability but low SQoL is much less likely.
Multiple factors have been linked to QoL in individuals living with schizophrenia and several meta-analyses have been completed. Davis and colleagues [25] found overall clinical insight to be negatively related to QoL i.e. higher QoL ratings linked with poorer insight. This relationship, however, was moderated by increased symptom severity. General psychopathology (e.g. depression and anxiety) was negatively linked with QoL and schizophrenia-specific symptoms (positive and/or negative symptoms) to be weakly linked at best [26]. A negative correlation between duration of untreated psychosis and QoL, and severity of symptoms and QoL exists in people experiencing first-episode psychosis [27]. Nevarez-Flores and colleagues [28] found global functioning to have a consistent positive association with QoL in people with psychotic disorders.
Each of the research teams who conducted the above meta-analyses, discussed QoL in generic terms. However, inspection of the included studies revealed that substantial proportions of studies used HRQoL measures. This is not unexpected since substantial heterogeneity abounds in the medical and psychological communities concerning QoL definitions, measurement tools and ways of reporting [29]. HRQoL studies are important. Arguably however, a person’s own appraisal of their life that we call SQoL (sometimes referred to as subjective wellbeing and/or satisfaction with life) can be as, if not more, important than an appraisal by a healthcare professional of the potentially negative impact of a health condition. The advantage of raising the profile of SQoL is that it encourages a more holistic appraisal of the individual’s life experiences and circumstances, putting the person ahead of the health condition. The issue is that HRQoL measures cannot examine beyond an absence of symptoms/lack of impact made by the health condition. Fundamentally HRQoL uses a deficit approach to measurement that is linked with, and contingent upon, the health condition [30] and consequently, cannot identify potential factors uniquely linked with good or high SQoL.
SQoL of individuals with schizophrenia has been the focus of other studies using a variety of measures. For example, a search of the Medline database using the parameters of: “subjective quality of life” and “schizophrenia” search terms, English language, and published between 2012 and November 2022, and after excluding citations that made only a brief reference to QoL [31,32,33,34], or reported a study protocol [35], yielded 71 citations. Of these, over a third of the studies used measures that were clearly HRQoL instruments such as the Schizophrenia Quality of Life Scale [36, 37], the Subjective Well-being under Neuroleptic Treatment Scale [e.g., 38, 39], and the health measures of MOS-36 [e.g., 40, 41] and the SF-12 [e.g., 42]. It seems there may be confusion between self-report as a data-gathering method and SQoL as a within person experience that is broader than the impact of a health condition.
One method to measure SQoL that cannot be confused with HRQoL is the use of a single question that asks: “What is your quality of life?”, “How would you rate your quality of life”, or similar. Single items to evaluate SQoL have been used to good effect in general population groups [e.g., 43, 44, 45] as well as with samples of adults living with schizophrenia [e.g., 46, 47,48,49]. In kee** with the disability paradox, in each of the samples the mean score sat just above the response scale midpoint suggesting that many individuals living with schizophrenia appraise their lives positively. However, there is a further unconsidered matter. In each instance, their analytical method assumed that their independent variables had a linear relationship with the SQoL dependent variable, implying that each factor is connected with both high and low SQoL in roughly equal measure. A more salutogenic approach is to ask, “What factors might be uniquely linked with high SQoL, despite exposure to the symptoms and consequences of living with schizophrenia”.
A recent large Chinese cohort study provided the opportunity to explore the relationship that biopsychosocial variables already linked with HRQoL including insight, psychopathology, duration of illness and symptomology, may have on high SQoL. The stability of SQoL could also be assessed. Four questions were posed.
-
1.
What is the SQoL in Chinese adults living with schizophrenia?
-
2.
Are there biopsychosocial variables connected with high SQoL?
-
3.
How stable is high SQoL over time?
-
4.
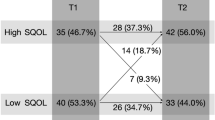
Is there a systematic difference between participants who reported their SQoL to be low at Time 1 (T1) and high at Time 2 (T2) compared to participants whose SQoL remained low?
Method
Study participants
Participants were adults (a) aged 18-years or older, (b) received a diagnosis of schizophrenia as per ICD-10 guidelines (c) fluent in Chinese - either Cantonese or Mandarin, (d) capable of understanding and completing the interview, and (e) registered for primary mental health services within one of the randomly chosen townships as per below. Both capacity and diagnosis were confirmed by one of the research psychiatrists during the clinical interview and by reviewing participants’ medical records. The exclusion criteria were history of significant head injury, seizures, cerebrovascular diseases, or other comorbid neurological disease.
A cohort study design with two time points was used to explore SQoL in adults with schizophrenia living in the county-level city of Luoding which is an underdeveloped and rural area in the south-west Guangdong province, southern China. This study used a random cluster sampling method to choose 21 of the 63 townships with primary mental health care services. All local patients with schizophrenia who were registered within these townships and managed within the Chinese National Psychiatric Management System (CNPMS) were approached. CNPMS was established to provide community follow-up management of people living with severe mental illness including schizophrenia; virtually all adults diagnosed with schizophrenia would be registered with CNPMS.
After eligibility was determined, written informed consent was obtained. Structured interviews with the adults and their caregivers, were undertaken by one of three research psychiatrists each of whom had 3-years or more of clinical and research experience. Data were collected within two 15-month periods (between time difference M = 24.7 months (SD = 3.80 months)): T1 Baseline in 2015 to 2016 (N = 742) and T2 Follow-up in 2017 to 2018 (N = 491), being a 66.2% response rate at follow-up. Those lost to follow-up did not differ significantly on any measure used in this study. The structured interviews encompassed socio-demographic and clinically related items and several validated measures which follow.
Survey tool
SQoL was measured using the single broad question that prefaces the WHOQOL-BREF [50] whereby participants are asked “How would you rate your quality of life?” using a 5-point Likert scale anchored with very poor (score = 1) to very good (score = 5) response choices. As highlighted previously, using single items to measure SQoL has been demonstrated to be a convenient, valid, and reliable approach, both in the general population [51] and populations with a disability [52]. To meet the objectives of this study, SQoL was also dichotomised into High SQoL (scores 4 or 5) and Low SQoL (scores 1 to 3).
The Brief Psychiatric Rating Scale (BPRS) [53, 54] is a clinician administered scale consisting of 18 items that assess positive, negative, and affective symptoms in individuals who have a psychotic disorder. Item scores range from not present = 1 to extremely severe = 7, and 0 is entered if the item is not assessed. Scores are summed providing a summary total score from 18 to 126 with higher scores indicating the presence of more severe symptoms. The BPRS is a widely used scale purposely developed to evaluate schizophrenia-related symptoms over time [54]. The BPRS has been translated into Chinese [70,71,72]. Moreover, this study extends those findings to a non-western country, namely China.
Time had a significant relationship with SQoL. Multivariate analyses revealed older age of illness onset was significantly associated with improving SQoL. Immonen et al. [73] conducted a meta-analysis into the effect of age of illness onset and found earlier age of onset to negatively impact individuals in a range of long-term outcomes including more relapses, more hospitalisations, poorer social/occupational functioning and poorer global outcomes. It seems reasonable that being more mature before the onset of schizophrenia could advantage individuals. The extra time could provide more opportunity for individuals to accrue more material assets, grow supportive adult relationships, and develop a stronger sense of self before having to endure the onslaught of their first psychotic episode. Research has demonstrated that each of those factors– material resources, supportive relationships, stronger/more positive sense of self– reduce the impact of negative experiences such as onset of schizophrenia [e.g., 74, 75,76,77].
There is some evidence that while time is a linear construct, its impact may not be. Rotstein et al. [78] found the age of illness onset in males to have a curvilinear (smile-shaped) relationship with self-appraised SQoL connected with poorer SQoL outcomes (bottom of smile) for those aged around their mid- thirties at illness onset. The researchers acknowledge however, that their results seemed to run counter to previous literature. Contemporary age was negatively associated with SQoL at Time 1 in our study but not significantly associated with improved SQoL suggesting that extra time before illness onset might establish an advantage that is not easily overcome with extra time post-diagnosis. Further evidence exists demonstrating that the trajectory of illness presentation, treatment and functioning varies according to whether adolescent-or adult-onset, favouring adult-onset [79].
Clearly, time is still a conundrum needing to be explored more fully. Nevertheless, our overall findings underscore the need to defer illness onset as much as possible by public health measures. These might include campaigns to encourage young people to delay their first use of cannabis [80], as well as family psychoeducation and/or school-based programs [81, 82] in childhood and adolescence with the potential to decrease the overall risk of early onset, by preventing bullying [83].
Exploring the stability of SQoL, we found that nearly half of the cohort who participated at both timepoints and reported their SQoL to be low at baseline, reported an improvement in their SQoL over 24-months, shifting to the high category. This was statistically significant with a small effect. Several possible reasons for this change spring to mind. Perhaps care in the medical clinics improved for many of the participants, or the economy improved for many families thus affording larger economic reserves to help with participants’ care, or that being asked about one’s quality of life reminded participants to take better care of themselves, or participants whose SQoL improved were more likely to remain in the study. Lange et al. [15] also examined the trajectory of SQoL in older Dutch people with schizophrenia, finding nearly 56% of their participants had a clinically relevant change in SQoL across five years - some improved and some deteriorated. This suggests that living with chronic schizophrenia requires great effort by patients, families, and carers in the maintenance of SQoL; an effort that transcends cultural differences.
The presence of clinically relevant psychiatric symptoms was negatively associated with high T1 SQoL. These results are in kee** with previous research such as Eack and Newhills’ meta-analysis that examined the connection between psychiatric symptoms and QoL [26]. Their result was not unexpected given the high prevalence of HRQoL measurements included in their study samples. But our findings, using an unambiguous SQoL measure, also makes sense. It would be more challenging for most people to maintain high SQoL when concurrently experiencing significant symptoms. They are also in kee** with the pooled analysis by Priebe and colleagues [84] who found reduction in psychiatric symptoms was associated with improvements in SQoL. Severity of negative symptoms (diminished expression, amotivation) is also negatively associated with subjective well-being [70]. Once more, this study extends those findings to a non-western country.
Illness insight and medication compliance, measured by ITAQ, were significantly associated with high T1 SQoL in the cross-sectional multivariate analysis, with increased insight at least doubling the odds of reporting high SQoL. This seems reasonable if we surmise that a level of insight is needed to accept and comply with treatment for symptom remission, thus providing better opportunity for individuals to live their lives. But it does run counter to much of the literature discourse that features the insight paradox whereby increased insight is associated with decreased QoL thought to be moderated by feelings of hopelessness as featured in the meta-analysis by Davis et al. [25]. Yet, this too makes sense as most of the QoL measures used in their included studies administered HRQoL measures. Individuals who lack insight into their illness and consequent need for treatment/medication would be unlikely to acknowledge the negative impact of schizophrenia symptomology, when responding to items that measure the impact of illness on various qualities of life as per HRQoL scales.
Other independent variables including medication, and functional impairment, were not connected with high SQoL in our study, contrary to the evidence in the aforementioned meta-analyses and, arguably perhaps, expectations. Examination of each meta-analysis sample revealed substantial numbers of studies that used a HRQoL measure. HRQoL measures are designed to examine the relative impact that a given health condition has on various aspects (qualities) of an individual’s life so can be useful in treatment or service evaluations and research. But that is qualitatively different to assessing how an individual might appraise their own life as a whole and thereby might explain this discrepancy.
HRQoL measures are constructed within a deficit-based framework whereby the absence of impact by the given health condition symptom(s) is considered to be the equivalent of high QoL [30, 85]. For example, the Schizophrenia Quality of Life Scale [86] is a 30-item self-report measure that consists of three subscales: Psychosocial (15 items), Motivation and Energy (7 items), and Symptoms and side-effects (8 items. Symptoms in body or mind, are a sign of illness. Experiencing any health condition including schizophrenia means the presence of symptoms that will, inevitably, have a downward impact on a HRQoL scale. Unsurprisingly therefore, clinical, and function-related measures will more often demonstrate a significant relationship with a HRQoL scale whether clinician or patient completed.
A strength of this study was study design being a large cohort study thus increasing confidence in the generalisability of the results. The study was based in China which may limit generalisability to western settings. However, several of our results were in kee** with studies based in western countries suggesting the findings reflect features of common humanity rather than any given culture. This study used a single item SQoL scale to good effect. This had the advantage of removing any ambiguity in study topic. Single items also have advantages of reduced burden and costs – important considerations in any research. Nevertheless, a higher-order complex concept such as SQoL is better represented by a comprehensive multi-faceted scale and a wider scoring range.
Conclusion
Of course, symptoms can and do change our own appraisals of SQoL but the impact in HRQoL is almost inevitable and, in SQoL, not so much, as found in the current study. In principle, even individuals living with significant disability such as tetraplegia [23] or living in extreme poverty [22], can report living a good life. HRQoL appraisals are important for health/treatment/service evaluation. But when examining an individual with any health condition it is important to remember they are just that – an individual with a health condition, and if one is interested in appraising overall QoL in general then using a general population SQoL measure is both appropriate and advisable. Consequently, care about the distinction between HRQoL and SQoL in study design and choice of measures is necessary and will depend on the purpose and context.
This study demonstrated that SQoL can change for individuals with schizophrenia. The implication for mental health services is that any individual living with schizophrenia and whose SQoL is currently good can change for the worse, and also importantly, vice versa. While symptomology and illness insight may affect SQoL self-appraisals in any given point in time, only (older) age of illness onset was connected with improving SQoL. Thus, it is important for public health departments to use activities such as campaigns to encourage young people (i.e. adolescents and young adults) to delay their first use of cannabis, and family psychoeducation and/or school-based programs in childhood and adolescence with the potential to decrease the overall risk of early onset e.g., anti-bullying programs, to delay the onset of schizophrenia.
Data availability
The original contributions presented in the study are included in the article, further inquiries can be directed to the Dr. Cailan Hou.
References
Mintz AR, Dobson KS, Romney DM. Insight in schizophrenia: a meta-analysis. Schizophr Res. 2003;61(1):75–88.
Wright IC, Rabe-Hesketh S, Woodruff PWR, David AS, Murray RM, Bullmore ET. Meta-analysis of Regional Brain volumes in Schizophrenia. Am J Psychiatry. 2000;157(1):16–25.
Aleman A, Hijman R, de Haan EHF, Kahn RS. Memory impairment in Schizophrenia: a Meta-analysis. Am J Psychiatry. 1999;156(9):1358–66.
Grube BS, Bilder RM, Goldman RS. Meta-analysis of symptom factors in schizophrenia. Schizophr Res. 1998;31(2):113–20.
Kaplan RM. The significance of quality of life in health care. Qual Life Res. 2003;12(1):3–16.
Bullinger M. Assessing health related quality of life in medicine. An overview over concepts, methods and applications in international research. Restor Neurol Neurosci. 2002;20(3–4):93–101.
Hayes RD, Reeve BB. Measurement and modeling of health-related quality of life. In: Epidemiology and demography in public health edn. Edited by Killewo J, Heggenbhougen HK, Quah SR: Elsevier Inc; 2008: 195–205.
Khanna D, Tsevat J. Health-related quality of LifeAn introduction. Supplements and Featured Publications 2007, 13(9 Suppl).
Chan SW-c, Hsiung P-C, Thompson DR, Chen S-C, Hwu H-G. Health-related quality of life of Chinese people with schizophrenia in Hong Kong and Taipei: a cross-sectional analysis. Res Nurs Health. 2007;30(3):261–9.
Chou C-Y, Ma M-C, Yang T-T. Determinants of subjective health-related quality of life (HRQoL) for patients with schizophrenia. Schizophr Res. 2014;154(1):83–8.
Hofer A, Mizuno Y, Wartelsteiner F, Wolfgang Fleischhacker W, Frajo-Apor B, Kemmler G, Mimura M, Pardeller S, Sondermann C, Suzuki T, et al. Quality of life in schizophrenia and bipolar disorder: the impact of symptomatic remission and resilience. Eur Psychiatry. 2017;46:42–7.
Constitution. [https://www.who.int/about/governance/constitution].
Bechdolf A, Klosterkötter J, Hambrecht M, Knost B, Kuntermann C, Schiller S, Pukrop R. Determinants of subjective quality of life in post acute patients with schizophrenia. Eur Arch Psychiatry Clin NeuroSci. 2003;253(5):228–35.
Wu C-H, Wu C-Y. Life satisfaction in persons with schizophrenia living in the community. Soc Indic Res. 2008;85(3):447.
Lange SMM, Meesters PD, Stek ML, Penninx BW, Rhebergen D. The 5-year outcome of subjective quality of life in older schizophrenia patients. Qual life Research: Int J Qual life Aspects Treat care Rehabilitation. 2022;31(8):2471–9.
Cummins RA. Objective and subjective quality of life: an interactive model. Soc Indic Res. 2000;52(1):55–72.
Parmenter TR. Quality of Life as a Concept and Measurable Entity. In: Improving the Quality of Life: Recommendations for People with and without Disabilities edn. Edited by Romney DM, Brown RI, Fry PS. Dordrecht: Springer Netherlands; 1994: 9–46.
Felce D, Perry J. Quality of life: its definition and measurement. Res Dev Disabil. 1995;16(1):51–74.
Fakhoury WKH, Priebe S. Subjective quality of life: it’s association with other constructs. Int Rev Psychiatry. 2002;14(3):219–24.
Cummins RA. Fostering quality of life. InPsych. 2013;35(1):1–11.
Health-Related quality of life (HRQOL).: well-being concepts [https://www.cdc.gov/hrqol/wellbeing.htm].
Blaauw P, Pretorius A, Viljoen K, Schenck R. Adaptive expectations and subjective well-being of Landfill Waste pickers in South Africa’s Free State Province. Urban Forum. 2020;31(1):135–55.
Migliorini C, Tonge B. Reflecting on subjective well-being and spinal cord injury. J Rehabil Med. 2009;41(6):445–50.
Albrecht GL, Devlieger PJ. The disability paradox: high quality of life against all odds. Soc Sci Med. 1999;48(8):977–88.
Davis BJ, Lysaker PH, Salyers MP, Minor KS. The insight paradox in schizophrenia: a meta-analysis of the relationship between clinical insight and quality of life. Schizophr Res. 2020;223:9–17.
Eack SM, Newhill CE. Psychiatric symptoms and quality of life in Schizophrenia: a Meta-analysis. Schizophr Bull. 2007;33(5):1225–37.
Watson P, Zhang J-P, Rizvi A, Tamaiev J, Birnbaum ML, Kane J. A meta-analysis of factors associated with quality of life in first episode psychosis. Schizophr Res. 2018;202:26–36.
Nevarez-Flores A, Sanderson K, Breslin M, Carr V, Morgan V, Neil A. Systematic review of global functioning and quality of life in people with psychotic disorders. Epidemiol Psychiatric Sci. 2019;28(1):31.
Costa DSJ, Mercieca-Bebber R, Rutherford C, Tait M-A, King MT. How is quality of life defined and assessed in published research? Qual Life Res. 2021;30(8):2109–21.
Cummins RA. Fluency disorders and life quality: subjective wellbeing vs. health-related quality of life. J Fluen Disord. 2010;35(3):161–72.
McEnery C, Lim MH, Tremain H, Knowles A, Alvarez-Jimenez M. Prevalence rate of social anxiety disorder in individuals with a psychotic disorder: a systematic review and meta-analysis. Schizophr Res. 2019;208:25–33.
Stoll J, Hodel MA, Riese F, Irwin SA, Hoff P, Biller-Andorno N, Trachsel M. Compulsory interventions in severe and persistent Mental illness: a Survey on attitudes among psychiatrists in Switzerland. Front Psychiatry. 2021;12:537379.
Burton CZ, Vella L, Kelsoe JR, Bilder RM, Twamley EW. Catechol-O-methyltransferase genotype and response to compensatory cognitive training in outpatients with schizophrenia. Psychiatr Genet. 2015;25(3):131–4.
de Jong S, Renard SB, van Donkersgoed RJ, van der Gaag M, Wunderink L, Pijnenborg GH, Lysaker PH. The influence of adjunctive treatment and metacognitive deficits in schizophrenia on the experience of work. Schizophr Res. 2014;157(1–3):107–11.
Mueller-Stierlin AS, Meixner F, Kohlmann A, Schumacher M, Hänsel A, Pouwels M, Bias N, Hartl S, Reichstein J, Prestin E, et al. Effectiveness and cost-effectiveness of a community-based mental health care programme (GBV) for people with severe mental illness in Germany: study protocol for a randomised controlled trial. Trials. 2020;21(1):598.
Kim J-H, Lee S, Han A-Y, Kim K, Lee J. Relationship between cognitive insight and subjective quality of life in outpatients with schizophrenia. Neuropsychiatr Dis Treat. 2015;11:2041–8.
Wang L, Fan XW, Zhao XD, Zhu BG, Qin HY. Correlation analysis of the quality of Family Functioning and Subjective Quality of Life in Rehabilitation patients living with Schizophrenia in the community. Int J Environ Res Public Health 2020, 17(7).
Ninomiya Y, Miyamoto S, Ten** T, Ogino S, Miyake N, Kaneda Y, Sumiyoshi T, Yamaguchi N. Long-term efficacy and safety of blonanserin in patients with first-episode schizophrenia: a 1-year open-label trial. Psychiatry Clin Neurosci. 2014;68(12):841–9.
Schroeder K, Huber CG, Jelinek L, Moritz S. Subjective well-being, but not subjective mental functioning shows positive associations with neuropsychological performance in schizophrenia-spectrum disorders. Compr Psychiatry. 2013;54(7):824–30.
Brink M, Andersen K. Subjective health-related quality of life in community-dwelling middle-aged and older adults with early-onset schizophrenia. Nord J Psychiatry. 2020;74(8):585–93.
Tan XW, Seow E, Abdin E, Verma S, Sim K, Chong SA, Subramaniam M. Subjective quality of life among patients with schizophrenia spectrum disorder and patients with major depressive disorder. BMC Psychiatry. 2019;19(1):267.
Chang WC, Cheung R, Hui CL, Lin J, Chan SK, Lee EH, Chen EY. Rate and risk factors of depressive symptoms in Chinese patients presenting with first-episode non-affective psychosis in Hong Kong. Schizophr Res. 2015;168(1–2):99–105.
Altrosko P, Bagińska P, Mokosińka M, Sawicki A, Atroszko B. Validity and reliability of single-item self-report measures of general quality of life, general health and sleep quality. In: CER Comparative European Research Edited by McGreevy M, Rita R. London: Sciemcee; 2015.
Cunny KA, Perri M. Single-item vs multiple-item measures of Health-Related Quality of Life. Psychol Rep. 1991;69(1):127–30.
de Boer AGEM, van Lanschot JJB, Stalmeier PFM, van Sandick JW, Hulscher JBF, de Haes JCJM, Sprangers MAG. Is a single-item Visual Analogue Scale as Valid, Reliable and Responsive as Multi-item scales in Measuring Quality of Life? Qual Life Res. 2004;13(2):311–20.
Bushong ME, Nakonezny PA, Byerly MJ. Subjective quality of life and sexual dysfunction in outpatients with schizophrenia or schizoaffective disorder. J Sex Marital Ther. 2013;39(4):336–46.
Fervaha G, Agid O, Takeuchi H, Foussias G, Remington G. Effect of antipsychotic medication on overall life satisfaction among individuals with chronic schizophrenia: findings from the NIMH CATIE study. Eur Neuropsychopharmacology: J Eur Coll Neuropsychopharmacol. 2014;24(7):1078–85.
Gardsjord ES, Romm KL, Friis S, Barder HE, Evensen J, Haahr U, ten Velden Hegelstad W, Joa I, Johannessen JO, Langeveld J, et al. Subjective quality of life in first-episode psychosis. A ten year follow-up study. Schizophr Res. 2016;172(1):23–8.
Voruganti L, Heslegrave R, Awad AG, Seeman MV. Quality of life measurement in schizophrenia: reconciling the quest for subjectivity with the question of reliability. Psychol Med. 1998;28(1):165–72.
World Health Organization. Programme on Mental Health: WHOQOL user Manual. In.: WHO Division of Mental Health and Prevention of Substance Abuse; 2012.
Atroszko P, Bagińska P, Mokosińka M, Atroszko B. Validity and reliabiity of single-item self-report measures of general quality of life, general health and sleep quality. In: 4th Biannual CER Comparative European Research Conference Edited by McGreevy M, Rita R. London UK: Sciemcee Publishing; 2015: 207–2011.
Siebens HC, Tsukerman D, Adkins RH, Kahan J, Kemp B. Correlates of a single-item quality-of-life measure in People Aging with disabilities. Am J Phys Med Rehabil. 2015;94(12):1065–74.
Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. 1962;10(3):799–812.
Shafer A. Meta-analysis of the brief Psychiatric Rating Scale factor structure. Psychol Assess. 2005;17(3):324–35.
Zhang M, Zhou T, Liang J, Wang Z, Tang Y, Chi Y, **a M. The application of translated brief psychiatric rating scale (BPRS) (2) validity test. Chin J Nerv Mental Dis. 1984;10:74–7.
Zhang M, Zhou T, Tang Y, Chi Y, **a M, Wang Z. The application of translated brief Psychiatric Rating Scale (BPRS) (1) reliability test. Chin J Nerv Mental Dis. 1983;9:76–80.
Phillips MR, **ong W, Wang RW, Gao YH, Wang XQ, Zhang NP. Reliability and validity of the Chinese versions of the scales for Assessment of positive and negative symptoms. Acta Psychiatrica Scandinavica. 1991;84(4):364–70.
Li J, Guo Y-B, Huang Y-G, Liu J-W, Chen W, Zhang X-Y, Evans-Lacko S, Thornicroft G. Stigma and discrimination experienced by people with schizophrenia living in the community in Guangzhou, China. Psychiatry Res. 2017;255:225–31.
Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. Clinical implications of brief Psychiatric Rating Scale scores. Br J Psychiatry. 2005;187(4):366–71.
Mortimer AM. Symptom rating scales and outcome in schizophrenia. Br J Psychiatry. 2007;191(S50):7–s14.
McEvoy J, Aland JRJ, Wilson WH, Guy W, Hawkins L. Measuring chronic schizophrenic patients’ attitudes toward their illness and treatment. Psychiatric Serv. 1981;32(12):856–8.
Gao H, Yu X, Lv F. Reliability and validity of insight and treatment attitude questionnaire (ITAQ) (in Chinese). Chin Mental Health J. 1998;2:3–5.
Montgomery SA, Åsberg M. A New Depression Scale designed to be sensitive to change. Br J Psychiatry. 1979;134(4):382–9.
Zhong B, Wang Y, Chen H, Wang X. Reliability, validity and sensitivity of Montgomery-Asberg depression rating scale for patients with current major depression disorder. Chin J Behav Med Brain Sci. 2011;20(1):85–7.
Hawley CJ, Gale TM, Sivakumaran T. Defining remission by cut off score on the MADRS: selecting the optimal value. J Affect Disord. 2002;72(2):177–84.
Hou C-L, Ma X-R, Cai M-Y, Li Y, Zang Y, Jia F-J, Lin Y-Q, Chiu HFK, Ungvari GS, Hall BJ, et al. Comorbid moderate–severe depressive symptoms and their Association with Quality of Life in Chinese patients with Schizophrenia treated in primary care. Commun Ment Health J. 2016;52(8):921–6.
Leon AC, Olfson M, Portera L, Farber L, Sheehan DV. Assessing Psychiatric Impairment in Primary Care with the Sheehan disability scale. Int J Psychiatry Med. 1997;27(2):93–105.
Leu SH, Chou JY, Lee PC, Cheng HC, Shao WC, Hsien WL, Huang CL, Chen VC. Validity and reliability of the Chinese version of the Sheehan disability scale (SDS-C). Asia Pac Psychiatry. 2015;7(2):215–22.
Mackinnon A. A spreadsheet for the calculation of comprehensive statistics for the assessment of diagnositic tests and inter-rater agreement. Comput Biol Med. 2000;30(3):124–34.
Fervaha G, Agid O, Takeuchi H, Foussias G, Remington G. Life satisfaction and happiness among young adults with schizophrenia. Psychiatry Res. 2016;242:174–9.
Agid O, McDonald K, Siu C, Tsoutsoulas C, Wass C, Zipursky RB, Foussias G, Remington G. Happiness in first-episode schizophrenia. Schizophr Res. 2012;141(1):98–103.
Agid O, McDonald K, Fervaha G, Littrell R, Thoma J, Zipursky RB, Foussias G, Remington G. Values in First-Episode Schizophrenia. Can J Psychiatry. 2015;60(11):507–14.
Immonen J, Jääskeläinen E, Korpela H, Miettunen J. Age at onset and the outcomes of schizophrenia: a systematic review and meta-analysis. Early Interv Psychiat. 2017;11(6):453–60.
Bjørlykhaug KI, Karlsson B, Hesook SK, Kleppe LC. Social support and recovery from mental health problems: a sco** review. Nordic Social Work Research. 2022;12(5):666–97.
Harvey CA, Jeffreys SE, McNaught AS, Blizard RA, King MB. The Camden Schizophrenia surveys III: five-year outcome of a sample of individuals from a Prevalence Survey and the importance of Social relationships. Int J Soc Psychiatry. 2007;53(4):340–56.
Vass V, Morrison AP, Law H, Dudley J, Taylor P, Bennett KM, Bentall RP. How stigma impacts on people with psychosis: the mediating effect of self-esteem and hopelessness on subjective recovery and psychotic experiences. Psychiatry Res. 2015;230(2):487–95.
Samele C, van Os J, McKenzie K, Wright A, Gilvarry C, Manley C, Tattan T, Murray R. On behalf of the UKG: does socioeconomic status predict course and outcome in patients with psychosis? Soc Psychiatry Psychiatr Epidemiol. 2001;36(12):573–81.
Rotstein A, Roe D, Gelkopf M, Levine SZ. Age of onset and quality of life among males and females with schizophrenia: a national study. Eur Psychiatry: J Association Eur Psychiatrists. 2018;53:100–6.
Hui CL-M, Li AW-Y, Leung C-M, Chang W-C, Chan SK-W, Lee EH-M, Chen EY-H. Comparing illness presentation, treatment and functioning between patients with adolescent- and adult-onset psychosis. Psychiatry Res. 2014;220(3):797–802.
Helle S, Ringen PA, Melle I, Larsen T-K, Gjestad R, Johnsen E, Lagerberg TV, Andreassen OA, Kroken RA, Joa I, et al. Cannabis use is associated with 3years earlier onset of schizophrenia spectrum disorder in a naturalistic, multi-site sample (N = 1119). Schizophr Res. 2016;170(1):217–21.
Arango C, Díaz-Caneja CM, McGorry PD, Rapoport J, Sommer IE, Vorstman JA, McDaid D, Marín O, Serrano-Drozdowskyj E, Freedman R, et al. Preventive strategies for mental health. The Lancet Psychiatry. 2018;5(7):591–604.
Fusar-Poli P, McGorry PD, Kane JM. Improving outcomes of first-episode psychosis: an overview. World Psychiatry. 2017;16(3):251–65.
Catone G, Marwaha S, Lennox B, Broome MR. Bullying victimisation and psychosis: the interdependence and independence of risk trajectories. BJPsych Adv. 2017;23(6):397–406.
Priebe S, McCabe R, Junghan U, Kallert T, Ruggeri M, Slade M, Reininghaus U. Association between symptoms and quality of life in patients with schizophrenia: a pooled analysis of changes over time. Schizophr Res. 2011;133(1):17–21.
Sosnowski R, Kulpa M, Ziętalewicz U, Wolski JK, Nowakowski R, Bakuła R, Demkow T. Basic issues concerning health-related quality of life. Cent Eur J Urol. 2017;70(2):206–11.
Wilkinson G, Hesdon B, Wild D, Cookson R, Farina C, Sharma V, Fitzpatrick R, Jenkinson C. Self-report quality of life measure for people with schizophrenia: the SQLS. Br J Psychiatry. 2000;177(1):42–6.
Acknowledgements
This study is supported by Guangdong Provincial Innovation Platform of Translational Medicine (Early recognition and intervention of major mental diseases), Guangdong Provincial innovation Platform of Public Health.
Funding
The cohort study was funded by Guangdong Provincial Foundation for Basic and Applied Basic Research Natural Science Foundation [grant number: 2022A1515010619].
Author information
Authors and Affiliations
Contributions
Study design: C.M., C-L.H. and C.H. Data collection analysis and interpretation: C.M., Z.-H.H., F.W., S.B.W. Drafting of the manuscript: C.M. Critical revision of the manuscript: C-L. H. and C.H. Approval of the final version for publication: all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval for the project was received from all relevant University and Health Network Human Ethics Committees: Public Health Ethics Committee of Guangdong Provincial People’s Hospital Z2019-120, and the University of Melbourne Human Ethics Committee 2021-20740-15415-3. The study was conducted in accordance with the Declaration of Helsinki. Informed written consent was obtained at the beginning of each interview.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Migliorini, C., Harvey, C., Hou, C. et al. Subjective quality of life and schizophrenia: results from a large cohort study based in Chinese primary care. BMC Psychiatry 24, 86 (2024). https://doi.org/10.1186/s12888-024-05558-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12888-024-05558-w