
Abstract
Background
In environments with limited resources, undernutrition is a serious public health risk. Its dual relationship to human immunodeficiency virus infection (HIV) leads to crises in a child's physical, emotional, social, and economic spheres of life. Nevertheless, little research has been done on the survival rate and risk factors that lead to poor survival outcomes in undernourished children receiving antiretroviral therapy. This study sought to evaluate survival status and its predictors among undernourished children on antiretroviral therapy (ART) in public health facilities, Bahir Dar city, September 1, 2010 – December 31, 2020.
Methods
An institution-based retrospective cohort study design was used among 414 study participants from September 1, 2010 – December 31, 2020. A simple random sampling method was applied to select study participants. All collected data were entered into epi data version 4.6 and exported to STATA version 14.0 for analysis. Each independent predictor variable with a p-value < 0.05 in the multivariable Cox proportional hazard regression was considered statistically significant.
Results
The overall incidence of mortality was 11.6 deaths per 1000 child year observation (95%CI: 7.7- 17.5). Baseline weight for age < -3 Z score (adjusted hazard ratio (AHR) = 4.9, 95% CI: 1.30–18.98), height for age < -3 Z score (AHR = 4.34, 95%CI 1.13–16.6), cotrimoxazole prophylaxis given (AHR = 0.27, 95%CI 0.08–0.87), hemoglobin level < 10 g/dl (AHR = 3.7, 95%CI 1.1–12.7), CD4 cells < threshold (AHR = 4.86, 95%CI 1.9–12.7), and WHO clinical disease stage III and IV (AHR = 8.1, 95%CI 1.97–33) were found independent predictors of mortality.
Conclusion and recommendation
The incidence of mortality was determined in the study to be 11.6 per 1000 child years. Mortality was predicted by severe stunting, severe underweight, a low hemoglobin level, a low CD4 count, and WHO clinical stages III and IV. But the risk of death is reduced by starting cotrimoxazole preventative therapy early. The risk factors that result in a low survival status should be the primary focus of all concerned bodies, and early cotrimoxazole preventive treatment initiation is strongly recommended.
Similar content being viewed by others


Introduction
Undernutrition is defined as an insufficient intake of energy and nutrients to meet an individual’s needs to maintain optimum health [1]. It is the consequence of an insufficient intake of macronutrients and/or micronutrients, poor absorption or rapid loss of nutrients due to increased energy expenditure or illness and manifests in four broad formation: stunting, underweight, wasting, and micronutrient deficiencies [2]. According to World Health Organization (WHO), low weight for age is referred to as underweight. Underweight children may be wasted, stunted, or both [3]. Being low weight relative to height is called wasting. It might also last for a very long period. Usually, it signifies recent and significant weight reduction [3, 4]. The definition of stunting is low height for age. It is brought on by persistent or recurring undernutrition, which is typically linked to poverty, a high rate of disease, and/or improper early nutrition and care [4].
The burden of undernutrition among children on antiretroviral-therapy (ART) remains public health concern and the pathophysiologic effect of undernutrition results in poor absorption of ART from the gut and leads to inadequate concentration of ART which may lead to unpleasant health outcome including death [5, 6].
Besides, its effect among children with HIV infection is devastating and has increased the risk of mortality even after nutritional and medical interventions. In addition to this, it has adverse consequences in later life such as; low intellectual ability, low work productivity, poor school achievements, and being in poverty [7, 8].
Despite the fact that ART has saved millions of children from death, studies have revealed a short survival time among undernourished children compared to well-nourished children in resource-limited settings [9]. Also, undernutrition is not confined to resource-limited settings; it has been noted in chronic infections like HIV anywhere in the world [10].
In Sub-Saharan Africa, including Ethiopia, the magnitude of undernutrition has increased since 2015 from 17 to 22%, and HIV/AIDS-related burdens remain high [11, 12]. In Nigeria, the prevalence of being underweight, stunting, and wasting among HIV-positive children under the age of five was 77%, 65%, and 63%, respectively [13]. In a Cameroonian hospital, undernutrition was 68.7% among children with HIV [14]. In Northwest Ethiopia, 64% of children with HIV infection were undernourished [15].
Due to an imbalance between the body’s calorie requirement and daily calorie intake among children with HIV infection, children are likely to rapid disease progression, increased morbidity, and reduced survival [16, 17]. Different studies have shown predictors of mortality among HIV positive children. Low CD4 count/below thresh hold at the time of ART initiation, advanced WHO stage of disease, compromised nutritional status, poor adherence to ART are some of the independent predictors of mortality [5, 6, 18, 19].
In order to end undernutrition by 2030, the Ethiopian government runs initiatives like the Sustainable Undernutrition Reduction in Ethiopia, which took the place of the previous community-based nutrition program and works in partnership with different concerned organizations like UNICEF, Nutrition International, and a significant number of others [20,21,22].
The efforts made by Ethiopian government has showed consistent economic growth, significant pro-poor spending, and appreciable agriculture and health extension networks that collectively have resulted in a remarkable reduction in undernutrition [23]. Nevertheless, the alarmingly high (28%) magnitude of child mortality linked to undernutrition persists [21].
Furthermore, in Ethiopia, the number of children to be treated for severe undernutrition in 2020 alone has increased by 24% due to the effects of desert locusts, the COVID-19 pandemic, ongoing and severe droughts, climatic change, and internal displacements [24]. A rise of this magnitude will surely result in child mortality, especially in children with chronic diseases, HIV/AIDS, and recurrent infections who are likely to die from undernutrition [22, 24]. Therefore, this study aimed to assess survival status and its predictors among undernourished children on ART in public health facilities, Bahir Dar city, Northwest Ethiopia, September1, 2010 – December 31, 2020.
Methods and materials
Study area and study period
Bahir Dar city is the administrative capital of Amhara regional state and located 565 km Northwest of Addis Ababa, Ethiopia’s capital city. The city has two referral hospitals, one primary hospital, and 10 health centers. From those public health facilities, one referral hospital, one primary hospital, and 8 health centers have been giving ART services. According to November 2019s Amhara regional health bureau report the people receiving ART are about 142,593 of these 5637 are children. The total number of children receiving ART from 2010 to 2020 accounts for 1621. Of these children, about 634 were undernourished at the initiation of ART. The chart review was held in Bahir Dar city from March 10 to April 10, 2021.
Study design
A Facility based retrospective cohort study design was used.
Source population
All undernourished children less than 15 years old who initiated ART in public health facilities, Bahir Dar city.
Study population
All undernourished children under 15 years old who received ART in Bahir Dar city public health facilities between September 1, 2010, and December 31, 2020. We only considered under fifteen children because children aged 15 and above were considered adults according to the national consolidated ART care, prevention, and treatment guidelines.
Inclusion and exclusion criteria
Inclusion criteria
All undernourished children who were on ART from September1, 2010 to December31, 2020.
Exclusion criteria
Patients with incomplete baseline information’s (like; the child’s age, baseline nutritional status, initiation date of ART and exit date from the cohort).
Study variables
Outcome variable
Death.
Independent variables
Socio demographic Factors: Age, Sex, Residence, Caregiver Relationship, Caregiver HIV Status, Parental Live Status, Caregiver Marital Status, and Caregiver Occupational Status. Baseline clinical and lab-related factors: WHO clinical stage, hemoglobin count, CD4 count, opportunistic infection, child’s function status, developmental status, nutritional status, IHN prophylaxis, and CPT prophylaxis. ART-related factors: Adherence to ART drugs, time of initiation, and regimen-related.
Sample size determination
By utilizing the double population proportion formula, along with the assumptions of a 95% confidence interval, 80% power, and a 1:1 ratio of exposed to unexposed individuals, the sample size was determined using Epi Info software. From the explanatory variables, height for age (normal/unexposed versus severely stunted/exposed), with 23.4% outcome among exposed and 4.5% outcome among unexposed, gave a sample size of 180. Again, weight for height (normal/unexposed versus severely wasted/exposed), with a 27.8% outcome among exposed and a 6.27% outcome among unexposed, gave a sample size of 218. The CD4 count outcome, with 12% of individuals falling below the threshold (exposed) and 4.3% above the threshold (unexposed), gave a sample size of 396. Further, many other variables other than the aforementioned were considered, but they gave a sample of small size. Based on this, the maximum required sample size was calculated to be 396 [25], and an additional 10% was added to account for incomplete charts, resulting in a final sample size of 436.
Sampling procedure and sampling technique
This procedure took into consideration the uniformity of ART-standard services offered by all public health facilities. All public health facilities provided the medical registration numbers (MRN) of the undernourished children, which were then combined and input into Microsoft Excel. After importing these data into the Statistical Package for the Social Sciences (SPSS) software, a random sample of 436 undernourished children out of the 634 total undernourished children across eleven public health facilities was created. Finally, the sample unit was reached by using a MRN (Fig. 1).

Diagrammatic representation of sampling procedure to assess survival status and its predictors among undernourished children on ART in public health facilities, Bahir Dar city from September 1, 2010 – December 31, 2020
Operational definitions
Survival status- Defined as the length of time from ART initiation to death or censure.
Undernutrition- Child having height for age < -2 Z score, and/or weight for age < -2 Z score, and/or Weight for height/length < -2 Z score according to (2006) WHO standard curve [4].
ART Adherence- For children is classified based on the percentage of ART dosage calculated from the total monthly doses of ART drugs: good > 95%, fair = 85 − 94%, and poor < 85% [26].
Censored- Children alive beyond the study period, lost to follow up and transfer out to other health facility.
Developmental miles- Were described as appropriate, delayed, and regressive for children under the age of five [27].
Developmentally appropriate- Refers to the child having achieved all domains of development milestones for his or her age.
Developmentally delayed- Means when a child is slowed to reach one or more developmental milestones compared to his/her peers.
Developmentally regressive- This is the loss of acquired milestones in a normally develo** child who has reached all developmental milestones.
Functional status- Was expressed as working (go to school, do normal activity, etc.), ambulatory (able to perform routine daily activities), and bedridden (not able to perform routine daily activities) for children aged five and above [27].
Data collection tools and procedures
Data were extracted through chart review using structured checklists that were adapted from ART intake and follow-up forms after reviewing different kinds of literature [6, 18, 25, 28,29,30,31]. The data extraction checklist comprises socio-demographic characteristics, which contained nine questions; baseline clinical, laboratory, and ART information, which in general had twenty-five questions; and the outcome variable (dead, dropout, transfer out, and alive on ART) section, which had six questions. The starting point for retrospective follow-up for each subject was from the date of ART initiation to the date of death if died, from the date of ART initiation to the date of the final visit if lost to follow-up, and from the date of ART initiation to the Alive on ART if alive at the end of the study. The WHO Anthro and AnthroPlus software for health data was used to gather information about the nutritional status and evaluate the children's growth and development for their age.
Data quality assurance
Prior to the actual data collection, a pretest involving 5% of the sample population was carried out to assess the checklists' consistency. Then variables in the tools that could have been incomplete were eliminated, considering the pretest results. Two days of training were given to both the supervisor and the data collectors. One BSc. nurse oversaw the data gathering process, while three diploma nurses collected the data. Before data analysis, the proper data entry methods were used with epi-data version 4.6. The frequency and completeness of the data were checked before exporting to Stata for further analysis.
Data processing and analysis
The entered data into epi-data software version 4.6 was exported to Stata version 14.0 for analysis. The socio-demographic and clinical features were described for the entire cohort by using frequencies for categorical variables. The mean with standard deviation were used to describe the characteristics of continuous variables. The outcome variable was dichotomized into censored and death. Before running the Cox regression model, multi-collinearity and interaction terms were checked by using the variance inflation factor (VIF), which gave an overall mean value of 1.74 and a mean value less than 10 for each independent variable. Cox proportional hazard model assumptions were checked by using a global test and graphically by using the Kaplan–Meier versus predicted survival plot of the categorical independent variables. The global test P-value greater than 0.05 shows the Cox proportional hazard model assumption was satisfied. Each independent predictor variable with a p-value < 0.2 in the bivariable analysis was included in the multivariable Cox proportional hazard regression model. In the multivariable Cox regression model, variables with a P-value < 0.05 were considered statistically significant. Differences in overall survival probability curves were displayed by using Kaplan–Meier plots, and a log-rank test was used to compare the survival time between different categories of explanatory variables. The hazard ratio and p-value were used to show the level of association between explanatory variables and an outcome variable.
Results
Baseline socio demographic characteristics of undernourished children on ART
Of the total 436 charts reviewed, 414 charts of undernourished children on ART were included in the analysis, which gave a completeness rate of 94.95%. Of those children, 220 (53.14%) were males, and 342 (82.61%) resided in urban areas. The mean age of children was 7.63 ± 0.2 years, and above two-thirds (69.81%) of children were following ART care services in hospitals. Regarding the incidence of death, the majority (52.2%) of deaths occurred among female children, and 35% of deaths occurred among adolescents aged 10 and less than 15 years. Around ¾ of deaths occurred among urban residents, and 87% of deaths occurred among children following ART services in hospitals (Table 1).
Baseline socio demographic characteristics of children’s primary care givers information
Of the total, 370 (89.37%) of children’s primary caregivers were parents and about (66.91%) of caregivers were married. Regarding to parental status of child, almost sixty six percent (65.7%) of parents were alive and around twenty nine percent 122 (29.47%) of children had at least one parent died. Concerning to occupational status of care givers, more than one fourth (25.79%) of care givers were house wife and around twenty two percent (22.14%) were merchants. The majority (56.6%) of deaths recorded were among children who had both alive parents, and approximately 83% of dead children live with one or both of their parents. The majority of primary caregivers of deceased children were married, and 74% of deaths happened among children living with HIV-positive caregivers. The majority (26.1%) of deaths were recorded among the children of merchants (Table 2).
Baseline clinical and laboratory profiles
From the total, approximately sixty percent 246 (59.42%) of children had at least one opportunistic infection(OI) at time of ART initiation and of these opportunistic infections the most common one was upper respiratory tract infections (URTI’s) which accounts around twenty three percent 56 (22.77%) (Fig. 2).

Baseline opportunistic infections among undernourished children on ART in public health facilities, Bahir Dar city, Northwest Ethiopia, September1, 2010 – December 31, 2020
The majority (69.08%) of children were in WHO clinical stages I and II, and about 82.78% of participant children had CD4 count greater than or equal to threshold. Concerning nutritional status; about 145 (35.02%) of children had moderate stunting, about 108 (26.08%) of children had moderate underweight, and above half (55.56%) of children had no wasting. The majority (95.54%) of children had baseline hemoglobin levels greater than or equal to 10 g/dl, and the majority (87.65%) of children had a viral load fewer than 1000 copies. About 338 (81.64%) of children had baseline cotrimoxazole preventive treatment history, and more than sixty one percent (61.11%) of children had no history of baseline isoniazid preventive treatment. Regarding developmental milestones, about 104 (85.25%) of under-five children had appropriate developmental miles for their age, and regarding to the functional status of five and above five years old children, the majority (92.81%) of the children were working. In regard to death, approximately 78% of deaths among children had one or more opportunistic infections, and 69.6% of deaths recorded among children were in WHO stages III and IV. The majority (80%) of deaths occurred among under-five children who had appropriate development for their age, and approximately 85% of deaths happened among children older than five years who were working. The majority (52%) of deaths were recorded among children who had a CD4 count lower than the threshold, and 30.4% of the deaths occurred among children who had a hemoglobin level less than 10 g/dl. About 65.2%, 78.3%, and 43.5% of deaths occurred among children who were severely underweight, severely stunted, and severely wasted, respectively. Regarding IHN and cotrimoxazole preventive therapy, 82.6% of deaths happened among children who didn’t take IHN prophylaxis, and 78.3% of deaths occurred among children who took cotrimoxazole prophylaxis (Table 3).
Antiretroviral therapy related factors
Regarding ART eligibility criteria, above half (53.62%) of children were eligible by both WHO clinical stage and immunological. Concerning the ART initiation time, about 211 (50.97%) of children initiated ART immediately within seven days of eligibility. The majority (65.22%) of participants had initial ART change history and a total of 245 (90.74%) of changes were within the first line. A frequent reason (41.85%) for change was the availability of new drugs, and about 77 (18.6%) of children had drug side effect reports. About 93% of children had good adherence to ART at first three months. In relation to death, approximately 74% of deaths were recorded among children who had no reports of ART drug side effects. The majority (78.3%) of deaths occurred among children who were eligible for ART by both CD4 count and WHO clinical stage criteria and 52.2% of deaths occurred among children who started ART on the 7th day or longer after ART eligibility. Approximately 60% of deaths were recorded among children who had no ART regimen change, and 87% of deaths occurred among children who had good ART adherence (Table 4).
Concerning the initial ART regimen, the majority (36.47%), 21.26%, and 16.18% of children initiated AZT-3TC-NVP, AZT-3TC-EFV, and d4T-3TC-NVP, respectively, and about 1.69, 0.97, and 0.72% of participants initiated ABC-3TC-DTG, AZT-3TC-LPV/r, and TDF-3TC-NVP, respectively (Fig. 3).

Initial ART regimen among undernourished children on ART in public health facilities, Bahir Dar city, Northwest Ethiopia, September 1, 2010 – December 31, 2020
Survival status of undernourished children on ART
This study followed for a minimum of one month and a maximum of one hundred twenty-three months. Within a median follow-up of 61 months, a total of 319 (77.05%) children were alive beyond the study period, 23 (5.56%) died (95% CI: 3.7–8.2), 6 (1.45%) dropped out, and 66 (15.94%) transferred out. Regarding time to death, 50%, 54.55%, and 68.18% of death occurred at twelve, twenty-four, and thirty-six months respectively. The mean survival time for the entire cohort was 116.1 months (95% CI: 113.35—118.85) with a standard deviation of 1.40 months. An estimated cumulative survival probability at 3, 6, 12, 24, 36, and 123 months were 0.985, 0.9704, 0.9704, 0.9677, 0.9587, and 0.9189 respectively. The overall incidence of death was 11.6 per 1000 child year observation (95% CI: 7.7—17.5). This entire cohort followed for a total of 23,760 months. An overall Kaplan Meier survival estimate showed that the incidence of death was highest at an early age (first 36 months) on ART compared to later ages on ART (Fig. 4).

Kaplan Meier Estimate of an overall survival functions among undernourished children on ART in public health facilities, Bahir Dar city, Northwest Ethiopia, September 1, 2010 – December 31, 2020
Comparison of survival curves over categorical variables
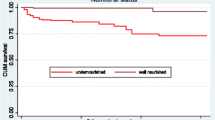
As a log-rank test results showed significant differences exist among different explanatory variables. Among the variables, baseline nutritional status, baseline CD4 count (less than threshold versus greater than or equal to threshold), baseline hemoglobin level greater than or equal to 10 g/dl versus less than 10 g/dl, WHO clinical stage I and II versus stage III and IV, and initial regimen changed versus not changed. The mean survival time for participants with baseline underweight was 111.6 ± 2.6 months while the mean survival time for not underweight participants was 118.3 ± 1.3 months (Fig. 5).

Kaplan Meier survival curves to compare undernourished children on ART with categories of weight for age in public health facilities, Bahir Dar city, Northwest Ethiopia, September 1, 2010 – December 31, 2020
Children presented with baseline height for age (H/A) < -2 Z score had shorter survival mean time compared to participants presented with ≥ -2 Z score. The mean survival time was 113.5 ± 2 months for participants H/A < -2 Z score and 118.7 ± 1.3 months for participants H/A ≥ -2 Z score (Fig. 6).

Kaplan Meier survival curves to compare undernourished children on ART with categories of height for age in public health facilities, Bahir Dar city, Northwest Ethiopia, September 1, 2010 – December 31, 2020
Children presented with baseline hemoglobin level < 10 g/dl had shorter survival mean time compared to participants presented with ≥ 10 g/dl. The mean survival time was 113.8 ± 2 months for participants < 10 g/dl and 117.9 ± 1.5 months for participants ≥ 10 g/dl (Fig. 7).

Kaplan Meier survival curves to compare undernourished children on ART with categories of baseline hemoglobin level in public health facilities, Bahir Dar city, Northwest Ethiopia, September 1, 2010 – December 31, 2020
The mean survival time for children presented with CD4 count below threshold was lower than for their counterpart children ≥ threshold (102 ± 5 months and 117 ± 1 months, respectively) (Fig. 8).

Kaplan Meier survival curves to compare undernourished children on ART with categories of baseline CD4 count in public health facilities, Bahir Dar city, Northwest Ethiopia, September 1, 2010 – December 31, 2020
An estimated mean survival time for children with advanced WHO clinical stage was 108 ± 3.5 months while 117.8 ± 1.2 months for those with mild WHO clinical stage presentation (Fig. 9).

Kaplan Meier survival curves to compare undernourished children on ART with categories of baseline WHO clinical stage in public health facilities, Bahir Dar city, Northwest Ethiopia, September1, 2010 – December 31, 2020
Predictors of mortality
Temporary relation between explanatory variables and death was analyzed using Cox proportional hazard regression model. In multivariable analysis, about six variables had a statistically significant relation to the risk of death among children. These are baseline weight for age (W/A) ≥ -2 Z score versus weight for Age (W/A) < 2 Z score, baseline height for age (H/A) ≥ -2 Z score Versus H/A <—2 Z score, baseline cotrimoxazole prophylaxis given versus not given, baseline hemoglobin level ≥ 10 g/dl versus hemoglobin level less than 10 g/dl, CD4 count ≥ threshold versus CD4 count less than threshold, WHO clinical stage I&II versus stage III & IV and regimen changed versus regimen not changed. As multivariable analysis result has shown, children with baseline weight for age (W/A) < -3 Z score were almost 4.9 times more likely to survive shorter duration as compared to children with baseline weight for age (W/A ≥ -2 Z score (AHR: 4.9, 95% CI: 1.3, 18.98) (p-value = 0.02). Children exposed to baseline stunting (H/A) < -3 standard Z score were 4.34 times at more risk to death as compared to children who didn’t expose to baseline stunting (H/A) ≥ -2 standard Z score (AHR = 4.34, 95%CI 1.13, 16.6) (p-value = 0.03). Regarding to cotrimoxazole prophylaxis, the estimated hazard of death among children who did take baseline cotrimoxazole prophylaxis properly was reduced by 73% as compared to their counterpart children who didn’t take baseline cotrimoxazole prophylaxis (AHR = 0.27, 95%CI 0.09, 0.87) (p-value = 0.03). Children presented with baseline hemoglobin level < 10 g/dl were almost 3.7 times more likely to survive a shorter duration than those children with baseline hemoglobin level ≥ 10 g/dl (AHR = 3.7, 95%CI 1.1, 12.7) (p-value = 0.037). In multivariable analysis, an estimated hazard of death was 4.86 times high among children with baseline CD4 < threshold as compared to those children with CD4 count ≥ threshold (AHR = 4.86, 95%CI 1.9, 12.7) (p-value = 0.001). Moreover, children with baseline WHO clinical disease stage (III and IV) were almost 8.1 times more risk to death than those children presented with WHO clinical stage I and II (AHR = 8.1, 95%CI 1.97, 33) (p-value = 0.004). Children who had a history of regimen change have a low risk of mortality compared to children with no regimen change history (AHR = 0.35, 95%CI 0.12, 1.00) (p-value = 0.05) (Table 5).
Discussion
The study found that the overall mortality rate was 11.6 per 1000 child-year observation (95% CI: 7.7—17.5). The mortality rate observed in this study aligns with findings from Southwest Ethiopia (11.2 deaths per 1000 child-year observations) [18], Asia–Pacific (16.5 deaths per 1000 child years) [32], and the International Maternal Pediatric Adolescent AIDS Clinical Trials (IMPAACT) P1074 multicenter cohort studies in the United States (7 per 1000 child years) [33]. However, the result indicate a lower mortality rate compared to studies conducted in the Benishangul Gumuz region (54 deaths per 1000 child years) [34], Northwest Ethiopia (54 deaths per 1000 child years) [35], referral hospitals of Amhara regional state (44 deaths per 1000 child years) [25], selected public hospitals of the Addis Ababa city administration (4.98 deaths per 1000 child months) [36], the government ART centers in Mumbai, India (22.75 deaths per 1000 child years) [37], and Tanzania (135 per 1000 child years) [38].
Possible reasons for the variations among these studies could be the difference in health care awareness and knowledge level of the community, sample size, study period, and/or characteristics of the study participants, the difference in the adherence level of the ART, the difference in utilization of cotrimoxazole preventive therapy, the difference in a level of efforts to overcome adherence barriers regarding ART care and treatment, and the availability of advanced treatment modalities with low side effects.
In this study, children having weight for age < -3 Z score were almost 4.9 times more risk to death compared to children with weight for age > -2 Z score. This finding was in line with studies done in Arbaminch Town Southern Ethiopia [31], Wolaita zone southern Ethiopia [29], Debre Tabor and Dessie Northern Ethiopia [28], and Tanzania [39]. These could be due to undernutrition: there may be a delayed recovery from infections, an accelerated disease progression, a tendency for opportunistic infections, and a reduced ART response. Height for age was another predictor of mortality. This finding was in agreement with researches conducted in Benishangul Gumuz region [34], Amhara referral hospitals and India [25, 40]. These could be because undernutrition is a major predictor of treatment failure [41, 42], and undernourished children are at increased risk of dying as a result of the detrimental effects of undernutrition on ART treatment.
Children presented with hemoglobin level < 10 g/dl had a higher risk of death compared to children presented with hemoglobin level ≥ 10 g/dl. Previous study findings in Ethiopia [25, 29, 36, 43], Tanzania [39], and Kenya [44] had shown that low hemoglobin level was a significant risk of death among children on ART. These could be justified by the fact that when ART is started after a child experiences anemia from HIV infection, the child’s condition may only be partially cured, which could eventually lead to a low quality of life and mortality [45].
Baseline CD4 count was found significant predictor of mortality in this study. Children who were presented with a CD4 count below threshold at the time of ART initiation were approximately 4.7 times high risk to death compared to children with a baseline CD4 count greater than threshold. This finding was consistent with study findings in Ethiopia [25, 31], multiregional cohort analysis (Asia Pacific, East Africa, Southern Africa, West Africa) [46], India [40], and Tanzania [39]. A possible reason might be that low CD4/ immunodeficiency results in serious life-threatening opportunistic infections of the CNS, RS, and GI, as well as others [8] which in turn increases the risk of death in the early stages of treatment before responding to initiated ART.
An advanced WHO clinical stage of disease at the time of ART initiation was a predictor of mortality among undernourished children on ART. Children presented with advanced WHO disease stages (WHO stages III and IV) were at high risk of death compared to their counterparts who presented with mild WHO clinical stages I and II. Similar findings were reported in previous studies in Ethiopia [18, 25, 31], Vietnam [47], Swaziland [48], India [40], Cameroon [49], Tanzania [39], and South Africa [50]. These could be explained by the fact that in these children, antiretroviral therapy initiation could result in an immune reconstitution inflammatory syndrome due to severe immune cell depletion and progressive disease [8].
Children who took baseline cotrimoxazole preventive therapy were less likely to die for a shorter duration compared to their counterparts. The risk of death among children who took baseline cotrimoxazole preventive therapy was reduced by 73%. This finding was supported in previous studies in Ethiopia [31, 51, 52], Sub-Saharan Africa [53], and Asia [54]. The possible justification might be related to the therapy’s crucial role in preventing opportunistic infections and promoting immune recovery [55].
Conclusion and recommendation
The incidence of mortality was determined in the study to be 11.6 per 1000 child years. Mortality was predicted by severe stunting, severe underweight, a low hemoglobin level, a low CD4 count, and WHO clinical stages III and IV. But the risk of death is reduced by starting cotrimoxazole preventative therapy early. The risk factors that result in a low survival status should be the primary focus of all concerned bodies, and early cotrimoxazole preventive treatment initiation is strongly recommended.
Limitations of the study
Due to the secondary nature of the data, important nutritional factors like micronutrient deficiencies, feeding practices, food insecurity, wealth index, parental educational status, and combined nutritional status were not included in the study.
Availability of data and materials
Data set used in this study will be available from corresponding author on reasonable request.
Abbreviations
- AHR:
-
Adjusted Hazard Ratio
- AIDS:
-
Acquired Immune Deficiency Syndrome
- ART:
-
Antiretroviral Therapy
- CD4:
-
Cluster of differentiation of cells
- CI:
-
Confidence interval
- COVID:
-
Corona Virus Disease
- FMOH:
-
Federal Ministry of Health
- HA:
-
Height for Age
- HIV:
-
Human Immunodeficiency Virus
- HR:
-
Hazard Ratio
- IMPAACT:
-
International Maternal Pediatric Adolescent AIDS Clinical Trials
- IHN:
-
Isoniazid
- MRN:
-
Medical Registration Number
- OI:
-
Opportunistic Infection
- PLHIV:
-
People Living with Human Immune Virus
- PYO:
-
Person Year Observation
- RR:
-
Relative Risk
- SD:
-
Standard Deviation
- SPSS:
-
Statistical Package for the Social Sciences
- UNAIDS:
-
Joint United Nations Program on HIV and AIDS
- UNICEF:
-
United Nations International Children’s Emergency Fund
- WA:
-
Weight for Age
- WH:
-
Weight for Height
References
Maleta K. Undernutrition. Malawi Med J. 2006;18(4):189–205.
Sheet P. Nutrition at the World Food Programme. 2012.
World Health Organization. Levels and trends in child malnutrition: key findings of the. 2019th ed. Geneva: World Health Organization; 2019.
World Health Organization. WHO child growth standards: length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methods and development. Geneva: World Health Organization; 2006.
Sunguya BF, Poudel KC, Otsuka K, Yasuoka J, Mlunde LB, Urassa DP, et al. Undernutrition among HIV-positive children in Dar es Salaam, Tanzania: antiretroviral therapy alone is not enough. BMC Public Health. 2011;11(1):1–11.
Mutanga JN, Mutembo S, Ezeamama AE, Song X, Fubisha RC, Mutesu-Kapembwa K, et al. Long-term survival outcomes of HIV infected children receiving antiretroviral therapy: an observational study from Zambia (2003–2015). BMC Public Health. 2019;19(1):1–12.
Bwakura-Dangarembizi M, Amadi B, Bourke CD, Robertson RC, Mwapenya B, Chandwe K, et al. Health outcomes, pathogenesis and epidemiology of severe acute malnutrition (HOPE-SAM): rationale and methods of a longitudinal observational study. BMJ Open. 2019;9(1):e023077.
Kliegman R, St Geme J, Blum N, Shah S, Tasker RC. Nelson Textbook of Pediatrics. Philadelphia: Elsevier; 2019.
Njom Nlend AE, Motaze AN, Ndiang ST, Fokam J. Predictors of virologic failure on first-line antiretroviral therapy among children in a referral pediatric center in Cameroon. Pediatr Infect Dis J. 2017;36(11):1067–72.
Luo H, Zyba SJ, Webb P. Measuring malnutrition in all its forms: An update of the net state of nutrition index to track the global burden of malnutrition at country level. Glob Food Sec. 2020;26:100453.
UNICEF. Children, food and nutrition: growing well in a changing world. The State of the World’s Children. 2019;2019.
United Nations Children's Fund WHO, International Bank for Reconstruction, Bank DTW. Levels and trends in child malnutrition: key findings of the 2018 Edition of the Joint Child Malnutrition Estimates. UNICEF New York, WHO Geneva and the Development Data Group of the World Bank, Washington DC; 2019.
Akintan PE, Akinsulie A, Temiye E, Esezobor C. Prevalence of wasting, stunting, and underweight among HIV infected underfives’, in Lagos using WHO z score. Nig Q J Hosp Med. 2015;25(2):124–8.
Penda CI, Moukoko ECE, Nolla NP, Evindi NOA, Ndombo PK. Malnutrition among HIV infected children under 5 years of age at the Laquintinie hospital Douala, Cameroon. Pan African Med J. 2018;30(1).
Melku M, Enawgaw B, Ayana S, Anlay DZ, Kebede A, Haile A, et al. Magnitude of anemia and undernutrition among HIV-infected children who took HAART: a retrospective follow-up study. Am J Blood Res. 2020;10(5):198–209.
Hu R, Mu W, Sun X, Wu H, Pang L, Wang L, et al. Growth of HIV-infected children in the early stage of antiretroviral treatment: a retrospective cohort study in China. AIDS Patient Care STDS. 2016;30(8):365–70.
World Health Organization. Guidelines for an integrated approach to the nutritional care of HIV-infected children (6 months-14 years). 2009.
Oumer A, Kubsa ME, Mekonnen BA. Malnutrition as predictor of survival from anti-retroviral treatment among children living with HIV/AIDS in Southwest Ethiopia: survival analysis. BMC Pediatr. 2019;19(1):1–10.
Sunguya BF, Poudel KC, Mlunde LB, Urassa DP, Yasuoka J, Jimba M. Poor nutrition status and associated feeding practices among HIV-positive children in a food secure region in Tanzania: a call for tailored nutrition training. PLoS ONE. 2014;9(5):e98308.
Buse K, Hawkes S. Health in the sustainable development goals: ready for a paradigm shift? Global Health. 2015;11:13.
UNICEF. For every child, nutrition. 2020; 2019.
Feyissa YM, Hanlon C, Emyu S, Cornick RV, Fairall L, Gebremichael D, et al. Using a mentorship model to localise the Practical Approach to Care Kit (PACK): from South Africa to Ethiopia. BMJ Glob Health. 2019;3(Suppl 5):e001108.
UNICEF. Joint malnutrition estimates. 2020.
Alebel A, Wagnew F, Tesema C, Kibret GD, Petrucka P, Eshite S. Effects of undernutrition on survival of human immunodeficiency virus positive children on antiretroviral therapy. Ital J Pediatr. 2018;44(1):1–10.
Health EFMo. Guidelines for paediatric HIV/AIDS care and treatment in Ethiopia. Addis Ababa: HIV/AIDS Prevention and Control Office; 2008.
FMoH. National consolidated guidelines for comprehensive HIV. 2018. https://www.afro.who.int/sites/default/files/201904/National%20Comprehensive%20HIV%20Care%20%20Guideline%202018.pdf
Arage G, Assefa M, Worku T, Semahegn A. Survival rate of HIV-infected children after initiation of the antiretroviral therapy and its predictors in Ethiopia: a facility-based retrospective cohort. SAGE open medicine. 2019;7:2050312119838957.
Bitew S, Mekonen A, Assegid M. Predictors on mortality of human immunodeficiency virus infected children after initiation of antiretroviral treatment in Wolaita zone health facilities, Ethiopia: retrospective cohort study. J AIDS HIV Res. 2017;9(4):89–97.
Collins IJ, Jourdain G, Hansudewechakul R, Kanjanavanit S, Hongsiriwon S, Ngampiyasakul C, et al. Long-term survival of HIV-infected children receiving antiretroviral therapy in Thailand: a 5-year observational cohort study. Clin Infect Dis. 2010;51(12):1449–57.
Sidemo NB, Hebo SH. Nutritional status and its effect on treatment outcome among HIV-infected children receiving first-line antiretroviral therapy in Arba Minch General Hospital and Arba Minch Health Center, Gamo Zone, Southern Ethiopia: retrospective Cohort Study. Nutrition and HIV/AIDS-Implication for Treatment, Prevention and Cure: IntechOpen; 2019.
Slogrove AL, Sohn AH. The global epidemiology of adolescents living with HIV: time for more granular data to improve adolescent health outcomes. Curr Opin HIV AIDS. 2018;13(3):170.
Neilan AM, Karalius B, Patel K, Van Dyke RB, Abzug MJ, Agwu AL, et al. Association of risk of viremia, immunosuppression, serious clinical events, and mortality with increasing age in perinatally human immunodeficiency virus-infected youth. JAMA Pediatr. 2017;171(5):450–60.
Molla M, Kebede F, Kebede T, Haile A. Effects of undernutrition and predictors on the survival status of HIV-positive children after started Antiretroviral Therapy (ART) in Northwest Ethiopia. Int J Pediatr. 2022;2022:1046220.
Kebede F. Severe Acute Malnutrition (SAM) associated mortality rate of children attending HIV/AIDS care in North West Ethiopia, 2009–2019. SAGE Open Med. 2022;10:20503121221081336.
Mekonnen E, Arega M, Belay DM, Birhanu D, Tesfaw T, Ayele H, et al. Time to death and its predictors among under-five children on antiretroviral treatment in public hospitals of Addis Ababa, Addis Ababa, Ethiopia, a retrospective follow up study. PLoS ONE. 2023;18(7):e0288475.
Acharya S, Palkar A, Sayed AP, Setia MS. Retrospective cohort analysis of survival of children living with HIV/AIDS in Mumbai, India. BMJ Open. 2021;11(9):e050534.
Auld AF, Agolory SG, Shiraishi RW, Wabwire-Mangen F, Kwesigabo G, Mulenga M, et al. Antiretroviral therapy enrollment characteristics and outcomes among HIV-infected adolescents and young adults compared with older adults—seven African countries, 2004–2013. Morb Mortal Wkly Rep. 2014;63(47):1097.
Mwiru RS, Spiegelman D, Duggan C, Seage GR III, Semu H, Chalamilla G, et al. Nutritional status and other baseline predictors of mortality among HIV-infected children initiating antiretroviral therapy in Tanzania. J Int Assoc Providers AIDS Care (JIAPAC). 2015;14(2):172–9.
Sanjeeva G, Chebbi PG, Pavithra H, Sahana M, Kumar DS, Hande L. Predictors of mortality and mortality rate in a cohort of children living with HIV from India. Indian J Pediatr. 2016;83(8):765–71.
Ahmed M, Merga H, Jarso H. Predictors of virological treatment failure among adult HIV patients on first-line antiretroviral therapy in Woldia and Dessie hospitals, Northeast Ethiopia: a case-control study. BMC Infect Dis. 2019;19(1):305.
Enderis BO, Hebo SH, Debir MK, Sidamo NB, Shimber MS. Predictors of time to first line antiretroviral treatment failure among adult patients living with HIV in public health facilities of Arba Minch Town, Southern Ethiopia. Ethiop J Health Sci. 2019;29(2):175–86.
Wubneh CA, Belay GM. Mortality and its association with CD4 cell count and hemoglobin level among children on antiretroviral therapy in Ethiopia: a systematic review and meta-analysis. Trop Med Health. 2020;48(1):1–11.
Wamalwa DC, Obimbo EM, Farquhar C, Richardson BA, Mbori-Ngacha DA, Inwani I, et al. Predictors of mortality in HIV-1 infected children on antiretroviral therapy in Kenya: a prospective cohort. BMC Pediatr. 2010;10(1):1–8.
Herd CL, Mellet J, Mashingaidze T, Durandt C, Pepper MS. Consequences of HIV infection in the bone marrow niche. Front Immunol. 2023;14:1163012.
Koller M, Patel K, Chi BH, Wools-Kaloustian K, Dicko F, Chokephaibulkit K, et al. Immunodeficiency in children starting antiretroviral therapy in low-, middle-and high-income countries. J Acquired Immune Def Syndr (1999). 2015;68(1):62.
Nguyen RN, Ton QC, Luong MH, Le LHL. Long-term outcomes and risk factors for mortality in a cohort of HIV-infected children receiving antiretroviral therapy in Vietnam. HIV/AIDS (Auckland, NZ). 2020;12:779–87.
Shabangu P, Beke A, Manda S, Mthethwa N. Predictors of survival among HIV-positive children on ART in Swaziland. African J AIDS Res. 2017;16(4).
Nlend AN, Loussikila A. Predictors of mortality among HIV-infected children receiving highly active antiretroviral therapy. Medecine et maladies infectieuses. 2017;47(1):32–7.
Puoane T, Muzigaba M, Van Wyk B, Sanders D, Sartorius B. The impact of HIV infection and disease stage on the rate of weight gain and duration of refeeding and treatment in severely malnourished children in rural South African hospitals. South African J Child Health. 2017;11(2):86–92.
Alemu YM, Andargie G, Gebeye E. High incidence of tuberculosis in the absence of isoniazid and cotrimoxazole preventive therapy in children living with HIV in northern Ethiopia: a retrospective follow-up study. PLoS ONE. 2016;11(4):e0152941.
Sidamo N, Debere M, Enderis B, Abyu D. Incidence and predictors of mortality among children on anti-retroviral therapy in public health facilities of Arba Minch town, Gamo Gofa Zone, Southern Ethiopia; retrospective cohort study. Clin Mother Child Health. 2017;14:3.
Kasirye R, Baisley K, Munderi P, Grosskurth H. Effect of cotrimoxazole prophylaxis on malaria occurrence in HIV-infected patients on antiretroviral therapy in sub-Saharan Africa. Trop Med Int Health. 2015;20(5):569–80.
Boettiger DC, Muktiarti D, Kurniati N, Truong KH, Saghayam S, Ly PS, et al. Early height and weight changes in children using cotrimoxazole prophylaxis with antiretroviral therapy. Clin Infect Dis. 2016;63(9):1236–44.
Bourke CD, Gough EK, Pimundu G, Shonhai A, Berejena C, Terry L, et al. Cotrimoxazole reduces systemic inflammation in HIV infection by altering the gut microbiome and immune activation. Sci Transl Med. 2019;11(486):eaav0537.
Acknowledgements
We would like to thank Bahir Dar city public health facility leaders, antiretroviral therapy unit coordinators, antiretroviral therapy unit health professionals, and data record room workers for their cooperation and for providing important information.
Funding
The study was not funded by any organization.
Author information
Authors and Affiliations
Contributions
All authors (FM, HM FT, and ZJ) equally contributed in conception of the research problem, initiated the research, wrote the research proposal, conducted the research, made data entry, analysis and interpretation and wrote and reviewed the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical clearance was received from Institutional Review Board (IRB), College of Medicine and health Sciences Bahir Dar University, and letter of permission were received from each health facility before actual data collection. Since the study is entirely relied on retrospective data from patient medical records, the authors are not able to provide informed consents from all the patients whose medical record is used in the study. However, a waiver of consent was officially obtained from institutional review board of College of Medicine and health Sciences Bahir Dar University. The obtained data was kept confidential throughout the study and only used for objective of this study. All of the methods employed in this study were done in compliance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Moga Lencha, F., Mekonnen Workie, H., Tadesse Mequanint, F. et al. Survival status and its predictors among undernourished children on antiretroviral therapy in Bahir Dar city, Northwest Ethiopia, 2010 – 2020, a multicenter retrospective cohort study. BMC Pediatr 24, 290 (2024). https://doi.org/10.1186/s12887-024-04745-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12887-024-04745-8