
Abstract
Background
To investigate the prevalence and risk factors for astigmatism in 7-19-year-old students in **njiang, China.
Methods
A school-based, cross-sectional study was conducted on students who underwent refraction examination in **njiang, China, between May and December 2019. The prevalence of astigmatism was determined. Astigmatism was defined as cylinder power (C) ≤-0.75 D, undefined astigmatism as ≤-1.50 D, and high astigmatism as C ≤-3.00 D. Astigmatism types were: against-the-rule astigmatism (maximum refraction of the main meridian in 180° ± 30°), with-the-rule astigmatism (maximum refraction of the main meridian at 90°±30°), and oblique astigmatism (all other cases).
Results
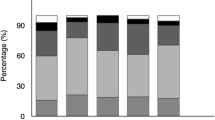
Of the 71,838 students examined (51.0% boys, 7 − 19 years old), 25,945 (36.1%, 95%CI: 35.52−36.68%) had astigmatism and 1267 (1.8%, 95%CI: 1.07−2.53%) had high astigmatism. The prevalence of astigmatism was greater in Han individuals (39.6%) compared with the Hui (34.0%), Kazakh (34.0%), Kyrgyz (32.1%), and Uyghur (26.4%) populations. Among the 25,945 students with astigmatism, 19,947 had with-the-rule astigmatism (76.9%), 3405 had against-the-rule astigmatism (13.1%), and 2593 had oblique astigmatism (10.0%). Multivariable logistic regression analysis showed that ethnicity (Han individuals more susceptible), male gender, age, and refractive errors (myopia and hyperopia) were independently associated with astigmatism, high astigmatism, and with-the-rule astigmatism (all P < 0.05).
Conclusions
The prevalence of astigmatism among children and adolescents in **njiang was 36.1%, including 1.8% of high astigmatism. In this population, astigmatism was mainly of the with-the-rule astigmatism type (76.9%). Han ethnicity, male gender, and myopia or hyperopia were independently associated with a high risk of astigmatism.
Similar content being viewed by others


Background
Astigmatism is a refractive state in which the refractive power of the eye differs at different meridians, creating two focal lines and a minimal diffuse spot [1, 2]. In recent years, the rising annual global prevalence of astigmatism in children and adolescents has become an important clinical and public health concern. Uncorrected astigmatism significantly reduces visual function [1] and can significantly affect visual development in childhood, leading to amblyopia [2]. Previous studies reported a significant correlation between astigmatism and myopia development based on animal models and observations in longitudinal trials involving children [3, 4]. Therefore, early detection and treatment of astigmatism in children and adolescents is particularly important.
Currently, the pathogenesis of astigmatism in children and adolescents is unclear, and genetics, extraocular muscle tone, eyelid pressure, visual feedback, and environmental pollution have been implicated [5]. In addition, studies identified young age, severe refractive error (myopia or hyperopia), maternal smoking during pregnancy [6], eyelid flaps [33]. Other studies have also found correlations between high spherical powers and with-the-rule astigmatism, with against-the-rule astigmatism increasing with decreasing spherical power [34]. Studies in Taiwan and Iran [22, 23] also confirmed the relationship between astigmatic axis position and spherical refractive error. In the above multivariable analysis, we also found that myopic or hyperopic individuals were more likely to develop astigmatism in the against-the-rule and oblique astigmatism than in emmetropia. Further longitudinal studies are needed to evaluate the causal relationship between the variation of the astigmatic axis and the degree of refractive error.
The strengths of this study are as follows. First, the sample size was large, including many regions and representative ethnicities. Secondly, there are relatively few reports on astigmatism prevalence, especially in Western China, a gap closed by this study. In addition, data for several diagnostic criteria were provided in this study, which could be compared with other investigations. However, there were also some limitations in this study. First, non-cycloplegic autorefraction reduces the accuracy of the diopter number. Secondly, it was a cross-sectional study, which cannot determine the causal relationships, e.g., between age and refractive state and between astigmatism prevalence and astigmatic axis, in children and adolescents. Further longitudinal cohort studies are required to accurately and scientifically analyze astigmatism data and provide an effective scientific basis for the prevention and control of astigmatism.
Conclusions
The above large-scale school survey showed that astigmatism was relatively high among children and adolescents in **njiang, China, with astigmatism mainly being with-the-rule astigmatism, which increased with age and education level. The risk of astigmatism, high astigmatism, and with-the-rule astigmatism was increased in the Han ethnicity, males, and myopia or hyperopia cases. The possible causal relationships of refractive error (myopia or hyperopia), ethnicity, astigmatism, and the astigmatic axis must be further confirmed by multicenter longitudinal studies with large sample sizes.
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Abbreviations
- SE:
-
Spherical equivalent refraction
- C:
-
Cylinder power
- D:
-
Diopter
- NA:
-
Not available
- MEPEDS:
-
Multi-Ethnic Pediatric Eye Disease Study
- CI:
-
Confidence Interval
- VIP:
-
Vision in Preschoolers
References
Read SA, Vincent SJ, Collins MJ. The visual and functional impacts of astigmatism and its clinical management. Ophthalmic Physiol Opt. 2014;34:267–94.
Harvey EM. Development and treatment of astigmatism-related amblyopia. Optom Vis Sci. 2009;86:634–9.
Gwiazda J, Grice K, Held R, McLellan J, Thorn F. Astigmatism and the development of myopia in children. Vis Res. 2000;40:1019–26.
Vyas SA, Kee CS. Early Astigmatism can alter Myopia Development in chickens. Invest Ophthalmol Vis Sci. 2021;62:27.
Read SA, Collins MJ, Carney LG. A review of astigmatism and its possible genesis. Clin Exp Optom. 2007;90:5–19.
Huang J, Maguire MG, Ciner E, Kulp MT, Cyert LA, Quinn GE, et al. Risk factors for astigmatism in the Vision in preschoolers Study. Optom Vis Sci. 2014;91:514–21.
Zhuo D, Chen S, Ren X, Wang B, Liu L, **ao L. The prevalence of lower eyelid epiblepharon and its association with refractive errors in Chinese preschool children: a cross-sectional study. BMC Ophthalmol. 2021;21:3.
Huang L, Yang GY, Schmid KL, Chen JY, Li CG, He GH et al. Screen exposure during early life and the increased risk of astigmatism among Preschool children: findings from Longhua Child Cohort Study. Int J Environ Res Public Health. 2020;17.
Fresina M, Benedetti C, Marinelli F, Versura P, Campos EC. Astigmatism in patients with idiopathic congenital nystagmus. Graefes Arch Clin Exp Ophthalmol. 2013;251:1635–9.
Li CG, Yang GY, Schmid KL, Huang LH, He GH, Liu L et al. Associations between Environmental Tobacco Smoke Exposure in Early Life and astigmatism among Chinese Preschool Children. Int J Environ Res Public Health. 2019;16.
Wang J, Cheng QE, Fu X, Zhang R, Meng J, Gu F, et al. Astigmatism in school students of eastern China: prevalence, type, severity and associated risk factors. BMC Ophthalmol. 2020;20:155.
Chuck RS, Jacobs DS, Lee JK, Afshari NA, Vitale S, Shen TT, et al. Refractive errors & refractive surgery Preferred Practice Pattern(R). Ophthalmology. 2018;125:P1–104.
**ao X, Liu WM, Ye YJ, Huang JZ, Luo WQ, Liu HT, et al. Prevalence of high astigmatism in children aged 3 to 6 years in Guangxi, China. Optom Vis Sci. 2014;91:390–6.
Li H, Li SM, Liu LR, Ji YZ, Kang MT, Gan JH, et al. Astigmatism and its components in 12-year-old Chinese children: the Anyang Childhood Eye Study. Br J Ophthalmol. 2019;103:768–74.
Chebil A, Jedidi L, Chaker N, Kort F, Limaiem R, Mghaieth F, et al. Characteristics of Astigmatism in a Population of Tunisian School-Children. Middle East Afr J Ophthalmol. 2015;22:331–4.
Namba H, Sugano A, Murakami T, Utsunomiya H, Nishitsuka K, Ishizawa K, et al. Age-related changes in astigmatism and potential causes. Cornea. 2020;39(Suppl 1):S34–8.
Yang S, Jiang Y, Cui G, Li Y. Age- and gender-related characteristics of astigmatism in a myopic population. Front Med (Lausanne). 2022;9:1011743.
Fan Q, Zhou X, Khor CC, Cheng CY, Goh LK, Sim X, et al. Genome-wide meta-analysis of five Asian cohorts identifies PDGFRA as a susceptibility locus for corneal astigmatism. PLoS Genet. 2011;7:e1002402.
Shah RL, Li Q, Zhao W, Tedja MS, Tideman JWL, Khawaja AP, et al. A genome-wide association study of corneal astigmatism: the CREAM Consortium. Mol Vis. 2018;24:127–42.
Huynh SC, Kifley A, Rose KA, Morgan IG, Mitchell P. Astigmatism in 12-year-old Australian children: comparisons with a 6-year-old population. Invest Ophthalmol Vis Sci. 2007;48:73–82.
Fotouhi A, Hashemi H, Yekta AA, Mohammad K, Khoob MK. Characteristics of astigmatism in a population of schoolchildren, Dezful, Iran. Optom Vis Sci. 2011;88:1054–9.
Shih YF, Hsiao CK, Tung YL, Lin LL, Chen CJ, Hung PT. The prevalence of astigmatism in Taiwan schoolchildren. Optom Vis Sci. 2004;81:94–8.
Hashemi H, Asharlous A, Khabazkhoob M, Yekta A, Emamian MH, Fotouhi A. The profile of astigmatism in 6-12-year-old children in Iran. J Optom. 2021;14:58–68.
Vincent SJ, Collins MJ, Read SA, Carney LG, Yap MK. Corneal changes following near work in myopic anisometropia. Ophthalmic Physiol Opt. 2013;33:15–25.
Fozailoff A, Tarczy-Hornoch K, Cotter S, Wen G, Lin J, Borchert M, et al. Prevalence of astigmatism in 6- to 72-month-old African American and hispanic children: the multi-ethnic Pediatric Eye Disease Study. Ophthalmology. 2011;118:284–93.
Mandalos AT, Peios DK, Mavrakanas TA, Golias VA, Megalou KG, Delidou KA, et al. Prevalence of astigmatism among students in northern Greece. Eur J Ophthalmol. 2002;12:1–4.
He M, Zeng J, Liu Y, Xu J, Pokharel GP, Ellwein LB. Refractive error and visual impairment in urban children in southern China. Invest Ophthalmol Vis Sci. 2004;45:793–9.
Wang M, Cui J, Shan G, Peng X, Pan L, Yan Z, et al. Prevalence and risk factors of refractive error: a cross-sectional study in Han and Yi adults in Yunnan, China. BMC Ophthalmol. 2019;19:33.
Wang M, Gan L, Cui J, Shan G, Chen T, Wang X, et al. Prevalence and risk factors of refractive error in Qinghai, China: a cross-sectional study in Han and Tibetan adults in **ning and surrounding areas. BMC Ophthalmol. 2021;21:260.
Kleinstein RN, Jones LA, Hullett S, Kwon S, Lee RJ, Friedman NE, et al. Refractive error and ethnicity in children. Arch Ophthalmol. 2003;121:1141–7.
Wen G, Tarczy-Hornoch K, McKean-Cowdin R, Cotter SA, Borchert M, Lin J, et al. Prevalence of myopia, hyperopia, and astigmatism in non-hispanic white and Asian children: multi-ethnic pediatric eye disease study. Ophthalmology. 2013;120:2109–16.
Xu Z, Wu Z, Wen Y, Ding M, Sun W, Wang Y, et al. Prevalence of anisometropia and associated factors in Shandong school-aged children. Front Public Health. 2022;10:1072574.
Farbrother JE, Welsby JW, Guggenheim JA. Astigmatic axis is related to the level of spherical ametropia. Optom Vis Sci. 2004;81:18–26.
Sheedy JE, Truong SD, Hayes JR. What are the visual benefits of eyelid squinting? Optom Vis Sci. 2003;80:740–4.
Li T, Zhou X, Chen X, Qi H, Gao Q. Refractive error in Chinese Preschool children: the Shanghai Study. Eye Contact Lens. 2019;45:182–7.
Wang X, Liu D, Feng R, Zhao H, Wang Q. Refractive error among urban preschool children in Xuzhou, China. Int J Clin Exp Pathol. 2014;7:8922–8.
Fan DS, Lai C, Lau HH, Cheung EY, Lam DS. Change in vision disorders among Hong Kong preschoolers in 10 years. Clin Exp Ophthalmol. 2011;39:398–403.
Harrington SC, Stack J, Saunders K, O’Dwyer V. Refractive error and visual impairment in Ireland schoolchildren. Br J Ophthalmol. 2019;103:1112–8.
Mayro EL, Hark LA, Shiuey E, Pond M, Siam L, Hill-Bennett T, et al. Prevalence of uncorrected refractive errors among school-age children in the School District of Philadelphia. J AAPOS. 2018;22:214–7. e2.
Norouzirad R, Hashemi H, Yekta A, Nirouzad F, Ostadimoghaddam H, Yazdani N, et al. The prevalence of refractive errors in 6- to 15-year-old schoolchildren in Dezful, Iran. J Curr Ophthalmol. 2015;27:51–5.
Wajuihian SO. Characteristics of astigmatism in Black South African high school children. Afr Health Sci. 2017;17:1160–71.
Soler M, Anera RG, Castro JJ, Jimenez R, Jimenez JR. Prevalence of refractive errors in children in Equatorial Guinea. Optom Vis Sci. 2015;92:53–8.
Acknowledgements
We thank the **njiang Uyghur Autonomous Region Primary and Secondary School Health Care Guidance Center for personnel support. We thank International Science Editing (http://www.internationalscienceediting.com) for editing this manuscript.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Yan Wang and **gyu Mu contributed to the design and conduct of the study, data collection and management, and data interpretation, and wrote the whole paper. Yunxian Gao and Yong Zhao contributed to data interpretation and critically revised the manuscript. Zhen Wang performed the statistical analysis and critically revised the manuscript. Wei Gong guided and participated in data statistical analysis and interpretation. Yining Yang contributed to the design and conduct of the study, and data collection, and critically revised the manuscript. **aolong Li, Han Qin, Batima·Mulati contributed to the design and conduct of the study, data collection, and critically revised the manuscript. All authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study passed the ethical review of the Traditional Chinese Medicine Hospital of **njiang Uyghur Autonomous Region (Ethics approval No 2019XE0151). All participants and their parents or guardians provided signed informed consent. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, Y., Mu, J., Yang, Y. et al. Prevalence and risk factors for astigmatism in 7 to 19-year-old students in **njiang, China: a cross-sectional study. BMC Ophthalmol 24, 116 (2024). https://doi.org/10.1186/s12886-024-03382-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12886-024-03382-0