
Abstract
Background
Primary tumor removal by cytoreductive nephrectomy in synchronous metastatic renal cell carcinoma patients has been investigated in the context of various treatment regimens. Two randomized controlled trials investigated the role and timing of cytoreductive nephrectomy in the era of targeted therapy and demonstrated that upfront nephrectomy should no longer be performed when patients require systemic therapy. Superiority of checkpoint immunotherapy agents has led to a paradigm change from targeted therapies to immunotherapy-based first-line treatment in patients with primary metastatic disease; thus, deferred cytoreductive nephrectomy needs to be verified in the immunotherapy setting. Furthermore, a need exists for personalizing treatment choices for the individual patient to avoid unnecessary overtreatment.
Methods/design
To explore the impact of cytoreductive nephrectomy in this patient group receiving checkpoint immunotherapy, we initiated a randomized, controlled trial comparing deferred cytoreductive nephrectomy with no surgery. The trial integrates a comprehensive translational research program with specimen sampling for biomarker analysis.
Discussion
The trial aims to show that deferred cytoreductive nephrectomy improves overall survival in patients with synchronous metastatic renal cell carcinoma, and furthermore, to identify relevant biomarkers for personalized renal cancer management.
Trial registration
ClinicalTrials.gov NCT03977571 June 6, 2019.
Similar content being viewed by others


Background
Cytoreductive nephrectomy in synchronous metastatic renal cell carcinoma patients
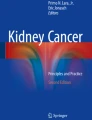
Around 20% of patients with Renal Cell Carcinoma (RCC) have synchronous metastatic disease at diagnosis, i.e. are diagnosed with a primary kidney tumor and metastases simultaneously. Patients presenting with metastatic disease at primary diagnosis have the worst prognosis due to underlying aggressive tumor biology and are often clinically challenging due to symptoms from either the primary tumor or the metastases [1, The deferred CN approach enables all patients to be treated with systemic therapy, restricting only patients benefitting from the therapy to receive surgery. However, current data are derived during the TKI era and only point towards a survival benefit for CN in the subgroup patients with a maximum of 3 IMDC risk factors. In this trial we aim to describe the effect of deferred CN in a contemporary patient population treated with IO-IO or TKI-IO therapy. Furthermore, the genomic landscape of the tumor, tumor microenvironment composition, peripheral immune subsets and the microbiome may be of great importance to the efficacy of treatment and to select candidates for surgery. To facilitate this, we will collect patient specimens longitudinally during the trial. The aim of this study is to conduct an open, randomized, multicenter comparison trial, evaluating the effect of deferred CN compared with no surgery, following initial nivolumab combined with ipilimumab or a TKI-IO-combination, in synchronous mRCC patients with ≤ 3 IMDC risk features and absence of progressive disease at metastatic sites. The primary endpoint is overall survival (OS) compared between synchronous mRCC patients receiving a deferred CN and patients not receiving surgery. Progression-free survival (PFS) Time to subsequent systemic therapy (TST) Objective response rate (ORR) and disease control rate (DCR) per RECIST 1.1 Surgery complications and 30-day mortality (Clavien-Dindo) Fractional percentage of tumor volume to survival outcome Percentage of pathological response to survival outcome Frequency of patients meeting the randomization criteria OS, PFS, TST, and ORR in patients not meeting the randomization criteria and in patients with clear cell and non-clear cell histology Immune cells, tumor cells, ctDNA, and the microbiome will be analyzed and compared with OS, PFS, TST, ORR, pathological response, DCR, and safety.<div class="NodiCopyInline">Immune cells, tumor cells, ctDNA, and the microbiome will be analyzed and compared with OS, PFS, TST, ORR, pathological response, DCR, and safety.</div> NORDIC-SUN is a multicenter open label randomized trial investigating the impact of CN in synchronous mRCC following 3 or 6 months of immunotherapy-based first-line treatment. Patients will be stratified by 1:1 allocation into Arm A (deferred CN) and Arm B (no surgery) based on criteria of surgical resectability, ≤ 3 IMDC risk features, and absence of progressive disease at metastatic sites. The remaining patients not eligible for randomization, referred to as Arm C, will be described, but are not a part of the main analysis. The study design is outlined in Fig. 1. Study design. Arm A: Deferred CN followed by nivolumab or TKI-IO therapy. Arm B: No surgery, nivolumab or TKI-IO therapy. Arm C: Patients not eligible for randomization into Arm A or B. CN: Cytoreductive Nephrectomy; IO: Immunotherapy; mRCC: metastatic Renal Cell Carcinoma; Nivo: Nivolumab; TKI: Tyrosine Kinase Inhibitor. Generated with BioRender.com The trial will include 400 mRCC patients with synchronous disease. Participating centers will be University Hospitals in Denmark and the Nordic Countries, and possibly a few European sites. The coordinating center, which includes a data manager, is placed at Aarhus University Hospital, Denmark, managing the trial in close collaboration with the PI and the steering committee. Collaborating centers report to the coordinating center.
Inclusion criteria:
Synchronous mRCC proven with a core needle biopsy (all histological subtypes are acceptable) and measurable as per RECIST v 1.1. Age > 18. Patients referred to standard immunotherapy-based first-line treatment according to the recommendations by the European Medicines Agency and the national health authorities. Both IO-IO and TKI-IO are considered as a standard treatment. Females not pregnant. Fertile patients must use effective means of contraception. Life expectancy > 4 months. Karnofsky Performance status > 70. Laboratory values acceptable for IO-IO or TKI-IO treatment. Able to speak and understand native language.
Exclusion criteria:
Prior systemic treatment for mRCC. Other cancer diagnosis within three years (except in situ basal cell carcinoma and radically treated localized prostate cancer with undetectable prostate-specific antigen). Major surgical procedure, open surgical biopsy, or significant traumatic injury within 14 days prior to enrollment, or non-healed lesion. Clinically significant (i.e. active) cardiovascular disease for example cerebrovascular accidents (< 6 months before inclusion), myocardial infarction (< 6 months before inclusion), unstable angina, New York Heart Association grade II or greater congestive heart failure. No symptomatic brain metastasis requiring systemic corticosteroids (> 10 mg daily prednisone equivalent). Recent (within the 30 days prior to inclusion) treatment with another investigational drug. Any active or recent history of a known or suspected autoimmune disease or recent history of a condition that requires systemic corticosteroids (> 10 mg daily prednisone equivalent) or other immunosuppressive medications, excluding inhaled steroids and local cutaneous steroids. Subjects with vitiligo or type I diabetes mellitus or residual hypothyroidism due to autoimmune thyroiditis only requiring hormone replacement, psoriasis not requiring systemic treatment are permitted to enroll. Known hypersensitivity to monoclonal antibodies. Known history of testing positive for human immunodeficiency virus or known acquired immunodeficiency syndrome (AIDS). Any positive test for hepatitis B- or C-Virus, indicating acute or chronic infection. Patients are randomized 1:1 into the two treatment arms: ARM A: 3 months of IO-IO or TKI-IO followed by deferred CN, followed by maintenance nivolumab or a TKI-IO-combination. ARM B: No surgery, 3 months of IO-IO or TKI-IO followed by maintenance nivolumab or a TKI-IO-combination. Patient eligible for surgery is randomized by a local project nurse using a computer-generated allocation sequence and is not blinded due to the circumstances; surgery versus no surgery. In Arm A patients are treated according to standard protocol with first-line IO-IO or TKI-IO combination treatment followed by a CN. In Arm B patients are receiving standard IO-IO or a TKI-IO combination first-line treatment (Fig. 1). Patients will be stratified by treatment choice (IO-IO vs TKI-IO). The remaining patients, referred to as Arm C, not eligible for randomization due to > 3 IMDC risk factors, progressive disease at metastatic sites, poor performance or a non resectable tumor will undergo three months of nivolumab or a TKI-IO combination and then be evaluated again after another 3 months. If still not eligible for randomization, the patients will continue nivolumab maintenance and TKI-IO combination and be followed on survival. Patients included in the NORDIC-SUN trial are stratified according to institution, treatment choice, number of IMDC risk factors, and combined elevated neutrophil–lymphocyte ratio and hyponatremia. All patients will receive systemic IO-IO or TKI-IO immediately after inclusion. After three months of nivolumab combined with ipilimumab or a TKI-IO combination, the patient will be discussed for resectability at the multidisciplinary meeting (MDT), whether the patient is eligible for CN. Patients with ≤ 3 IMDC risk factors and deemed suitable for CN including an acceptable performance status and absence of progression at metastatic sites will then undergo randomization. Patients deemed not suitable for surgery or have > 3 IMDC risk features at the 3 month evaluation continue systemic therapy for 3 months, followed by a 2nd evaluation 6 months after inclusion. Patients with ≤ 3 IMDC risk factors and deemed suitable for CN at 2nd evaluation will then undergo randomization. Patients deemed not suitable for surgery or have > 3 IMDC risk features at the 6 month evaluation continue systemic therapy (Arm C). Nivolumab may continue until unacceptable toxicity or total treatment length of two years from inclusion. Allocating patients to Arm C promotes participant retention, securing outcome data of patients not randomized. Inclusion began right before the Corona epidemic set in. The study was therefore paused and has now been re-initiated in January 2023. Presently, 40 patients are included (10% accrual) and the study will continue until full accrual (400 patients) have been reached in 2026, with a follow-up period of additional three years. The primary endpoint is expected to be reached and ready for publication in 2029. All patients will have blood samples collected at baseline, week 12, and week 24. Rectal swabs are taken as a proxy for stool samples at baseline and week 12. At baseline, a fresh frozen tumor core biopsy is seeked to be obtained and for Arm A biopsies from the nephrectomy specimen will be fixed and stored according to the Danish Cancer Biobank for future analyses. All samples will be anonymously labeled with a pseudo patient study identifier. See Fig. 1. ctDNA will be detected and measured in plasma samples using sequence-based methods. Bacterial species will be identified using 16 s ribosomal RNA gene sequencing and linked to response data to determine the role of the colonic microflora in immunotherapy response. The beta chain gene repertoire of T cell receptors will be sequenced to determine T cell clone dynamics and composition. Whole exome and genome sequencing will be applied to explore and validate predictive markers of treatment response. RNA-sequencing will be performed to investigate the association between molecular subtypes, immune subtypes, and gene expression signatures of cellular processes and treatment response. Sample size calculations are based on simulated survival data and cox regression. With the assumption that 60% of patients meet the randomization criteria, and to demonstrate a 50% improvement in OS, with a 3-year follow-up, a sample size of 400 patients is needed to achieve 80% power at a 5% significance level. Hence, 400 patients will be included in NORDIC-SUN with the estimation of 240 patients (60%) being randomized (120 in each arm) and 168 occurred deaths upon reach of appropriate power. Difference in primary and secondary endpoints between the two treatment arms will be tested with a two-sided log rank test at the 5% alpha level. Statistical methods including Kaplan–Meier and cox proportional hazard regression will be performed adjusted and unadjusted for the stratification factor. Furthermore, linear regression, logistic regression, and machine learning approaches (e.g. Random Forest, Neural Networks, and Gradient Boost models) will be applied in an exploratory manner to identify any correlation between molecular measures and clinical outcome parameters. Blood, tissue, and fecal swab samples collected during the trial will be stored in the Bio- and Genome Bank, Denmark. Residual blood and tissue biopsies as well as clinical and sequencing data will be transferred to the Renal Cancer Research Biobank at Aarhus University Hospital for future research, where it will be saved and stored in a pseudonymized form. Any protocol modifications will be reported timely to the relevant authorities, investigators/centers, and if necessary, patients. No protocol modification is effected before the necessary approval have been given. Results from the NORDIC-SUN trial will be published in peer-reviewed scientific journals. For synchronous mRCC, the question whether the primary tumor responds just as well as the remaining systemic disease to combinational IO-IO or TKI-IO treatment remains. Moreover, the timing of surgery versus systemic treatment is still debated. The impact of debulking the primary tumor in patients with synchronous mRCC has been evaluated in two prospective randomized studies in the TKI era. The SURTIME trial questioned the timing of CN, upfront or deferred, and reported that unnecessary surgery could be avoided through pre-treatment with sunitinib to identify patients inherently resistant to systemic targeted therapy [13]. The CARMENA trial tested the benefit of initial nephrectomy and showed no benefit of upfront nephrectomy over sunitinib alone [12]. As 20% of the patients in the sunitinib alone arm in CARMENA had a deferred CN, both SURTIME and CARMENA can be regarded as proof-of-concept trials demonstrating that patients who require systemic therapy should receive drug therapy first with the option to be offered deferred CN after disease consolidation. Now that the preferred treatment for mRCC has changed to favoring doublet IO or TKI-IO, the role of deferred CN in this setting is yet to be determined. In the presented randomized clinical trial, the NORDIC-SUN trial, the role of surgery will be determined in both poor and intermediate risk patients. It is expected that the initial first-line of IO-IO or TKI-IO treatment will reduce the IMDC risk score for some patients, thereby making more patients eligible for surgery. Similarly to the NORDIC-SUN trial, the Prospective Randomized Open Blinded Endpoint (PROBE) trial (NCT04510597) has been initiated to evaluate if CN provides an overall survival benefit in patients responding to first-line systemic therapy (objective response or stable disease) [22]. The PROBE trial tests CN and systemic therapy (IO-IO or TKI-IO) against systemic therapy alone. Enrollment started in 2021 and the study is expected to be completed in 2033. Comparison of the results from these two trials would be warranted. We hypothesize that deferred CN after initial immunotherapy-based first-line treatment will improve OS in patients with synchronous metastatic RCC and ≤ 3 IMDC risk features. Furthermore, this study will identify potential predictive and prognostic biomarkers based on immune subsets in blood and tumor, gene expression, tumor mutational burden, overall genetic alterations, ctDNA, and gut microbiome. Our findings aim at hel** clinicians to stratify patients more accurately for surgery and/or immunotherapy-based combinational treatment. Patients with de novo, synchronous metastatic disease are clinically challenging. The NORDIC-SUN trial is a randomized clinical trial evaluating the effect of deferred CN during first-line immunotherapy doublet or TKI-IO treatment only in synchronous metastatic RCC patients. The trial will identify potential predictive and prognostic biomarkers, thereby seeking to personalize the treatment for each patient.Methods/design
Rationale
Objectives and endpoints
Primary endpoint
Secondary endpoints include
Exploratory endpoints
Study design

Study population
Detailed enrollment criteria are listed below
Randomization and masking
Study procedure
Status
Sample collection
Experimental plans
Statistical analyses
Sample size determination
Data analysis
Biobank
Dissemination
Discussion
Conclusion
Availability of data and materials
Future data from the trial will be available after publication of trial results from the corresponding author on reasonable request.
Abbreviations
- CN:
-
Cytoreductive nephrectomy
- ctDNA:
-
Circulating tumor DNA
- DCR:
-
Disease control rate
- IMDC:
-
International metastatic renal cell carcinoma database consortium
- IO:
-
Immunotherapy
- PFS:
-
Progression free survival
- RCC:
-
Renal cell carcinoma
- mRCC:
-
Metastatic renal cell carcinoma
- Nivo:
-
Nivolumab
- ORR:
-
Objective response rate
- OS:
-
Overall survival
- TKI:
-
Tyrosine kinase inhibitor
- TST:
-
Time to subsequent systemic therapy
References
Kammerer-Jacquet SF, Brunot A, Pladys A, Bouzille G, Dagher J, Medane S, et al. Synchronous metastatic clear-cell renal cell carcinoma: a distinct morphologic, immunohistochemical, and molecular phenotype. Clin Genitourin Cancer. 2017;15(1):e1–7.
Donskov F, **e W, Overby A, Wells JC, Fraccon AP, Sacco CS, et al. Synchronous versus metachronous metastatic disease: impact of time to metastasis on patient outcome-results from the international metastatic renal cell carcinoma database consortium. Eur Urol Oncol. 2020;3(4):530–9.
Heng DY, **e W, Regan MM, Harshman LC, Bjarnason GA, Vaishampayan UN, et al. External validation and comparison with other models of the International metastatic renal-cell carcinoma database consortium prognostic model: a population-based study. Lancet Oncol. 2013;14(2):141–8.
Choueiri TK, Motzer RJ. Systemic therapy for metastatic renal-cell carcinoma. N Engl J Med. 2017;376(4):354–66.
Bex A, Albiges L, Ljungberg B, Bensalah K, Dabestani S, Giles RH, et al. Updated European association of urology guidelines for cytoreductive nephrectomy in patients with synchronous metastatic clear-cell renal cell carcinoma. Eur Urol. 2018;74(6):805–9.
Heng DY, Wells JC, Rini BI, Beuselinck B, Lee JL, Knox JJ, et al. Cytoreductive nephrectomy in patients with synchronous metastases from renal cell carcinoma: results from the International metastatic renal cell carcinoma database consortium. Eur Urol. 2014;66(4):704–10.
Massari F, Di Nunno V, Gatto L, Santoni M, Schiavina R, Cosmai L, et al. Should CARMENA really change our attitude towards cytoreductive nephrectomy in metastatic renal cell carcinoma? A systematic review and meta-analysis evaluating cytoreductive nephrectomy in the era of targeted therapy. Target Oncol. 2018;13(6):705–14.
Motzer RJ, Russo P. Cytoreductive nephrectomy - patient selection is key. N Engl J Med. 2018;379(5):481–2.
Guo L, Bi X, Li Y, Wen L, Zhang W, Jiang W, et al. Characteristics, dynamic changes, and prognostic significance of TCR repertoire profiling in patients with renal cell carcinoma. J Pathol. 2020;251(1):26–37.
Routy B, Gopalakrishnan V, Daillere R, Zitvogel L, Wargo JA, Kroemer G. The gut microbiota influences anticancer immunosurveillance and general health. Nat Rev Clin Oncol. 2018;15(6):382–96.
Grimm MO, Oya M, Choueiri TK, Motzer RJ, Schmidinger M, Quinn DI, et al. Impact of prior cytoreductive nephrectomy on efficacy in patients with synchronous metastatic renal cell carcinoma treated with Avelumab plus Axitinib or Sunitinib: post hoc analysis from the JAVELIN renal 101 phase 3 trial. Eur Urol. 2024;85(1):8–12.
Mejean A, Ravaud A, Thezenas S, Colas S, Beauval JB, Bensalah K, et al. Sunitinib alone or after nephrectomy in metastatic renal-cell carcinoma. N Engl J Med. 2018;379(5):417–27.
Bex A, Mulders P, Jewett M, Wagstaff J, van Thienen JV, Blank CU, et al. Comparison of immediate vs deferred cytoreductive nephrectomy in patients with synchronous metastatic renal cell carcinoma receiving sunitinib: the SURTIME randomized clinical trial. JAMA Oncol. 2019;5(2):164–70.
Donskov F, Michaelson MD, Puzanov I, Davis MP, Bjarnason GA, Motzer RJ, et al. Sunitinib-associated hypertension and neutropenia as efficacy biomarkers in metastatic renal cell carcinoma patients. Br J Cancer. 2015;113(11):1571–80.
Soerensen AV, Geertsen PF, Christensen IJ, Hermann GG, Jensen NV, Fode K, et al. A five-factor biomarker profile obtained week 4–12 of treatment for improved prognostication in metastatic renal cell carcinoma: results from DARENCA study 2. Acta Oncol. 2016;55(3):341–8.
Singla N, Hutchinson RC, Ghandour RA, Freifeld Y, Fang D, Sagalowsky AI, et al. Improved survival after cytoreductive nephrectomy for metastatic renal cell carcinoma in the contemporary immunotherapy era: An analysis of the National Cancer Database. Urol Oncol. 2020;38(6):604 e9-e17.
Motzer RJ, Tannir NM, McDermott DF, Aren Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus Ipilimumab versus Sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277–90.
Lyskjaer I, Iisager L, Axelsen CT, Nielsen TK, Dyrskjot L, Fristrup N. Management of renal cell carcinoma: promising biomarkers and the challenges to reach the clinic. Clin Cancer Res. 2024;30(4):663-72.
Corcoran RB, Chabner BA. Application of cell-free DNA analysis to cancer treatment. N Engl J Med. 2018;379(18):1754–65.
Geertsen L, Koldby KM, Thomassen M, Kruse T, Lund L. Circulating tumor DNA in patients with renal cell carcinoma a systematic review of the literature. Eur Urol Open Sci. 2022;37:27–35.
Turajlic S, Xu H, Litchfield K, Rowan A, Chambers T, Lopez JI, et al. Tracking cancer evolution reveals constrained routes to metastases: TRACERx renal. Cell. 2018;173(3):581-94 e12.
Bell H, Cotta BH, Salami SS, Kim H, Vaishampayan U. “PROBE”ing the role of cytoreductive nephrectomy in advanced renal cancer. Kidney Cancer J. 2022;6(1):3–9.
Acknowledgements
We thank the Bio- and Genome Bank Denmark for handling the sample collection. We are grateful for the patients participating and donating invaluable samples for research.
Funding
The trial and analysis are supported by The Danish Health Authority (05–0400-48) after international peer-review. While molecular analyses and salaries are supported by the Lundbeck Foundation (R413-2022–606), the Danish Cancer Society (R352-A20516), DCCC Danish Research Centre for circulating tumor DNA guided treatment (20230426_2), and the Independent Research Fund Denmark (2100-00017B).
Lundbeck Foundation,R413-2022-606,Kræftens Bekæmpelse,R352-A20516,DCCC Danish Research Centre for circulating tumor DNA guided treatment,20230426_2,Danmarks Frie Forskningsfond,2100-00017B,The Danish Health Authority,05-0400-48
Author information
Authors and Affiliations
Contributions
The authors confirm contribution to the paper as follows: FD, NF, BL, AB, LL study conception and design, FD, NF drafted the protocol, IL, LI, JA, NF wrote the manuscript. All authors read and accepted the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study is conducted according to the guidelines of the Declaration of Helsinki and approved by the Danish National Center for Ethics (1–10-72–158-19, version 2.0 approved 14–09-2023 l). The patient should be informed about the protocol prior to the diagnostic (routine) biopsy in order to have the fresh baseline biopsy to coincide with the diagnostic (routine) biopsy, thereby avoiding delay in systemic therapy initiation. It is the responsibility of the investigator, or a person designated by the investigator (if acceptable by local regulations), to obtain written informed consent from each patient participating in this study, after adequate explanation of the aims, methods, anticipated benefits, and potential hazards of the study. Patient information is collected and maintained in an Aarhus University controlled REDCap database by the project nurse and the responsible data manager.
Consent for publication
Not applicable.
Competing interests
NF has performed consultancy for Pfizer, Eisai, MSD, BMS, and has received speaker honoraria from AstraZeneca, BMS, MSD. BL: Company speaker: Novartis, IPSEN, BMS; Company consultant: Janssen, Ipsen, MSD; Trial participation: Jenssen—Astellas – Medivation. AB: grants from Pfizer and steering committee membership of Roche and BMS, consultancy for IPSEN. The other authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Checklist for SPIRIT guidelines.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Iisager, L., Ahrenfeldt, J., Donskov, F. et al. Multicenter randomized trial of deferred cytoreductive nephrectomy in synchronous metastatic renal cell carcinoma receiving checkpoint inhibitors: the NORDIC-SUN-Trial. BMC Cancer 24, 260 (2024). https://doi.org/10.1186/s12885-024-11987-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-024-11987-3