
Abstract
Background
Tuberculous meningitis (TBM), complicated with cerebral venous thrombosis (CVT), has been sparsely reported and needs to be investigated further.
Methods
Among those with tuberculous meningitis in Haihe Hospital, Tian** University, 3 patients with venous sinus thrombosis were identified retrospectively. “Tuberculous meningitis” and “cerebral venous thrombosis” were used as keywords, and the retrieved literature was summarized and analyzed. Our data were combined with previously reported case data to describe this new condition.
Results
Among 28 patients with a median onset age of 31 years for TBM, 17 were females. The manifestations were fever, headache, and seizure. Magnetic resonance imaging (MRI) venography showed that the most common site of venous sinus thrombosis involved superior sagittal sinus, left transverse sinus, left sigmoid sinus, cavernous sinus, and straight sinus. The abnormalities found on MRI include hydrocephalus, exudates, hemorrhage, meningeal enhancement, infarction, and tuberculoma. In the acute phase, all patients received standard anti-TB treatment, and 14/28 patients received anticoagulant treatment. The mortality rate of these patients was 17.9%, and 21/28 (75%) became functionally independent.
Conclusions
CVT is one of the rare complications of TMB and must be considered a differential diagnosis in patients with TBM who show poor clinical features and/or develop new neurological signs.
Similar content being viewed by others


Background
Central nervous system tuberculosis (CNS TB) is a major cause of morbidity and mortality in develo** countries and may present as tubercular meningitis (TBM), meningoencephalitis, tuberculomas, and abscesses. TBM manifests as critical and serious complications. Cerebral venous thrombosis (CVT) is characterized by a thrombus in the dural venous sinuses. The association of TBM with CVT is rare. However, most of the previous studies were case reports. Herein, we analyzed the clinical and radiological features, treatment responses, and outcomes of the patients with tuberculous meningitis (TBM) complicated with cerebral venous thrombosis (CVT). Subsequently, we combined our data with those reported previously to outline the features of this rare co-morbidity.
Methods
Current case series
This study was approved by the Ethics Committee of Haihe Hospital, Tian** University. Among the patients with tuberculous meningitis hospitalized from January 2018–May 2021, 3 were complicated with venous sinus thrombosis. These 3 patients were diagnosed with tuberculous meningitis according to the consensus scoring system of The Lancet [evidence of positive culture for Mycobacterium tuberculosis in the CSF(cerebrospinal fluid) samples). All 3 patients underwent head MRV( magnetic resonance venography) examination, which indicated clear diagnosis of venous sinus thrombosis. All patients were followed up and had good prognosis.
Literature review
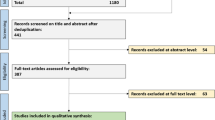
To further clarify the clinical features of patients with TBM and cerebral sinus venous thrombosis, we searched PubMed (Medline) through January 14, 2022, for articles published in English using the search string (“cerebral venous and sinus thrombosis, cerebral venous thrombosis” [MeSH Terms] OR “cortical vein thrombosis” OR “intracranial thrombosis”) AND (“Tubercular Meningitis ” [MeSH Terms]). We also searched the references for related published articles. The retrieved articles were reviewed to identify cases with TBM and cerebral sinus venous thrombosis.
After combining our data with those from previously reported cases, the clinical and radiological features, treatment, and outcomes of the patients with TBM and cerebral sinus venous thrombosis were analyzed further to characterize the new condition.
Results
Results from the present case series study
Case #1
A 34-year-old female was admitted because of fever and headache. She got pregnant with assisted reproductive technology 6 months ago and delivered a dead baby under the protection of the perineum 8 days before admission. The general physical examination was unremarkable, and the neurological examination was normal. CSF test showed that gene X-pert was positive for M. tuberculosis, which was confirmed by metagenomics next-generation sequencing (mNGS). Brain magnetic resonance imaging (MRI) of the brain showed an abnormal signal shadow of the bilateral parietal lobe. MRI venography showed partial visualization with thrombosis of the straight sinus, suggesting CVT (Fig. 1). She was treated with anti-tuberculosis drugs and low-molecular-weight heparin. The patient was treated in the hospital for 2 months and continued to take oral warfarin for 6 months, and ingested anti-TB drugs regularly for 14 months. After completing the regimen, the patient was followed up for 3 months; the last modified Rankin score (mRS) of the patient was 0.

Radiographic findings of the patient in case 1. A: MRV shows partial visualization with thrombosis of the straight sinus; B: T1-weighted MRI of the brain with contrast images showing enhancement of multiple nodules in the temporal and occipital lobes; C, D, and E: MRI revealed infarction of bilateral frontoparietal temporal and left occipital lobes
Case #2
A 29-year-old female was admitted with fever, headache, vomiting, and diplopia. She had a history of induced abortion 2 months before admission. mNGS detected M. tuberculosis in CSF samples. MRI of the brain showed a focal infection in the left temporoparietal lobe with enhanced manifestations. MRI venography showed thrombosis of the left transverse sinus and sigmoid sinus (Fig. 2). She received anti-TB drugs and low molecular weight heparin for 2 months. After discharge, she continued to take rivalsaban orally for 6 months and anti-TB drugs regularly for 14 months. After completion of the medication, the patient was followed up for 3 months, and her last mRS was 0.

Radiographic findings of the patient in case 2. A: Brain plain MRI FLAIR sequence shows multiple high-signal intensity patches in bilateral frontal parietal cortex and subcortical white matter. B: MRV shows a locally narrowed right sigmoid sinus, while the left transverse sinus and sigmoid sinus are not shown. C and D: Post-contrast MRI T1WI shows filling defects in the right sigmoid sinus, left transverse sinus, and sigmoid sinus. E: After 6 months, the re-examination image shows that the right sigmoid sinus is normal, and the filling defect of the left transverse sinus and sigmoid sinus was better than before
Case #3
A 30-year-old female was admitted with fever, headache, and vomiting. She was healthy in the past. The general physical examination and the nervous system were normal. The mNGS of CSF showed the presence of M. tuberculosis. Brain MRI indicated multiple tuberculomas in the brain. MRI venography showed thrombosis of the left transverse sinus and sigmoid sinus (Fig. 3). She was treated with anti-TB drugs and low-molecular-weight heparin for 2 months. After discharge, she continued oral administration of anti-TB drugs. The prognosis was satisfactory, and the patient was followed up for 6 months after discharge; the last mRS was 0.

Radiographic findings of the patient in case 3. A: Brain plain MRI DWI sequence shows high-signal intensity nodules in the right cerebellum. B, C, and D: Post-contrast MRI T1WI (axial and coronal) shows patchy enhancement around the right cerebellum near the right sigmoid sinus area and enhancement of pia mater of the basal cistern around the midbrain. E and F: Post-contrast MRI T1WI shows filling defects in the left transverse sinus and sigmoid sinus
The characteristics of the patients are summarized in Table 1.
Results from a literature review and pooled data analysis
The initial literature search yielded 11 published reports. The reports and the references were reviewed to identify any related published articles. A total of 25 patients with TBM and cerebral sinus venous thrombosis were identified. After pooling the data, the characteristics of the previously reported and our 3 patients are summarized (Table 2).
The median onset age of the patients was 31 (range: 1–61) years, and 17 were females. The manifestations were mainly fever (85.7%), headache (82.1%), and seizure (64.3%). According to the magnetic resonance imaging venography (MRV) findings, the most common sites of venous sinus thrombosis were superior sagittal sinus (60.7%), left transverse sinus (39.3%), and left sigmoid sinus (32.1%). The abnormalities detected on MRI were hydrocephalus (42.9%), exudates (39.3%), hemorrhage (21.4%), meningeal enhancement (21.4%), infarction (14.3%), and tuberculoma (14.3%). In the acute phase, all patients received standard anti-TB treatment, while 14/28 (50.0%) of patients received anticoagulant treatment, and 1/28 received oral aspirin. The mortality rate of these patients was 17.9%. Subsequently, 21/28 (75%) became functionally independent [the last modified Rankin scale (mRS) ≤ 2].
Discussion
Venous sinus or cerebral veins is a specific anatomical location of venous thrombosis [1] and a particular type of stroke, which commonly affects young adults, with 75% of events occurring in women. The clinical manifestations of CVT are highly variable. The symptoms and signs of CVT can be grouped into presenting syndromes; the most frequent types are isolated intracranial hypertension syndrome (manifesting as headache, vomiting, papilledema, or visual problems), focal neurological deficits (hemiparesis, dysphasia, cranial nerve deficits, and altered sensorium), and encephalopathy (with multifocal signs and altered mental status [2]. The less frequent presentation is cavernous sinus syndrome or syndromes of multiple palsies of the lower cranial nerves. The risk factors associated with CVT include oral contraceptives, pregnancy, head injury, neurological procedures, lumbar puncture, infections, otitis and mastoiditis, and meningitis [2]. Typically, these risk factors are associated with the thrombogenic triad of Virchow, including vessel wall injury, blood stasis, and hypercoagulability [3].
Vascular endothelial injury caused by infections (bacterial, TB, fungal), especially meningitis, is one of the risk factors of CVT [4], and a few studies have reported TBM complicated with CVT; however, its true prevalence is uncertain. Tuberculous meningitis often occurs in an environment with insufficient resources. Also, since tuberculous meningitis and CVT have the same clinical manifestations (such as headache, epilepsy, and limb paralysis caused by cerebral infarction), not all TBM patients undergo MRI or CT venous examination. Low detection rates are likely to contribute to low reported prevalence rates of this complication. In the current study, TBM was the main factor of CVT in these patients [5,6,7,8,9,10,11,12]. In addition, one patient was complicated with spondylitis with epidural abscess, one patient used oral contraceptives [13], and one case was combined with coronavirus disease-19 (COVID-19) [14]. Herein, 2/3 patients were sick after artificial abortion, and one was pregnant by assisted reproductive technology.
The current study demonstrated diverse and nonspecific clinical manifestations of TBM patients complicated with CVT, such as fever, headache, and epilepsy. Seizures are common manifestations in patients with TBM or CVT, especially in the acute phase of the disease. Previous studies have shown that seizures occur in 34% of patients with TBM, and the incidence of seizures in CVT patients is 44.3% [15]. In this study, adult cases had a high incidence of epilepsy (64.3%), suggesting that when adult patients with TBM have seizures, we should be alert to whether the patients also present CVT concurrently.
The most common sites of CVT complicated with TBM were superior sagittal sinus (65.4%), left transverse sinus (34.6%), and left sigmoid sinus (26.9%). These findings were similar to those of International Study of Cerebral Venous and dural sinus Thrombosis (ISCVT), indicating that the most common sites of CVT are superior sagittal (62%) and left lateral sinuses (44.7%), including transverse and sigmoid sinuses [2].
Next, we analyzed the possible mechanisms of TBM complicated with CVT, including endothelial injury due to inflammatory response, sluggish venous flow, increased platelet aggregation, and release of pro-coagulant factors [16]. The host inflammatory response is critical in TBM pathology [17]. Microglial cells and migrated infected neutrophils and macrophages are rapidly activated and secrete cytokines and chemokines [18], such as tumor necrosis factor-alpha (TNF-a), interleukin-6 (IL-6), IL-1b, CCL2, CCL5, and CXCL10 [19]. TNF-a and IL-6 have an additive effect in pro-coagulant activity on human endothelial cells via platelet aggregation and thrombosis [20]. The other host mediators implicated in the pathology of TBM include matrix metalloproteinases (MMPs) and vascular endothelial growth factor (VEGF). Moreover, VEGF is a potent factor in vascular permeability and angiogenesis [20]. It is also vasculotoxic, prothrombotic, reduces cerebral blood flow, and produces nitric oxide and oxygen free radicals [21]. In our cases, two patients had a history of induced abortion, and one had undergone artificial assisted pregnancy, which is a high-risk factor for CVT.
Taken together, anti-TB treatment is essential. In the cases summarized above, all patients received standardized anti-TB treatment for TBM; anticoagulation therapy is the mainstay of CVT treatment. The currently recommended treatment is anticoagulation with heparin, followed by oral anticoagulation for 3–6 months. In the current study, 50% of patients received anticoagulant therapy for CVT. Two other patients received other treatment (one child used aspirin; another patient received emergency surgery because of critical illness and died shortly after surgery). The other 12 patients did not receive anticoagulation treatment due to safety concerns as they believed that anticoagulants in infectious venous thrombosis may lead to new cerebral hemorrhage. Our study concluded that most patients who received anticoagulation therapy had a good prognosis (last mRS < 2), and no new cerebral hemorrhage was indicated. Of the 7 patients with poor prognosis (including 2 with last mRS 3–5 and 5 with last mRS 6), only 1 received anticoagulant treatment. This finding suggested that anticoagulant therapy improves the prognosis of patients.
Conclusion
CVT is one of the rare complications of TBM. Venous stroke may contribute to unexplained worsening of the neurological status. Thus, CVT must be sought as a differential diagnosis in patients with TBM showing worsening clinical features and/or new neurological signs.
Data Availability
All data generated or analyzed during this study are included in this published article.
Abbreviations
- TBM:
-
tuberculous meningitis
- CVT:
-
cerebral venous thrombosis
- MRI:
-
magnetic resonance imaging
- CNS TB:
-
central nervous system tuberculosis
- mNGS:
-
metagenomics next-generation sequencing
- CSF:
-
cerebrospinal fluid
- COVID-19:
-
coronavirus disease-19
- ISCVT:
-
International Study of Cerebral Venous and dural sinus Thrombosis
- TNF-a:
-
tumor necrosis factor-alpha
- IL-6:
-
interleukin-6
- MMPs:
-
matrix metalloproteinases
- VEGF:
-
vascular endothelial growth factor
- mRS:
-
modified Rankin scale
References
Ageno W, Beyer-Westendorf J, Garcia DA, Lazo-Langner A, McBane RD, Paciaroni M. Guidance for the management of venous thrombosis in unusual sites. J Thromb Thrombolysis. 2016;41:129–43. https://doi.org/10.1007/s11239-015-1308-1.
Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus thrombosis (ISCVT). Stroke. 2004;35:664–70. https://doi.org/10.1161/01.Str.0000117571.76197.26.
Saposnik G, Barinagarrementeria F, Brown RD Jr, Bushnell CD, Cucchiara B, Cushman M, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:1158–92. https://doi.org/10.1161/STR.0b013e31820a8364.
Marx GE, Chan ED. Tuberculous meningitis: diagnosis and treatment overview. Tuberc Res Treat. 2011;2011:798764. https://doi.org/10.1155/2011/798764.
Bansod A, Garg RK, Rizvi I, Malhotra HS, Kumar N, Jain A, et al. Magnetic resonance venographic findings in patients with tuberculous meningitis: predictors and outcome. Magn Reson Imaging. 2018;54:8–14. https://doi.org/10.1016/j.mri.2018.07.017.
Dhar J, Chhabra G, Khandelwal L, Anuradha S, Batra A. Cortical venous thrombosis complicating tubercular meningitis. J Coll Physicians Surg Pak. 2021;31:221–4. https://doi.org/10.29271/jcpsp.2021.02.221.
Dhawan SR, Chatterjee D, Radotra BD, Vaidya PC, Vyas S, Sankhyan N, et al. A child with tuberculous meningitis complicated by cortical venous and cerebral sino-venous thrombosis. Indian J Pediatr. 2019;86:371–8. https://doi.org/10.1007/s12098-018-2830-x.
Elkeslassy A, Weill A, Miaux Y, Savin D, Martin Duverneuil N, Chiras J. Dilatation of deep medullary veins in cortical venous occlusion due to focal tuberculous leptomeningitis. Neuroradiology. 1997;39:705–7. https://doi.org/10.1007/s002340050490.
Kumar RM, Saini L, Kaushik JS, Chakrabarty B, Kumar A, Gulati S. A combination of Moyamoya Pattern and cerebral venous sinus thrombosis: a case of Tubercular Vasculopathy. J Trop Pediatr. 2015;61:393–6. https://doi.org/10.1093/tropej/fmv036.
Ramdasi R, Mahore A, Kawale J, Thorve S. Cerebral venous thrombosis associated with tuberculous meningitis: a rare complication of a common disease. Acta Neurochir (Wien). 2015;157:1679–80. https://doi.org/10.1007/s00701-015-2493-6.
Tsimiklis CA, Gragnaniello C, Abou-Hamden A. Venous sinus thrombosis secondary to tuberculous meningitis: a novel cause of trigeminal neuralgia. BMJ Case Rep. 2014;2014. https://doi.org/10.1136/bcr-2014-207238.
Verma R, Lalla R, Patil TB, Tiwari N. A rare presentation of cerebral venous sinus thrombosis associated with tubercular meningitis. BMJ Case Rep. 2013;2013. https://doi.org/10.1136/bcr-2013-009892.
Guenifi W, Boukhrissa H, Gasmi A, Rais M, Ouyahia A, Hachani A, et al. [Cerebral venous thrombosis during tuberculous meningoencephalitis]. J Mal Vasc. 2016;41:210–4. https://doi.org/10.1016/j.jmv.2016.03.002.
Essajee F, Solomons R, Goussard P, Van Toorn R. Child with tuberculous meningitis and COVID-19 coinfection complicated by extensive cerebral sinus venous thrombosis. BMJ Case Rep. 2020;13. https://doi.org/10.1136/bcr-2020-238597.
Stam M, JJNEJo. Thromb Cereb Veins Sinuses. 2005;352:1791–8.
Leonard JM. Central Nervous System Tuberculosis. Microbiol Spectr. 2017;5. https://doi.org/10.1128/microbiolspec.TNMI7-0044-2017.
Rohlwink UK, Figaji A, Wilkinson KA, Horswell S, Sesay AK, Deffur A, et al. Tuberculous meningitis in children is characterized by compartmentalized immune responses and neural excitotoxicity. Nat Commun. 2019;10:3767. https://doi.org/10.1038/s41467-019-11783-9.
Almolda B, González B, Castellano B. Are microglial cells the regulators of lymphocyte responses in the CNS? Front Cell Neurosci. 2015;9:440. https://doi.org/10.3389/fncel.2015.00440.
Rock RB, Olin M, Baker CA, Molitor TW, Peterson PK. Central nervous system tuberculosis: pathogenesis and clinical aspects. Clin Microbiol Rev. 2008;21. https://doi.org/10.1128/cmr.00042-07. :243 – 61, table of contents.
Misra UK, Kalita J, Singh AP, Prasad S. Vascular endothelial growth factor in tuberculous meningitis. Int J Neurosci. 2013;123:128–32. https://doi.org/10.3109/00207454.2012.743127.
Misra UK, Kalita J, Maurya PK. Stroke in tuberculous meningitis. J Neurol Sci. 2011;303:22–30. https://doi.org/10.1016/j.jns.2010.12.015.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
QL, JH, YW and YS contributed to conception and design of the study. JH organized the database. YW performed the statistical analysis. QL wrote the first draft of the manuscript. JH, YW and YS wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version”.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. The study was approved by the Ethics Approval Committee of Tian** Haihe Hospital, and all participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, Q., Han, J., Wang, Y. et al. Cerebral venous thrombosis (CVT) complicating tubercular meningitis. BMC Neurol 23, 245 (2023). https://doi.org/10.1186/s12883-023-03286-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-023-03286-4