
Abstract
Background
Before the COVID-19 pandemic, many long-term care (LTC) homes experienced difficulties in providing residents with access to primary care, typically delivered by community-based family physicians or nurse practitioners (NPs). During the pandemic, legislative changes in Ontario, Canada enabled NPs to act in the role of Medical Directors thereby empowering NPs to work to their full scope of practice. Emerging from this new context, it remains unclear how NPs and physicians will best work together as primary care providers. NP/physician collaborative models appear key to achieving optimal resident outcomes. This sco** review aims to map available evidence on existing collaborative models of care between NPs and physicians within LTC homes.
Methods
The review will be guided by the research question, “What are the structures, processes and outcomes of collaborative models of care involving NPs and Physicians in LTC homes?” This sco** review will be conducted according to the methods framework for sco** reviews outlined by Arksey and O’Malley and refined by Levac et al., Colquhoun et al., and Daudt et al., as well as the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Sco** Reviews (PRISMA-ScR) Statement. Electronic databases (MEDLINE, Embase + Embase Classic, APA PsycInfo, Cochrane Central Register of Controlled Trials, AMED, CINAHL, Ageline, and Scopus), grey literature, and reference lists of included articles will be searched. English language studies that describe NP and physician collaborative models within the LTC setting will be included.
Discussion
This sco** review will consolidate what is known about existing NP/physician collaborative models of care in LTC homes. Results will be used to inform the development of a collaborative practice framework for long-term care clinical leadership.
Similar content being viewed by others
Introduction
As the older adult population grows, worldwide the number of older adults who will require care in long-term care (LTC) homes will also increase. LTC homes provide 24/7 health and personal care support to residents with multiple health and social complexities including neurological, circulation, and musculoskeletal diseases, dementia, acute medical conditions, and stroke [1]. The pandemic impacted the LTC sector significantly, including the disproportionately high rate of COVID-19 deaths amongst LTC residents, the effects of social isolation on residents’ wellbeing, challenges with infection prevention and control practices, and staffing shortages due to limiting staff to single workplaces [2, 3]. This unprecedented situation illuminated long-standing deficiencies in LTC such as timely access to primary care for this complex, mainly older adult population [4]. The current model does not meet the needs of residents experiencing acute and chronic health issues, as limited accessibility to primary care providers is internationally cited as a common challenge [5,6,7,8].
There has been a steady increase in the number of NPs employed within the LTC sector over the last 20 years [9]. NPs are advanced practice nurses requiring graduate education for entry; their scope of practice include diagnosis, prescribing medications, and performing medical procedures [10]. Quality of care provided by NPs in LTC homes is comparable to that of physicians and has been shown to improve resident outcomes and reduce hospital transfers [11,12,13]. Additionally, NPs bring a breadth of advanced nursing skills to resident care, resulting in improved communication with family and care-partners, staff capacity-building, and strong clinical leadership and care coordination [11, 14].
The COVID-19 pandemic made in-person access to physicians increasingly difficult, as some physicians were recommended to adopt a “virtual-first” approach [15]. This experience provided an opportunity to examine the effects of optimizing the NP role and empowered NPs to work to their full scope of practice in a leadership role in LTC homes [16]. Several studies have reported positive outcomes from NP care during the pandemic, including successful COVID-19 recoveries, effective pain and symptom management, and ensuring dignified deaths for residents, demonstrating how NPs can provide urgently needed support to LTC residents [17, 18].
Similar to their physician colleagues, consultation and collaboration with other physicians and specialists is an essential component of the NP provider role; NPs do not function in isolation [3, 19, 20]. The intrinsic collaboration between NP and physician roles has resulted in a higher quality of resident care, decreased hospitalization rates, and the creation of an improved working environment for direct care providers [20]. Studies have investigated the abstract qualities inherent to the collaboration process. For optimal resident care, the NP-physician collaborative relationship requires commitment and time for development, where each care provider is able to employ qualities unique to their role [20]. When the collaborative process remains informal, it can result in an absence of funding to support collaborative practice models, inadequate educational preparation, and a lack of clarity regarding role definitions and the facilitators and barriers in implementing this process. The resources and capacities required to ensure successful collaboration have not yet been clearly elucidated. With some understanding of the underlying principles required for success, several collaborative models for the LTC context have been developed, such as the Evercare model and the Missouri Quality Initiative [21]. However, a comprehensive review and comparison of existing models has not been reported. Further, frameworks evaluating these models to inform best practices do not exist. While it is clear that residents, their care partners, and LTC care providers have benefitted from collaborative practices, a review of the existing models of care involving NP and physician collaboration is required to identify current gaps in the literature. A description of the structures, processes, and outcomes of models of NP-physician collaborative care will inform the development of a collaborative practice framework for LTC clinical leadership.
Objective
This sco** review will examine and map evidence for collaborative models of care between NPs and physicians in LTC homes.
Methodology
This sco** review will be conducted according to the methods framework for sco** reviews outlined by Arksey and O’Malley [22] and refined by Levac et al. [23], Colquhoun et al. [24], and Daudt et al. [25]. This framework is appropriate as the nature of the research question is exploratory, with the intention of map** key concepts, evidence gaps, and implications. This sco** review will also be conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Sco** Reviews (PRISMA-ScR) Statement [26].
Stage 1: Identifying the research questions
Primary question
-
What are the structures, processes, and outcomes of collaborative models of care involving NPs and Physicians in LTC homes?
Secondary questions
-
What are the strengths and weaknesses of each model?
-
What are the barriers and facilitators for implementation of each model?
-
How does each model impact resident, staff, health systems, and cost outcomes?
Stage 2: Identifying relevant literature
We will conduct a comprehensive search of the scientific and grey literature as per sco** review methods [22,23,24,25]. We will implement a search strategy developed by our health sciences information specialist in conjunction with team members and key stakeholders. Prior to funding, a preliminary MEDLINE ALL (Ovid) search was conducted to ensure adequate literature availability and was validated through the retrieval of a key set of relevant studies. The search strategy has since been refined to meet the revised review scope (Appendix 1). This MEDLINE strategy will be translated to the following databases: Cochrane Central Register of Controlled Trials (Ovid), Embase and Embase Classic (Ovid), APA PsycInfo (Ovid), AMED (Ovid), AgeLine (EBSCO), CINAHL Complete (EBSCO), and Scopus. The database search strategy consists of two broad concepts: (1) NPs and (2) LTC. When functionality is available in the databases, searches will be limited to identify English language publications as restricting reviews to English language publications appears to have little impact on conclusions of reviews [27]. We will conduct the search from 1960 onwards as this marked the introduction of the NP role nationally and internationally.
A search of the grey literature will be conducted using grey literature databases (e.g., OpenGrey) and search engines (e.g., Google) to identify any relevant non-indexed literature or alternative media. The reference list of the included studies will be hand searched for additional relevant scientific and grey literature. In addition to calling upon the expertise and experience of team members, we will reach out to experts in fields related to interprofessional models of care to further identify unpublished yet relevant data.
Stage 3: Study Selection
Process
Following the search, all citations will be uploaded to Covidence systemic review software and duplicates will be removed [28]. A minimum of two independent reviewers will screen all retrieved titles and abstracts against a priori inclusion and exclusion criteria to identify potentially relevant studies. Reviewers will retrieve full-text articles of potentially relevant studies/reports and two reviewers will evaluate them against the a priori criteria. Any disagreements will be resolved through consultation with other team members to reach consensus. Throughout, we will hold monthly meetings with team researchers and collaborators to discuss progress and findings. Data extraction and literature quality assessments will be managed using Covidence [28].
Inclusion Criteria
This sco** review will incorporate the Population-Concept-Context Framework to ensure clarity in our scope of inclusion [29]. The population represented are NPs and physicians, the concept is ‘collaborative models of care’, and the context is LTC homes.
The following literature will be included:
-
The population includes NPs and physicians primary care providers. The NP role will be operationalized as graduate-prepared advanced practice nurses who assess, diagnose, and treat patients in collaboration with other healthcare professionals. The physician role will be operationalized as any clinician with a medical degree, including all specialties.
-
The literature describes a collaborative model of care. We have loosely operationalized models using Davidson’s definition [30]: “An overarching design for the provision of a particular type of health care service”. Based upon our broad approach to study retrieval, the concepts of ‘collaboration’ and ‘models of care’ will be identified when reviewing the literature in this step, and manually included.
-
The setting is LTC homes, operationalized as a residential, long-stay facility that provides 24/7 health and personal care.
-
All methodologies of scientific literature (e.g., qualitative, quantitative, mixed, reviews, case studies, theoretical, applied, etc.).
-
Published editorials and commentaries.
-
Grey literature, including published and unpublished data, such as community and policy reports, government or public agency publications, conference proceedings, dissertations, practice guidelines, educational materials, etc.
-
Literature published in English.
-
Literature published since 1960.
Exclusion Criteria
The following literature will not be included
-
Books and book chapters.
-
The context is not described as LTC (e.g., acute care, community care, home care, transitional care programs, skilled nursing facilities, etc.).
Stage 4: Charting the data
Data charting and literature quality assessments will be managed using Covidence to sift, categorize, and sort findings according to key issues and themes. The data charting form (Table 1) includes study characteristics, population and setting data, and the multiple components of models of care. Structure will be charted, including the characteristics of NPs and physicians in LTC homes, the LTC type, size, setting, funding models, and educational components. Process will include a description of the collaborative models of care and the specific roles of the NP and physician, strategies used for care through interprofessional collaboration, and barriers and facilitators for implementation. Outcomes will be specified for residents, staff, healthcare systems, and cost where applicable.
The charting form will be piloted on five studies by two independent analysts to ensure adequacy and consistency. Any changes to the form will be made in consultation with the team prior to extraction of data from all articles.
Quality appraisal
The Joanna Briggs Institute’s critical appraisal tools will be used for quality appraisal of all studies included for synthesis [31]. A minimum of two appraisers will use these checklists to assess trustworthiness, relevance and results of scientific papers, opinion, and grey literature to ultimately inform data interpretation and synthesis. We will employ appraisal tools that are relevant to the study type, including qualitative, quantitative, reviews, case studies and opinion texts [31].
Stage 5: Collating, summarizing and reporting results
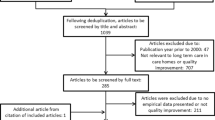
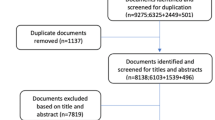
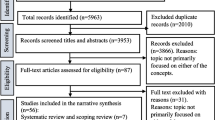
To capture the extent and nature of the data retrieved, we will present it both qualitatively and quantitatively. Findings of this sco** review will be summarized with the PRISMA flowchart [26]. An overview of the categorical features of the literature will be presented numerically. We will also take a narrative synthesis approach to present the descriptive findings of the selected literature [22,23,24,25]. Using this narrative map** exercise, a framework will be generated according to Donabedian’s structure-process-outcome model [32]. We will aim to summarize models of care, NP and physician roles, strategies for interprofessional collaboration, and associated outcomes to inform future implementation and evaluation.
Stage 6: Consultation
Our consultation plan includes both integrated and end-of-grant knowledge translation (KT). We will engage stakeholders in a formal review of the collaborative NP/physician models and the emerging framework developed in the synthesis of the data. Stakeholders will include representatives from organizations representing NPs and physicians working in LTC; organizations representing not-for-profit, private, and municipal LTC homes, who are team members of the project. These individuals include healthcare providers, policy decision makers, and leaders of healthcare organizations. We will adopt a qualitative approach to solicit input from stakeholders to determine the relevance of the emerging framework to Ontario LTC settings and suggest ways to modify it as needed to enhance its applicability. We will share information on the collaborative NP/physician models and the framework, inviting them to discuss structures, processes, and outcomes of the emerging framework. Discussions will be audio-recorded and transcribed verbatim [33]. Transcripts will undergo content analysis by two independent members of the research team to develop themes and subthemes representative of stakeholder findings, which we anticipate will be modified iteratively through these processes.
Once data are analyzed, we will hold a meeting to present findings to the whole team and to solicit feedback on the final content before broader dissemination of findings to decision-makers within the LTC sector, and NP and physician associates. Findings from the sco** review will be presented at national and international conferences and published in peer-reviewed journals. With the support of our stakeholders, we will also disseminate fact sheets, evidence briefs, and reports targeted at specific audiences. Existing resources and platforms of our stakeholder organizations, including websites, mail-outs, and information sessions, will be used to disseminate evidence briefs to accelerate the impact of our findings.
Discussion
This study procedure is grounded in a collaborative, interdisciplinary approach that will strengthen our understanding of NP and physician collaborative models of care within LTC homes. Findings will report on resident, staff, health systems, and cost outcomes associated with various collaborative models; synthesize findings that focus on best workforce experience for NPs and physicians; and elucidate suitability and applicability of these models from the perspective of our knowledgeable stakeholders.
Our ultimate aim is to provide decision-makers and knowledge users with high-quality, timely, and relevant evidence of the models of physician and NP collaboration in LTC homes. Consideration of the reported structures, process and outcomes of these models of care and subsequent input from stakeholders across Ontario will inform the development of a collaborative practice framework for long-term care clinical leadership. Findings of this sco** review will inform the development of a framework that when implemented, should be evaluated for its value to improvements in primary care for LTC home residents.
Availability of data and materials
The data analyzed during the current study will be available from the corresponding author on reasonable request.
Abbreviations
- KT:
-
Knowledge Translation
- LTC:
-
Long-Term Care
- MRP:
-
Most Responsible Provider
- NP:
-
Nurse Practitioner
References
Ontario Long-Term Care Association. This is long-term care 2019. 2019. Available from: https://www.oltca.com/OLTCA/Documents/Reports/TILTC2019web.pdf. Accessed 19 Oct 2021.
National Institute on Ageing. NIA Long term care COVID-19 tracker, 2020–2021 (pandemic LTC deaths). Available from: https://www.cihi.ca/en/covid-19-resources/impact-of-covid-19-on-canadas-health-care-systems/long-term-care. Accessed 5 May 2022.
McGilton KS, Krassikova A, Boscart V, Sidani S, Iaboni A, Vellani S, et al. Nurse practitioners rising to the challenge during the Coronavirus Disease 2019 pandemic in long-term care homes. Gerontologist. 2021;61(4):615–23. https://doi.org/10.1093/geront/gnab030.
Lam JM, Anderson GM, Austin PC, Bronskill SE. Family physicians providing regular care to residents in Ontario long-term care homes: characteristics and practice patterns. Can Fam Physician. 2012;58(11):1241–8.
Ryskina KL, Song W, Sharma V, Yuan Y, Intrator O. Characterizing physician practice in nursing homes using claims-based measures: correlation with nursing home administrators’ perceptions. Med Care Res Rev. 2021;78(6):806–15. https://doi.org/10.1177/1077558720960900.
Barańska I, Kijowska V, Engels Y, Finne-Soveri H, Froggatt K, Gambassi G, et al. Factors associated with perception of the quality of physicians’ end-of-life communication in long-term care facilities: PACE cross-sectional study. J Am Med Dir Assoc. 2020;21(3):438.e1-439.e8. https://doi.org/10.1016/j.jamda.2019.07.018.
Kobewka DM, Kunkel E, Hsu A, Talarico R, Tanuseputro P. Physician availability in long-term care and resident hospital transfer: a retrospective cohort study. J Am Med Dir Assoc. 2020;21(4):469-75.e1. https://doi.org/10.1016/j.jamda.2019.06.004.
Ouslander JG, Lamb G, Perloe M, Givens JH, Kluge L, Rutland T, et al. Potentially Avoidable Hospitalizations of Nursing Home Residents: Frequency, Causes, and Costs. Journal of the American Geriatrics Society (JAGS). 2010;58(4):627–35. https://doi.org/10.1111/j.1532-5415.2010.02768.x.
Goodwin JS, Agrawal P, Li S, Raji M, Kuo Y-F. Growth of physicians and nurse practitioners practicing full time in nursing homes. J Am Med Dir Assoc. 2021;22(12):2534-9.e6. https://doi.org/10.1016/j.jamda.2021.06.019.
Nurse Practitioners’ Association of Ontario. What is a nurse practitioner?. 2020. Available from: https://npao.org/about-npao/what-is-a-np/. Accessed 19 Oct 2021.
Donald F, Martin-Misener R, Carter N, Donald EE, Kaasalainen S, Wickson-Griffiths A, et al. A systematic review of the effectiveness of advanced practice nurses in long-term care. J Adv Nurs. 2013;69(10):2148–61. https://doi.org/10.1111/jan.12140.
Kilpatrick K, Tchouaket É, Jabbour M, Hains S. A mixed methods quality improvement study to implement nurse practitioner roles and improve care for residents in long-term care facilities. BMC Nurs. 2020;19:6. https://doi.org/10.1186/s12912-019-0395-2.
Tchouaket É, Kilpatrick K, Jabbour M. Effectiveness for introducing nurse practitioners in six long-term care facilities in Québec, Canada: a cost-savings analysis. Nurs Outlook. 2020;68(5):611–25. https://doi.org/10.1016/j.outlook.2020.06.002.
Carranza AN, Munoz PJ, Nash AJ. Comparing quality of care in medical specialties between nurse practitioners and physicians. J Am Assoc Nurse Pract. 2020;33(3):184–93. https://doi.org/10.1097/JXX.0000000000000394.
Ontario College of Family Physicians. Considerations for family physicians: balancing in-person and virtual care. 2021. Available from: https://www.ontariofamilyphysicians.ca/considerations-for-in-person-visits-aug2021.pdf. Accessed 19 Oct 2021.
Government of Ontario. O. Reg. 95/20: streamlining requirements for long-term care homes. 2020. Available from: https://www.ontario.ca/laws/regulation/200095.
Thomas-Gayle P, Muller LS. Nurse practitioners bridging the gap: the absence of medical doctors during the COVID-19 crisis. Prof Case Manag. 2021;26(1):38–42. https://doi.org/10.1097/NCM.0000000000000481.
Vellani S, Boscart V, Escrig-Pinol A, Cumal A, Krassikova A, Sidani S, et al. Complexity of nurse practitioners’ role in facilitating a dignified death for long-term care home residents during the COVID-19 pandemic. J Pers Med. 2021;11(5). doi:https://doi.org/10.3390/jpm11050433.
Sox HC. Independent primary care practice by nurse practitioners. JAMA. 2000;283(1):106–8. https://doi.org/10.1001/jama.283.1.106.
Bridges S. Exploration of the concept of collaboration within the context of nurse practitioner-physician collaborative practice. J Am Assoc Nurse Pract. 2014;26(7):402–10. https://doi.org/10.1002/2327-6924.12043.
Cacchione PZ. Innovative care models across settings: providing nursing care to older adults. Geriatr Nurs. 2020;41(1):16–20. https://doi.org/10.1016/j.gerinurse.2020.01.011.
Arksey H, O’Malley L. Sco** studies: towards a methodological framework. Int J Soc Res Methodol Theory Pract. 2005;8(1):19–32. https://doi.org/10.1080/1364557032000119616.
Levac D, Colquhoun H, O’Brien KK. Sco** studies: advancing the methodology. Implement Sci. 2010;5:69. https://doi.org/10.1186/1748-5908-5-69.
Colquhoun HL, Levac D, O’Brien KK, Straus S, Tricco AC, Perrier L, et al. Sco** reviews: time for clarity in definition, methods, and reporting. J Clin Epidemiol. 2014;67(12):1291–4. https://doi.org/10.1016/j.jclinepi.2014.03.013.
Daudt HML, Van Mossel C, Scott SJ. Enhancing the sco** study methodology: a large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med Res Methodol. 2013:(13)48. doi:https://doi.org/10.1186/1471-2288-13-48.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29;372:n71. doi:https://doi.org/10.1136/bmj.n71.
Dobrescua A, Nussbaumer-Streita B, Kleringsa I, Wagnera G, Persada E, Sommera I, et al. Restricting evidence syntheses of interventions to English-language publications is a viable methodological shortcut for most medical topics: a systematic review. J Clin Epidemiol. 2021;137:209–17. https://doi.org/10.1016/j.jclinepi.2021.04.012.
Veritas Health Innovation. Covidence systematic review software. VHI, Melbourne Australia. 2020. Available from: https://www.covidence.org/.
Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil, H. Chapter 11: sco** reviews (2020 version). In: Aromataris E, Munn Z (Editors). JBI Manual for Evidence Synthesis, JBI, 2020. doi:https://doi.org/10.46658/JBIMES-20-12.
Davidson P, Halcomb E, Hickman L, Phillips J, Graham B. Beyond the rhetoric: what do we mean by a “model of care”? Aust J Adv Nurs. 2006;23(3):47–55.
JBI. Critical appraisal tools. Joanna Briggs Institute (JBI). 2020. Available from: https://jbi.global/critical-appraisal-tools. Accessed 19 Apr 2022.
Donabedian A. Evaluating the quality of medical care. Milbank Q. 2005;83(4):691–729. https://doi.org/10.1111/j.1468-0009.2005.00397.x.
Morgan DL. Qualitative content analysis: a guide to paths not taken. Qual Health Res. 1993;3(1):112–21. https://doi.org/10.1177/104973239300300107.
Acknowledgements
We gratefully acknowledge our stakeholders Dana Cooper, Nancy Cooper, Paul Katz, Kathryn May, Andrea Moser, and Lisa Levin for their valuable and constructive guidance in develo** the study concept and design.
Funding
This study has been funded by the Canadian Institutes of Health Research. JB and KM are supported by the Walter & Maria Schroeder Institute for Brain Innovation and Recovery.
Author information
Authors and Affiliations
Contributions
All authors contributed to study concept and design. KM, LH, and AW drafted the manuscript and all authors contributed critical revision of the manuscript for important intellectual content. All authors approve the submitted version of the manuscript and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This sco** review will require ethics approval for the stakeholder consultations and will be submitted to the University Health Network Research Ethics Board.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:
Appendix 1. MEDLINE search strategy
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
McGilton, K.S., Haslam-Larmer, L., Wills, A. et al. Nurse practitioner/physician collaborative models of care: a sco** review protocol. BMC Geriatr 23, 98 (2023). https://doi.org/10.1186/s12877-023-03798-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-023-03798-1