
Abstract
Background
Impact of advanced age on disease characteristics of acute cholecystitis (AC), and surgical outcomes after laparoscopic cholecystectomy (LC) has not been established.
Methods
This single-center retrospective study included patients who underwent LC for AC between April 2010 and December 2020. We analyzed the disease characteristics and surgical outcomes according to age: Group 1 (age < 60 years), Group 2 (60 ≤ age < 80 years), and Group 3 (age ≥ 80 years). Risk factors for complications were assessed using logistic regression analysis.
Results
Of the 1,876 patients (809 [43.1%] women), 723 were in Group 1, 867 in Group 2, and 286 in Group 3. With increasing age, the severity of AC and combined common bile duct stones increased. Group 3 demonstrated significantly worse surgical outcomes when compared to Group 1 and 2 for overall (4.0 vs. 9.1 vs. 18.9%, p < 0.001) and serious complications (1.2 vs. 4.2 vs. 8.0%, p < 0.001), length of hospital stay (2.78 vs. 3.72 vs. 5.87 days, p < 0.001), and open conversion (0.1 vs. 1.0 vs. 2.1%, p = 0.007). Incidental gallbladder cancer was also the most common in Group 3 (0.3 vs. 1.5 vs. 3.1%, p = 0.001). In the multivariate analysis, body mass index < 18.5, moderate/severe AC, and albumin < 2.5 g/dL were significant risk factors for serious complications in Group 3.
Conclusion
Advanced age was associated with severe AC, worse surgical outcomes, and a higher rate of incidental gallbladder cancer following LC. Therefore, in patients over 80 years of age with AC, especially those with poor nutritional status and high severity grading, urgent surgery should be avoided, and surgery should be performed after sufficient supportive care to restore nutritional status before LC.
Similar content being viewed by others


Background
Acute cholecystitis (AC) is one of the most common surgical indications of gastrointestinal diseases. Cholecystectomy is a treatment of choice for AC, and currently, laparoscopic cholecystectomy (LC) is the golden standard on AC [1, 2].
The most common cause of AC is gallstones, the prevalence and complications of which have been shown to increase with age [3, 4]. As life expectancy has increased, the incidence of AC has also increased. Although LC is considered relatively safe, a 6–9% risk of serious complication and 0.1–0.3% of mortality still exist [5, 6]. Advanced age may be associated with a high risk of postoperative complications owing to greater comorbidities and poorer general conditions [7]. Percutaneous transhepatic gallbladder drainage (PTGBD) is considered an alternative treatment option for high-risk older patients. However, we previously reported that elective LC is better than conservative treatment in older patients with AC [8]. Therefore, the treatment strategy for AC in older patients remains controversial.
Recently, some studies have reported poor surgical outcomes for LC in older patients [9, 10]. Nevertheless, data on clinical characteristics of the disease and on the surgical outcomes of LC in elderly patients with AC are still lacking. In addition, treatment outcomes of AC can differ from clinical features, such as the severity of AC and combined common bile duct (CBD) stones [11]. Therefore, the aim of this study is to establish the impact of advanced age on disease characteristics of AC and surgical outcomes after LC.
Methods
Patients
From April 2010 to December 2020, all consecutive patients diagnosed with AC who underwent elective LC at Konyang University Hospital were evaluated. Patients with suspected gallbladder cancer, based on imaging studies, or those who underwent emergency LC and other combined surgeries were excluded. A total of 1876 patients were included in the study. The diagnosis and classification of AC severity were based on the 2018 Tokyo Guidelines [12]. We divided the study population into three groups according to age and retrospectively reviewed the patients’ demographics, disease characteristics, and surgical outcomes: Group 1 (age < 60 years), Group 2 (60 ≤ age < 80 years), and Group 3 (age ≥ 80 years).
This study was approved by the Institutional Review Board of Konyang University Hospital (IRB No. 2022-01-016), and the requirement for obtaining informed consent was waived owing to the retrospective study design by the Institutional Review Board of Konyang University Hospital. All methods were performed in accordance with the relevant guidelines and regulations.
Definition of demographics and surgical outcomes
The general condition and physical fitness of each patient were evaluated using the Charlson Age Comorbidity Index (CACI) [13] and American Society of Anesthesiologists physical status (ASA PS) classification [14]. The nutritional status of the patients was assessed using body mass index (BMI) and preoperative serum albumin level. The presence of gallstones and CBD stones was confirmed by imaging studies using abdominal ultrasonography, computed tomography, or magnetic resonance cholangiopancreatography. PTGBD is indicated in patients with AC who are not fit for immediate surgery due to the high risk of surgery at the time of presentation. The detailed indication for PTGBD has been described in our previous study [15]. When PTGBD was performed, following LC was performed within the same hospitalization period. Operation time was calculated as the time from skin incision to skin closure. Blood loss estimates were obtained from surgical records. Subtotal cholecystectomy was defined as making an incision in the gallbladder, aspirating the contents, and removing as much of the gallbladder wall as possible, with the aim of treating the stump instead of removing the entire gallbladder [16].
Postoperative complications were graded according to the Clavien-Dindo classification [17]. Adjacent organ injury was defined as unintended damage requiring repair of organs other than the gallbladder, such as the bile duct, hepatic artery, duodenum, small intestine, and colon. Serious complications were defined as a level greater than grade III of the Clavien-Dindo classification. The postoperative hospital stay was defined as the number of days of hospital stay after LC. The total hospital stay was defined as the number of days between admission and discharge. Pulmonary complications were defined as any complication affecting the respiratory system after general anesthesia and LC, including pneumonia, atelectasis, pleural effusion, and respiratory failure [18]. The diagnosis of bile leakage was based on the definition provided by the International Study Group of Liver Surgery [19].
Statistical analysis
Continuous variables were summarized as mean and standard deviation and compared using analysis of variance. Categorical variables are presented as counts and percentages and were compared using the Chi-square test. Univariate and multivariate analyses were performed to identify the predictors of serious complications after LC in patients of advanced age. Multivariate analyses of the significant factors identified in univariate analyses were performed using a logistic regression model. All tests were two-sided, and p-values less than 0.05 were considered statistically significant. Statistical analyses were performed using SPSS version 27 (SPSS Inc., Chicago, IL, USA).
Results
Patients’ characteristics
The demographic and disease characteristics of the study population are shown in Table 1. A total of 1876 patients were divided into three groups according to age: Group 1 (age < 60 years, n = 723), Group 2 (60 ≤ age < 80 years, n = 867), and Group 3 (age ≥ 80 years, n = 286). Female patients were most common in group 3 (45.0% vs. 37.4% vs. 55.9%, p < 0.001). With increasing age, BMI decreased (25.5 kg/m2 vs. 24.7 kg/m2 vs. 23.0 kg/m2, p < 0.001), and ASA PS (≥ III; 6.1% vs. 33.9% vs. 60.8%, p < 0.001), CACI (≥ 6; 0.0% vs. 3.6% vs. 27.6%, p < 0.001), severity of AC (grade III; 0.4% vs. 4.5% vs. 8.7%, p < 0.001), acalculous cholecystitis (22.7% vs. 29.5% vs. 35.0%, p < 0.001), and combine CBD stones (15.6% vs. 19.5% vs. 24.8%, p < 0.001) increased. There was no significant difference in previous abdominal surgery history among the three groups. In laboratory findings, there were significant differences between the three groups in WBC, hemoglobin, platelet, PT INR, creatinine, albumin, total bilirubin, and CRP levels; however, there were no significant differences in AST and ALT levels.
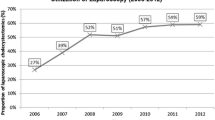
A total of 1876 patients, preoperative PTGBD was performed in 1020 (54.4%) with a median interval from PTGBD to LC of 5 days (minimum 1 and maximum 64. of interval days). Preoperative PTGBD was most frequently performed in Group 3 (37.5% vs. 61.0% vs. 76.9%, p < 0.001).
Surgical outcomes
A comparison of the surgical variables according to age is presented in Table 2. There were no significant differences in operation time, adjacent organ injury detected during surgery, or subtotal cholecystectomy. With increasing age, estimated blood loss (19.4 mL vs. 26.6 mL vs. 28.9 mL, p = 0.028), open conversion (0.1% vs. 1.0% vs. 2.1%, p = 0.007), overall complication (4.0% vs. 9.1% vs. 18.9%, p < 0.001), serious complication (1.2% vs. 4.2% vs. 8.0%, p < 0.001), 90-day mortality (0.0% vs. 0.1% vs. 2.1%, p < 0.001), postoperative hospital stay (2.02 days vs. 3.72 days vs. 5.87 days, p < 0.001), total hospital stay (3.76 days vs. 6.64 days vs. 10.69 days, p < 0.001), surgical site infection (1.5% vs. 4.2% vs. 6.3%, p < 0.001), pulmonary complication (0.6% vs. 2.5% vs. 6.6%, p < 0.001), and re-admission (0.3% vs. 0.8% vs. 1.7%, p = 0.048) increased.
In the univariate analysis, age ≥ 80 years was a statistically significant risk factor for incidental gallbladder cancer after LC (odds ratio [OR] 11.713, p = 0.002) (Table 3).
Details of the serious postoperative complications
Serious postoperative complications were classified according to the Clavien-Dindo classification, and 65 were reported (Table 4). The percentage of serious complications (1.2% vs. 4.2% vs. 8.0%) increased with advancing age. In grade IIIa complications, fluid collection with percutaneous drain (PCD) insertion was the most common, followed by bile leakage with endoscopic nasobiliary drainage or endoscopic retrograde biliary drainage insertion, pleural effusion with PCD insertion, CBD stone with endoscopic stone extraction, and wound dehiscence with local repair. Re-operation included mechanical ileus, bile leakage, wound dehiscence, pressure sore, and empyema of the lung, and was reported as grade IIIb. With increasing age, grade IV and V complications increased (Grade IV, 0.1% vs. 0.7% vs. 2.4%); Grade V, 0.0% vs. 0.1% vs. 2.0%). Among grade IV complications, pneumonia with mechanical ventilation was the most common, followed by mechanical ileus with re-operation and cerebrovascular accident with ICU care. Among grade V complications, five cases of pneumonia and two cases of organ space surgical site infection have been reported.
Risk factor for serious complications in patients over 80 years of age
The results of univariate and multivariate analyses for serious complications (Clavien-Dindo classification grade III to V) in patients aged > 80 years are presented in Table 5. Univariate analysis revealed that low BMI (< 18.5 kg/m2), severity of AC (moderate and severe AC), and low serum albumin (< 2.5 g/dL) were statistically significant. In multivariate analysis, low BMI (< 18.5 kg/m2, OR 4.254, p = 0.019), severity of AC (moderate, OR 3.545, p = 0.015; severe, OR 3.924, p = 0.048), and low serum albumin (> 2.5 g/dL, OR 4.414, p = 0.032) were identified as significant risk factors for serious complications after LC in older patients.
Discussion
AC is an inflammatory disease of the gallbladder caused by impacted gallstone obstruction of the outlet of the gallbladder, either in the infundibulum or in the cystic duct, in approximately 90–95% of patients with AC [20]. In contrast, acalculous cholecystitis accounts for approximately 5–10% of all cases of AC. Acalculous cholecystitis usually occurs in critically ill patients receiving total parenteral nutrition; it has been reported to occur mainly in men over 50 years of age [21, 22]. Several studies have reported an increased incidence of acalculous cholecystitis in the outpatient population, including patients with atherosclerosis, as seen in hypertension and diabetes [23, 24]. In the present study, there was an increase in acalculous cholecystitis with age, which seems to be related to an increase in atherosclerotic vascular disease with age.
CBD stones, cholangitis, and gallstone pancreatitis may be present in patients with AC. In the general population, 5% of patients with cholecystitis have coexisting CBD stones [25]. The risk of gallstones increases with age regardless of ethnicity [26], and concomitant gallbladder and CBD stones have been reported to be associated with increasing age [27]. In the present study, we confirmed that the proportion of CBD stones combined with AC gradually increased with age. Therefore, older patients with AC should be checked for combined CBD stones, and an appropriate treatment plan should be established.
LC is accepted as a relatively safe procedure with a mortality rate of less than 1% [28]. However, the risk of postoperative complications increases in patients with advanced age, and recently published studies reported a mortality rate of 1.7–10.0% after LC for AC in octogenarians [10, 29, 30]. Similar to previous studies, our study also reported a mortality rate of 2.1% after LC in patients aged > 80 years. In elderly patietns with AC, ASA classification and CACI increase with increasing age and comorbidity, which can increase the risk of general anesthesia and postoperative complications. In addition, as show in our study, the severity of AC increases with age, making surgery technically challenging. In general, elderly patietns are slower to return to mobility and daily activities after surgery. Early discharge after surgery can be a social issue, especially for older patients who live alone and require daily care. These factors contribute to an increased length of hospital stay after LC in elderly patietns with AC, and indeed, in this study, we confirmed that the length of hospital stay increased with increasing age. Therefore, in the treatment of AC, older patients over 80 years of age should fully consider the risk of LC and decide to undergo surgery.
PTGBD is an alternative treatment to avoid urgent surgery for AC in high-risk or older patients. However, PTGBD is not a definitive treatment option for AC that can replace LC. We previously reported that elective LC is recommended in AC after PTGBD for patients aged > 80 years because of the high recurrence rate of biliary events after PTGBD removal and the difficulty associated with PTGBD maintenance [8]. In older patients with AC, it is important to decide on surgery by evaluating the risks and benefits of LC through a detailed preoperative evaluation rather than by avoiding LC in all cases. In the multivariate analysis of our study, BMI < 18.5 kg/m2, serum albumin < 2.5 mg/dL, and moderate/severe AC were statistically significant risk factors for serious complications after LC in patients aged > 80 years. It was confirmed that the severity of AC and the patient’s preoperative nutritional status had a significant impact on postoperative outcomes. Therefore, in older and malnourished patients with AC, urgent surgery should be avoided, and surgery should be performed after sufficient supportive care to restore nutritional status before LC.
In particular, in patients with AC, it is not easy to distinguish early gallbladder cancer through imaging studies in which a mass is not clearly formed due to wall thickening of the gallbladder due to inflammation. Several previous studies have reported an increased risk of incidental gallbladder cancer diagnosed after LC for benign gallbladder disease associated with advanced age [31, 32]. In the present study, it was confirmed that the risk of incidental gallbladder cancer increased with age, particularly in patients with AC (age ≥ 80 years; OR 11.713, p = 0.002). Therefore, in older patients with AC, the possibility of gallbladder cancer should be sufficiently explained before LC, and sufficient attention should be paid during LC to prevent the occurrence of bile spillage, which may adversely affect prognosis [33].
The present study had several limitations. First, this was a single-institutional retrospective study, and our results may have limited generalizability, although a relatively large number of patients who underwent LC were included. Second, there was a selection bias as the study included only patients who underwent surgical treatment. Finally, our study only evaluated short-term surgical outcomes. Further studies that include long-term outcomes, such as quality of life, are needed.
Conclusion
Advanced age was associated with severe AC, worse surgical outcomes, and a higher rate of incidental gallbladder cancer following LC. Therefore, in patients over 80 years of age with AC, especially those with poor nutritional status and high severity grading, urgent surgery should be avoided, and surgery should be performed after sufficient supportive care to restore nutritional status before LC.
Data Availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AC:
-
acute cholecystitis
- LC:
-
laparoscopic cholecystectomy
- PTGBD:
-
percutaneous transhepatic gallbladder drainage
- CBD:
-
common bile duct
- CACI:
-
Charlson Age Comorbidity Index
- ASA PS:
-
American Society of Anesthesiologists physical status
- BMI:
-
body mass index
- PCD:
-
percutaneous drain
References
Strasberg SM. Clinical practice. Acute calculous cholecystitis. N Engl J Med. 2008;358(26):2804–11.
Okamoto K, Suzuki K, Takada T, Strasberg SM, Asbun HJ, Endo I, Iwashita Y, Hibi T, Pitt HA, Umezawa A, et al. Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):55–72.
Festi D, Dormi A, Capodicasa S, Staniscia T, Attili AF, Loria P, Pazzi P, Mazzella G, Sama C, Roda E, et al. Incidence of gallstone disease in Italy: results from a multicenter, population-based italian study (the MICOL project). World J Gastroenterol. 2008;14(34):5282–9.
Krasman ML, Gracie WA, Strasius SR. Biliary tract disease in the aged. Clin Geriatr Med. 1991;7(2):347–70.
Tufo A, Pisano M, Ansaloni L, de Reuver P, van Laarhoven K, Davidson B, Gurusamy KS. Risk prediction in Acute Calculous Cholecystitis: a systematic review and Meta-analysis of prognostic factors and predictive models. J Laparoendosc Adv Surg Tech A. 2021;31(1):41–53.
Wu XD, Tian X, Liu MM, Wu L, Zhao S, Zhao L. Meta-analysis comparing early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg. 2015;102(11):1302–13.
Kuy S, Sosa JA, Roman SA, Desai R, Rosenthal RA. Age matters: a study of clinical and economic outcomes following cholecystectomy in elderly Americans. Am J Surg. 2011;201(6):789–96.
Lee SJ, Choi IS, Moon JI, Yoon DS, Lee SE, Sung NS, Kwon SU, Bae IE, Roh SJ, Choi WJ. Elective laparoscopic cholecystectomy is better than conservative treatment in Elderly patients with Acute Cholecystitis after Percutaneous Transhepatic Gallbladder Drainage. J Gastrointest Surg. 2021;25(12):3170–7.
van Heesewijk AE, Lammerts RGM, Haveman JW, Meerdink M, van Leeuwen BL, Pol RA. Outcome after cholecystectomy in the elderly. Am J Surg. 2019;218(2):368–73.
De la Serna S, Ruano A, Pérez-Jiménez A, Rojo M, Avellana R, García-Botella A, Pérez-Aguirre E, Diez-Valladares LI, Torres AJ. Safety and feasibility of cholecystectomy in octogenarians. Analysis of a single center series of 316 patients. HPB (Oxford). 2019;21(11):1570–6.
Endo I, Takada T, Hwang TL, Akazawa K, Mori R, Miura F, Yokoe M, Itoi T, Gomi H, Chen MF, et al. Optimal treatment strategy for acute cholecystitis based on predictive factors: Japan-Taiwan multicenter cohort study. J Hepatobiliary Pancreat Sci. 2017;24(6):346–61.
Yokoe M, Hata J, Takada T, Strasberg SM, Asbun HJ, Wakabayashi G, Kozaka K, Endo I, Deziel DJ, Miura F, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018;25(1):41–54.
Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–51.
Mayhew D, Mendonca V, Murthy BVS. A review of ASA physical status - historical perspectives and modern developments. Anaesthesia. 2019;74(3):373–9.
Lee JS, Lee SJ, Choi IS, Moon JI. Optimal timing of percutaneous transhepatic gallbladder drainage and subsequent laparoscopic cholecystectomy according to the severity of acute cholecystitis. Ann Hepatobiliary Pancreat Surg. 2022;26(2):159–67.
Wakabayashi G, Iwashita Y, Hibi T, Takada T, Strasberg SM, Asbun HJ, Endo I, Umezawa A, Asai K, Suzuki K, et al. Tokyo Guidelines 2018: surgical management of acute cholecystitis: safe steps in laparoscopic cholecystectomy for acute cholecystitis (with videos). J Hepatobiliary Pancreat Sci. 2018;25(1):73–86.
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, de Santibañes E, Pekolj J, Slankamenac K, Bassi C, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–96.
Jammer I, Wickboldt N, Sander M, Smith A, Schultz MJ, Pelosi P, Leva B, Rhodes A, Hoeft A, Walder B, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: european Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105.
Koch M, Garden OJ, Padbury R, Rahbari NN, Adam R, Capussotti L, Fan ST, Yokoyama Y, Crawford M, Makuuchi M, et al. Bile leakage after hepatobiliary and pancreatic surgery: a definition and grading of severity by the International Study Group of Liver surgery. Surgery. 2011;149(5):680–8.
Indar AA, Beckingham IJ. Acute cholecystitis. BMJ. 2002;325(7365):639–43.
Barie PS, Eachempati SR. Acute acalculous cholecystitis. Gastroenterol Clin North Am. 2010;39(2):343–57. x.
Stinton LM, Shaffer EA. Epidemiology of gallbladder disease: cholelithiasis and cancer. Gut Liver. 2012;6(2):172–87.
Parithivel VS, Gerst PH, Banerjee S, Parikh V, Albu E. Acute acalculous cholecystitis in young patients without predisposing factors. Am Surg. 1999;65(4):366–8.
Ryu JK, Ryu KH, Kim KH. Clinical features of acute acalculous cholecystitis. J Clin Gastroenterol. 2003;36(2):166–9.
Siegel JH, Kasmin FE. Biliary tract diseases in the elderly: management and outcomes. Gut. 1997;41(4):433–5.
Shaffer EA. Gallstone disease: epidemiology of gallbladder stone disease. Best Pract Res Clin Gastroenterol. 2006;20(6):981–96.
Tazuma S. Gallstone disease: epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best Pract Res Clin Gastroenterol. 2006;20(6):1075–83.
Murphy MM, Ng SC, Simons JP, Csikesz NG, Shah SA, Tseng JF. Predictors of major complications after laparoscopic cholecystectomy: surgeon, hospital, or patient? J Am Coll Surg. 2010;211(1):73–80.
Nikfarjam M, Yeo D, Perini M, Fink MA, Muralidharan V, Starkey G, Jones RM, Christophi C. Outcomes of cholecystectomy for treatment of acute cholecystitis in octogenarians. ANZ J Surg. 2014;84(12):943–8.
Park Y, Hwang DW, Lee JH, Song KB, Jun E, Lee W, Kwon J, Kim SC. Clinical outcomes of octogenarians according to preoperative disease severity and comorbidities after laparoscopic cholecystectomy for acute cholecystitis. J Hepatobiliary Pancreat Sci. 2020;27(6):307–14.
Pitt SC, ** LX, Hall BL, Strasberg SM, Pitt HA. Incidental gallbladder cancer at cholecystectomy: when should the surgeon be suspicious? Ann Surg. 2014;260(1):128–33.
Muszynska C, Nilsson J, Lundgren L, Lindell G, Andersson R, Sandström P, Andersson B. A risk score model to predict incidental gallbladder cancer in patients scheduled for cholecystectomy. Am J Surg. 2020;220(3):741–4.
Horkoff MJ, Ahmed Z, Xu Y, Sutherland FR, Dixon E, Ball CG, Bathe OF. Adverse outcomes after bile spillage in Incidental Gallbladder Cancers: a Population-based study. Ann Surg. 2021;273(1):139–44.
Acknowledgements
None.
Funding
This work was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIT) (No. 2022R1G1A1013072).
Author information
Authors and Affiliations
Contributions
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; all authors. Drafting the work or revising it critically for important intellectual content; Cho Eun Lee, Seung Jae Lee. Final approval of the version to be published; Cho Eun Lee, Seung Jae Lee. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved; Cho Eun Lee, Seung Jae Lee, In Seok Choi, and Ju Ik Moon.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Konyang University Hospital (IRB No. 2022-01-016), and the requirement for obtaining informed consent was waived owing to the retrospective study design.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lee, C.E., Lee, S.J., Moon, J.I. et al. Acute cholecystitis in old adults: the impact of advanced age on the clinical characteristics of the disease and on the surgical outcomes of laparoscopic cholecystectomy. BMC Gastroenterol 23, 328 (2023). https://doi.org/10.1186/s12876-023-02954-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-023-02954-6