
Abstract
Introduction
Collagenous colitis (CC) is a common cause of chronic diarrhea and is characterized by a subepithelial thickened collagen layer in the colonic mucosa.
It shares many of the characteristics found in autoimmune diseases, but no autoantibodies have been identified. In CC, an imbalance in collagen turnover is evident. The purpose of the present study was to investigate whether any collagen-associated autoantibodies or other antibodies such as TPO and ASCA were present, and if levels of total IgE were increased.
Methods
Sera from women with active CC were analysed with ELISA for detection of autoantibodies against collagen type III and IV (Col III and IV), matrix metalloproteinase-9 (MMP-9), tissue inhibitors of metalloproteinase-1 (TIMP-1) and tenascin-C (TNC). Sera were also analysed for TPO, ASCA and total IgE. Healthy female blood donors served as controls. The cut-off value in the control group was defined as relative units > 97.5th percentile.
Results
Sixty-six women were included (mean age 60 years; range 31–74, mean disease duration 6 years; range 1–22). No autoantibody was significantly overexpressed in the CC population compared to controls. The mean disease duration was lower (p = 0.03) in the subjects who expressed collagen-associated autoantibodies (3.7 years; range 1–14), compared to those who did not (6.4 years; range 1–22). Treatment with budesonide was not associated with any of these autoantibodies.
Conclusion
No increased presence of the investigated antibodies could be found in the present study of CC. Neither could antibodies against ASCA or TPO, or elevated levels of IgE, be found. Consequently, no association was found between CC and these proteins, even though this may not be generalizable to other compounds in the collagen layer.
Similar content being viewed by others


Introduction
Collagenous colitis (CC) is an inflammatory disorder in the colonic mucosa that predominantly affects elderly women and causes chronic, non-bloody diarrhoea with normal or close to normal endoscopic findings. The condition was first described 1976 in Malmö, Sweden, by Lindström [1]. The histological criteria for CC are a thickened subepithelial collagen layer (> 10 µm) in the extracellular matrix (ECM) of the mucosa, epithelial damage and presence of an inflammatory infiltrate in the lamina propria [2] (Fig. 1). The excessive subepithelial collagen deposition is located underneath the basement membrane and seems to be caused by myofibroblast dysfunction, leading to collagen overproduction with ECM-remodelling, as well as an imbalance between fibrogenesis and fibrinolysis which results in an impaired degradation of ECM proteins [3, 4].

Histological features of collagenous colitis. High magnification micrograph of collagenous colitis, H&E stain (Collagenous colitis—high mag—Collagenous colitis—Wikipedia) by Michael Bonert, MD, FRCPC. Copyright © 2011 Michael Bonert, MD, FRCPC (https://commons.wikimedia.org/wiki/User:Nephron / https://fhs.mcmaster.ca/pathology/contact_us/faculty/faculty_bios/Bonert.html. Licensed under CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0/legalcode)
Whether CC is an autoimmune disease is yet not clear, although some characteristics suggest an autoimmune association. First, patients with CC are to a large extent HLA DQ2-carriers, a HLA-haplotype associated with autoimmune diseases [5,6,7]. In line with this, celiac disease (CeD), thyroid disorders and other autoimmune diseases are often identified in patients with CC [8]. Second, an inflammatory Th1-dominated mucosal cytokine profile has been observed [9, 10]. Third, the disease is prevalent mainly in a certain age and gender group, something that is typical for autoimmune diseases in general [11, 12].
A typical prerequisite for a classical autoimmune disorder is presence of autoantibodies [13]. Previous studies have suggested an increased presence of some antibodies in patients with CC, such as anti-nuclear antibodies (ANA) [14,15,16], serum IgM [14], thyroid peroxidase (TPO) [16] and anti-Saccharomyces cerevisiae antibodies (ASCA) [15, 16]. However, the sensitivity of these antibodies is too low to be able to consider them as diagnostic tools in CC. Antibody response in autoimmunity is often mediated via IgG, but also other subclasses are involved. Increased total IgE levels have been reported in patients with inflammatory bowel disease (IBD) [17, 18].
While general autoantibodies such as ANA are present in many different types of autoimmune diseases, the majority of antibodies in autoimmune disease have a defined target organ directed against a key enzyme and/or substrate in that organ, such as in transglutaminase autoantibodies in CeD (transglutaminase and gliadin) and anti-citrullinated protein antibodies in rheumatoid arthritis (RA; peptidylarginine deiminase and citrulline) [19, 20]. The central mechanism is that these enzymes and their substrates are active and involved in the inflamed tissue, something that might increase the risk that these proteins also could be targets in the immune response. In other words, any presence of autoantibodies against central enzymes and their substrates should predominantly be found in the active site, i.e. where the inflammation is most active. In CC, a disrupted collagen turnover is evident. If the same mechanisms are present in CC as in CeD or RA, autoantibodies against active enzymes involved in collagen turnover could be expected.
Collagen
The thickened collagen layer in CC is believed to reflect a local disturbance of ECM turnover, resulting in the formation of a disrupted ECM. Previous studies have shown increased levels of collagen type III (Col III) [3, 21] and both Col III and collagen type IV (Col IV) [22] in patients with CC. Col IV is a major component of basement membrane collagens and Col III is active in wound healing [23, 24].
Matrix metalloproteinase (MMP)
MMP is a family of zinc-dependent enzymes involved in the degradation of different components of the ECM. These proteinases play a central role in tissue remodelling during inflammation [25]. The MMP genes are responsive to several factors including cytokines such as TNF alfa and IL-1 [26]. MMP-9 is involved in inflammatory and remodelling processes in IBD and its levels are elevated in patients with ulcerative colitis [25, 27,28,29,30]. An allelic variation of MMP-9 has been suggested as a risk factor [31], and enhanced mRNA expression levels of the gene has been described in CC-patients [32].
Tissue inhibitors of metalloproteinase (TIMP)
The activity of MMPs is regulated by TIMPs TIMPs are typically induced by inflammatory cytokines such as IL-6 that is related to the Th1 mediated pathway [33]. Previous studies have shown increased transcripts of TIMP-1 in patients with CC [3, 32].
Tenascin-C (TNC)
Tenascins are a family of four extracellular matrix glycoproteins TNC is expressed in wound healing and inflammation [34, 35]. TNC also interacts with MMPs [35]. Previous studies have shown that TNC is increased in the collagen layer in patients with CC [3, 4, 36, 37]. This glycoprotein is regulated by cytokines, and it seems as if both the Th1 (TNF, IL-1 and IFN) and the Th2 (IL-4 and IL-13) pathways are involved. Exogenous TNC stimulates collagen gene expression via TLR4 signaling [38] which induces a Th1-response [39].
In view of this aspect, we have primarily focused on the frequency of autoantibodies directed against specific endogenous proteins that are active in the turnover of the collagen layer in the intestinal mucosa in patients with CC, namely, Col III and Col IV, MMP-9, TIMP-1 and TNC. Furthermore, we have scrutinized the occurrence of other putative antibodies active in the immune-driven process behind CC, namely TPO and ASCA, and total levels of IgE.
Patients and methods
Patients
Patients with CC were diagnosed according to established clinical and histopathological criteria [40]. They were recruited from the out-patient clinics at the hospitals in Region Skåne. The procedure has been described in detail in a previous study [16].
To reassure that only patients with more pronounced and verified CC were included, only patients with at least two flare-ups or two histological examinations with positive findings in accordance to the histopathological criteria of CC were included. Patient characteristics (including clinical information) were retrieved from a questionnaire sent to the participants, and in some cases, completed with patient files. Blood samples were collected according to standardized methods.
Control group
Serum from healthy, female blood donors served as controls for all immunological analyses. The criteria for being a blood donor is strict and these individuals do not take any medication of relevance [41]. For the collagen-associated antibody-analyses, one hundred female blood donors served as controls. The size of the groups differed slightly due to shortage of blood samples, but they were all picked from the same cohort. Blood donors also served as controls for analyses of ASCA, TPO and total IgE, but these were selected by the Department of Immunology and Department of Clinical Chemistry at Skåne University Hospital, Malmö according to their standardized methods.
Immunological analyses
Collagen type III and IV
In-house enzyme-linked immunosorbent assays (ELISAs) were set up for analysis of anti-IgM and IgG antibodies against Col III and IV. The microtiter plates (82.158.001, Sarstedt, Nümbrecht, Germany) were coated with a recombinant Col III (Merck CC054 lot nr 2,861,783, 2,943,191) or Col IV (ab7536 lot no GR281135-14 Abcam, Cambridge, UK), 1 µg/mL in phosphate buffer saline (PBS), pH 7.4, pre-incubated 15 min in 50 °C, 100 µl/well in PBS or buffer only (to provide an internal blank). After overnight incubation at 4 °C the plates were washed three times with PBS with 0.05% Tween 20 (MP Biomedicals 02,194,724.5) (PBS-T) and blocked with 0.5% bovine serum albumin (A7030, Sigma) (BSA) in PBS-T. Dilutions of serum from patients and blood donors of 1:800 (IgG and IgM) and rabbit IgG anti-human Col III antibody (PA136061 lot no 2861783 Fisher Scientific, Göteborg Sweden) or Col IV antibody (ab6585 lot no GR322984-8, Abcam) in serial dilution (to construct a standard curve) with BSA in PBS-T were then added to the plates in triplicate (two wells coated with Col III or IV and one well coated with PBS) and incubated for 1 h at room temperature (RT). The washing procedure was repeated and deposition of autoantibodies directed to Col III and IV was detected using HRP-conjugated rabbit anti-human IgG or IgM (P0214 and P0216, respectively, DAKO Glostrup, Denmark), or goat anti-rabbit IgG (P0448, DAKO) appropriately diluted in PBS-T. To develop a color reaction, a tetramethylbenzidine (TMB) peroxidase substrate system (2-C) (KPL50-76-00, Gaitheraburg, USA) 1:1 was used. The absorbance at 450 nm was measured after 15 min of incubation at RT. Antibody levels are presented as relative units (RU) (absorbance values after subtracted background) and the concentration in each doublet is interpolated from the standard curve.
The cut-off value to determine presence of antibodies in the control group of 70 (Col III) and 51 (Col IV) healthy blood donors was defined as RU > 97.5th percentile.
The intra-assay correlation coefficient of variation (CV) of Col III IgG and IgM antibodies was 12.5% (n = 10) and 8.1% (n = 8), respectively, and inter-assay CV was 8.5% (n = 6) and 6.9% (n = 4), respectively. The intra-assay correlation CV of Col IV IgG and IgM antibodies was 6.6% and 3.2%, respectively (n = 6), and inter-assay CV was 13.5% and 6.2%, respectively (n = 10).
MMP-9 and Tenascin
Analyses of antibodies against MMP-9 and TNC were conducted by in-house ELISAs as previously described in detail [42]. Briefly, IgM-and IgG- antibodies against MMP-9 were analysed on microtiter plates (442,404, Nunc) coated with a recombinant MMP-9 (Pierce RP-75655 lot no. QA 1,951,751, Thermo Scientific, Rockford, IL, USA) in PBS-T or in PBS-T only. IgM and IgG autoantibodies against TNC were analysed on microtiter plates (442,404, Nunc, Roskilde, Denmark) coated with recombinant TNC (MBS1265425, Mybiosource, San Diego, CA, USA) in PBS-T, or in PBS-T only (to provide an internal blank), and incubated at 4 °C overnight. The absorbance at 450 nm was measured after 30 min of incubation at RT. Antibody levels are presented as RU, and the concentration in each doublet is interpolated from the standard curve. The cut-off value to determine presence of antibodies in the control group of 100 healthy blood donors was defined as RU > 97.5th percentile.
The intra-assay CV of MMP-9 IgM and IgG antibodies was 10.1% (n = 5) and 6.9% (n = 8), respectively, and inter-assay CV was 14% and 8.5%, respectively (n = 4). The intra-assay correlation CV of TNC IgM and IgG antibodies was 9.1% and 7.6%, respectively (n = 8), and inter-assay CV was 20.3% and 13.6%, respectively (n = 4).
TIMP-1
Another in-house ELISA was set up for analysis of IgM and IgG antibodies against TIMP-1. The microtiter plates (82.158.001 Sarstedt) were coated with a recombinant TIMP-1 (MBS8249878 lot no JA1F10A, MyBiosource, San Diego, USA) in Carbonate buffer pH 9.6 or buffer only (to provide an internal blank). After overnight incubation at 4 °C the plates were washed three times with PBS-T and blocked with 0.5% BSA (A7030, Sigma) in PBS-T. Dilutions of serum from patients and blood donors of 1:100 (IgG and IgM) or rabbit IgG anti-human TIMP-1 antibody (MBS2544120 lot no AC5441, MyBiosource) in serial dilution (to construct a standard curve) with BSA in PBS-T were then added to the plates in triplicate (two wells coated with TIMP-1 and one well coated with Carbonate buffer) and incubated for 1 h at RT. The washing procedure was repeated and deposition of autoantibodies directed to TIMP-1 was detected using HRP-conjugated rabbit anti-human IgG or IgM (DAKO P0214 and P0216 respectively), or goat anti-rabbit IgG (P0448, DAKO) appropriately diluted in PBS-T. To develop a color reaction, a TMB Peroxidase substrate system (2-C) (50-76-00 KPL) 1:1 was used. The absorbance at 450 nm was measured after 30 min of incubation at RT. Antibody levels are presented as RU and the concentration in each doublet is interpolated from the standard curve.
The cut-off value to determine presence of antibodies in the control group of 65 healthy blood donors was defined as RU > 97.5th percentile.
The intra-assay CV of TIMP-1 IgG and IgM antibodies was 5.1% and 22%, respectively (n = 8), and inter-assay CV was 18% and 8.6%, respectively (n = 10).
ASCA, TPO and total IgE
ASCA and total IgE were both analysed at the Department of Immunology at Skåne University Hospital, Malmö. ASCA IgG were analysed by a fluorescent enzyme immunoassay method (FEIA) for which the reference value is set > 10 U/mL in accordance with the manufacturer’s recommendation (Orgentec Diagnostika, AlegriaH, Mainz, Germany). Of 50 healthy blood donors tested at our laboratory, 10% were positive for ASCA IgG, whereas other studies have found 0.6%–3.1% positive among healthy blood donors by the same method [43]. Total IgE were also analysed by FEIA method. The cut-off value to determine increased titers of total IgE was set to > 129 kU/L. Out of 100 healthy blood donors, 14% had increased titers at our laboratory.
TPO antibodies were analysed by a chemiluminescence enzyme immunological method (Atellica IM, Siemens Healthcare GmbH, Erlangen, Germany) at the Department of Clinical Chemistry at Skåne University Hospital, Malmö. TPO antibodies are found in 10% of blood donors when the cut-off level is set to 60 kIU/L.
Statistical analyses
Fisher’s exact test was used to calculate differences in antibody prevalence between controls and patients. Student’s t-test was used to calculate differences between mean values of continuous variables. A p-value < 0.05 was considered statistically significant.
Results
Patient characteristics
In total, 66 women with CC were included in the study. The mean age at inclusion was 60 years (range 31–74 years) and mean age at diagnosis was 55 years (range 28–69 years). At inclusion, the mean symptom duration was 11 years and mean disease duration was 6 years. More than one-third of the patients were smokers, and another third were former smokers. The most common concomitant diseases were hypertension (30%), RA (15%) and asthma and cancer (14%). Budesonide was used by 38% of the patients, and high blood pressure therapy (HBPT), proton pump inhibitors (PPI) and levothyroxine were used in 20–30% of patients (Table 1).
Control group
The size of the control groups differed but they were selected from the same cohort consisting of 100 healthy female blood donors. The mean age of the total control group was 41.7 years (range 19–69).
Presence of antibodies
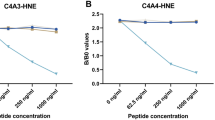
Levels of IgM and IgG autoantibodies against Col III, Col IV, MMP-9, TIMP-1 and TNC are illustrated in Fig. 2a–e. There was no difference in prevalence of these collage-associated autoantibodies between CC patients and controls (Fig. 3a). Sixteen patients expressed one type of autoantibody, whereas two patients expressed two different types. The mean disease duration was significantly lower (p = 0.03) in the subjects who expressed collagen-associated autoantibodies (3.7 years), compared to those who did not (6.4 years). Treatment with budesonide was not associated with any of these autoantibodies and no difference in prevalence of autoimmune/immune-mediated diseases between the two groups were seen (Table 2).

Levels of collagen-associated antibodies in patients with collagenous colitis and controls. Col III = collagen type III, Col IV = collagen type IV, MMP-9 = matrix metalloproteinase-9, TIMP-1 = tissue inhibitors of metalloproteinases-1, TNC = tenascin-C. CC = collagenous colitis (n = 66); treated = current budesonide treatment, controls = healthy blood donors (n = a 70, b 51, c 100, d 65, e 100). Black bars state median values. Y axis: Antibody levels in relative units (RU) (absorbance values after subtracted background). Cut-off value set at the 97.5 th percentile. Fischer's exact test was used to calculate the differences between controls and CC pat (including both treated and untreated)

a Presence of collagen-associated autoantibodies. Col III = collagen type III, Col IV = collagen type IV, MMP-9 = matrix metalloproteinase-9, TIMP-1 = tissue inhibitors of metalloproteinases-1, TNC = tenascin-C, CC = collagenous colitis. Relative units > 97.5 percentile in a cohort of healthy blood donors were considered as presence of antibodies. Controls consisted of α = 70, β = 51, γ = 100, δ = 65 healthy blood donors. Fischer's exact test was used to calculate the differences between groups. None of the differences between groups were statistically significant (P < 0.05). b Presence of antibodies against saccharomyces cerevisiae (ASCA), thyroid peroxidase (TPO) and increased total serum IgE. CC = Collagenous colitis. Controls consisted of α = 50 healthy blood donors, β = 254 healthy blood donors, γ = 100 healthy blood donors. Fischer's exact test was used to calculate the differences between groups. None of the differences between groups were statistically significant (P < 0.05)
The presence of autoantibodies against TPO and ASCA was slightly increased compared to controls, but not statistically significant (Fig. 3b) (p-values 0.78 and 0.36, respectively). Out of the nine TPO positive patients, six did neither declare thyroid disease nor levothyroxine treatment. However, when comparing the levels of the TPO titers between patients that were treated with levothyroxine/declared thyroid disease with those who did not, no differences were observed (data not shown).
Increased levels of total IgE were not more present in the CC patients than in the control group (p-value 1.00) and there could not be observed any correlation between total IgE-positivity and presence of any autoantibodies (data not shown).
Discussion
The present study has not been able to identify presence of autoantibodies against Col III, Col IV, MMP-9, TIMP-1 or TNC to a larger extent in CC patients compared to healthy blood donors. In accordance with this, the presence of antibodies against TPO, ASCA as well as the levels of total IgE did not differ significantly from what could be expected in the background population. Even though we have tried to select specific antigens of relevance for CC there are a large number of other possible candidates.
Potential autoantigens
Since Col III and IV seem to be crucial in the collagen turnover in CC and it would have been logical if they had been involved in development of autoantibodies. However, previous studies have also shown increased presence of both collagen type I and VI in the tissue [3, 36] as well as increased transcripts of procollagen type I and IV [26] in patients with CC. Increased presence as well as degradation of collagen type I is also described in Crohn’s disease [44] which make these collagens possible candidates for future studies.
A pathogenetic role of MMP-9 could have been plausible, since this MMP seem to be active in CC. Despite these circumstances we could not find any increased presence of autoantibodies against MMP-9. However, several different MMP types are involved in collagen turnover and autoantibodies could be directed towards other MMPs, most likely against MMP-1, -2, -8, -13 and -18, since they all degrade collagen [45]. In CC, the expression of MMP-1, 7 or 13 was not elevated, thus indicating that development of autoantibodies against these structures is less probable [3, 31].
Despite that both TIMP-1 and TNC seem to be active players in the pathogenic process in CC, no autoantibodies against these glycoproteins could be found.
Even though there was no association between CC and the collagen-associated autoantibodies, the autoantibody-positive patients had a significant shorter disease duration compared to those without autoantibodies. This subgroup did not have more concomitant diseases. Instead, this may be explained by a general increased immunological activation at the time of disease onset, which can cause development of non-disease-specific autoantibodies that can still be detected a few years after onset. As time goes by, a decrease in circulating antibodies may reflect an contemporary decrease in non-specific immune activation, something that has previously been described in CeD [46]. In conclusion, autoantibody prevalence reflects time from disease onset.
CC and thyroid diseases are related to each other, which in this study can be confirmed by the higher levothyroxine consumption among the CC patients (20%). This can be compared with 10–12% which is the proportion levothyroxine consumers among all women between 55 and 64 years in Skåne [47]. Despite this, no significant increase in occurrence of TPO antibodies could be observed in CC in the present study. This is in line with a previous investigation from our group [16]. The difference in design in the present compared to the former study [16] was that the present cohort consisted of cases with verified two flare-ups or two histological specimens indicating a more active and continuous disease. However, this did not make any difference in the results. Somewhat surprising, two thirds of those with CC that had positive TPO neither declared thyroid disease nor levothyroxine consumption. Positive TPO has been described as an early predictor of hypothyroidism so it is plausible that some of these individuals may develop thyroid disorder within a few years [48].
Even though previous studies indicated a possible association between CC and ASCA, we could not find any increased frequency in the present cohort. ASCA is observed in Crohn’s disease [49], which is a disease with a more severe disease course with organ damage. The different clinical characteristics could indicate a different pathogenetic background, something that could explain the negative results in CC.
Despite the increased levels of total IgE in IBD [17, 18], there was no such increase in CC. Different mechanisms are probably at hand in the different diseases.
Even though MC is driven by a Th1-dominated cellular immune response [10], the local symptoms and the low frequency of extra-intestinal manifestations indicate that the systemic immunological impact in MC is significantly lower than in other immune-driven diseases in the same organ system, such as classical IBD. In tissue samples activation of genes involved in presentation of luminal antigens to bacteria and viruses has been found. A bacterial origin for CC could thus be contemplated (51). Furthermore, the only effective treatment, budesonide, mediates its effect locally in the large intestine, while systemic corticosteroid treatment has lower impact. Consequently, in CC, inflammatory markers may only be seen in the intestinal wall rather than in the systemic circulation. On the other hand, MC is related to coeliac disease where the inflammatory activity is present locally in the intestine, but systemic antibodies are still present.
To the best of our knowledge, this is the first study that has investigated autoantibody prevalence against defined structures in the collagen layer in patients with CC. No such association could be found. Furthermore, the prevalence of antibodies against ASCA and TPO and the levels of total IgE were not increased. This talks against any autoimmune pathogenetic mechanism based on these structures. On the other hand, the many autoimmune features found in CC are still apparent why the possibility of an autoimmune pathogenesis via other antigens cannot yet be ruled out.
Strengths and limitations
A strength of this study was that the cohort consisted of 66 women with verified active and pronounced disease that demonstrated the typical characteristics for CC patients in general, i.e., postmenopausal age of disease onset, an increased number of smokers and concomitant autoimmune disorders [8, 12]. The controls were not age matched. However, since the cut-off value to assess presence of antibodies in the CC patients was determined from a control group, this selection of individuals must come from a healthy cohort, otherwise there is a risk of a type II error. In contrast, in a control group consisting of older women that commonly are affected by inflammatory diseases/processes, there would have been an increased risk of presence of autoantibodies [11]. The sample size in this study was rather small. However, if any autoantibody should have any relevance, at least a significant minority ought to have it. The strict selection of this homogenous group should have increased the probability to identify any type of antibody but failed to do so, which increases the likelihood that our results are generalizable. Five individuals with CC and levothyroxine consumption declared neither thyroid dysfunction nor medication in the questionnaires, something that highlights the weakness with questionnaires without possibilities to validate the outcome.
Conclusion
In conclusion, Col III, Col IV, MMP-9, TIMP-1 or TNC are all proteins related to the collagen layer and its turnover and could thus have been expected to be targets for an immunological reaction and thereby prove that CC is of an autoimmune origin. Such autoantibodies could also have served as a diagnostic tool. Nevertheless, no increased presence of these autoantibodies could be found in the present study of CC. Neither could antibodies against ASCA or TPO, or elevated levels of IgE, be found. Consequently, no association was found between CC and these proteins, even though this may not be generalizable to other compounds in the collagen layer.
Availability of data and materials
The datasets generated and analysed during the current study are not publicly available due to a rather extensive amount of data files of which some furthermore requires some explanations, but will be available from the corresponding author on reasonable request.
Abbreviations
- ANA:
-
Anti-nuclear antibodies
- ASCA:
-
Anti-Saccharomyces cerevisiae antibodies
- BSA:
-
Ovine serum albumin
- CC:
-
Collagenous colitis
- CeD:
-
Celiac disease
- ColIII:
-
Collagen type III
- ColIV:
-
Collagen type IV
- CV:
-
Coefficient of variation
- ECM:
-
Extracellular matrix
- ELISA:
-
Enzyme-linked immunosorbent assay
- FEIA:
-
Fluorescent enzyme immunoassay
- HBPT:
-
High blood pressure therapy
- IBD:
-
Inflammatory bowel disease
- MMP:
-
Matrix metalloproteinase
- PBS:
-
Phosphate buffer saline
- PBS-T:
-
Phosphate buffer saline with 0.05% Tween 20
- PPI:
-
Proton pump inhibitor
- RA:
-
Rheumatoid arthritis
- RT:
-
Room temperature
- RU:
-
Relative units
- TIMP:
-
Tissue inhibitors of metalloproteinase
- TMB:
-
Tetramethylbenzidine
- TNC:
-
Tenascin-C
- TPO:
-
Thyroid peroxidase
References
Lindstrom CG. “Collagenous colitis” with watery diarrhoea–a new entity? Pathol Eur. 1976;11(1):87–9.
Miehlke S, Guagnozzi D, Zabana Y, Tontini GE, Kanstrup Fiehn AM, Wildt S, et al. European guidelines on microscopic colitis: United European gastroenterology and European microscopic colitis group statements and recommendations. United Eur Gastroenterol J. 2021;9(1):13–37.
Gunther U, Schuppan D, Bauer M, Matthes H, Stallmach A, Schmitt-Graff A, et al. Fibrogenesis and fibrolysis in collagenous colitis. Patterns of procollagen types I and IV, matrix-metalloproteinase-1 and -13, and TIMP-1 gene expression. Am J Pathol. 1999;155(2):493–503.
Salas A, Fernandez-Banares F, Casalots J, Gonzalez C, Tarroch X, Forcada P, et al. Subepithelial myofibroblasts and tenascin expression in microscopic colitis. Histopathology. 2003;43(1):48–54.
Fine KD, Do K, Schulte K, Ogunji F, Guerra R, Osowski L, et al. High prevalence of celiac sprue-like HLA-DQ genes and enteropathy in patients with the microscopic colitis syndrome. Am J Gastroenterol. 2000;95(8):1974–82.
Koskela RM, Karttunen TJ, Niemela SE, Lehtola JK, Ilonen J, Karttunen RA. Human leucocyte antigen and TNFalpha polymorphism association in microscopic colitis. Eur J Gastroenterol Hepatol. 2008;20(4):276–82.
Westerlind H, Mellander MR, Bresso F, Munch A, Bonfiglio F, Assadi G, et al. Dense genoty** of immune-related loci identifies HLA variants associated with increased risk of collagenous colitis. Gut. 2017;66(3):421–8.
Vigren L, Tysk C, Strom M, Kilander AF, Hjortswang H, Bohr J, et al. Celiac disease and other autoimmune diseases in patients with collagenous colitis. Scand J Gastroenterol. 2013;48(8):944–50.
Park EK, Park YS, Park DR, Jung SA, Han DS, Jang BI, et al. Cytokine expression of microscopic colitis including interleukin-17. Gut Liver. 2015;9(3):381–7.
Tagkalidis PP, Gibson PR, Bhathal PS. Microscopic colitis demonstrates a T helper cell type 1 mucosal cytokine profile. J Clin Pathol. 2007;60(4):382–7.
Goronzy JJ, Weyand CM. Immune aging and autoimmunity. Cell Mol Life Sci: CMLS. 2012;69(10):1615–23.
Larsson JK, Sonestedt E, Ohlsson B, Manjer J, Sjoberg K. The association between the intake of specific dietary components and lifestyle factors and microscopic colitis. Eur J Clin Nutr. 2016;70(11):1309–17.
Witebsky E, Rose NR, Terplan K, Paine JR, Egan RW. Chronic thyroiditis and autoimmunization. J Am Med Assoc. 1957;164(13):1439–47.
Bohr J, Tysk C, Yang P, Danielsson D, Jarnerot G. Autoantibodies and immunoglobulins in collagenous colitis. Gut. 1996;39(1):73–6.
Holstein A, Burmeister J, Plaschke A, Rosemeier D, Widjaja A, Egberts EH. Autoantibody profiles in microscopic colitis. J Gastroenterol Hepatol. 2006;21(6):1016–20.
Roth B, Gustafsson RJ, Ohlsson B. Auto-antibodies and their association with clinical findings in women diagnosed with microscopic colitis. PLoS ONE. 2013;8(6):e66088.
D’Arienzo A, Manguso F, Astarita C, D’Armiento FP, Scarpa R, Gargano D, et al. Allergy and mucosal eosinophil infiltrate in ulcerative colitis. Scand J Gastroenterol. 2000;35(6):624–31.
Levo Y, Shalit M, Wollner S, Fich A. Serum IgE levels in patients with inflammatory bowel disease. Ann Allergy. 1986;56(1):85–7.
Roth EB, Sjöberg K, Stenberg P. Biochemical and immuno-pathological aspects of tissue transglutaminase in coeliac disease. Autoimmunity. 2003;36(4):221–6.
Roth EB, Stenberg P, Book C, Sjöberg K. Antibodies against transglutaminases, peptidylarginine deiminase and citrulline in rheumatoid arthritis–new pathways to epitope spreading. Clin Exp Rheumatol. 2006;24(1):12–8.
Flejou JF, Grimaud JA, Molas G, Baviera E, Potet F. Collagenous colitis ultrastructural study and collagen immunoty** of four cases. Arch Pathol Lab Med. 1984;108(12):977–82.
Mori S, Kadochi Y, Luo Y, Fujiwara-Tani R, Nishiguchi Y, Kishi S, et al. Proton pump inhibitor induced collagen expression in colonocytes is associated with collagenous colitis. World J Gastroenterol: WJG. 2017;23(9):1586–93.
Randles MJ, Humphries MJ, Lennon R. Proteomic definitions of basement membrane composition in health and disease. Matrix Biol. 2017;57–58:12–28.
Stumpf M, Krones CJ, Klinge U, Rosch R, Junge K, Schumpelick V. Collagen in colon disease. Hernia. 2006;10(6):498–501.
Lakatos G, Sipos F, Miheller P, Hritz I, Varga MZ, Juhasz M, et al. The behavior of matrix metalloproteinase-9 in lymphocytic colitis, collagenous colitis and ulcerative colitis. Pathol Oncol Res. 2012;18(1):85–91.
Medina C, Radomski MW. Role of matrix metalloproteinases in intestinal inflammation. J Pharmacol Exp Ther. 2006;318(3):933–8.
Annaházi A, Molnár T, Farkas K, Rosztóczy A, Izbéki F, Gecse K, et al. Fecal MMP-9: a new noninvasive differential diagnostic and activity marker in ulcerative colitis. Inflamm Bowel Dis. 2013;19(2):316–20.
Bai X, Bai G, Tang L, Liu L, Li Y, Jiang W. Changes in MMP-2, MMP-9, inflammation, blood coagulation and intestinal mucosal permeability in patients with active ulcerative colitis. Exp Ther Med. 2020;20(1):269–74.
Baugh MD, Perry MJ, Hollander AP, Davies DR, Cross SS, Lobo AJ, et al. Matrix metalloproteinase levels are elevated in inflammatory bowel disease. Gastroenterology. 1999;117(4):814–22.
Jakubowska K, Pryczynicz A, Iwanowicz P, Niewiński A, Maciorkowska E, Hapanowicz J, et al. Expressions of matrix metalloproteinases (MMP-2, MMP-7, and MMP-9) and their inhibitors (TIMP-1, TIMP-2) in inflammatory bowel diseases. Gastroenterol Res Pract. 2016;2016:2456179.
Madisch A, Hellmig S, Schreiber S, Bethke B, Stolte M, Miehlke S. Allelic variation of the matrix metalloproteinase-9 gene is associated with collagenous colitis. Inflamm Bowel Dis. 2011;17(11):2295–8.
Liu Q, Harpaz N. Expression profiling of inflammatory and immunological genes in collagenous colitis. J Crohns Colitis. 2019;13(6):764–71.
Bokarewa M, Dahlberg L, Tarkowski A. Expression and functional properties of antibodies to tissue inhibitors of metalloproteinases (TIMPs) in rheumatoid arthritis. Arthritis Res Ther. 2005;7(5):R1014–22.
Chiquet-Ehrismann R, Chiquet M. Tenascins: regulation and putative functions during pathological stress. J Pathol. 2003;200(4):488–99.
Jones FS, Jones PL. The tenascin family of ECM glycoproteins: structure, function, and regulation during embryonic development and tissue remodeling. Dev Dyn. 2000;218(2):235–59.
Aigner T, Neureiter D, Muller S, Kuspert G, Belke J, Kirchner T. Extracellular matrix composition and gene expression in collagenous colitis. Gastroenterology. 1997;113(1):136–43.
Müller S, Neureiter D, Stolte M, Verbeke C, Heuschmann P, Kirchner T, et al. Tenascin: a sensitive and specific diagnostic marker of minimal collagenous colitis. Virchows Arch. 2001;438(5):435–41.
Bhattacharyya S, Wang W, Morales-Nebreda L, Feng G, Wu M, Zhou X, et al. Tenascin-C drives persistence of organ fibrosis. Nat Commun. 2016;7:11703.
Manicassamy S, Pulendran B. Modulation of adaptive immunity with Toll-like receptors. Semin Immunol. 2009;21(4):185–93.
Munch A, Aust D, Bohr J, Bonderup O, Fernandez Banares F, Hjortswang H, et al. Microscopic colitis: current status, present and future challenges: statements of the European microscopic colitis group. J Crohns Colitis. 2012;6(9):932–45.
GeBlod.nu 23rd Feb 2022. Available from: https://geblod.nu/fragor-och-svar/kan-jag-ge-blod-om-jag-ater-mediciner/. 2022.
Ek M, Roth B, Valentin L, Nordengren J, Ohlsson B. Autoantibodies common in patients with gastrointestinal diseases are not found in patients with endometriosis: a cross-sectional study. Eur J Obstet Gynecol Reprod Biol. 2019;240:370–4.
Mankaï A, Sakly W, Thabet Y, Achour A, Manoubi W, Ghedira I. Anti-Saccharomyces cerevisiae antibodies in patients with systemic lupus erythematosus. Rheumatol Int. 2013;33(3):665–9.
Kjeldsen J, de Muckadell OBS, Junker P. Seromarkers of collagen I and III metabolism in active Crohn’s disease. Relation to disease activity and response to therapy. Gut. 1995;37(6):805–10.
Visse R, Nagase H. Matrix metalloproteinases and tissue inhibitors of metalloproteinases: structure, function, and biochemistry. Circ Res. 2003;92(8):827–39.
Ventura A, Neri E, Ughi C, Leopaldi A, Città A, Not T. Gluten-dependent diabetes-related and thyroid-related autoantibodies in patients with celiac disease. J Pediatr. 2000;137(2):263–5.
The Swedish Prescribed Drug Register Stockholm: Socialstyrelsen; 29th Sept 2021. Available from: https://www.socialstyrelsen.se/statistik-och-data/statistik/statistikdatabasen/. 2021.
Prummel MF, Wiersinga WM. Thyroid peroxidase autoantibodies in euthyroid subjects. Best Pract Res Clin Endocrinol Metab. 2005;19(1):1–15.
Main J, McKenzie H, Yeaman GR, Kerr MA, Robson D, Pennington CR, et al. Antibody to saccharomyces cerevisiae (bakers’ yeast) in Crohn’s disease. BMJ. 1988;297(6656):1105–6.
Acknowledgements
Not applicable.
Funding
Open access funding provided by Lund University. We want to thank Lund University and Sweden’s Southern Healthcare Region for financial support. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Author information
Authors and Affiliations
Contributions
Conceptualization, JKL, BR and KS; methodology, JKL, BR, BO and KS; validation, JKL, BR, BO, KS; formal analysis, JKL and BR; investigation, JKL, BR, BO and KS; resources, JKL and KS; data curation, JKL, BR, BO and KS; writing—original draft preparation, JKL and KS; writing—review and editing, JKL, BR, BO and KS; visualization, JKL and KS; supervision, BO and KS; project administration, JKL, BR, BO and KS; funding acquisition, KS. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Regional Ethical Committees in Lund (2009/565 and 2011/209) and Stockholm (2016/271-31/1). All participants provided written informed consent to participate in the study. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
JK, L., B, R., B, O. et al. Lack of autoantibodies against collagen and related proteins in collagenous colitis. BMC Immunol 23, 29 (2022). https://doi.org/10.1186/s12865-022-00504-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12865-022-00504-5