
Abstract
Background
Benign prostatic enlargement (BPE) and lower urinary tract symptoms (LUTS) are pro-inflammatory cytokine interleukin-8 (IL-8)-associated which causes epithelial hyperplasia of the prostate transitional zone. This study aimed to determine the correlation between the levels of IL-8 serum and the prostate volume with the degree of LUTS severity in patients with BPE.
Methods
Determination of the correlation between serum IL-8 levels and prostate volume with the LUTS severity degree was conducted using a cross-sectional approach. The International Prostate Symptom Score was used to measure the LUTS severity degree, the enzyme-linked immunosorbent assay (ELISA) technique was used to measure the serum IL-8 level, and the transabdominal ultrasonography (TAUS) was used to measure the prostate volume. The sample used in this study was 32 patients with BPE grouped by the degree of LUTS severity of the patients. The correlation between variables was then analyzed using the Pearson correlation test.
Results
The prostate volume was higher in severe LUTS degree (38.19 cc) than in the mild LUTS degree (13.05 cc). The levels of serum IL-8 were higher in the severe LUTS degree (21.65 pg/mL) than in the mild LUTS degree (8.44 pg/m). Both the levels of serum IL-8 and the degree of LUTS did not have a significant correlation with the volume of prostate (p > 0.05). On the other side, the prostate volume and the degree of LUTS severity had a significant positive correlation (p = 0.001, R = 0.913).
Conclusion
The prostate volume and the levels of serum IL-8 are higher in the severe LUTS degree. There is a trend of increasing prostate volume with the severity of LUTS symptoms and higher serum IL-8 levels. The severity of prostate enlargement can be assessed by measuring the levels of IL-8 in the serum.
Similar content being viewed by others


1 Background
Benign prostatic enlargement (BPE) is a non-malignant enlarged prostate gland that describes a stromal epithelium and gland hyperplasia in the prostate transitional zone. The histological increase in prostate volume, which characterizes BPE, is caused by a disruption in the balance between cell proliferation and cell death, thus favoring cell proliferation. Histopathologically, this process can lead to the accumulation of stromal and epithelial cells in the periurethral area of the prostate [1,2,3].
The pathogenesis of BPE is closely associated with the inflammatory process. In this condition, T and B lymphocytes and macrophages significantly infiltrate the tissue, causing hyperplasia within the prostate. Additionally, the elevation in levels of pro-inflammatory cytokines secreted exacerbates the inflammatory response [4]. Prostate stromal cells play a crucial role by stimulating CD4 + lymphocytes and producing pro-inflammatory cytokines and chemokines, including stromal-derived Interleukin-8 (IL-8). IL-8 and its receptors are predominant in inducing inflammation in the prostate’s transitional zone, contributing to gland hypertrophy and enlargement. IL-8 directly influences epithelial and stromal proliferation by generating various chemokines, such as the CXC group, which attract immune cells into prostate tissue. These recruited inflammatory cells secrete multiple cytokines, stimulating chemokine production by stromal cells, thereby contributing to prostate cell proliferation and the development of BPE [5,6,7]. By promoting senescent epithelial cell proliferation and the development of a reactive myofibroblast phenotype and indirectly by increasing the production of fibroblast growth factor 2 (FGF-2), IL-8 enhances the overgrowth of prostatic stromal and epithelial cells. The lymphomononuclear cells of prostate gland expressing CXCR1 and CXCR2 receptors attract IL-8, which directly stimulates prostate cell proliferation through autocrine and endocrine effects, and indirectly through the production of FGF-2. Consequently, IL-8 is a crucial link between the T-cell-mediated inflammatory response and cell proliferation in the etiology of BPE [8].
Lower urinary tract symptoms (LUTS) are common in older men and are often associated with BPE. These symptoms can be classified into two categories: obstructive symptoms (voiding symptoms) and irritative symptoms (storage symptoms). Obstructive symptoms arise from urethral constriction attributed to prostatic enlargement, resulting in urinary difficulties, diminished flow, and incomplete bladder emptying. Conversely, irritative symptoms stem from the detrusor muscle in the bladder exhibiting frequent contractions, even when the bladder is not fully distended, and thus can manifest as urgency, frequency, and urinary incontinence [5]. The International Prostate Symptom Score (IPSS) is commonly used to measure the degree of LUTS severity in patients with BPE. The IPSS assesses the severity of symptoms in patients with BPE on a scale ranging from 0 to 35. Scores between 0 and 7 indicate mild symptoms, scores between 8 and 19 indicate moderate symptoms, and scores between 20 and 35 indicate severe symptoms [9, 10].
Previous research by Al-Barzinji showed an increase in IL-8 in patients with BPE. According to a study by Smith et al., PMN and monocyte infiltration may cause potential chronic inflammation in the transitional zone of the prostate through an increase in chemokine and chemokine receptor levels, with a preponderance of IL-8 in the BPE. Augmented IL-8 levels correlate with heightened prostatic epithelial and stromal cells proliferation outside the prostate. The urethral constriction effect is associated with the expansion of prostatic epithelial and stromal cells in patients with BPE. Hence, elevated IL-8 levels in patients are directly associated with the degree of LUTS severity experienced [6, 7]. However, prior research has yet to thoroughly clarify the combined effect of prostate volume and IL-8 on the degree of LUTS severity in patients diagnosed with BPE. Therefore, this study aimed to determine the correlation between serum IL-8 levels and prostate volume on the severity degree of LUTS in patients with benign prostatic enlargement.
2 Methods
2.1 Study design
In order to determine the correlation between serum IL-8 levels and prostate volume on the severity degree of lower urinary tract symptoms (LUTS), this study used a cross-sectional approach. Approval for this study was granted by our institution’s Health Research Ethics Commission under protocol number 491/UN4.6.4.5.31/PP36/2022. All patients provided their consent prior to participating in the study.
2.2 Population and study setting
The study enrolled patients diagnosed with benign prostatic enlargement from the urology outpatient clinic of our institution between August and October 2022. Serum IL-8 levels were evaluated at the Clinical Pathology Laboratory within our institution. The study population comprised all patients seeking outpatient care at our institution’s urology outpatient clinic. All patients diagnosed with benign prostatic enlargement by urologists who met the following inclusion criteria: newly registered male outpatients aged 40 years or older, who consented to participate by providing signed informed consent, had no history of medication use related to LUTS complaints, were not catheterized, had IPSS scoring based on medical history, and underwent transabdominal ultrasound for prostate volume measure. Exclusion criteria were patients who had undergone invasive therapeutic interventions for benign prostatic enlargement, including transurethral resection or laser prostatectomy, afflicted with urethral strictures or neurogenic bladder, and with serum samples exhibiting lipemia or lysis, rendering resampling unfeasible.
2.3 Variable
Serum IL-8 levels and prostate volume were independent variables in this study, whereas the degree of LUTS was the dependent variable. The diagnosis of BPE was established through a comprehensive assessment involving medical history, physical examination (including digital rectal palpation), and transabdominal ultrasound (TAUS). In the current study context, the term of benign prostatic enlargement was considered more appropriate than the term benign prostatic hyperplasia, given that the diagnosis was not confirmed through histological examination of the patient’s prostate tissue. This approach was adopted to uphold scientific rigor and accuracy in the diagnostic process [11].
Interleukin (IL)-8 is a pro-inflammatory protein synthesized by various cells, including neutrophils, macrophages, endothelial cells, and cancer cells. It induces chemotaxis, degranulation, and the generation of superoxide and hydrogen peroxide (H2O2) in polymorphonuclear cells. Moreover, IL-8 triggers an inflammatory response, resulting in the proliferation of both prostate stromal and epithelial cells.
Prostate volume is a prostate size measured by transabdominal ultrasound (TAUS) and presented in cc. Recent studies have proposed TAUS as a preferable examination method over transrectal ultrasound (TRUS) due to its widespread availability and enhanced patient comfort. Furthermore, TAUS has demonstrated comparable accuracy to magnetic resonance imaging (MRI) examinations [12]. Additionally, TAUS and TRUS have demonstrated similar accuracy in detecting enlarged prostate volume, making TAUS a valuable alternative to TRUS in clinical practice [13]. Lower urinary tract symptoms (LUTS) refer to a range of obstructive and irritative symptoms affecting the lower urinary tract. These symptoms are often assessed using the International Prostate Symptom Score (IPSS), a standardized scoring system.
2.4 Serum IL-8 levels measurement
Serum IL-8 levels were quantified using the Human IL-8 ELISA Kit from MyBioSource (USA), employing the enzyme-linked immunosorbent assay (ELISA) technique. The assay utilized a sandwich approach, with 96-well plates pre-coated with the capture antibody. Biotin-conjugated detection antibodies were then added. Following the addition of standards, test samples, and detection antibodies, the wells were washed with a wash buffer to remove unbound conjugate. HRP–streptavidin was subsequently added, and the HRP enzymatic reaction was visualized using a TMB substrate. The catalysis of TMB by HRP produced a blue product, which turned yellow upon exposure to an acidic stop solution. The density of the yellow color varied according to the number of sample targets captured on the plate. The target concentration was determined by measuring the optical density (O.D) using a microplate reader at 450 nm. The reference range for serum IL-8 levels was 2.84–16.5 pg/mL.
2.5 Prostatic volume measurement
The prostate volume data from the participants were obtained from the results of a transabdominal ultrasound examination conducted by the attending radiologist. The prostate volume values were expressed in cubic centimeters (cc).
2.6 Classification of LUTS severity
Lower urinary tract symptoms scoring was assessed using the International Prostatic Symptom Score through patient interviews. The interpretation of IPSS by the World Health Organization (WHO) ranges from 0 to 7 for mild symptoms, 8–19 for moderate symptoms, and 20–35 for severe symptoms.
2.7 Sampling size and method
A purposive sampling method was utilized to select study samples. The normogram approach developed by Harry King was employed to determine the sample size. The population size in this study was assumed to be 30, with a 5% error rate (95% confidence level). The calculated percentage of the sample size in this study was 89%. Consequently, the minimum number of samples required for all groups (mild, moderate, and severe degrees of LUTS in this study was 32.
2.8 Data analysis
The obtained data were analyzed using SPSS version 25. Statistical analysis involved frequency distribution and descriptive statistical calculations. The Kolmogorov–Smirnov test was employed to assess the normal distribution of the data, with a significance level set at p > 0.05. Additionally, three hypothesis tests were conducted: Mann–Whitney, Independent-T, and Spearman’s correlation. Results with a p-value less than 0.05 were deemed statistically significant.
3 Results
3.1 Characteristics of participants
The study, conducted between August and October 2022, enrolled 32 subjects diagnosed with BPE who met the inclusion criteria. The participants’ ages ranged from 51 to 83 years, with a mean age of 67.4 ± 8.2 years. The average prostate volume was 35.83 ± 12.12 cc, ranging from 11.00 to 62.29 cc. The median serum IL-8 level was 20.41 pg/mL, with values ranging from 0.10 to 205.69 pg/mL. The median IPSS was 26.00, with values ranging from 4 to 33. Table 1 presents an overview of the characteristics of the participants.
Results of the study indicate that the degree of LUTS severity based on IPSS was predominantly severe (29 individuals, 90.6%), with a smaller proportion experiencing mild degrees (3 individuals, 9.4%). No samples were classified into the medium-degree category. The study findings reveal a median IPSS of 26 among the sample, indicating severe symptoms. This outcome was anticipated, given the study’s setting in a national-level referral hospital, where patients with more severe symptoms were more likely to seek treatment. However, it is essential to acknowledge that the sample may not comprehensively represent the broader patient population due to the restricted research duration. Table 2 presents the distribution of LUTS severity degree according to age. Across all age categories, the prevalence of severe LUTS typically outweighs that of mild LUTS. However, no statistically significant variation observed in the distribution of LUTS severity degrees based on age (p = 0.467).
3.2 Association and correlation between IL-8 serum, prostate volume, and LUTS in patients with benign prostatic enlargement
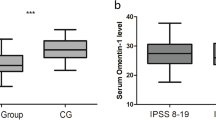
Table 3 presents a comparative analysis of serum IL-8 levels and prostate volume across varying degrees of LUTS severity. Prostate volume substantially increased among individuals experiencing a severe LUTS degree, with a mean volume of 38.19 cc, compared to those with mild LUTS, who exhibited a mean volume of 13.05 cc (p = 0.000). While serum IL-8 levels displayed a greater magnitude in patients with severe LUTS compared to those with moderate LUTS, with mean values of 21.65 pg/mL and 8.44 pg/mL, respectively, this difference did not achieve statistical significance (p = 0.771).
The correlation between prostate volume and serum IL-8 levels to LUTS severity degree in BPE patients is presented in Table 4. Although not statistically significant, a positive correlation observed between serum IL-8 levels and prostate volume (R = 0.297, p = 0.09). Similarly, a positive correlation was observed between serum IL-8 levels and LUTS severity degree (R = 0.237, p = 0.191). LUTS severity degree and prostate volume notably showed a significant positive correlation (p = 0.000). With an R-value of 0.913, the correlation between LUTS severity and prostate volume suggests a strong correlation (R > 0.750).
4 Discussion
The research subject used in this study consisted of male patients, with ages ranging from 51 to 83 years and prostate volumes ranging from 11.00 to 62.29 cc. Among older men, the prevailing condition identified was benign prostatic enlargement, characterized by the proliferation of prostatic epithelial and stromal cells within the transition zone of fibromuscular tissue surrounding the periurethral region, leading to urinary retention. This hyperplastic process is intricately linked to hormonal influences, including estrogen and androgens, as well as interactions between stromal cells and epithelial cells, along with various growth factors [10]. Furthermore, the dynamic effects resulting from the tone of alpha-1 receptors within the smooth muscle of the prostate and bladder neck also play a role in the pathogenesis of benign prostatic enlargement (BPE) [14].
The study results revealed that the severe degree, precisely 29 subjects (90.6%), were attributed to patients seeking medical attention only when experiencing symptoms significantly affecting their daily activities. Among the patients who visited the hospital, the severe degree was prevalent in the age group of 60–74 years, with 17 subjects affected. The prevalence of symptomatic BPE demonstrated an age-related increase. In the 50–59 age group, the prevalence was nearly 25%, escalating to approximately 43% at age 60 and reaching nearly 70% among men over 60. Among men aged over 80 years, the prevalence continued to rise, exceeding 90% [15].
The results of this study indicated that prostate volume was significantly higher in severe LUTS than in mild LUTS. This result follows Tjahodjati et al.’s investigation, which found more significant prostate volumes at severe LUTS levels (IPSS 20–35). The LUTS severity was categorized into three degrees: mild (scores 0–7), moderate (scores 8–19), and severe (scores 20–35). This significant finding is also corroborated by a study conducted by Awaisu et al., which identified a positive significant correlation between prostate volume and the LUTS severity degree in patients with benign prostatic enlargement; an enlarged prostate is known to induce obstructive symptoms of LUTS [9, 10, 16, 17].
Compared to the mild degree, individuals with severe degree exhibited higher levels of serum IL-8. Elevated IL-8 levels promote the proliferation of epithelial and stromal cells in the prostate. This proliferation contributes to urethral compression in patients with BPE. Consequently, the degree of LUTS severity experienced by BPE patients was closely associated with increased IL-8 levels [6].
This study also showed no statistically significant correlation between serum IL-8 levels and prostate volume concerning the degree of LUTS severity although they have a positive correlation. A positive R-value implies a tendency for blood IL-8 levels to increase as LUTS severity increases. Interleukin-8 actively contributes to the chronic inflammation associated with BPE and regulates the proliferation of prostate stromal and epithelial cells. Prostatic epithelial and stromal cell proliferation will increase IL-8 levels, expanding prostate volume. An increase in prostate volume will cause obstructive symptoms of LUTS [8].
The degree of LUTS severity and prostate volume had a statistically significant positive correlation. This result is consistent with Purwanggono’s study, which discovered an association between prostate volume and the degree of LUTS severity with a 0.517 correlation coefficient. The prostate volume was assessed through an ultrasound examination of the abdomen, performed at the initial hospital admission, where the results showed that increased prostatic volume impaired the lower urinary tract, elevated urethral resistance, and altered bladder function, worsening LUTS symptoms by increasing frequency, urgency, and nocturia [18].
A temporal relationship between serum IL-8 levels, prostate volume, and the degree of LUTS severity was found through this study. The primary limitation of this study lies in its utilization of a cross-sectional design with data collected from 32 research participants. Consequently, due to the necessity for a more representative sample size, the findings of this study cannot definitively assert the absence of a relationship when extrapolated to a larger population. Thus, no significant correlation was found between serum IL-8 levels and prostate volume-related factors, as well as the degree of LUTS severity, in this study's sample. Furthermore, this study might have a selection bias, as patients reported visiting the hospital only when their symptoms were severe.
5 Conclusions
The findings reveal that in patients with benign prostatic enlargement (BPE), the volume of the prostate gland and the levels of serum Interleukin-8 are higher in the severe degree of LUTS degree classification than in the mild category. The levels of serum IL-8 and the degree of LUTS severity have no significant correlation with the volume of prostate (p > 0.05) in the Patients with BPE, even though the prostate volume and the degree of LUTS severity have a significant positive correlation. According to this study and previous findings, the degree of LUTS severity has a positive correlation with the prostate volume. Thus, it can be concluded that assessing serum IL-8 levels in BPE patients can be used to estimate the severity of symptoms related to benign prostatic enlargement.
Availability of data and materials
All data used in this study are available from the corresponding author.
Abbreviations
- BPE:
-
Benign prostatic enlargement
- LUTS:
-
Lower urinary tract symptoms
- IL:
-
Interleukin
- ELISA:
-
Enzyme-linked immunosorbent assay
- FGF:
-
Fibroblast growth factor
- H2O2:
-
Hydrogen peroxide
- IPSS:
-
International Prostatic Symptom Score
References
Aaron L, Franco OE, Hayward SW (2016) Review of prostate anatomy and embryology and the etiology of benign prostatic hyperplasia. Urol Clin North Am 43(3):279–288. https://doi.org/10.1016/j.ucl.2016.04.012
Miernik A, Gratzke C (2020) Current treatment for benign prostatic Hyperplasia. Dtsch Arzteblatt Int 117(49):843–854. https://doi.org/10.3238/arztebl.2020.0843
Skinder D, Zacharia I, Studin J, Covino J (2016) Benign prostatic hyperplasia: a clinical review. JAAPA Off J Am Acad Physician Assist 29(8):19–23. https://doi.org/10.1097/01.JAA.0000488689.58176.0a
Naiyila X, Li J, Huang Y et al (2023) A Novel Insight into the Immune-Related Interaction of inflammatory cytokines in benign prostatic hyperplasia. J Clin Med 12(5):1821. https://doi.org/10.3390/jcm12051821
Lokeshwar SD, Harper BT, Webb E et al (2019) Epidemiology and treatment modalities for the management of benign prostatic hyperplasia. Transl Androl Urol 8(5):529–539. https://doi.org/10.21037/tau.2019.10.01
Smith DK, Hasanali SL, Wang J et al (2020) Promotion of epithelial hyperplasia by interleukin-8—CXCR axis in human prostate. Prostate 80(12):938–949. https://doi.org/10.1002/pros.24026
Al-Barzinj RMGT (2020) Estimation levels of prostate-specific antigen, interleukin-8, oxidative stress and some inflammatory markers in sera of benign prostatic hyperplasia patients who have smoking habits as a risk factor. Cell Mol Biol 66(7):124–130. https://doi.org/10.14715/cmb/2020.66.7.19
Lotti F, Maggi M (2013) Interleukin 8 and the male genital tract. J Reprod Immunol 100(1):54–65. https://doi.org/10.1016/j.jri.2013.02.004
Langan RC (2019) Benign prostatic hyperplasia. Prim Care 46(2):223–232. https://doi.org/10.1016/j.pop.2019.02.003
D’Agate S, Wilson T, Adalig B et al (2020) Impact of disease progression on individual IPSS trajectories and consequences of immediate versus delayed start of treatment in patients with moderate or severe LUTS associated with BPH. World J Urol 38(2):463–472. https://doi.org/10.1007/s00345-019-02783-x
Madersbacher S, Sampson N, Culig Z (2019) Pathophysiology of benign prostatic hyperplasia and benign prostatic enlargement: a mini-review. Gerontology 65(5):458–464. https://doi.org/10.1159/000496289
Guo S, Zhang J, Jiao J et al (2023) Comparison of prostate volume measured by transabdominal ultrasound and MRI with the radical prostatectomy specimen volume: a retrospective observational study. BMC Urol 23(1):62. https://doi.org/10.1186/s12894-023-01234-5
Jardine E (2021) A comparison of how prostate volume obtained using transabominal ultrasound differs to volume obtained using transrectal ultrasound approach. Sonography 8(2):43–49. https://doi.org/10.1002/sono.12252
Mansbart F, Kienberger G, Sönnichsen A, Mann E (2022) Efficacy and safety of adrenergic alpha-1 receptor antagonists in older adults: a systematic review and meta-analysis supporting the development of recommendations to reduce potentially inappropriate prescribing. BMC Geriatr 22(1):771. https://doi.org/10.1186/s12877-022-03415-7
Purnomo B (2003) Basic of urology. CV Sagung Seto
Tjahodjati, Soebadi M, Umbas R, Purnomo B, Widjanarko S (2017) Guideline for Clinical Management of Benign Prostate Hyperplasia. Ikatan Ahli Urologi Indonesia (IAUI)
Awaisu M, Ahmed M, Lawal AT et al (2021) Correlation of prostate volume with severity of lower urinary tract symptoms as measured by international prostate symptoms score and maximum urine flow rate among patients with benign prostatic hyperplasia. Afr J Urol 27(1):16. https://doi.org/10.1186/s12301-021-00122-4
Lee CL, Kuo HC (2017) Pathophysiology of benign prostate enlargement and lower urinary tract symptoms: current concepts. Tzu-Chi Med J 29(2):79–83. https://doi.org/10.4103/tcmj.tcmj_20_17
Acknowledgements
The authors would like to thank Farhamna Academic for assisting in the preparation of this manuscript. Thanks to urology department staff and installation of clinical pathology laboratory of the Hasanuddin University Medical Faculty who have assisted in providing treatment and monitoring variables.
Funding
Authors did not receive any funding for the conduct of this study.
Author information
Authors and Affiliations
Contributions
UB and YKAAA conceived and designed the analysis, collected the data, contributed data or analysis tools, performed the analysis, and wrote the paper. AM, FM, and MAP conceived and designed the analysis and wrote the paper. BB conceived and designed the analysis and contributed data or analysis tools. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Health Research Ethics Commission of our institution issued approval for this study with the number 491/UN4.6.4.5.31/PP36/2022. All patients gave their consent prior to involve in the study.
Consent for publication
Written informed consent was obtained from all involving patients for publication of accompanying data or images.
Competing interests
The authors declare no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Bahrun, U., Atmanto, Y.K.A.A., Nurulita, A. et al. Correlation of serum interleukin-8 levels and prostate volume to the degree of lower urinary tract symptoms in patients with benign prostate enlargement: a cross-sectional study. Afr J Urol 30, 24 (2024). https://doi.org/10.1186/s12301-024-00427-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-024-00427-0