
Abstract
Background
Physical activity (PA) changes throughout an individual’s life, but the association between such changes and cancer risk seems to be overlooked in the literature. Thus, this study aimed to examine the association between the trajectories of PA frequency and cancer incidence among middle-aged Korean adults.
Methods
A total of 1,476,335 eligible participants (992,151 men and 484,184 women) aged ≥40 years from the National Health Insurance Service cohort (2002–2018) were included. Assessment of PA frequency was a self-reported measure, based on the question: “How many times per week do you perform exercise that makes you sweat?”. PA frequency trajectories (i.e., trajectory classes of change in PA frequency) from 2002 to 2008 were identified using group-based trajectory modeling. Cox proportional hazards regression was used to assess the associations between the PA trajectories and cancer incidence.
Results
Five PA frequency trajectories over 7 years were identified: persistently low (men:73.5%; women:74.7%), persistently moderate (men:16.2%; women:14.6%), high-to-low (men:3.9%; women:3.7%), low-to-high (men:3.5%; women:3.8%), and persistently high (men:2.9%; women:3.3%). Compared with persistently low frequency, maintaining a high PA frequency was associated with a lower risk of all cancers (Hazard ratio (HR) = 0.92, 95%CI = 0.87–0.98) and breast cancer (HR = 0.82, 95%CI = 0.70–0.96) among women. There was a lower risk for thyroid cancer among men in the high-to-low (HR = 0.83, 95%CI = 0.71–0.98), low-to-high (HR = 0.80, 95%CI = 0.67–0.96), and high PA trajectories (HR = 0.82, 95%CI = 0.68–0.99). There was a significant association between moderate trajectory and lung cancer in men (HR = 0.88, 95%CI = 0.80–0.95), in both smoking and non-smoking men.
Conclusion
Long-term persistent high frequency of PA as part of the daily routine should be widely promoted and encouraged to reduce the risk for all cancer development in women.
Similar content being viewed by others

Background
The protective effect of physical activity (PA) on cancer risk via multiple potential mechanisms, such as reduction in circulating estrogen levels, insulin resistance, and inflammation, has been well-documented [1]. Strong evidence has shown that PA has a protective effect and reduces the risk for colon, breast, and endometrial cancer [1], while the impact of PA on the decreased risk for esophageal, lung, and liver cancer was suggestive [2]. Additionally, PA was reported to reduce weight gain, and this was indirectly attributed to a lower risk for obesity-related cancers [1]. However, such scientific evidence was accumulated from observational studies that investigated the association between PA at a single time point (i.e., baseline) and cancer outcomes. In fact, our behaviors, pertaining to performing PA, continuously change throughout the life course; this could modify the effects of PA on cancer risk suggested in existing evidence.
Recently, group-based trajectory modeling (GBTM) was developed as a novel approach that overcomes the disadvantages of the traditional method. GBTM can fully capture behaviors accounted for within-individual variation throughout the life course, and it has been commonly utilized for determining risky behaviors, such as tobacco use and alcohol consumption. Although GBTM has been increasingly applied to identify PA trajectories in relation to mortality and several disease outcomes [3,4,5,6], its association with cancer seems to be typically overlooked.
The association between the trajectory of PA and cancer risk has not been well-explored. To date, only one case-control study has investigated the impact of PA trajectory on pancreatic cancer risk [7]. The trajectory of moderate and vigorous PA from the 20s to 50s age was identified, including six latent groups: persistent inactivity, low activity, increasingly active, high activity with substantial decrease, high activity with a slight decrease, and persistent high activity. The results showed that none of these trajectories was significantly associated with the risk for pancreatic cancer. Thus, further investigation with a stronger study design, such as cohort study, is needed to elucidate the causal association between the trajectory of PA and cancer risk.
In South Korea, a high proportion of adults participate in insufficient PA [8], and it had been observed to increase from 24.6% in 2008 to 42.9% in 2014 [9]. The transition of PA status could affect cancer incidence; however, no studies have been dedicated to this issue in South Korea. Thus, we aimed to examine the association between different trajectories of PA frequency and cancer incidence among middle-aged Korean adults.
Methods
Study population
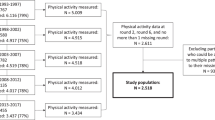
This study used data from a nationwide population-based cohort study that used the database provided by the National Health Insurance Services (NHIS) in South Korea [10]. In brief, the NHIS is a mandatory single-payer insurance provider that conducts a non-payment general health examination program for all insured adults biennially. The participation rate of this program was 74.1% in 2019 [11]. The data of 5,544,985 enrollees aged ≥40 years who underwent health examination in 2002–2003 were used. After excluding individuals with missing information regarding sex, age, and PA, 1,476,335 cancer-free individuals (992,151 men and 484,184 women) had information on PA frequency four times from the cohort between 2002 and 2008, were included and followed-up until 2018. As this study used anonymous secondary data, the study was exempted from review by the Institutional Review Board of the National Cancer Center, Korea (NCC2018–0279). This study was conducted according to the Declaration of Helsinki.
PA trajectory
The frequency of PA was measured using a questionnaire as part of the general health examination, the main question used was: “How many times per week do you perform exercise that makes you sweat?”, and the five responses were 1) none, 2) 1–2 times, 3)3–4 times, 4)5–6 times, or 5) almost every day. We decided to determine the trajectories of PA frequency from 2002 to 2008 because the questionnaire has changed since 2009. As the general health examination was recommended biennially, four 2-year period time points (2002–2003, 2004–2005, 2006–2007, and 2008) were used to measure the trajectories of PA frequency. As aforementioned, we aimed to determine PA trajectories during the longest observable duration; therefore, we chose the exposure period of 7 years, from starting of the database (i.e., 2002) to the end of time before revising the health examination questionnaire (i.e., 2008).
PA trajectories were identified using the GBTM method proposed by Nagin with the PROC TRAJ in SAS [12]. The maximum number of trajectories was chosen based on the findings of a systematic review, in which the number of PA trajectories throughout the life-course commonly ranged from 3 to 5 [13]. Additionally, the maximum number of trajectories recommended is six; therefore, we tested on a maximum number of 6 trajectories. The process of choosing polynomial components was performed as the general rule, following the tutorial by Andruff [14]. Therein, initial testing involved a model with two cubic components (syntax ‘ORDER 3 3’). Once the only one component showed significant results, a model with one cubic component and one quadratic component (syntax “ORDER 3 2” or “ORDER 2 3) was tested. If significance were shown in none of the cubic component, the model’s quadratic components would be assessed (syntax “ORDER 2 2). Then, a model with one quadratic and one linear component (syntax “ORDER 1 2” or “ORDER 2 1”) or one with two linear components (syntax “ORDER 1 1”) was evaluated if the model’s quadratic components for two trajectories were not significant. Eventually, if all polynomial components of a model were significant, the analysis for two trajectories was finished, and the Bayesian information criterion (BIC) values and proportion of group membership (i.e., the percentage of each trajectory) were noted. Testing in three, four, five and six trajectories was repeated through this process, separately for men and women, until the best-fitting models was found. As recommended, the best-fitting model was chosen based on the smallest Bayesian Information Criteria (BIC) value, and the proportion of each group membership was ≥5% [15]. In our study, although we decreased the number of groups within the model, one trajectory group remained to have a low proportion (around 3.0% of the study population). Thus, five trajectories of PA frequency were identified in both men and women: low, moderate, high-to-low, low-to-high, and high (Fig. 1). Supplemental Table 1 summarizes the best-fitting models based on the number of groups. For the final models, the average posterior probabilities for the group 1 to 5 in men were 0.93, 0,88, 0,81, 0.95, and 0.92, respectively, and those in women were 0.81, 0.96, 0.94, 0.93, and 0.91, respectively, all of which were higher than the recommended cut-off value of 0.7 [16].

Trajectories of physical activity frequency over 7 years. A) Men, B) Women
Cancer outcome
The International Classification of Diseases 10th edition (ICD-10) codes were used to evaluate the incidence of all cancer types (C00–C97) and several specific cancers, including colon and rectal (C18–20), liver (C22), lung (C33, C34), breast (C50), corpus uteri (C54), and thyroid gland cancers (C73). Furthermore, a special code for cancer claims (V193) was additionally used to identify cancer occurrence during the follow-up period. All participants were followed-up until the date of cancer onset, death, or the end of the follow-up period (December 31, 2018).
Covariates
Covariates were retrieved from baseline (2002–2003). Sex and age were included, and income levels were divided into quartiles, from Q1 (lowest income) to Q4 (highest income).
Behavioral risk factors were measured, including smoking status, body mass index (BMI), and alcohol consumption. Smoking status was categorized into three groups: non-smoker, former smoker, and current smoker. BMI was classified as underweight (< 18.5 kg/m2), normal (18.5–22.9 kg/m2), overweight (23–24.9 kg/m2), and obesity (≥25 kg/m2), according to the World Health Organization (WHO) obesity standard for the Asian population [17]. Alcohol consumption was classified into the following groups: rarely drinking, 2–3 times/month, 1–2 times/week, 3–4 times/week, and almost every day. Additionally, the Charlson Comorbidity Index (CCI) was also calculated for inpatients using ICD-10 codes [18].
Statistical analysis
Descriptive statistics were used to describe the variables of participants’ characteristics. PA trajectories were identified based on the GBTM approach using PROC TRAJ in SAS 9.4 software. Cox proportional hazards regression was used to estimate the risk for cancer. In the multivariate model, we adjusted for age, income level, smoking status, alcohol consumption, BMI, and CCI score. We additionally adjusted for chronic viral hepatitis (i.e., B18 in ICD-10) in the multivariate model for liver cancer. For sensitivity analysis, we examined the association between PA trajectories and cancer incidence by smoking status and BMI groups. All statistical analyses were stratified by sex and performed using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
More than two-thirds of the study participants had a low frequency of PA (73.51% in men; 74.66% in women), while approximately 15% and only 3% had a moderate and high frequency of PA during approximately 7 years, respectively.
The baseline characteristics according to the trajectories PA frequency in men and women are shown in Table 1 and Table 2, respectively. Compared to individuals with low PA frequency, both men and women with a higher frequency of PA tended to be richer and overweight/obese. Men in the low PA frequency category tended to be younger, had a higher proportion of current smokers, and were less likely to consume alcohol every day.
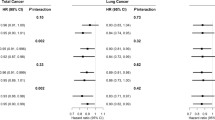
During the 9,368,662 person-years of follow-up, 84,703 men developed cancer. In the age-adjusted model, compared to the low category, men with a moderate trajectory of PA had a lower risk for all cancers (HR = 0.97, 95%CI = 0.95–0.98), and specific cancer of colorectum (HR = 0.92, 95%CI = 0.88–0.97) and lung (HR = 0.76, 95%CI = 0.72–0.81). A significantly lower risk for lung cancer was also observed in men with high-to-low and high frequency trajectory of PA. After adjusting for other potential confounders, only significant effect of the moderate trajectory of PA on a lower risk for lung cancer incidence remained (HR = 0.88, 95%CI = 0.82–0.93). Additionally, compared to the low trajectory, there was a lower risk for thyroid cancer among men in the high-to-low (HR = 0.83, 95%CI = 0.71–0.98), low-to-high (HR = 0.80, 95%CI = 0.67–0.96), and high trajectories (HR = 0.82, 95%CI = 0.68–0.99) (Table 3).
During the 4,615,930 person-years of follow-up, 35,049 women developed cancer. A negative association between moderate frequency of PA and breast cancer incidence was observed in the age-adjusted model; however, a significant association was not observed in the fully-adjusted model. After adjusting for covariates, a high frequency of PA during the 7 years was significantly associated with a decreased risk of all cancers (HR = 0.92, 95%CI = 0.87–0.98) and breast cancer (HR = 0.82, 95%CI = 0.70–0.96) (Table 3).
In the subgroup analysis by smoking status, in men, moderate frequency of PA was significantly associated with a lower risk for colorectal cancer in male smokers, while low-to-high and high frequencies of PA were significantly associated with a lower risk for thyroid cancer in non-smoking men. A significant association between moderate PA trajectory and lung cancer was observed in both non-smoking and smoking men. In women, a high PA trajectory was associated with a decreased risk for all cancers and breast cancer among non-smoking women, whereas a null association was observed in smoking women (Table 4).
In the subgroup analysis by BMI, a significant negative impact of moderate trajectory of PA on the risk for colorectal and lung cancers was observed in men who were underweight or had a normal BMI. There was an association between high-to-low PA trajectory and lower risk for thyroid cancer among overweight/obese men. Notably, the high PA trajectory was associated with an increased risk for corpus uteri cancer compared to the low PA trajectory (Supplemental Table 2).
Discussion
Our study was the first to identify the trajectories of PA frequency and its relationship with all cancer risk and several specific cancers. Our findings showed that more than two-thirds of middle-aged Korean adults remained at a low frequency of PA, and only 5% had a high frequency of PA during approximately 7 years. Additionally, this study revealed that a small proportion of people changed their frequency of PA from low to high and from high to low, and each trajectory accounted for approximately only 5% in both sexes. Existing evidence suggests that PA has a protective effect on cancer prevention, and PA in almost studies was usually measured at a single time point (i.e., baseline) [19,20,21,22,23]. Hence, we hypothesized that PA trajectories during the 7 years could have modified the association between PA and cancer incidence. The present study unveiled a novel finding that, compared to persistent low frequency, maintaining a high frequency of PA over a period of approximately 7 years was significantly associated with a lower risk of all cancer incidence among women.
The link between PA and cancer risk, especially that of specific cancers, has been established in observational studies; however, to our knowledge, no study has assessed the effect of PA trajectories on the risk for all cancers. Limited research has shown an inverse impact of non-trajectory-based PA on the development of all cancers [ More than two-thirds of the middle-aged Korean population had a low frequency of PA for approximately 7 years. Compared to persistent low frequency, maintaining a high frequency of PA was significantly associated with a lower risk for the onset of all cancers and breast cancer in women; and thyroid cancer among men. A reduction in the risk for lung and colorectal cancer was also observed for smoking men who had a moderate level of PA frequency relative to those who had a low level of PA frequency. Thus, our study suggests that increasing physical activity as part of the daily routine should be widely promoted to protect individuals against cancer development for women.Conclusions
Availability of data and materials
The datasets generated and analyzed in the current study are available upon request from the National Health Insurance Sharing Service (https://nhiss.nhis.or.kr/).
Abbreviations
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
- PA:
-
Physical activity
- NHIS:
-
National Health Insurance Services
- GBTM:
-
Group-based trajectory modeling
- ICD-10:
-
International Classification of Diseases 10th edition
- BIC:
-
Bayesian Information Criteria
- BMI:
-
Body mass index
- CCI:
-
Charlson Comorbidity Index
- RR:
-
Relative risk
- WCRF/AICR:
-
World Cancer Research Fund/American Institute for Cancer Research
- OR:
-
Odds ratio
References
World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: a Global Perspective. 2018.
World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Export Report 2018: Physical activity and the risk of cancer; 2018.
Mok A, Khaw KT, Luben R, Wareham N, Brage S. Physical activity trajectories and mortality: population based cohort study. BMJ. 2019;365:l2323.
Willey JZ, Voutsinas J, Sherzai A, Ma H, Bernstein L, Elkind MSV, et al. Trajectories in Leisure-Time Physical Activity and Risk of Stroke in Women in the California Teachers Study. Stroke. 2017;48(9):2346–52.
Laddu DR, Rana JS, Murillo R, Sorel ME, Quesenberry CP Jr, Allen NB, et al. 25-Year Physical Activity Trajectories and Development of Subclinical Coronary Artery Disease as Measured by Coronary Artery Calcium: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Mayo Clin Proc. 2017;92(11):1660–70.
Pettee Gabriel K, Griswold ME, Wang W, Conway SH, Windham BG, Palta P, et al. Physical activity trajectories and subsequent fall risk: ARIC Study. Prev Med. 2019;121:40–6.
Sandhu J, De Rubeis V, Cotterchio M, Smith BT, Griffith LE, Brenner DR, et al. Trajectories of physical activity, from young adulthood to older adulthood, and pancreatic cancer risk; a population-based case-control study in Ontario, Canada. BMC Cancer. 2020;20(1):139.
An KY. Physical activity level in Korean adults: the Korea National Health and Nutrition Examination Survey 2017. Epidemiol Health. 2019;41:e2019047.
Yang YJ. Current status of physical activity and policy proposals of the national level. Korean J Health Educ Promot. 2016;33:47–54.
Seong SC, Kim Y-Y, Park SK, Khang YH, Kim HC, Park JH, et al. Cohort profile: the National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open. 2017;7(9):e016640.
National Health Insurance Service. National Health Screening Statistical Yearbook (2019). Wonju2020.
Nagin DS. Group-based modeling of development. Cambridge: Havard University Press; 2005.
Lounassalo I, Salin K, Kankaanpaa A, Hirvensalo M, Palomaki S, Tolvanen A, et al. Distinct trajectories of physical activity and related factors during the life course in the general population: a systematic review. BMC Public Health. 2019;19(1):271.
Andruff H, Carraro N, Thompson A, Gaudreau P, Louvet B. Latent Class Growth Modelling: A Tutorial; 2009.
Zheng H, Tumin D, Qian Z. Obesity and mortality risk: new findings from body mass index trajectories. Am J Epidemiol. 2013;178(11):1591–9.
Nagin DS. Group-Based Modeling of Development: Harvard University Press; 2005.
WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–63.
Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–51.
Ho V, Parent ME, Pintos J, Abrahamowicz M, Danieli C, Richardson L, et al. Physical activity and lung cancer risk in men and women. Cancer Causes Control. 2017;28(4):309–18.
Rundle A, Richie J, Steindorf K, Peluso M, Overvad K, Raaschou-Nielsen O, et al. Physical activity and lung cancer among non-smokers: a pilot molecular epidemiological study within EPIC. Biomarkers. 2010;15(1):20–30.
Steindorf K, Friedenreich C, Linseisen J, Rohrmann S, Rundle A, Veglia F, et al. Physical activity and lung cancer risk in the European Prospective Investigation into Cancer and Nutrition Cohort. Int J Cancer. 2006;119(10):2389–97.
Fiore M, Cristaldi A, Okatyeva V, Lo Bianco S, Oliveri Conti G, Zuccarello P, et al. Physical Activity and Thyroid Cancer Risk: A Case-Control Study in Catania (South Italy). Int J Environ Res Public Health. 2019;16(8).
Xhaard C, Lence-Anta JJ, Ren Y, Borson-Chazot F, Sassolas G, Schvartz C, et al. Recreational Physical Activity and Differentiated Thyroid Cancer Risk: A Pooled Analysis of Two Case-Control Studies. Eur Thyroid J. 2016;5(2):132–8.
**e F, You Y, Huang J, Guan C, Chen Z, Fang M, et al. Association between physical activity and digestive-system cancer: An updated systematic review and meta-analysis. J Sport Health Sci. 2021;10(1):4–13.
Moore SC, Lee IM, Weiderpass E, Campbell PT, Sampson JN, Kitahara CM, et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA. Intern Med. 2016;176(6):816–25.
Jackson SS, Marks MA, Katki HA, Cook MB, Hyun N, Freedman ND, et al. Sex disparities in the incidence of 21 cancer types: Quantification of the contribution of risk factors. Cancer. 2022;128(19):3531–40.
Liu Y, Li Y, Bai YP, Fan XX. Association Between Physical Activity and Lower Risk of Lung Cancer: A Meta-Analysis of Cohort Studies. Front Oncol. 2019;9:5.
Brenner DR, Yannitsos DH, Farris MS, Johansson M, Friedenreich CM. Leisure-time physical activity and lung cancer risk: A systematic review and meta-analysis. Lung Cancer. 2016;95:17–27.
Zhong S, Ma T, Chen L, Chen W, Lv M, Zhang X, et al. Physical Activity and Risk of Lung Cancer: A Meta-analysis. Clin J Sport Med. 2016;26(3).
Leitzmann MF, Brenner A, Moore SC, Koebnick C, Park Y, Hollenbeck A, et al. Prospective study of body mass index, physical activity and thyroid cancer. Int J Cancer. 2010;126(12):2947–56.
Kitahara CM, Platz EA, Beane Freeman LE, Black A, Hsing AW, Linet MS, et al. Physical activity, diabetes, and thyroid cancer risk: a pooled analysis of five prospective studies. Cancer Causes Control. 2012;23(3):463–71.
Zhao ZG, Guo XG, Ba CX, Wang W, Yang YY, Wang J, et al. Overweight, obesity and thyroid cancer risk: a meta-analysis of cohort studies. J Int Med Res. 2012;40(6):2041–50.
Hong S, Won YJ, Lee JJ, Jung KW, Kong HJ, Im JS, et al. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2018. Cancer Res Treat. 2021;53(2):301–15.
Chen X, Wang Q, Zhang Y, **e Q, Tan X. Physical Activity and Risk of Breast Cancer: A Meta-Analysis of 38 Cohort Studies in 45 Study Reports. Value Health. 2019;22(1):104–28.
Oyeyemi SO, Braaten T, Licaj I, Lund E, Benjaminsen BK. Physical activity patterns and the risk of colorectal cancer in the Norwegian Women and Cancer study: a population-based prospective study. BMC Cancer. 2018;18(1):1216.
Dai Z, Xu YC, Niu L. Obesity and colorectal cancer risk: a meta-analysis of cohort studies. World J Gastroenterol. 2007;13(31):4199–206.
Voskuil DW, Monninkhof EM, Elias SG, Vlems FA, van Leeuwen FE. Physical activity and endometrial cancer risk, a systematic review of current evidence. Cancer Epidemiol Biomark Prev. 2007;16(4):639–48.
John EM, Koo J, Horn-Ross PL. Lifetime physical activity and risk of endometrial cancer. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2010;19(5):1276–83.
Friberg E, Mantzoros CS, Wolk A. Physical Activity and Risk of Endometrial Cancer: A Population-Based Prospective Cohort Study. Cancer Epidemiology Biomarkers &; Prevention. 2006;15(11):2136–40.
Lin ZZ, Xu YC, Liu CX, Lu XL, Wen FY. Physical Activity and Liver Cancer Risk: A Systematic Review and Meta-analyses. Clin J Sport Med. 2021;31(1):86–90.
Armstrong T, Bull F. Development of the World Health Organization Global Physical Activity Questionnaire (GPAQ). J Public Health. 2006;14(2):66–70.
Acknowledgments
Not applicable.
Funding
This work was supported by the National Cancer Center [grant number: NCC-2010301 and NCC-2210862].
Author information
Authors and Affiliations
Contributions
Conceptualization: JKO and MKL. Methodology: TPTT, NML, MH, and TTB, Formal analysis: TPTT, Investigation: JKO and TPTT, Writing-original draft preparation: TPTT, Writing-review and editing: JKO and MKL. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
As this study used anonymous secondary data, the study was exempted from review by the Institutional Review Board of the National Cancer Center, Korea (NCC2018–0279).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tran, T.P.T., Luu, N.M., Bui, T.T. et al. Trajectory of physical activity frequency and cancer risk: Findings from a population-based cohort study. Eur Rev Aging Phys Act 20, 4 (2023). https://doi.org/10.1186/s11556-023-00316-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s11556-023-00316-5