
Abstract
The correlation between tonsil microbiome and tonsillar hypertrophy has not been well established. Given that oral dysbiosis is related to several metabolic diseases and that tonsillar hypertrophy leads to disordered breathing during sleep and obesity in children, it is necessary to investigate the relationship between the oral microbiome and tonsillar hypertrophy. After 16S rRNA amplicon sequencing of tonsillectomy samples, we evaluated the correlation between the tonsil microbiome and biochemical blood indices in pediatric patients who underwent tonsillectomy. Groups are classified into two categories: based on BMI, and grades 2, 3, and 4 based on tonsil size. Children with obesity and tonsillar hypertrophy have similar microbiome compositions and induce comparable changes in microbiome abundance and composition, confirming the association from a metagenomic perspective. In addition, obesity and tonsillar hypertrophy demonstrated a strong correlation with the Proteobacteria to Firmicutes (P/F) ratio, and among various biochemical indicators, alanine aminotransferase (ALT) levels increase with obesity and tonsillar hypertrophy, indicating a possible association of tonsil microbiome and liver metabolism. These novel findings demonstrate the significance of the tonsil microbiome and suggest the need for tonsil regulation, particularly during childhood.
Similar content being viewed by others

Introduction
The oral microbiome is the second largest microbial community in humans after the gut microbiome. Bacterial growth occurs in the human oral cavity in a variety of habitats including the tongue, teeth, hard and soft palates, and the tonsils1. Oral bacteria contribute to oral diseases and are a significant risk factor for several diseases affecting other parts of the body, including diabetes2, atherosclerosis3, and inflammatory bowel disease4. The composition of the oral microbiome is influenced by host health and lifestyle-related factors, and the host immune system plays an important role in the homeostasis of the oral microbiome. Thus, oral microbiome dysfunction is associated with several oral and systemic diseases5, and occasionally, the oral microbiome can also enhance the host immune system6.
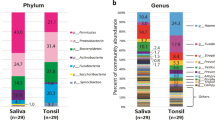
Tonsils are connected to both the digestive and the respiratory systems and can be affected by bacteria from the saliva and the digestive tract. We previously investigated the association between the saliva and the tonsil microbiomes and reported similar diversity and composition between the two microbiomes7. Obesity, adenoid vegetation, and tonsillar hypertrophy are significant risk factors for develo** obstructive sleep apnea (OSA), which adversely affects physical growth8, neurocognitive functions9, and behavioral functioning10 in children. A previous study reported a larger tonsil size in children with obesity and sleep-disordered breathing, with a positive correlation between the palatine tonsil and adenoid size and the apnea–hypopnea index in both children with obesity and those with normal weights11. OSA caused by obesity and tonsillar hypertrophy can lead to oral microbiome alterations due to respiratory failure. A recent study demonstrated a correlation between the tonsillar microbiome and chronic tonsillitis and OSA in children, as well as a correlation between the gut microbiome and host weight12. Moreover, people with OSA had significantly decreased bacterial diversity compared to people without OSA, with the most significant decrease occurring in people with moderate OSA.
Oral bacteria are substantial risk factors for systemic disorders such as diabetes, preterm birth, and cardiovascular disease, as the oral cavity is a clinically relevant microbial habitat and a gateway to the gut2,Full size image
In category 2, the 113 ASVs in grade 2, 125 ASVs in grade 3, and 229 ASVs in grade 4 are presented as a Venn diagram (Fig. 3b). The 67 common ASVs shared by grade 2, 3, and 4 groups corresponded to 59.3%, 53.6%, 29.3% of the groups, respectively. Similar to the obese group in category 1, the composition of Firmicutes was the highest in the grade 4 group in category 2. The number of ASVs of Firmicutes in the lean, grade 2, and grade 3 groups was comparable, while the number of ASVs in the obese and grade 4 groups was approximately 2.6 ± 0.3-fold.
Association of microbial communities based on obesity and tonsil size
To investigate the association of microbial communities between the obese and tonsil grade groups, the composition of obese-exclusive ASVs in category 1 and grade 4-exclusive ASVs in category 2 was classified using a Venn diagram in Fig. 4. We identified 79 shared ASVs among the obese-exclusive and grade 4-exclusive ASVs, corresponding to 73% of the obese-exclusive and 65% of the grade 4-exclusive ASVs (Fig. 4a). Firmicutes dominated the phyla of common ASVs in the Venn diagram, accounting for 70% of the total ASVs (56 out of 79 ASVs) (Fig. 4c). Additionally, Firmicutes accounted for 10 out of 29 (34%) ASVs unique to the obese group (Fig. 4b), and 25 out of 43 (25%) ASVs unique to the grade 4 group (Fig. 4d).

Classification of exclusive ASVs in the obese and grade 4 groups. The Venn diagram shows the overall number of ASVs overlap** between obese-exclusive ASVs in category 1 and grade 4-exclusive ASVs in category 2. The bar plot shows the microbial composition at the genus level of the unique ASVs and common ASVs in each group.
Association between biochemical parameters and bacterial communities of the patients
We used Spearman correlation analysis to compare the correlations between the 79 common ASVs shared by obese-exclusive and grade 4-exclusive ASVs, using data from 20 biochemical indices and five anthropometric measurements (Fig. 5). Regardless of the group in each category, we observed mostly positive correlations between the ASVs (Fig. S2). More ASVs had a significant correlation with the obese and grade 4 groups than with the lean and grade 2 and 3 groups.

Correlation of biochemical indices and 79 ASVs obtained from overlap** of obese-exclusive ASVs and grade 4-exclusive ASVs. Correlation plot of 79 ASVs in obese and grade 4 groups with 20 biochemical indices and five anthropometric measurements. A correlation matrix plot based on Spearman correlation was developed. Positive and negative correlations are represented by red and blue circles, respectively, and the size and color of the circles refer to the correlation value. All circles show a significant correlation (P ≤ 0.05).
In the obese group, ASVs showed a significant negative correlation with blood sugar concentration, HCT, RBC, and total protein, but a positive correlation with ALT. In the grade 4 group, ASVs showed a significant negative correlation with HCT and RBC, and a significantly positive correlation with weight, BMI, body weight percentile, body surface area, total cholesterol, and ALT. In both the obese and grade 4 groups, HCT and RBC showed a significant negative correlation with ASVs, and ALT showed a significant positive correlation.

