
Abstract
The association between pancreatitis and acute myocardial infarction or stroke remains incompletely understood. This study aimed to evaluate the long-term risk of acute atherosclerotic cardiovascular disease (ASCVD) in people with acute and chronic pancreatitis. Using research database of Taiwan's National Health Insurance, we identified 2678 patients aged ≥ 20 years with newly diagnosed pancreatitis in 2000–2008. A cohort of 10,825 adults without pancreatitis was selected for comparison, with matching by age and sex. Both cohorts were followed from 2000 to the end of 2013, and incident acute ASCVD was identified during the follow-up period. Adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) of acute ASCVD associated with pancreatitis were calculated. Compared with the comparison cohort, the adjusted HR of acute ASCVD were 1.76 (95% CI 1.47–2.12) and 3.42 (95% CI 1.69–6.94) for people with acute pancreatitis and chronic pancreatitis, respectively. A history of alcohol-related illness (HR 9.49, 95% CI 3.78–23.8), liver cirrhosis (HR 7.31, 95% CI 1.81–29.5), and diabetes (HR 6.89, 95% CI 2.18–21.8) may worsen the risk of acute ASCVD in patients with chronic pancreatitis. Compared with people had no pancreatitis, patients with acute pancreatitis who had alcohol-related illness (HR 4.66, 95% CI 3.24–6.70), liver cirrhosis (HR 4.44, 95% CI 3.05–6.47), and diabetes (HR 2.61, 95% CI 2.03–3.36) were at increased risk of acute ASCVD. However, the cumulative use of metformin was associated with a reduced risk of acute ASCVD in the acute pancreatitis cohort (HR 0.30, 95% CI 0.17–0.50). Compared with the control group, patients with acute or chronic pancreatitis were more likely to have an increased risk of acute ASCVD, while the use of metformin reduced the risk of acute ASCVD. Our findings warrant a survey and education on acute ASCVD for patients with acute and chronic pancreatitis.
Similar content being viewed by others

Introduction
Coronary artery disease and stroke are the second and third leading causes of death in the world, respectively1. Atherosclerosis is a common pathological process characterized by the accumulation of lipids and lymphocytes/macrophages in the walls of large and medium-sized arteries2,3. Atherosclerotic cardiovascular disease (ASCVD), including coronary artery disease and ischemic stroke, accounts for the majority of cardiovascular mortality, imposes enormous economic burdens and continues to be a major public health issue worldwide1,4.
Pancreatitis, which is characterized by inflammation of the pancreas, have been classified in either acute, recurrent acute or chronic forms5,6. Acute pancreatitis often leads to a number of sequelae long after clinical resolution, and should no longer be considered a self-limited disease6. Around 21% of patients suffering a first acute pancreatitis will develop recurrent acute pancreatitis. Of those develo** recurrent acute pancreatitis, up to 36% will develop chronic pancreatitis5. Alcohol abuse and gallstones are common etiologies for acute pancreatitis, accounting for over 80% of all cases5. In most areas, the gallstone is the most common etiology following by idiopathic etiology. Acute pancreatitis is associated with profound hypotension, hyperglycemia and increased circulating levels of inflammatory cytokines/proteolytic enzymes7,8. Chronic pancreatitis is a chronic inflammatory and fibrotic disease of the pancreas with a prevalence of 42 to 73 per 100,000 adults in the United States9. Chronic pancreatitis often results in chronic abdominal pain and is most commonly caused by excessive alcohol use, smoking, or genetic mutations9. Suggestions of treatment included alcohol and smoking cessation, pain control, replacement of pancreatic insufficiency, or mechanical drainage of obstructed pancreatic ducts for some patients5,9,10,11.
Some studies have suggested that patients with acute or chronic pancreatitis are more likely to have acute ASCVD, including acute myocardial infarction and stroke, compared with those without pancreatitis7,8,10,11. However, there is heterogeneity in these previous reports because of study limitations, such as small sample sizes8, inadequate control of confounding factors7,8,10,11, and unclear definitions of pancreatitis cases7,9,11. In addition, the influence of pancreatitis severity on the risk of acute ASCVD is unclear. Using research data from the health insurance program in Taiwan, we conducted this retrospective cohort study to evaluate the risk of acute ASCVD in patients with acute and chronic pancreatitis.
Methods
Source of data
In this study, we used research data from the health insurance program, and it covers at least 99% of residents in Taiwan. The research database included the patient’s basic characteristics, examination, diagnoses, prescriptions, and treatments of inpatient and outpatient medical services. The detailed description and reviews of this database were reported previously7,8,10,11. Our study waived the need of informed consent and it was approved by the institutional review board of Taipei Medical University (TMU-JIRB-201701050; TMU-JIRB-201705063; TMU-JIRB-201705065; TMU-JIRB-201808012; TMU-JIRB-201912046). All methods were carried out in accordance with relevant guidelines and regulations.
Study design
We conducted this retrospective cohort study using a random sample of 1 million beneficiaries from the research database and there is no direct participation of patients in the current study. The database of Taiwan’s National Health Insurance was available since 1996. We identified 2737 patients aged over 20 years who were newly diagnosed with pancreatitis in the period 2000–2008; 10,948 persons without a history of pancreatitis were selected as the control group, with frequency matching by age and sex (case–control ratio nearly 1:4). In this study, the wash-out period was 4 years (confirming both cohorts had no physician’s diagnosis of pancreatitis within past 4 years). To strictly identify pancreatitis cases, we defined pancreatitis by requiring inpatient care with pancreatitis as the physician's primary diagnosis. The pancreatitis and non-pancreatitis cohorts had no history of acute ASCVD at the start, and both were followed up from the index date until December 31, 2013, or until they were censored because of death. The event of acute ASCVD was considered the outcome during the follow-up period.
Measures and definitions
The low-income patients were identified according to the criteria from the Ministry of Health and Welfare. For indentifying medical conditions and major outcomes, we used the physician’s diagnoses and the International Classification of Diseases-Clinical Modification, 9th edition (ICD-9-CM) including acute pancreatitis (code 577.0), chronic pancreatitis (code 577.1), stroke (codes 430–437), acute myocardial infarction (codes 410), diabetes (codes 250), hypertension (codes 401–405), mental disorders (codes 290–319), alcohol-related illness (codes 291, 303, 305, 571.0, 571.1, 571.2, 571.3), liver cirrhosis (codes 571.2, 571.5, 571.6), hyperlipidemia (codes 272.0, 272.1, and 272.2), chronic obstructive pulmonary disease (codes 491, 492, 496), and cholecystitis (codes 574). The insurance codes (D8, D9) were used to identify medical dialysis of kidney.
Based on our previous drug-related studies12,13,14,15, we defined people who visited medical care (included outpatient, inpatient, and emergency care) and received a physician’s prescription for metformin under the coverage of Taiwan’s National Health Insurance Program. The prescription of metformin was identified from the medication records of payment of Taiwan’s National Health Insurance Program. In this study, we check the date of prescription of metformin and confirm that the use of metformin fall at time point after an attack of pancreatitis. We collected and calculated the cumulative use of metformin during the follow-up period.
To avoid immortal time bias (which might result in overestimation of the intervention’s beneficial effects) in the metformin group, we followed up the pancreatitis patients from the first date when they received metformin after index the diagnosis of pancreatitis until December 31, 2013 or until an event (developed a acute ASCVD, lost to follow-up, or death). The follow-up time, in person-years, was calculated for each pancreatitis patient from the index date to the end-point. We compared the risk of an incident acute ASCVD during the follow-up period between the pancreatitis patients who received metformin treatment and those who did not.
Statistical analyses
We compared sociodemographic factors (age, sex and low income) and coexisting medical conditions (diabetes, hypertension, mental disorders, alcohol-related illness, liver cirrhosis, hyperlipidemia, chronic obstructive pulmonary disease, cholecystitis, and renal dialysis) in the cohorts of patients with and without pancreatitis using chi-square tests. In the overall population and subgroup analysis stratified by age and sex, we used multivariate Cox proportional hazard models to calculate the adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for acute ASCVD associated with pancreatitis. The effects of pancreatitis-related diseases and metformin medication on the risk of acute ASCVD in patients with pancreatitis were also evaluated using Cox proportional hazard models.
Results
Under the frequency matching procedure, there were no significant differences in age or sex between subjects with and without pancreatitis (Table 1). Higher proportions of low income, diabetes, hypertension, mental disorders, alcohol-related illness, liver cirrhosis, hyperlipidemia, chronic obstructive pulmonary disease, cholecystitis, and renal dialysis were found in pancreatitis patients than in subjects without pancreatitis (all p < 0.05).
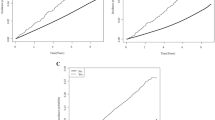
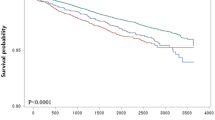
As shown in Table 2, a higher incidence of acute ASCVD was found in patients with acute (11.8 per 1000 person-years) and chronic (17.7 per 1000 person-years) pancreatitis than in those without pancreatitis (6.81 per 1000 person-years, p < 0.0001) during the follow-up period. The corresponding HR of acute ASCVD associated with acute pancreatitis and chronic pancreatitis were 1.76 (95% CI 1.47–2.12) and 3.42 (95% CI 1.69–6.94), respectively. Among people with 1 (HR 2.01, 95% CI 1.49–2.71) and ≥ 2 (HR 2.02, 95% CI 1.53–2.67) medical conditions, pancreatitis was associated with the risk of acute ASCVD. Table S1 showed the stratified analyses (by sex and age) for the risk of acute ASCVD in patients with acute and chronic pancreatitis.
Compared with people without pancreatitis (Table 3), those with acute pancreatitis who had alcohol-related illness (HR 4.66, 95% CI 3.24–6.70), liver cirrhosis (HR 4.44, 95% CI 3.05–6.47), diabetes (HR 2.61, 95% CI 2.03–3.36), and cholecystitis (HR 2.24, 95% CI 1.30–3.87) were more likely to have acute ASCVD. The increased risk of ASCVD was found in patients with chronic pancreatitis who had alcohol-related illness (HR 9.49, 95% CI 3.78–23.8), liver cirrhosis (HR 7.31, 95% CI 1.81–29.5), and diabetes (HR 6.89, 95% CI 2.18–21.8). In patients with acute pancreatitis, the use of metformin ≥ 2 times (HR 0.30, 95% CI 0.17–0.50) was associated with a reduced risk of ASCVD.
During the follow-up period (Table 4), patients with acute pancreatitis had an increased risk of acute myocardial infarction (HR 1.75, 95% CI 1.11–2.74) or stroke (HR 1.76, 95% CI 1.44–2.15). The risks of hemorrhagic stroke (HR 2.14, 95% CI 1.42–3.23), ischemic stroke (HR 1.46, 95% CI 1.05–2.02), and other stroke (HR 1.62, 95% CI 1.17–2.23) were associated with acute pancreatitis. Chronic pancreatitis was associated with risk of stroke (HR 4.20, 95% CI 2.07–8.56), included ischemic stroke (HR 6.20, 95% CI 2.25–17.1) and other stroke (HR 3.78, 95% CI 1.19–12.0).
Table S2 showed the stratified analyses for the risk of acute myocardial infarction in patients with acute and chronic pancreatitis. Table S3 showed the stratified analyses for the risk of stroke in patients with acute and chronic pancreatitis.
Discussion
Our population-based cohort study showed that patients with pancreatitis had increased risks of acute ASCVD, including acute myocardial infarction and stroke. The association between pancreatitis and acute ASCVD was significant in various subgroups. Patients with pancreatitis showed higher risks of acute ASCVD as well as complications such as liver cirrhosis, diabetes, and cholecystitis. Our study also reported the safety of metformin in patients with pancreatitis.
The association between pancreatitis and acute ASCVD could not be clarified completely in this observational study, we reviewed some relevant studies to explain the mechanism. First, the endothelium is considered a regulator of vascular homeostasis. Inflammation may cause endothelial dysfunction, which contributes to the initiation and progression of atherosclerosis2. Inflammation of the pancreas causes the aggregation of neutrophils, macrophages, and injured pancreatic acinar cells, releasing cytokines such as interleukin (IL)-10, IL-6, tumor necrosis factor-α, transforming growth factor-β, platelet-derived growth factor, and the chemokine monocyte chemoattractant protein-111,16. These inflammatory cytokines play a pivotal role in the pathogenesis of atherosclerosis17,18. These inflammatory cells further enhance inflammation and tend to precipitate unstable or ruptured atherosclerotic plaques. Second, severe hemodynamic disturbances such as profound hypotension and hypovolemia decrease coronary artery or cerebrovascular perfusion8. Third, metabolic disturbances include hyperglycemia and hyperlipidemia, which exert equal stimulatory effects on platelet activation and vascular events19,20.
The long-term effect of gallstone disease on cardiovascular outcomes is highly debated21,22,23,24. Although we investigated that pancreatitis patients with cholecystitis had increased risk of acute ASCVD in this study, we recommend further prospective studies to examine this epiphenomenon.
Post-pancreatitis diabetes mellitus is an exemplar secondary diabetes that represents a sequela of pancreatitis—the most common disease of the exocrine pancreas25,26. People have at least two-fold higher lifetime risk of develo** diabetes after an attack of pancreatitis than those in the general population25. Both basic research and population-based study provide strong evidence suggesting that hypertriglyceridemia could be involved in the pathophysiology of acute ASCVD20,27,28. We considered that the effect of hypertriglyceridemia as the etiology of acute pancreatitis as well as a risk factors for severe disease and the potential link with cardiovascular disorders.
It has been shown that the use of metformin is beneficial for reducing the risk of cardiovascular events in diabetic patients24,29. Growing evidence suggests that metformin has a protective effect against acute ASCVD beyond its hypoglycemic effects29,30. Possible explanations for the cardio-protective role of metformin may be due to its pleiotropic effects, including antioxidant, improved endothelial cell function, decreased smooth muscle cell migration, decreased cholesterol deposition and anti‑inflammatory activities, which may reduce atherosclerotic plaques29,31. Furthermore, metformin has been reported to reduce the levels of certain inflammatory cytokines involved in pancreatitis, as mentioned previously30. Our study is the first to report that the use of metformin is associated with a reduced risk of acute ASCVD in patients with pancreatitis. However, these interesting findings need to be verified by future randomized clinical trials.
Among people with post-pancreatitis diabetes mellitus, ever users of metformin had a significantly lower mortality, whereas ever-users of insulin did not have a significantly changed risk of mortality compared with never users of antidiabetic medications32. Therefore, metformin promotes a survival benefit in people with post-pancreatitis diabetes mellitus. Previous studies found that 23% and 30% of people after the first attack of acute pancreatitis and chronic pancreatitis developed post-pancreatitis diabetes mellitus, respectively25. Individuals with post-pancreatitis diabetes mellitus had higher rate of all-cause mortality than those with type 2 diabetes and metformin monotherapy is recommended as the first-line therapy for post-pancreatitis diabetes mellitus25.
Emerging data suggest that the acute, recurrent acute and chronic forms of pancreatitis represent a disease continuum33. Although clinical factors and pancreatic enzymes have been identified, discriminating between acute and chronic pancreatitis in individual patients remains difficult. We included patients with pancreatitis irrespective of chronicity to ensure diagnostic accuracy, and our report is comparable with previous studies7,10,11,34,35.
The limitations of this present study are as follows. First, information on each individual’s socioeconomic characteristics, lifestyle factors, physical examination results, laboratory measurements, and imaging results was unavailable in Taiwan’s National Health Insurance database. Smoking is an important factor for the association between pancreatitis and ASCVD. It is one of our study limitations that the information of smoking is not available in the database of Taiwan’s National Health Insurance. Second, although our results showed that use of metformin is associated with a decreased risk of acute ASCVD, the compliance of medication intake is one of study limitations.
In conclusion, we reported that patients with acute or chronic pancreatitis were more likely to have acute ASCVD, particularly those with pancreas-related comorbidities, while the use of metformin is associated with a reduced risk of acute ASCVD. Our results highlight the importance of using a multidisciplinary team to adopt an integrated approach to prevent patients with pancreatitis from develo** acute ASCVD. Further clinical trials are warranted to provide more evidence regarding the beneficial effects of metformin on reducing acute ASCVD in this susceptible population.
Abbreviations
- ICD-9-CM:
-
International Classification of Diseases, 9th Revision, Clinical Modification
- CI:
-
Confidence interval
- HR:
-
Hazard ratio
- ASCVD:
-
Atherosclerotic cardiovascular disease
References
Benjamin, E. J. et al. Heart Disease and Stroke Statistics-2019 update: A report from the American Heart Association. Circulation 139(10), e56-528 (2019).
Badimon, L., Padró, T. & Vilahur, G. Atherosclerosis, platelets and thrombosis in acute ischaemic heart disease. Eur. Heart J. Acute Cardiovasc. Care 1(1), 60–74 (2012).
Gimbrone, M. A. Jr. & García-Cardeña, G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ. Res. 118(4), 620–636 (2016).
Li, Y. H. et al. 2017 Taiwan lipid guidelines for high risk patients. J. Formos. Med. Assoc. 116(4), 217–248 (2017).
Banks, P. A., Conwell, D. L. & Toskes, P. P. The management of acute and chronic pancreatitis. Gastroenterol. Hepatol. 6(2 Suppl 3), 1–16 (2010).
Petrov, M. S. & Yadav, D. Global epidemiology and holistic prevention of pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 16(3), 175–184 (2019).
Chung, W. S. & Lin, C. L. Incidence and risk of acute coronary syndrome in patients with acute pancreatitis: A nationwide cohort study. Pancreatology 17(5), 675–680 (2017).
Vasantha Kumar, A., Mohan Reddy, G. & Anirudh Kumar, A. Acute pancreatitis complicated by acute myocardial infarction—A rare association. Indian Heart J. 65(4), 474–477 (2013).
Singh, V. K., Yadav, D. & Garg, P. K. Diagnosis and management of chronic pancreatitis: A review. JAMA 322(24), 2422–2434 (2019).
Hsu, M. T., Lin, C. L. & Chung, W. S. Increased risk of acute coronary syndrome in patients with chronic pancreatitis: A nationwide cohort analysis. Medicine 95(20), e3451 (2016).
Wong, T. S. et al. Chronic pancreatitis correlates with increased risk of cerebrovascular disease: A retrospective population-based cohort study in Taiwan. Medicine 95(15), e3266 (2016).
Huang, Y. C. et al. The protective effect of statins against pressure ulcers in stroke patients: A propensity-score matched study based on a real-world database. Atherosclerosis 317, 22–28 (2021).
Chen, T. L., Yeh, C. C., Lin, C. S., Shih, C. C. & Liao, C. C. Effects of red yeast rice prescription (LipoCol Forte) on adverse outcomes of surgery. QJM 112(4), 253–259 (2019).
Lin, C. S. et al. Outcomes after surgery in patients with diabetes who used metformin: A retrospective cohort study based on a real-world database. BMJ Open Diabetes Res. Care 8(2), e001351 (2020).
Chen, T. L. et al. Evaluating risk of incident diabetes between patients who used lovastatin and red yeast rice prescriptions (LipoCol Forte): A retrospective cohort study based on a real-world database. Diabetes Metab. Syndr. Obes. 13, 89–98 (2020).
Habtezion, A. Inflammation in acute and chronic pancreatitis. Curr. Opin. Gastroenterol. 31(5), 395–399 (2015).
Ramji, D. P. & Davies, T. S. Cytokines in atherosclerosis: Key players in all stages of disease and promising therapeutic targets. Cytokine Growth Factor Rev. 26(6), 673–685 (2015).
Tousoulis, D., Oikonomou, E., Economou, E. K., Crea, F. & Kaski, J. C. Inflammatory cytokines in atherosclerosis: Current therapeutic approaches. Eur. Heart J. 37(22), 1723–1732 (2016).
Pawelczyk, M., Kaczorowska, B. & Baj, Z. The impact of hyperglycemia and hyperlipidemia on plasma P-selectin and platelet markers after ischemic stroke. Arch. Med. Sci. 13(5), 1049–1056 (2017).
Ohmura, H. Triglycerides as residual risk for atherosclerotic cardiovascular disease. Circ. J. 83(5), 969–970 (2019).
Olaiya, M. T., Chiou, H. Y., Jeng, J. S., Lien, L. M. & Hsieh, F. I. Significantly increased risk of cardiovascular disease among patients with gallstone disease: A population-based cohort study. PLoS One 8(10), e76448 (2013).
Lv, J. et al. Gallstone disease and the risk of ischemic heart disease. Arterioscler. Thromb. Vasc. Biol. 35(10), 2232–2237 (2015).
Yu, K. J. et al. Gallstone disease is associated with arterial stiffness progression. Hypertens. Res. 40(1), 31–34 (2017).
Hong, J. et al. Effects of metformin versus glipizide on cardiovascular outcomes in patients with type 2 diabetes and coronary artery disease. Diabetes Care 36(5), 1304–1311 (2013).
Petrov, M. S. Diagnosis of endocrine disease: Post-pancreatitis diabetes mellitus: Prime time for secondary disease. Eur. J. Endocrinol. 184(4), R137–R149 (2020).
Quilliot, D. et al. Diabetes mellitus worsens antioxidant status in patients with chronic pancreatitis. Am. J. Clin. Nutr. 81(5), 1117–1125 (2005).
Roubille, F. et al. Is hypertriglyceridemia atherogenic?. Presse Med. 47(9), 757–763 (2018).
Saadatagah, S. et al. Coronary heart disease risk associated with primary isolated hypertriglyceridemia; A population-based study. J. Am. Heart Assoc. 10(11), e019343 (2021).
Luo, F. et al. Metformin in patients with and without diabetes: A paradigm shift in cardiovascular disease management. Cardiovasc. Diabetol. 18(1), 54 (2019).
Cameron, A. R. et al. Anti-inflammatory effects of metformin irrespective of diabetes status. Circ. Res. 119(5), 652–665 (2016).
Jenkins, A. J., Welsh, P. & Petrie, J. R. Metformin, lipids and atherosclerosis prevention. Curr. Opin. Lipidol. 29(4), 346–353 (2018).
Cho, J., Scragg, R., Pandol, S. J., Goodarzi, M. O. & Petrov, M. S. Antidiabetic medications and mortality risk in individuals with pancreatic cancer-related diabetes and postpancreatitis diabetes: A nationwide cohort study. Diabetes Care 42(9), 1675–1683 (2019).
Sankaran, S. J. et al. Frequency of progression from acute to chronic pancreatitis and risk factors: A meta-analysis. Gastroenterology 149(6), 1490–1500 (2015).
de la Iglesia, D. et al. Pancreatic exocrine insufficiency and cardiovascular risk in patients with chronic pancreatitis: A prospective, longitudinal cohort study. J. Gastroenterol. Hepatol. 34(1), 277–283 (2019).
Yegneswaran, B., Kostis, J. B. & Pitchumoni, C. S. Cardiovascular manifestations of acute pancreatitis. J. Crit. Care 26(2), e11–e18 (2011).
Acknowledgements
This study is based in part on data obtained from Taiwan’s Ministry of Health and Welfare. The authors’ interpretations and conclusions do not represent Taiwan’s Ministry of Health and Welfare.
Funding
This work was supported in part by The Higher Education Sprout Project by the Ministry of Education (DP2-109-21121-01-N-08-04) and Taiwan’s Ministry of Science and Technology (MOST106-2314-B-038-036-MY3; MOST108-2221-E-038-006; MOST110-2314-B-038-108-MY2).
Author information
Authors and Affiliations
Contributions
L.C.S. and C.C.L.: conception and design, analysis and interpretation of the data, drafting the article, critical revision of the manuscript for important intellectual content and final approval of the version to be published. C.C.C., C.S.L., C.C.Y., Y.G.C., and T.L.C.: conception and design, interpretation of the data, critical revision of the manuscript for important intellectual content and final approval of the version to be published. All authors have read and approved the submitted manuscript. TLC has equal contribution with the corresponding author.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sung, LC., Chang, CC., Lin, CS. et al. Risk of acute atherosclerotic cardiovascular disease in patients with acute and chronic pancreatitis. Sci Rep 11, 20907 (2021). https://doi.org/10.1038/s41598-021-99915-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-99915-4
- Springer Nature Limited
This article is cited by
-
Increased ERCP-related adverse event from premature urgent ERCP following symptom onset in acute biliary pancreatitis with cholangitis
Scientific Reports (2024)
-
Hsa_circ_0032389 Enhances Proliferation and Migration in PDGF-BB-Induced Human Aortic Vascular Smooth Muscle Cells
Cardiovascular Toxicology (2024)
-
Risk of cardiovascular disease and mortality in patients with diabetes and acute pancreatitis history: a nationwide cohort study
Scientific Reports (2022)