
Abstract
Objective
To study the epidemiology and landscape of ocular infections in patients undergoing microbiological investigations across a multi-tier ophthalmology network in India.
Methods
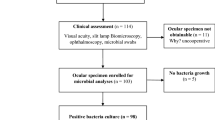
This cross-sectional hospital-based study included 15,822 patients in whom microbiology samples were analysed between September 2013 and December 2021. Ocular tissue of patients in whom a microbiology sample was processed in at least one eye were included. The data were collected using an indigenously developed electronic medical record system.
Results
Among the 15,822 patients, bacteria (51.06%) was the most common aetiology followed by fungus (38.27%). The majority of the patients were male (68.10%) and adults (90.01%). The most common age group was during the sixth decade of life with 2,914 (18.42%) patients. The patients were more commonly from the lower socio-economic status (51.61%) and from the rural geography (46.82%). Majority of the specimens sent for microbiological analysis were corneal scra**s (68.61%) followed by vitreous (8.77%). The most common bacteria isolated was Staphylococcus aureus (14.45%) followed by Pseudomonas aeruginosa (12.53%) and among the fungus were Fusarium (30.53%) and Aspergillus species (29.86%). Acanthamoeba (1.26%) and Microsporidia (0.38%) accounted for a minority of the infections in the samples. Fungus (53.10%; p ≤ 0.00001) and virus (51.08%; p = 0.000673) aetiology was found to be significantly higher in patients presenting from the rural geography.
Conclusion
The most common aetiology of infection in ocular disease is bacterial but fungal infections also accounted for a significant proportion. The majority of the patients with ocular infections presented from the rural geography and from lower socio-economic status.
Similar content being viewed by others

Introduction
Ocular infections cause an unprecedented challenge for healthcare systems and communities worldwide, not only because of their visual complications but also their social and economic consequences [1, 2], and these include keratitis, conjunctivitis, blepharitis, dacryocystitis, orbital cellulitis and endophthalmitis manifestations [3,4,5,6]. Compared to Western countries, agrarian and tropical regions have greater incidence of traumatic infections in addition to post-surgical and systemic induced ocular morbidities, and the poor are at the greatest risk [4,5,6]. Management and empirical therapy for such infections demands knowledge of the aetiological landscape and patient dynamics across environmental settings. A central challenge to studying the spectrum of these infections is the uneven distribution of burden of blindness due to these infections, distinct clinical presentations and skewed socio-economic factors. Analysing such data is additionally cumbersome and prone to human errors. Increased adoption of electronic medical records (EMRs) in clinical settings, and the subsequent emergence of big data analytics in health care is opening new door to personalised medical therapies and precision medicine [7]. These EMRs are digital versions of a patient’s health related information and documentation, gathered in real time and stored in an electronic format, designed to facilitate clinical decision making and workflow to enhance the quality and safety of healthcare [8, 9].
However, while prevalence and studies on trend analysis of ocular disorders is available in the western literature, there are inadequate studies from the eastern region of the world detailing the use of electronic health record systems to describe the distribution of ocular infections and its effect on eye health in the population. Also, the landscape epidemiology of ocular infections is not well studied, and most are restricted to single infection disorders like keratitis or endophthalmitis [3,4,5,6,7] or have small sample size. Ultimately the goals of public health ophthalmic-microbiology is to recognise and help at-risk populations and to ensure delivery of intervention programs and access to eye care to ultimately support eye health.
There is a paucity of literature on the microbiology profile of ocular diseases in the Indian population. The purpose of this study was to unravel the demographic patterns and frequency of ocular infections from the microbiology laboratory database using an indigenously developed EMR system (eyeSmart™) of a large three-tier ophthalmology network in South India and to describe the possibility of real-time analytics from a huge cohort of labelled datasets. This study also reviewed the pathogenic landscape of the different types of ocular infections in over >15,000 patients, in order to come up with substantial real time information for ophthalmologists and policy makers who deals with infections of the eye.
Materials and methods
Study design, location and time-period
This is a cross-sectional, observational, large hospital-based study and included all patients in whom microbiology samples were analysed between September 2013 and December 2021 to a three-tier ophthalmology network located in India [10]. The three-tier eyecare model of LVPEI includes 176 vision centres that provide primary care in districts and villages in the states of Andhra Pradesh, Telangana, Odisha and Karnataka. These are linked to 18 secondary eyecare centres, which are in turn linked to LVPEI tertiary centres in Hyderabad (Telangana), Visakhapatnam (Andhra Pradesh), Vijayawada (Andrea Pradesh) and Bhubaneswar (Odisha). A detailed description of the LVPEI model of patient eyecare delivery is described at the LVPEI website (http://www.lvpei.org/about-us). LVPEI’s Centre of Excellence at Hyderabad is at the apex of the Eye Care Pyramid. The medical records of all patients who presented to any of these Centres during the period were reviewed.
Either guardians of the patient or the patient themselves filled out a standard consent form for privacy of their digital eye health data during registration at the hospital. The patient parameters used for data analysis were practically non-identifiable. The patient’s clinical data were collected into a standard template of the browser-based electronic medical records system (eyeSmart EMR) during a comprehensive ophthalmic examination by uniformly trained ophthalmic personnel and supervised by an ophthalmologist. The microbiology requisition and the subsequent reports of the patients were entered into the EMR as well [11]. The study was approved by the Institutional Ethics Committee [LEC-BHR-R-12-21=788] and adhered to the Declaration of Helsinki.
Cases
A total of 15,822 patients in whom microbiology samples was analysed combinedly at the three tertiary centres and one centre of excellence of the multi-tier ophthalmology network during the study period. The eyeSmart EMR was screened for patients whose ocular tissue was processed for microbiological work-up in at least one eye. The microbiology samples were processed under standard protocols involving direct microscopy and culture and the organism where possible was identified using the VITEK-2 machine for bacterial isolates and spore and colony characteristics for fungal isolates.
Data retrieval and processing
The data of 15,822 patients included in this study were retrieved from the electronic medical record database and segregated into an excel sheet. The columns included the data on patient demographics, specimen information, smear report, culture report, the organism identified and were exported for analysis. The excel sheet with the required data was then used for analysis using the appropriate statistical software. Standardised definitions were used for defining geographic delineation based on urban, rural or metropolitan areas of the country and socio-economic status in relation to others, based on income, education, and occupation.
Statistical analysis
Descriptive statistics using mean ± standard deviation and median with inter-quartile range (IQR) were used to elucidate the demographic data. All tables for age, gender, geography, socio-economic status and microbiology reports were drawn by using Microsoft Excel (Microsoft Corporation 2018. Redmond, USA). Chi square test (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP) was used for univariate analysis to detect statistically significant differences if any among the groups. An interactive analysis of the dataset is available at the following weblink – https://www.lvpei.org/aeye/microbiology.html.
Results
Overall, 15,822 patients had a microbiology sample from at least one eye analysed at the tertiary centres of the multi-tier ophthalmology network during the study period. The overall summary comparing all the aetiology according to gender is detailed in Table 1. The decade wise distribution of the patients is described in Fig. 1A and the geographical trends of the aetiology is detailed in Fig. 1B. The state wise distribution is given in Fig. 2. We find that a lot of concentration of patients was from the 3 states where we are actively present. The trends in ocular infections and its distribution month wise across the multi-tier network is given in Table 2, which reveals that there was no seasonal distribution among the patients seen. The landscape of infections diagnosed and managed across the network is shown in Fig. 3.

A Decade wise distribution of patients with an analysis of a microbiology sample. B Geography wise distribution of the aetiology of the ocular infection.

State wise distribution of patients who presented to the institute with ocular infections.

Graphical representation of landscape of ocular infections diagnosed across the network.
Bacterial aetiology
There were 8079 (51.06%) patients diagnosed with bacterial aetiology. There were 5377 (66.56%) male and 2702 (33.44%) female patients. The majority were adults in 6910 (85.53%) patients followed by paediatric in 1169 (14.47%) patients. The mean age of the patients was 44.36 ± 22.13 years while the median age was 48 (IQR: 28–62) years and mode was 61 years. The most common age group of the patients were distributed between 61 and 70 years (n = 1398; 17.30%) followed by 51 and 60 years (n = 1379; 17.07%). The patients presented more commonly from the urban geography (n = 4017; 49.72%) and from the lower socio-economic status (n = 4082; 50.53%). Among the tissue analysed, corneal scra** accounted for the majority in 4515 (55.89%) patients followed by vitreous in 1125 (13.92%) patients and pus in 356 (4.41%) patients. Gram positive cocci were isolated in 4621 (53.13%) patients, gram positive bacilli in 1379 (15.85%) patients, gram negative bacilli in 2673 (30.73%) patients and gram negative cocci in 25 (0.29%) patients. The most common organism isolated was Staphylococcus aureus in 1257 (14.45%) patients followed by Pseudomonas aeruginosa in 1090 (12.53%) patients and Streptococcus pneumoniae in 936 (10.76%) patients.
Fungal aetiology
There were 6055 (38.27%) patients diagnosed with fungal aetiology. There were 4240 (70.56%) male and 1815 (29.98%) female patients. The majority were adults in 5761 (95.14%) patients followed by paediatric in 294 (4.86%) patients. The mean age of the patients was 46.58 ± 16.79 years while the median age was 47 (IQR: 36–60) years and mode was 46 years. The most common age group of the patients were distributed between 41 and 50 years (n = 1339; 22.11%) followed by 51 and 60 years (n = 1227; 20.26%). The patients presented more commonly from the rural geography (n = 3215; 53.10%) and from the lower socio-economic status (n = 3253; 53.72%). Among the tissue analysed, corneal scra** accounted for the majority in 5004 (82.64%) patients followed by corneal button in 293 (4.84%) patients and vitreous in 163 (2.69%) patients. Fusarium species were isolated in 2032 (30.53%) patients, Aspergillus species in 1987 (29.86%) patients, Unidentified dematiaceous fungus in 558 (8.38%) patients and Curvularia species in 333 (5%) patients. The most common organism isolated was Aspergillus flavus in 1359 (19.38%) patients followed by Fusarium solani in 697 (10.17%) patients.
Viral infections spectrum
There were 830 (5.25%) patients diagnosed with viral aetiology. There were 586 (70.6%) male and 244 (29.4%) female patients. The majority were adults in 765 (92.17%) patients followed by paediatric in 65 (7.83%) patients. The mean age of the patients was 45.35 ± 19.2 years while the median age was 47 (IQR: 34–60) years and mode was 35 years. The most common age group of the patients were distributed between 41 and 50 years (n = 166; 20%) followed by 51 and 60 years (n = 148; 17.83%). The patients presented more commonly from the rural geography (n = 424; 51.08%) and from the higher socio-economic status (n = 440; 53.01%). Among the tissue analysed, corneal scra** accounted for the majority in 654 (78.8%) patients followed by vitreous in 73 (8.8%) patients and anterior chamber aspirate in 62 (7.47%) patients. Herpes Simplex Virus (HSV-1) was isolated in 812 (97.83%) patients, Cytomegalovirus (CMV) in 13 (1.57%) patients, Varicella Zoster virus (VZV) in 4 (0.48%) patients and Adenovirus in 1 (0.12%) patients.
Mixed aetiology
There were 619 (3.91%) patients diagnosed with mixed aetiology. There were 419 (67.69%) male and 200 (32.31%) female patients. The majority were adults in 576 (93.05%) patients followed by paediatric in 43 (6.95%) patients. The mean age of the patients was 47.34 ± 18.56 years while the median age was 50 (IQR: 35–61) years and mode was 51 years. The most common age group of the patients were distributed between 51 and 60 years (n = 131; 21.16%) followed by 41 and 50 years (n = 121; 19.55%). The patients presented more commonly from the urban geography (n = 330; 53.31%) and from the lower socio-economic status (n = 328; 52.99%). Among the tissue analysed, corneal scra** accounted for the majority in 457 (73.83%) patients followed by vitreous in 27 (4.36%) patients and foreign body in 17 (2.75%) patients. A combined bacterial and fungal infection was isolated in 599 (96.76%) patients, combined bacterial and acanthamoeba infection in 20 (3.23%) patients. The most common organism isolated among bacteria was Staphylococcus aureus in 101 (16.32%) patients and among fungus was Aspergillus flavus in 105 (16.96%) patients.
Parasitic infections
There were 239 (1.51%) patients diagnosed with parasitic aetiology. There were 152 (63.60%) male and 87 (36.40%) female patients. The majority were adults in 229 (95.82%) patients followed by paediatric in 10 (4.18%) patients. The mean age of the patients was 40.56 ± 15.99 years while the median age was 39 (IQR: 30–51) years and mode was 36 years. The most common age group of the patients were distributed between 31 and 40 years (n = 63; 26.36%) followed by 21 and 30 years (n = 48; 20.08%). The patients presented more commonly from the rural geography (n = 118; 49.37%) and from the higher socio-economic status (n = 127; 53.14%). Among the tissue analysed, corneal scra** accounted for the majority in 225 (94.14%) patients followed by corneal button in 9 (3.77%) patients and corneal biopsy in 2 (0.84%) patients. Acanthamoeba was isolated in 179 (74.9%) patients and Microsporidia was isolated in 60 (25.1%) patients.
Discussion
Increasing rates of ocular infections is responsible for increased ocular damage and high degree of morbidity globally [12]. This study aimed to understand the microbiology landscape of ocular infections in a huge cohort of patients presenting to a large ophthalmology based multi-tier network in India using electronic health records-based data analytics. eyeSmart™ EMR is an indigenously developed EMR system and includes digitisation of clinical records across nearly 200 centres of the LVPEI network, including 3 Tertiary Centres, and a Centre of Excellence, across the states of Telangana, Andhra Pradesh and Odisha. L V Prasad Eye Institute (LVPEI) eye health pyramid model has a centre of excellence (CoE) at the apex catering to 50 million population followed by tertiary centres (TC), each serving a population of 5 million. At the next level, secondary centres (SC) cover 0.5–1 million population, followed by vision centres (VC) at the primary level for 50,000 population. At present, the network covers four Indian states, Andhra Pradesh (AP), Telangana state (TS), Odisha, and Karnataka state (KS) [10]. CoE and TCs are in urban locations whereas SCs and VCs are in rural areas and touches all levels of society, from remote rural villages to busy urban centres [10]. From primary eye care to advanced tertiary (quaternary). Integrating EMR data–based phenotypes into the existing health information systems is an important step for improving healthcare quality. This information allows us to perform big data analytics that have now evolved from the hundreds and thousands to millions and billions of data points that allows data mining to gather new information with transformative benefits. The primary purpose of the study was to provide an overview of the socio-demographic profile and microbiological aetiology in all types of ocular samples across the network.
Our study found bacteria to be the most common aetiology of infection in ocular disease followed by fungal infections with an equitable distribution of patients accessing eye care services. A male gender predisposition was noted among patients who presented to the LVPEI network and this was in all categories of infections, probably due to the significant association with ocular trauma and this pattern was also observed in previous studies [13, 14]. Interestingly, bacterial and fungal infections were seen mostly in patients >60 years, the average age of patients with viral and parasitic infections were <50 years. While similar associations between increasing age and bacterial and fungal infections has been reported in literature [5, 6, 12, 13], the trends in viral and parasitic infections is surprising. The study also revealed that the spectrum of infections did not follow any seasonal trend, though there was a slight peak coinciding with the rainy season in India, but this difference was not statistically significant. Especially because ocular infections are mostly associated with trauma, also indicates its prevalence throughout the year. In addition, S. aureus was the most frequent aetiology of ocular infections combined in the present study, which is consistent with similar studies done USA [15], United Kingdom [16] and other parts of India [17]. P. aeruginosa was however the second most common isolate which is typical to this part of the world [5, 6, 17].
Power BI by Microsoft has taken the world of artificial intelligence, data analytics and visualisation of reports by storm. Whether the data points are in in the form of text files, spreadsheets, or databases, it can be explored and edited to load the platform for Analytical insights of research data. In this study, an attempt has been made to demonstrate that the microbiology dataset of can be easily transformed by Power BI into a visual report and dashboards, to help assess the burden and epidemiology of ocular infections. In our study, we found that the cornea and anterior segment infections constituted about two-thirds of the ocular infections seen in the network. Considering the environmental risk factors along with socio-economic conditions for infectious diseases along with the at-risk populations, we cannot expect the incidence of these infections to reduce without population-based intervention. The novelty of this study is that we have used Power BI to map the diagnosis with a large, comprehensive, and systemic population-based cohort which provides a chance to investigate the prevalence along with the interactions of environment and personal lifestyle with disease onset and progression, across levels of care. The main aetiologies of ocular infections, including bacteria, fungi and parasites, are often clinically indistinguishable and any attempt to reduce their burden must take the broad range of causative organisms into consideration. Rethinking ocular infections in this manner may improve our current poor understanding of its global epidemiology and provide the necessary information to generate interest among regional health agencies. This study provides a baseline for map** of key endemic areas and establishment of disease surveillance systems, particularly in areas where no such data exists as well as develop innovations in the treatment of recalcitrant infections that predominate in low-income countries. It also helps in the design of relevant national antimicrobial prescribing guidelines for ophthalmic infections, especially for primary and secondary care where there may be a high proportion of patients do not undergo microbiological sampling according to age groups and include earlier adoption of alternative agents, and tailoring prescribing policies by patient age and clinical setting.
The limitations of this study include a patient referral bias to a tertiary care institute, and lack of data on systemic status of the population and the analytics being based only on the distribution of ocular infections and not their treatment per se. Duplication of patient records might also be a possible limitation in the respective tertiary centres though we have tried to minimise on the same. Another possibility is that our search did not involve all qualifiable datasets in the field. However, some strengths should be highlighted which include a huge cohort of patients with complete distribution and demographics of ocular infections in patients seeking ophthalmic services in a large ophthalmic hospital-based network in South India. EMR based data analytics allowed rapid visualisation of disease classification and helped to accelerate the dissemination of information to ophthalmologists needed to make informed clinical decisions, and advocacy makers who may use them to assess population-based real time information for making public health decisions, and understand evolving trends with regard to the burden of ocular diseases to design the effective prevention strategies.
In conclusion, this study aimed to describe the microbiological landscape of ocular infections in patients presenting to a multi-tier ophthalmology network in India. The findings show that the most common aetiology of infection in ocular disease is bacterial followed by fungal infections. The majority of the patients with ocular infections presented from the rural geography and from lower socio-economic status. Further research is required to establish the scope of practice for EMR data quality assessment.
Summary
What was known before
-
Trend analysis of ocular infections is are restricted to single infection disorders and have small sample size. Additionally, there is no study, detailing the use of electronic health record systems to describe the distribution of ocular infections and its effect on eye health in the population.
What this study adds
-
This study proves that fungal infections account for a significant proportion in this part of the world. While there was an equitable distribution of patients accessing eye care services, no seasonal variation was observed or majority of the patients with ocular infections presented during the fifth and sixth decade of life and were from the rural geography.
Data availability
The data generated in this study is available at the following weblink – https://www.lvpei.org/aeye/microbiology.html and further clarifications are available with the corresponding author on request.
References
Miller D. Update on the epidemiology and antibiotic resistance of ocular infections. Middle East Afr J Ophthalmol. 2017;24:30–42.
Teweldemedhin M, Gebreyesus H, Atsbaha AH, Asgedom SW, Saravanan M. Bacterial profile of ocular infections: a systematic review. BMC Ophthalmol. 2017;17:212.
Epling J. Bacterial conjunctivitis. Clin Evid. 2012;2:704.
Joseph J, Karolia R, Sharma S, Choudhary H, Naik MN. Microbiological profile and antibiotic susceptibility trends in orbital cellulitis in India: an analysis over 15 years. Orbit 2021;23:1–7.
Das S, Samantaray R, Mallick A, Sahu SK, Sharma S. Types of organisms and in-vitro susceptibility of bacterial isolates from patients with microbial keratitis: a trend analysis of 8 years. Indian J Ophthalmol. 2019;67:49–53.
Joseph J, Sontam B, Guda SJM, Gandhi J, Sharma S, Tyagi M, et al. Trends in microbiological spectrum of endophthalmitis at a single tertiary care ophthalmic hospital in India: a review of 25 years. Eye. 2019;33:1090–5.
Lee S, Doktorchik C, Martin EA, D’Souza AG, Eastwood C, Shaheen AA, et al. Electronic medical record–based case phenoty** for the Charlson conditions: sco** review. JMIR Med Inf. 2021;9:e23934 https://doi.org/10.2196/23934
Adler-Milstein J, Jha AK. HITECH act drove large gains in hospital electronic health record adoption. Health Aff. 2017;36:1416–22.
Gagnon MP, Payne-Gagnon J, Breton E, Fortin JP, Khoury L, Dolovich L, et al. Adoption of electronic personal health records in Canada: perceptions of stakeholders. Int J Health Policy Manag. 2016;5:425–33.
Rao GN, Khanna RC, Athota SM, Rajshekar V, Rani PK. Integrated model of primary and secondary eye care for underserved rural areas: the L V Prasad Eye Institute experience. Indian J Ophthalmol. 2012;60:396–400.
Das AV, Kammari P, Vadapalli R, Basu S. Big data and the eyeSmart electronic medical record system - an 8-year experience from a three-tier eye care network in India. Indian J Ophthalmol. 2020;68:427–32.
Ayehubizu Z, Mulu W, Biadglegne F. Common bacterial causes of external ocular infections, associated risk factors and antibiotic resistance among patients at ophthalmology unit of Felege Hiwot Referral Hospital, Northwest Ethiopia: a cross-sectional study. J Ophthal Inflamm Infect. 2021;11:7 https://doi.org/10.1186/s12348-021-00238-2
Srinivasan M, Gonzales CA, George C, Cevallos V. Epidemiology and aetiological diagnosis of corneal ulceration in Madurai, south India. Br J Ophthalmol. 1997;81:965–71.
Ormerod LD, Hertzmark E, Gomez DS, Stabiner RG, Schanzlin DJ, Smith RE. Epidemiology of microbial keratitis in southern California. A multivariate analysis. Ophthalmology 1987;94:1322–33.
Sand D, She R, Shulman IA, Chen DS, Schur M, Hsu HY. Microbial keratitis in los angeles: The doheny eye institute and the los angeles county hospital experience. Ophthalmology. 2015;122:918–24.
Silvester A, Neal T, Czanner G, Briggs M, Harding S, Kaye S. Adult bacterial conjunctivitis: resistance patterns over 12 years in patients attending a large primary eye care Centre in the UK. BMJ Open Ophthalmol. 2016;11:e000006.
Bharathi MJ, Ramakrishnan R, Shivakumar C, Meenakshi R, Lionalraj D. Etiology and antibacterial susceptibility pattern of community-acquired bacterial ocular infections in a tertiary eye care hospital in South India. Indian J Ophthalmol. 2010;58:497.
Acknowledgements
The authors wish to acknowledge the Hyderabad Eye research Foundation and the support of our Department of eyeSmart EMR & AEye team specially Mr. Ranganath Vadapalli and Mr. Mohammad Pasha. Hyderabad Eye Research Foundation, Hyderabad, India.
Author information
Authors and Affiliations
Contributions
The corresponding author states that authorship credit of this manuscript was based on 1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; 2) drafting the article or revising it critically for important intellectual content; 3) final approval of the version to be published. All listed authors met conditions 1, 2, and 3. All persons designated as authors qualify for authorship, and all those who qualify are listed. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Das, A.V., Joseph, J. The microbiological landscape and epidemiology of ocular infections in a multi-tier ophthalmology network in India: an electronic medical record driven analytics report. Eye 37, 1590–1595 (2023). https://doi.org/10.1038/s41433-022-02191-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-022-02191-3
- Springer Nature Limited