
Abstract
Virtual crime scene investigation using numerical models has the potential to assist in the forensic investigation of firearm-related fatalities, where ethical concerns and expensive resources limit the scope of physical experiments to comprehend the post-impact biomechanics comprehensively. The human cranial numerical model developed in this study incorporates three main components (skin, skull, and brain) with dynamic biomaterial properties. The virtual model provides valuable insights into the post-impact biomechanics of cranial ballistic injuries, particularly in high-speed events beyond conventional investigative capabilities, including the velocity of ejected blood backspatter, cavitation collapsing, and pressure waves. The validation of the numerical model, both quantitatively and qualitatively, demonstrates its ability to replicate similar bone fractures, entrance wound shapes, and backward skin ballooning observed in physical experiments of the human cranial geometry. The model also yields similar temporary cavity sizes, wound sizes, and blood backspatter time against the physical cranial model, aiding in bloodstain pattern analysis. Additionally, the numerical model enables exploration of ballistic factors that vary in each crime scene environment and influence cranial injuries, such as projectile type, velocity, impact location, and impact angle. These established injury patterns contribute to crime scene reconstruction by providing essential information on projectile trajectory, discharge distance, and firearm type, assisting in the resolution of court cases. In conclusion, the developed human cranial geometry in this study offers a reliable tool for investigating firearm-related cranial injuries, serving as a statistical reference in forensic science. Virtual crime scene investigations using these models have the potential to enhance the accuracy and efficiency of forensic analyses.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
One of the primary focal topics in cranial ballistic forensic investigations and subsequent court resolutions is the determination of the manner of decease, whether it is classified as homicide or suicide. This analysis involves a comprehensive examination of the cause of injury, such as the range and type of calibre employed, as well as assessing viable post-penetration biomechanical scenarios, including wound morphology and blood backspatter characteristics. Backspatter represents an important aspect of molecular ballistics, which serves as a forensic methodology to analyse the biological traces generated in firearm-related crime scenes [1]. The term “backspatter” refers to the ejection of biological debris from a wound entrance in the opposite direction of the trajectory of a projectile. In cranial injuries, backspatter consists of a complex mixture comprising brain tissue, skin tissue, bone fragments, adipose debris, and blood [2, 3]. However, comprehending the intricate formation of backspatter poses challenges due to the complex combination of three main mechanisms: (1) subcutaneous gas effects, (2) temporary cavitation, and (3) tail splashing [4,5,6,7,8,9].
Ballistic factors vary in different crime scene environments, including the angle of impact, speed and type of the projectile, anatomical impact location, and range of shot. These influence the post-impact firearm-related wound characteristics, post-impact biomechanics, and the severity of cranial injuries [10, 11]. A comprehensive understanding of the effects of these factors enables the effective evaluation of evidence during forensic investigations.
For many years, the utilisation of numerical techniques has garnered significant interest in the field of biomedical engineering as an economical choice [12]. Employing computational simulations to recreate cranial ballistic impacts offers advantages, such as ease of modification of ballistic factors in a repetitive manner and adherence to ethical rightfulness. Moreover, the computational method can facilitate post-ballistic impact analysis, enabling the visualisation of the model at a specific layer and location. Consequently, stress, strain, and internal pressure within each layer can be obtained, in contrast to the physical model that has challenges in integrating measurement devices. Furthermore, this technique assists in validating actual crime scene investigations without interfering with any physical evidence.
The first pioneer of biomechanical skull-brain modelling under a penetrating ballistic condition was the study by Pintar et al. [13] in 2001. Subsequently, numerous experts have attempted to establish reliable finite element-based models of both the human head and its surrogate, particularly in personal protection development [14,15,16]. The conventional finite element method was used to analyse complex biological structures by discretising them into interconnected mesh elements with shared nodes [17].
Several researchers [18,19,20,21] have employed 3D simple block models to evaluate a viable brain surrogate, aiming to replicate post-impact behaviours similar to those of the human brain. Wang et al. [22] and Wen et al. [23] conducted both experimental and numerical investigations involving pistol projectiles penetrating a gelatine block, serving as a soft tissue simulant. Their studies focused on examining the temporary cavitation and the trajectory of the projectile after impact. Notably, both approaches demonstrated a similar movement of the projectile, highlighting the consistency between experimental and computational findings. The result indicated that an increase in the angle of attack and projectile velocity led to a larger maximum temporary cavity and greater dissipation of kinetic energy. Additionally, radial movement of the gelatine perpendicular to the projectile flight direction caused the expansion of the temporary cavity [23, 24].
Chen et al. [25] and Xu et al. [26] adopted a porcine bone geometry for their numerical simulations and subsequent experimental validation. They established the correlation between the porcine bone experiments and their simulations in terms of wound appearances. Due to the challenge associated with conducting human head experiments, an animal model was introduced to provide a reasonable validation approach. Nonetheless, the animal model remains controversial due to the differences in geometry and biological properties compared to the human cranium. Subsequently, researchers [27,28,29,30,31] numerically investigated ballistic impacts using three different projectiles (0.40, 0.380 and 9 × 19 mm) at different impact locations on human skulls. They found that the highest velocity ammunition, the 9 × 19 mm projectile, caused a rounded wound entrance on the frontal skull. Conversely, the lowest velocity projectile, the 0.40 flat point nose, produced an irregular wound shape [29]. This event indicated that the shape of a projectile influenced the wounding mechanism. However, in these studies, skin and brain parts, which are the other two crucial cranial structures, were absent. Tang et al. [32] and Zhen et al. [33] also adopted the human mandible and compared their results with porcine head models reported in [25, 26], assuming that post-impact damage observed in porcine heads might be comparable to that in human heads.
The conventional finite element-based models encountered limitations in maintaining the integrity of elements during highly non-linear impact fracture and explosion events due to the incapability of handling high-velocity impacts and large deformations, which compromised the accuracy. To address this, mesh-free smoothed particle hydrodynamics (SPH), initially introduced by [34], has been proposed to improve the accuracy of simulations because of its capabilities of effectively capturing the high-strain plastic deformation in ballistic events and fragmentation [35].
SPH solves a system of partial differential equations by discretising the model into a series of particles. Each particle represents a specific material density and volume. Some recent biomechanics studies employed the SPH model, such as in femoral cortical bone remodelling [36] and ballistic impacts on the plate geometries of skull simulants [2]. Kwon et al. [4] conducted a ballistic penetration to an anatomical SPH model of the human head, which consisted of two layers, the cranial skin and the cranium or brain-encased bone. Biomaterials were utilised for the simulation. Adopting biomaterials as human head surrogates in both physical and computational models provided a straightforward way of validating the accuracy of numerically generated post-impacted responses. Consequently, the physical head model experiment and simulation using the same biomaterials were compared, revealing a good agreement in terms of the timing of first backspatter generation and wound morphology. Backspatter from tail splashing and temporary cavitation was observed. The researchers also noted that the percentage of energy received by both the cranial skin and cranium did not significantly depend on the velocity of a projectile.
Overall, research on numerical ballistic impact simulation on the human head remains limited in comprehensively comprehending post-impact biomechanics. Most studies have focused only on the skull layer, with the exception of Kwon et al. [4], who included the skin layer. Consequently, the absence of the brain component indicates that there is plenty of room for further development in accurately replicating the post-impact human cranial behaviours. The strain rate sensitivity or the material behaviour that varies with speed has been overlooked by simplifying it as static material behaviour. Additionally, the numerical simulations specifically targeting molecular ballistics are still scarce in forensic applications. Furthermore, only a limited range of data is available regarding the influences of ballistic factors on post-impact biomechanics.
In the present study, a three-layered numerical model of a female human head was developed. This novel model consisted of the skin, skull, and brain, represented by various biomaterials that replicate the biomechanical properties of the respective layers. The SPH-based anatomical geometry model was constructed with the aim of simulating ballistic projectile impacts and investigating post-ballistic responses of the head model. The SPH method was employed due to its capability to capture large deformations effectively. Furthermore, the SPH approach facilitated the replication of blood particles that spatter after impact, which is crucial for forensic investigations in ballistic incidents. For the first time, this study encompassed several key findings related to cranial ballistic injuries, including (1) the post-impact ballistic and wound ballistic mechanisms of the model and a comparison with experimental data from the literature; (2) quantitative dynamic responses of the simulation, such as stress, pressure wave, and kinetic energy; and (3) a parametric study of crime scene ballistic factors, namely, skin properties, impact location, impact angle, and projectile type, as well as modelling parameters, such as element size.
2 Materials and modelling methods
The research methodology of SPH numerical simulations involved four major stages: (1) human cranial geometry and projectile generation, (2) SPH modelling creation, (3) parametric studies of ballistic factors, and (4) the post-processing stage. In the first stage, human cranial and projectile geometries were obtained from the utilisation of MRI scans and computer-aided design techniques. These geometries were then prepared as solid models. Three-layered solid models representing the human cranial structure (skin–skull–brain) were established. In the second stage, the solid models were discretised into particles with the desired resolution. Material constitutive models were appropriately selected for each layer of the cranial geometry. Initial condition values and dynamic analysis modelling parameters were imposed. Subsequently, various crime scene ballistic factors were altered, including impact location and angle. Finally, the simulations solved the specified problems and produced the defined research outcomes.
2.1 Model geometry creation
The human cranial geometry used in this study was procured from a voluntary MRI dataset provided by the Auckland Bioengineering Institute at The University of Auckland, New Zealand, and was approved by The University of Auckland Human Participants Ethics Committee. The MRI dataset was selected based on sex, age, and thickness of the skin layer to represent an average normal human condition. In this research, a female MRI image was adopted to compare the results with those of previous studies [4, 7]. The age selected for the MRI dataset was between 20 and 25 years old, as this age group has been identified as having the highest casualties in ballistic incidents [37]. The thicknesses of the skin and skull layers were determined based on the average values.
The MRI images were segmented into three regions, skin, skull, and brain, using imaging software called Stradwin and Creo Parametric to digitise each layer boundary. Subsequently, the skin layer was extrapolated from the skull using the average thickness of human skin. The geometries were smoothed and verified to ensure that the brain volume (1.18 × 106 mm3) closely matched the average female intracranial volume of 1.29 × 106 mm3 [38]. The volumes of the skin and skull layers were measured as 0.45 × 106 mm3 and 0.54 × 106 mm3, respectively. The solid parts and MRI images of the human cranial model are depicted in Fig. 1a, b.

The human skin-skull-brain a solid geometry from b an MRI image (University of Auckland) and the solid geometries of c 9 mm, d 0.22 LR, and 0.45 ACP projectiles
Solid parts representing 9 mm Luger (FMJ) (8 g), 0.22 LR (3 g), and 0.45 (15 g) projectiles are illustrated in Fig. 1c–e. They were created based on drawings of projectiles by the manufacturer. The model did not include the projectile cartridge to simulate realistic ballistic penetration. The projectiles have a solid lead core with a copper jacket. The projectiles were then constrained to contact the desired impact location on the human cranial.
2.2 SPH modelling
SPH is a meshless or particle-based continuum method used for numerical simulations. This method discretises the model into a series of particles, where each particle represents a specific material volume. These particles can be assigned various properties, functions and attributes. In the case of cranial injury simulations, SPH can be used to predict parameters, such as stress, strain, displacement, and velocity, by smoothing kernel interpolation, which solves a system of partial differential equations using the Lagrangian method.
The interpolation function is a cubic spline Gaussian function (Bell curve), which represents an analytical weighting function (kernel). The weighting function has compact support defined by a circular shape in a two-dimensional problem or a spherical shape in a three-dimensional problem. The spherical shape domain has a radius, called smoothing length, from its centre at the desired location of interest. The surrounding particles located inside the support smoothing radius are selected for the weighting interpolation of the interested variables at the centre point. Subsequently, the weighting interpolation model is applied to all particles in the model to achieve continuum distributions of the relevant parameter [36].
2.2.1 SPH particle size
In order to generate the desired particles and element sizes, the human cranial and projectile models were imported to mesh in ANSYS Workbench 19.2. The software provided effective meshing capabilities using tetrahedral elements for the geometries. A nearly even distribution of the meshes was achieved to ensure numerical accuracy and SPH stability. The meshed model was then exported as an input file for further SPH generation in LS-PrePost 4.8 software.
Initially, the skin and skull layers were meshed with an element size of 1.5 mm, while the brain component, having the highest volume, was meshed with a 3 mm element size. Subsequently, the meshes for the skin and skull layers were refined to 1.0 mm and 0.7 mm, which was the finest refinement allowance, considering the available computational power and memory in this research. The limitation arises from the significant increase in the number of neighbouring particles within the smoothing radius of each particle. These small mesh sizes were selected to replicate realistic blood spatter, as most blood spatters observed in animal and physical model experiments were below 1 mm [39]. Furthermore, the SPH element size of approximately 1 mm was considered to be adequate, according to [40].
A high-performance research computing environment provided by the National Computational Infrastructure in Australia was utilised to simulate these large-scale simulations, as shown in Table 1. However, the LS-DYNA software also limited the total number of particles in the model, with a maximum of 7 digits in the single precision version. Additionally, Kwon [40] highlighted the need to limit the number of particles to around 5 million per model to avoid truncation errors of the SPH method. Therefore, the baseline human cranial model was meshed using the finest element size available of 0.7 mm. Subsequently, the SPH method was implemented, as depicted in Fig. 2.

SPH generation of a the human cranial geometry subjected to a 9 mm projectile and b cross-sectional geometries of the brain (yellow), skull (orange), and skin (pink) layers. (Color figure online)
2.2.2 Material models
The simulated models comprise four distinct parts: the projectile, skin, skull, and brain. The accurate representation of their material properties is crucial for obtaining reliable and realistic simulation results when using biomaterial as a substitution for human biological parts. Each layer exhibits different material behaviours, which were mathematically described through constitutive material models available in the LS-DYNA material library. The suitable material models were selected for each part based on their mechanical characteristics. The material input parameters for the skin layer were obtained directly from experimental data, while those for the skull and brain layers were procured from the previous studies [4, 40]. The surrogate materials for the skull and brain parts have been validated and deemed suitable for ballistic simulations.
The material properties of the human skin and its silicone-based skin simulant were found to exhibit sensitivity to strain rate [41, 42]. Specifically, the behaviour of the skin simulant at high strain rates (4000 s−1) was significantly stiffer compared to its behaviour at the quasi-static strain rate (0.48 s−1) [42, 43]. This difference implies that the quasi-static material properties cannot be directly applied in the ballistic study, where the strain rates exceed 4000 s−1. As the strain rate increases, the silicone-based skin simulant behaves as a hyperelastic material, a combination of elastic and non-linear viscous material. Among the available hyperelastic models in LS-DYNA, the Ogden model (*MAT_077-O_OGDEN_RUBBER) was selected as it closely matched the experimental curves of the silicone-based composite skin simulant under both quasi-static and dynamic conditions [42]. In contrast, the Mooney–Rivlin model is suitable for the rubber material under less than 100% strain or less deformation, as opposed to this ballistic study. The skin simulant was modelled as an incompressible isotropic hyperelastic material, and its properties were extracted from compressive testing at various strain rates, as presented in Table 2. Multiple skin properties were employed to explore the influence of skin material properties on the post-ballistic responses of the model.
The skull simulant used in this study was urethane material (TC-891). The material properties were obtained from a previous study by Kwon [40]. An isotropic elastic-perfectly plastic material model with a specified failure strain was employed to represent the behaviour of the skull simulant. The material card, *MAT_013_ISOTROPIC_ELASTIC_FAILURE, was utilised, and its input parameters are presented in Table 3. The chosen material model is suitable for the skull simulant since the failure strain criteria of this model can accurately capture the fracture behaviour of the skull under ballistic impacts.
In this study, a gelatine material with a concentration of 10%, commonly used in ballistic events, was adopted as a brain simulant. The gelatine demonstrates viscoelastic behaviour, which means it can dissipate a portion of impact energy through hysteresis, emulating the energy absorption characteristic of the brain. The viscoelastic model, *MAT_006_VISCOELASTIC, was selected, and its specific material input parameters are shown in Table 4. In this ballistic simulation, the blood component was ignored to simplify the model. However, the model still included other portions of the backspatter, the debris of the skin, skull, and brain.
The copper jacket of a projectile is the first component to interact with the target, making its material properties essential to understanding the impact dynamics. In this study, the material properties of copper were obtained from the Johnson–Cook model [44], which is commonly used to describe the material response under large strains and high strain rates. These material properties were adopted from the Johnson–Cook copper material database in ANSYS, as shown in Table 5. However, the density of the projectiles was replaced with that of lead to replicate the realistic kinetic energy input to the model since the projectiles were made of lead with a copper cover jacket.
2.2.3 Initial condition and boundary constraints
The impact velocity of the projectiles was set to vary within the range of 350–380 m/s based on the manufacturer data of each projectile. To represent the connection between the cranial model and the neck, the lower region of the human cranial models was constrained with a pinned boundary condition, as visualised in Fig. 3. This boundary condition restricts the translation of the bottom part of the cranium to simulate a realistic movement. Additionally, other modelling parameters, such as the smoothing length of the particles, memory allocation, and artificial bulk viscosity, were set according to the specific requirements of the study mentioned earlier.

a Constraint conditions and b various post-impact injury responses of the human cranial model subjected to a ballistic projectile
2.3 Ballistic factors
The sensitivity studies of the modelling parameters, including skin material inputs and element size, were conducted to investigate their impact on the post-impact responses of the model. Regarding the crime scene investigation, it is important to consider the variation in ballistic conditions that can affect cranial injuries and physical evidence in each crime scene scenario. These factors include the projectile impact location, projectile angle of attack, projectile type, and projectile velocity, which can be influenced by air drag over long ranges. Table 6 provides an overview of the variation of these ballistic factors in the present study.
2.4 Simulation and result analysis
The simulations were executed using LS-Dyna SPH module in ANSYS 19.2 on the computer cluster (NCI, Australia). During the simulations, the position and velocity of each particle were updated at each time step interval. The software allows visualisation and analysis of the simulation results, providing quantitative measurements of various parameters, such as stress, strain, time history, and the size of wounds and cavities. The post-ballistic impact biomechanics and cranial injuries were categorised into two groups, qualitative behaviours and quantitative responses, as shown in Table 7; Fig. 3b. The qualitative characteristics can be observed from experimental and simulation methods, facilitating a comparison between the two approaches. On the other hand, the quantitative simulation results are primarily used for parametric studies to analyse the sensitivity of the alteration of ballistic factors.
3 Results and discussion
3.1 Validation with physical experiments
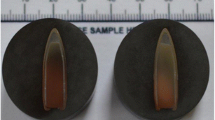
The simulation results were validated by comparing them with a physical model consisting of three components: skin, skull, and brain, developed by Kwon [40]. The physical model shared the same material properties as this numerical model to assess the accuracy and reliability of the developed numerical model. For post-impact qualitative response validation, the skin deformation in the numerical model exhibited a ballooning mechanism similar to that observed in the physical model, as depicted in Fig. 4a. Both numerical and physical approaches generated circular wound shapes in Fig. 4b. Furthermore, the computational model successfully reproduced the skull fractures observed in the physical model, as shown in Fig. 4c,d. The radial fractures originating from the entrance and extending through the middle and back of the skull were accurately captured by the numerical model. The simulation also generated small branches of cracks on the top of the skull, stemming from the main radial crack, which was consistent with the observation made in the physical model. The numerical model also replicated the radial fractures at the exit. Additionally, the SPH numerical simulation also generated a circular entrance shape of the skull, which is consistent with the findings of previous studies [27, 28]. It is worth noting that the circular entrance shape was reported to occur in approximately 82% of real human skull cases [45]. On the contrary, the skull layer in the numerical model exhibited an irregular exit wound, which was also observed in the physical model [40] and the previous study [46], specifically under the ballistic impact at the left parietal and temporal skulls. Overall, the qualitative validation of the post-ballistic impact simulation results against the physical model and the human skull demonstrated that the developed numerical model was able to replicate important characteristics and behaviours, including skin deformation, wound shape, and skull fractures.

Qualitative comparison of a skin deformation, b entrance wound morphology, c skull fractures at the projectile entrance, and d skull fractures at the projectile exit between the ballistic simulation subjected to a 9 mm projectile, the physical model [40], and the human skull in temporal bone [46, 47]
Additionally, the quantitative validation of the ballistic simulation was also carried out. The skin ballooning height in the simulation, represented by the purple dot in Fig. 5a, falls within the range of both animal and physical human head models in both full cranial (P model) and half cranial (P model- HC) physical models. This measurement and the skin ballooning observed in the qualitative response indicate that the numerical model accurately captures the skin deformation and the resulting ballooning effect caused by the ballistic impact. The skin cavity diameter predicted by the numerical model is on the lower end of the range observed in both animal and physical models, as shown in Fig. 5b. This difference may arise from the variations in the ballistic setup, such as the projectile velocity or material properties.

Comparison of a skin ballooning height, b skin cavity diameter, c time duration of the collapse of skin (STC) and brain cavities (BTC) and the generation of the first and second backspatters between the simulation, the physical model of half cranial (HC) and full, and animal experiments [5, 40, 48]. d The ejected velocity of the backspatter particle. The considered craniums were subjected to an impact with a 9 mm projectile
Figure 5c illustrates the time duration of first and second backspatters and their sources of generation, which are the STC and BTC cavities collapse. The simulation accurately recreates the timing of the first backspatter and skin collapse, matching the results from the physical models. It is observed that the beginning and end of the first backspatter occur before the initiation and completion of STC, respectively.. This phenomenon has also been reported in [40]. However, the occurrence of the second backspatter in the simulation is slightly earlier compared to the physical models. Since other outer skull and skin layers entirely enclose the brain part, it is important to note that the inability to capture the collapse of the brain cavity in experiments highlights the advantage of numerical simulations in providing insights into complex phenomena. The larger size of the temporary cavity of the brain compared to the skin leads to a longer pulsation and collapse time. As a result, the duration of the second backspatter is longer than the first backspatter. In general, two main backspatters are generated from firearm-related injuries. The first backspatter, which occurs prior to the complete collapse of the skin and brain cavities, corresponds to tail splashing. This phenomenon has been successfully replicated by this numerical simulation. The second blood spatter, resulting from the collapse of the brain temporary cavity, was also captured by the simulation at a subsequent timeframe. This phenomenon is indicated by the termination of the second backspatter that occurs before the complete collapse of the brain temporary cavity. The simulation results demonstrate that the numerical model is capable of capturing two distinct mechanisms that contribute to the generation of backspatters.
The analysis of the ejected particle velocity, as depicted in Fig. 5d, can provide insight into the potential blood stain location. Initially, the velocity of the ejected particle from the first backspatters rapidly increases until the formation of backward skin ballooning occurs at stage (1), attributed to the radial displacement and stretching of the skin at 0.2 ms. This mechanism, as described in [8, 49], leads to a decrease in particle velocity due to the dissipation of energy. After the collapse of the skin ballooning at approximately 0.5 ms in stage (2), the repulsion force drives the particle and accelerates its velocity. At its maximum velocity, stage (3), the velocity begins to decline as the particle collides with other released particles and eventually reaches a stable state at stage (4). The similar behaviour of the velocity profile was reported by [4]. Regarding the velocity ranges, the numerical model exhibits particle velocities between 15 and 60 m/s for the first backspatter, which is consistent with the reported range of 13 to 61 m/s in [39]. Similarly, the velocity range of the second backspatter is between 10 and 50 m/s. By analysing the backspatter ballistic, the simulation can aid in the interpretation and reconstruction of crime scenes involving firearm-related injuries.
3.1.1 Stress and pressure wave
The ballistic pressure wave generated by a projectile impact radiates both radially and axially from the impact area [5, 18, 50], as illustrated in Fig. 6a. When the pressure wave passes through the cranium, it induces continuous oscillation, resulting in local compression (indicated by the blue colour) and tension (indicated by the light green colour) within the tissue. The outer surface of the cavity experiences compression, causing it to press and narrow down the temporary cavity, which can be identified as the projectile path in this simulation due to the reaction from the brain during the transfer of the kinetic energy from the projectile into the internal energy of the brain. On the other hand, the skull develops stress in the radial direction from the entrance to the exit wound over time, as depicted by the red colour. This stress distribution highlights the effects of the pressure wave on the skull. Notably, the ballistic pressure shockwave travels and propagates faster than the projectile. This phenomenon causes the pre-existing stress at the exit site from the pressure wave before the projectile impacts, resulting in a larger exit wound [51].

Stress wave propagation, with a limited range between -4 and 8 MPa, through the penetrating time of the SPH model subjected to a 9 mm projectile impact in a the coronal and b sagittal cross-sectional views
The propagation of the circumference stress wave is believed to be responsible for the formation of radial cracks in the skull from the entrance to the exit wound, as illustrated in Fig. 6b. Additionally, the temporary cavitation of the brain is hypothesised to cause indirect skull fractures in high-stress areas [52]. In this study, it is observed that the stress wave in the skull propagates at the same speed as the propagation of the stress wave in the temporary cavity. This phenomenon may reflect that the stress wave in the temporary cavity contributed to the propagation of the stress wave in the skull. However, there is limited direct supporting evidence about the relation between the stress wave in the temporary cavity and the skull fracture.
Figure 6b also shows the maximum stress distribution, with the highest stress observed in the skull. The areas of high stress at 1 and 1.4 ms are at the frontal lobe base and around the occipital lobe base. These findings correspond well with the studies by [40, 53, 54], providing supporting evidence for the localisation of high stresses and fractures in specific regions of the head during ballistic impacts. In the current study, the maximum stress of the head model ranges between 52 and 81 MPa in the skull layer. These values are lower than those reported in [30, 31], which are between 97 and 182 MPa, under the impact at temporal and occipital regions, respectively. The difference in stress values can be attributed to the inclusion of the skin layer in the current study. Some of the stress and damage from the impact have been transferred to the skin layer, resulting in relatively lower stress values in the skull layer.
In the skin layer, a maximum compressive stress of around 4 MPa is observed, and it is localised at the entrance wound. This stress value is comparable to the maximum stress in the skin layer reported in [4]. The high stress in the skin layer causes it to stretch and pulsate due to its hyperelastic behaviour, attempting to recover its original state after the projectile enters the cranium.
There is limited data in the literature to compare kinetic energy dissipation because many of these studies did not include the brain in the models. The brain plays a crucial role in absorbing a significant portion of the kinetic energy transferred from the projectile during the penetration. As a result, the responses of a model with a skull-encased brain differ from those conducted with a block of gelatine brain simulant, which has fewer constraints on the brain.
The importance of including the essential cranial parts in the model and ensuring anatomical correctness can be observed when examining the energy absorption during the post-impact cranial injuries, as indicated by the velocity of the projectile in Fig. 7. In this case, the projectile dissipates more than 40% of its energy while penetrating the skin and skull. The skull absorbs the energy from the projectile and expresses it in terms of crack formation. Another portion, approximately 40%, is dissipated through the brain. This behaviour highlights the significant effect that suitable material properties and the incorporation of the main layers of the head have on the ballistic impact and the overall understanding of cranial injuries.

The velocity of a 9 mm projectile over time during penetration at the right temple
3.1.2 Skin property sensitivity
The investigation on the influence of skin biomaterial properties on the post-ballistic impact response of the numerical simulation revealed some significant findings. There was no significant difference in the skin ballooning height among the simulations with different strain rate skin properties, as shown in Fig. 8a. This response indicates that the strain rate sensitivity of the skin biomaterial did not have a major impact on the skin deformation in terms of ballooning height. However, the simulations with medium and low strain rate skin properties generated larger skin cavity diameters compared to the simulation with high strain rate skin properties and the physical models in [5, 40, 48], as presented in Fig. 8b. The numerical model with quasi-static (low strain rate) skin properties exhibited the largest skin and brain temporary cavity size. This suggests that the strain rate sensitivity of the skin affects the skin cavity expansion under impact.

Comparison of a skin ballooning height, b skin cavity diameter, and c time and duration of the collapse of skin and brain cavities and the generation of the first and second backspatters between the simulations with high (4000 s−1), medium (50 s−1), and low strain rate (0.48 s−1) skin properties subjected to a 9 mm projectile and the physical model
The additional results of this study indicate that the diameter of the skin entry wound varies depending on the strain rate and elasticity of the skin. The models with low and intermediate strain rate skin properties subjected to a 9 mm projectile exhibited larger entrance wound diameters, measuring 9.2 mm and 10.5 mm, respectively, compared to the model with high strain rate skin properties, which had a diameter of 7.1 mm. This difference can be attributed to the tearing of the skin due to less elasticity in models with lower strain rate properties. The entrance wound that is smaller than the diameter of the projectile was also reported in some case studies due to the elasticity of the skin [55, 56]. For a comparison, Radford [5] measured a wound diameter between 4 and 8 mm for a 9 mm projectile in a silicone model, while butchered and live porcine head experiments showed entry wounds of 7–8 mm, and 4–5 mm in non-contact shots, respectively.
The model with quasi-static skin properties, which lacks the ability to accurately represent the dynamic behaviours of the skin, can lead to the overprediction of cranial injury severity. This is evident in the earlier occurrence of blood spatter in the first and second instances, as well as the collapsing of the cavity compared to those of the model with intermediate and high strain rate skin properties, as shown in Fig. 8c. The collapse of the brain temporary cavity typically occurs 2 to 4 ms after the projectile exits the head, which is at 1 ms [8]. By incorporating stiffer skin properties into the model, the occurrence of brain cavity collapse is delayed, aligning more closely with the behaviour observed in physical models.
In terms of cranial injury severity, the models with low and medium strain rate skin properties generated higher levels of cranial injury severity, including a more significant number of skull fractures, a greater maximum size of the brain temporary cavity, tearing skin, and irregular wound shapes compared to the model with high strain rate skin properties. These findings highlight the influence of skin properties on the characteristics of cranial injuries and emphasise the need for an accurate representation of skin properties in models to improve cranial injury prediction.
3.1.3 Projectile angle of attack
Figure 9 illustrates the evolution of the projectile trajectory within a cross-sectional representation of the head model. Yawing, characterised by the deviation of the projectile from its central axis in the vertical direction, is observed in Fig. 9a since the projectile becomes susceptible to resisting force within the high-density nature of the human head, with its tissue densities approximately 800 times greater than air. Yawing induces the expansion of the wound cavity, resulting in augmented contact areas and resistance forces. Consequently, the severity of cranial damage increases as the amount of energy transferred to tissues relies on these two factors. An amplified impact angle causes the projectile to become unstable more easily, as demonstrated in Fig. 9b–d. The unstable projectile continues yawing along the projectile trajectory and cannot recover to its initial impact angle. This scenario contributes to higher levels of cranial injuries, evidenced by larger skin and brain cavities but less skin ballooning height, as shown in Fig. 10a, b, elevated stress levels in the skull and brain, increased wound diameter, and enhanced dissipation of kinetic energy, as presented in Table 8. Notably, the height of skin ballooning decreases with an increasing angle of impact, potentially attributed to the oblique shape of ballooning.

The coronal cross-sectional view of the ballistic impact simulations at 0.4 ms, 1 ms, and 2 ms subjected to a 4°, b 10°, c 15°, and d 20° impact angles of the 9 mm projectile

Comparison of a skin ballooning height, b skin cavity diameter, and c time and duration of the collapse of skin and brain cavities and the generation of the first and second backspatters between the simulations subjected to different angles of attack of the 9 mm projectile
Qualitative observations indicate that an increased angle of attack (AOA), defined as the deviation of the projectile from its central axis in the negative vertical direction, caused a greater skull damage fracture. In Fig. 11, the model with a 10° impact angle exhibits more severe skull fractures compared to the model with a 4° impact angle. Fragments of bone travel inside the brain cavity along with the projectile, as illustrated in the orange colour in Fig. 9. Additionally, the resulting entrance wound shape shows an inward bevelling and tends to deviate from circularity into an oval-like configuration with some irregularities, which correlates well with the case study in [57]. The exit wound exhibits an outward bevelling and a larger size compared to the entrance wound due to the tumbling motion of the projectile, which creates a greater contact surface area.

Skull fractures of the SPH cranial models subjected to a 4° and b 10° angles of attack of the 9 mm projectile
Regarding backspatter, the mechanism is observed whereby retentive forces propel backspatter debris back towards the entrance wound, as illustrated at 1 and 2 ms in Fig. 9. All models show no significant difference in the timing and duration of the first backspatter, as depicted in Fig. 10c. However, the start of skin collapsing is delayed in models subjected to higher angles of attack. This phenomenon correlates with the reduction in skin ballooning when the angle of attack increases.
The model with a higher angle of attack generates an earlier occurrence of the second backspatter and temporary collapsing of the brain due to the advancement of the maximum temporary cavity towards the entrance wound. Moreover, a higher angle of attack yields a more significant amount of backspatter and a higher ejected particle velocity, which describes a higher level of cranial injuries. The shape of the brain cavity in this study exhibits similarities with the findings in [23], where the furthest part of the brain near the exit displays a smaller diameter compared to the region closer to the impact entrance. This shrink of the brain temporary cavity along the projectile track is more pronounced as the angle of attack of the projectile increases.
Wang et al. [22], Wen et al. [23], and Tang et al. [32] have drawn similar conclusions regarding the post-ballistic behaviours observed in brain gelatine blocks and the human mandible. Their findings highlighted that an increase in the angle of attack leads to early instability and rolling motion of the projectile, an advancement of the maximum cavity location towards the impact side, and a higher dissipation of projectile kinetic energy [58].
The positioning of a firearm and its distance from the target can determine the angle of attack or impact of a projectile, causing different post-ballistic impact biomechanical responses. Overall, an elevated angle of attack corresponds to an overall greater cranial injury.
3.1.4 Impact location
The selection of impact locations for investigation was based on the statistical distribution of firearm-related fatalities reported by [59]. According to the study, the majority of cases involved impacts at the right temple, accounting for 67% of the total cases. The mouth region was the second most common impact location, comprising 16% of the cases. Other impact locations included the forehead (7%), left temple (6%), submental region (2%), and parietal region (1%). Therefore, the right temple, forehead, and left temple were selected in this study.
It was found that there is no significant correlation between the site of impact and the severity of cranial injuries. However, some patterns can be identified when comparing different impact regions within the same cranial side. The upper region of the cranial side exhibits more significant cranial injuries compared to the lower region, including earlier backspatter generation, higher dissipation of kinetic energy and a number of skull fractures, as well as greater entrance wound diameter and skin ballooning height, as depicted in Fig. 12a, b, with the exception of skin cavity diameter. This disparity can be attributed to the thicker bone structure in the lower region than the upper region, as illustrated in the orange colour in Fig. 2b.

Comparison of a skin ballooning height and b skin cavity between the simulations subjected to the 9 mm projectile at different impact locations
The timing of first and second backspatter occurrences was observed within the time intervals of 0–0.6 ms and 1–7 ms, respectively, across all impact locations. In the cases where the impact occurred at the forehead, the model demonstrated the least extent of cranial injuries among the various impact locations. The maximum diameter of the brain temporary cavity was found to be the smallest in cases of impact at the forehead, measuring 32 mm, whereas it expanded to beyond 36 mm in other locations. Similarly, the entrance wound diameter at the forehead was observed to be smaller at 6 mm compared to the range of 7–9 mm observed in other impact locations. It should be noted that skull fractures propagated from the entrance to the exit wound across all impact locations, as depicted in Fig. 13. The findings suggest that the location of impact can influence the resulting skull fracture. The maximum stress exerted on the skull during impact at the forehead was measured at 68 MPa, which represents the lowest value among all impact locations considered.

a Skull fracture and b stress wave propagation of the SPH cranial model subjected to the 9 mm projectile at the forehead
On the other hand, the model subjected to impact at the forehead exhibited the highest dissipation of kinetic energy compared to impacts at other locations. This can be attributed to the more extended brain cavity and the increased contact area between the projectile and the brain. These results raise an argument on the complex relationship between kinetic energy dissipation and other cranial injury behaviours. However, the maximum stress experienced by the brain did not exhibit any significant differences across the various impact sites.
3.1.5 Projectile type and velocity
The design of a projectile plays a crucial role in determining the amount of energy dissipation and how it transfers to the surrounding tissues. The velocity of a projectile can vary depending on the type of handgun calibre used. For instance, the 0.22 LR ammunition is characterised to be the smallest, shortest, and lightest among the three projectile types, while the 0.45 ACP projectile is the largest and roundest. The 9 mm projectile features a pointed nose that leads to a small interface contact. In this study, the human cranial models were subjected to ballistic impacts by these three different projectiles at the same location, specifically the right temple.
The results depicted in Fig. 14a, b indicate that the height of skin ballooning and the diameter of skin cavity are significantly influenced by the projectile diameter and, to a lesser extent, by its velocity. These differences are consistent with previous porcine experiments conducted by Kwon [40]. The higher level of cranial injuries due to an elevated diameter of the projectile is observed in the maximum diameter of the brain cavity, where the 0.22 LR projectile resulted in a diameter of 32 mm, compared to 36 mm for the 9 mm projectile and 40 mm for the 0.45 ACP ammunition. The study by Karger, Teige and Brinkmann [60] provides information on the diameter and shape of an entrance wound in a case study involving a ballistic .22LR to the chest. According to their findings, the entrance wound was circular in shape and had an approximate diameter of 5 mm. In this study, the larger calibres produce larger wound sizes. The entrance wound diameter for the 0.22 LR (5.7 mm in diameter) is 5.5 mm, while it measures 7.1 mm for the 9 mm projectile and 10.5 mm for the 0.45 ACP counterpart (11.5 mm in diameter). This trend was also reported by Henwood, Oost and Fairgrieve [61], who provided a comparison of the wound diameters of two different projectiles. Similarly, larger wound diameters are associated with elevated projectile velocities, all of which exhibit circular shapes. The stress distributions in the area adjacent to the entrance wound exhibited a similar pattern in all models, with a reduction in its intensity as the distance from the impact entrance increased.

Comparison of a skin ballooning height, b skin cavity diameter, c time and duration of the collapse of skin and brain cavities and the generation of the first and second backspatters between the simulations subjected to three different projectile types and velocities
Regarding stress on the skull, the model subjected to the 0.22 LR projectile generated the least maximum principal stress at 60 MPa, while the one subjected to the 9 mm projectile produced moderated stress. The model subjected to the 0.45 ACP ammunition, on the other hand, resulted in considerably higher stress on the skull and the most extensive bone fracturing, measuring 84 MPa, which is consistent with the literature [28, 62]. This phenomenon can be attributed to the .22LR and 9 mm projectiles being able to penetrate the skull with less resistance due to their streamlined point nose shape and the smaller contact surface. This summary was also reported in [29].
The similar effect of the projectile type also influences the amount of kinetic energy loss from the projectile, which depends on the cross-sectional area and velocity of the projectile. In this study, the .22LR projectile, which has less initial kinetic energy, could not penetrate through if the impact angle exceeded 20°. This incapability of penetration of the projectile was also highlighted in some studies [63, 64].
The influences of elevated impact velocity and weight of the projectile on damage creation have been studied in various research papers, including studies conducted on gelatine blocks [21, 65,66,67,68] and an anatomical human head model [4]. These studies concluded that higher velocities and larger projectile weights result in deeper penetration depths [20, 21, 67], higher pressure peaks after the impact [69], greater intensities of radiating impact stresses and strains [4], larger maximum temporary cavity sizes, and more perforation resistance [19, 22, 65]. Remarkably, with the same initial kinetic energy, larger mass projectiles with lower impact velocities can trigger deeper penetration depths compared to lighter projectiles [21, 65, 66, 67]. This characteristic indicates that the mass of the projectile has a greater influence on penetration depth than the initial velocity [64]. This phenomenon aligns with the findings of the present study, in which the projectile velocity did not significantly influence the energy dissipation from the projectile to the model compared to the type of projectile.
An increase in projectile size leads to a longer duration of both first and second backspatters, as illustrated in Fig. 14c, which was also observed by Kwon [40]. Additionally, the larger projectile diameters result in an earlier generation of the second backspatter, contrary to the findings of Kwon [40], who reported that only the duration of the backspatter showed a significant difference in the investigation of different projectile types. In this study, the duration of the collapse of the brain temporary cavity does not significantly change with an increase in the projectile diameter. The most significant amount of backspatters was captured in the model subjected to the 0.45 ACP, whose large diameter potentially created more debris that induced the ejection of the backspatter. On the other hand, the model subjected to the 0.22 LR projectile generated less than half of the amount of backspatter observed in the model with the 0.45 ACP ammunition. It should be noted that the first backspatter, known as tail splashing, does not occur after the last collapse of the skin cavity since the skin cavity itself is the main contributing factor. Furthermore, backspatter was generated in all three cases of different projectile types, contrary to the findings reported by Kwon [40]. Overall, the type and velocity of the projectile influence wound ballistics or geometric shape more than the molecular ballistics of backspatters.
The developed SPH numerical simulation has been validated and used to enhance understanding of post-ballistic impact biomechanics, cranial injuries severity and molecular ballistic responses. The limitations exist, such as the lack of incorporation of blood interaction, anisotropic properties of human head tissues, and the inability to replicate heat-related characteristics, including the ring of soot. The variation in biological factors, such as age, sex, and head weight, and more accurate anatomical and structural representation of the human head also require further development and investigation.
Despite these limitations, the SPH numerical model in this study offers flexibility, cost-effectiveness, and potential capabilities for studying terminal ballistics. The model has significant implications not only in the forensic field but also in other research areas, such as biomedical brain injury and defence protective design.
4 Conclusions
The study describes the development of a human cranial skin-skull-brain SPH numerical model to enhance understanding of post-ballistic impact biomechanics and cranial injuries. The virtual simulation was compared with animal and human case studies and a physical model to assess their accuracy. The numerical model successfully replicated important post-impact characteristics, such as skin deformation, wound shape, and skull fractures. Quantitative validation confirmed the ability of the model to capture key behaviours, including skin ballooning height, skin cavity diameter, and backspatter timing and duration.
The numerical results emphasised the significance of including the brain in the model, as a substantial portion of the kinetic energy of the projectile is transferred to the brain during penetration. The dynamic strain rate and elasticity of biomaterials, specifically skin, were found to influence skin deformation as well as temporary cavity expansion and collapse. The research also explored the effects of ballistic factors on the model, revealing that higher impact angles and diameters of the projectile result in more severe cranial injuries. The relationship between these factors and the post-impact biomechanics has also been established.
Overall, the SPH numerical simulation model provides valuable insights into post-ballistic impact behaviours, cranial injuries, and molecular ballistic responses. Its applications extend beyond forensic analysis to biomedical brain injury research and defence protective design.
References
Euteneuer J, Courts C (2021) Ten years of molecular ballistics—a review and a field guide. Int J Legal Med 135(4):1121–1136
Das R, Collins A, Verma A, Fernandez J, Taylor M (2015) Evaluating simulant materials for understanding cranial backspatter from a ballistic projectile. J Forensic Sci 60(3):627–637
Budday S, Sommer G, Birkl C, Langkammer C, Haybaeck J, Kohnert J, Bauer M, Paulsen F, Steinmann P, Kuhl E (2017) Mechanical characterization of human brain tissue. Acta Biomater 48:319–340
Kwon E, Singh MR, Vallabh RD, Das R, Taylor MC, Fernandez JW (2018) Modelling ballistic cranial injury and backspatter using smoothed particle hydrodynamics. Comput Methods Biomech Biomed Eng Imaging Vis 1–14
Radford GE (2010) Modelling cranial gunshot wounds and backspatter. University of Otago
Yoon GH, Mo JS, Kim KH, Yoon CH, Lim NH (2015) Investigation of bullet penetration in ballistic gelatin via finite element simulation and experiment. J Mech Sci Technol 29:3747–3759
Foote N (2012) The role of the temporary cavity in cranial Backspatter, ResearchSpace@ Auckland
Karger B (2008) Forensic ballistics. Forensic Pathol Rev 139–172
Black A, Burns BD, Zuckerman S (1941) An experimental study of the wounding mechanism of high-velocity missiles. BMJ 2(4224):872
Stefanopoulos PK, Hadjigeorgiou GF, Filippakis K, Gyftokostas D (2014) Gunshot wounds: a review of ballistics related to penetrating trauma. J Acute Dis 3(3):178–185
Berryman HE (2019) A systematic approach to the interpretation of gunshot wound trauma to the cranium. Forensic Sci Int 301:306–317
Zhang L, Ademiloye A, Liew K (2019) Meshfree and particle methods in biomechanics: prospects and challenges. Arch Comput Methods Eng 26(5):1547–1576
Pintar FA, Kumaresan S, Yoganandan N, Yang A, Stemper B, Gennarelli TA (2001) Biomechanical modeling of penetrating traumatic head injuries: a finite element approach. Biomed Sci Instrum 37:429–434
Karimi A, Razaghi R, Navidbakhsh M, Sera T, Kudo S (2016) Dynamic finite element simulation of the gunshot injury to the human forehead protected by polyvinyl alcohol sponge. J Mater Sci Mater Med 27(4):74
Pinnoji PK, Mahajan P (2007) Finite element modelling of helmeted head impact under frontal loading. Sadhana 32:445–458
Mahoney P, Carr D, Harrison K, McGuire R, Hepper A, Flynn D, Delaney RJ, Gibb I (2019) Forensic reconstruction of two military combat related shooting incidents using an anatomically correct synthetic skull with a surrogate skin/soft tissue layer. Int J Legal Med 133:151–162
Costa ST, Freire AR, Rossi AC, Daruge Junior E, Prado FB (2017) Systematic review of finite element analysis utilisation in craniofacial gunshot wounds. Aust J Forensic Sci 49(4):369–378
Datoc D (2010) Finite element analysis and modeling of a.38 lead round nose ballistic gelatin test. The faculty of California Polytechnic State University, p 274
Hub J, Komenda J, Novak M (2012) Expansion limit estimation of pistol hollow point bullet penetrating the block of substitute material. In: 18thInternational conference engineering mechanics, Svratka, Czech Republic, p 95
Frissane H, Taddei L, Lebaal N, Roth S (2018) SPH modeling of high velocity impact into ballistic gelatin. Development of an axis-symmetrical formulation. Mech Adv Mater Struct 26(22):1881–1888
Taddei L, Awoukeng Goumtcha A, Roth S (2015) Smoothed particle hydrodynamics formulation for penetrating impacts on ballistic gelatine. Mech Res Commun 70:94–101
Wang Y, Shi X, Chen A, Xu C (2015) The experimental and numerical investigation of pistol bullet penetrating soft tissue simulant. Forensic Sci Int 249:271–279
Wen Y, Xu C, ** Y, Batra RC (2017) Rifle bullet penetration into ballistic gelatin. J Mech Behav Biomed Mater 67:40–50
Liu S, Xu C, Wen Y, Wang S, Zhou J, Zhou X (2018) Cavity dynamics in 10 wt% gelatin penetration of rifle bullet. Int J Impact Eng 122:296–304
Chen Y, Miao Y, Xu C, Zhang G, Lei T, Tan Y (2010) Wound ballistics of the pig mandibular angle: a preliminary finite element analysis and experimental study. J Biomech 43(6):1131–1137
Xu C, Chen Y, Li B, Zhang L, Wang J, Kang J, Chen Z, Li X (2015) Finite element analysis vs experimental study of head firearm wound in pig. Technol Health Care 23(1):S61–70
Rodrigues LL, Costa ST, Rossi AC, Daruge Júnior E, Prado FB, Freire AR (2018) Computational simulation of projectile injuries to human parietal bone using finite element analysis. Aust J Forensic Sci 51(4):446–454
Costa ST, Freire AR, Matoso RI, Daruge Junior E, Rossi AC, Prado FB (2017) Computational approach to identify different injuries by firearms. J Forensic Sci 62(2):361–368
Matoso RI, Freire AR, Santos LS, Daruge Junior E, Rossi AC, Prado FB (2014) Comparison of gunshot entrance morphologies caused by.40-caliber Smith & Wesson,. 380-caliber, and 9-mm luger bullets: a finite element analysis study. PLoS ONE 9(10):e111192
Maciel DR (2016) Simulation of impact of firearm projectiles with different calibers on temporal bone: biomechanical characterization by finite element method. Universidade Estadual de Campinas
Quintero Y (2016) Dynamic simulation of region of the human skull—finite element analysis bullets fired at the occipital fired at the occipital finite element analysis. Universidade Estadual de Campinas
Tang Z, Tu W, Zhang G, Chen Y, Lei T, Tan Y (2012) Dynamic simulation and preliminary finite element analysis of gunshot wounds to the human mandible, Injury. Int J Care Injured 43:660–665
Zhen T, Zhonghua Z, Gang Z, Yubin C, Tao L, Yinghui T (2012) Establishment of a three-dimensional finite element model for gunshot wounds to the human mandible. J Med Colleges PLA 27(2):87–100
Gingold RA, Monaghan JJ (1977) Smoothed particle hydrodynamics: theory and application to non-spherical stars. Mon Not R Astron Soc 181(3):375–389
Taddei L, Frissane H, Lebaal N, Roth S (2017) Smoothed particle hydrodynamics–based method for penetrating impacts in a biomechanical context. Comput Methods Biomech BioMed Eng 20(sup1):S199–S200
Fernandez J, Das R, Cleary P, Hunter P, Thomas C, Clement J (2013) Using smooth particle hydrodynamics to investigate femoral cortical bone remodelling at the haversian level. Int J Numer Methods Biomed Eng 29(1):129–143
Naghavi M, Marczak LB, Kutz M, Shackelford KA, Arora M, Miller-Petrie M, Aichour MTE, Akseer N, Al-Raddadi RM, Alam K (2018) Global mortality from firearms, 1990–2016. JAMA 320(8):792–814
Matsumae M, Kikinis R, Mórocz IA, Lorenzo AV, Sándor T, Albert MS, Black PM, Jolesz FA (1996) Age-related changes in intracranial compartment volumes in normal adults assessed by magnetic resonance imaging. J Neurosurg 84(6):982–991
Karger B, Nüsse R, Brinkmann B, Schroeder G, Wüstenbecker S (1996) Backspatter from experimental close-range shots to the head: I. Macrobackspatter. Int J Legal Med 109:66–74
Kwon EE (2018) Anatomically realistic physical and computational models of cranial ballistic impact and associated backspatter, ResearchSpace@ Auckland
Trotta A, Annaidh AN (2019) Mechanical characterisation of human and porcine scalp tissue at dynamic strain rates. J Mech Behav Biomed Mater 100:103381
Chattrairat A, Kandare E, Aimmanee S, Tran P, Das R (2022) Development and characterisation of hybrid composite skin simulants based on short polyethylene fibre and bioactive glass particle-reinforced silicone. J Mech Behav Biomed Mater 136:105424
Chattrairat, A., Aimmanee, S., Kandare, E., Tran, P., & Das, R. (2023) Modelling and characterisation of the dynamic behaviours of silicone-based composite skin simulant with short polyethylene fibres and bioactive glass particles. Mechanics of Materials 184:104740
Johnson GR, Cook WH (1985) Fracture characteristics of three metals subjected to various strains, strain rates, temperatures and pressures. Eng Fract Mech 21(1):31–48
Quatrehomme G, I̊şcan MY (1998) Gunshot wounds to the skull: comparison of entries and exits. Forensic Sci Int 94(1–2):141–146
Quatrehomme G, İşcan MY (1997) Bevelling in exit gunshot wounds in bones. Forensic Sci Int 89(1–2):93–101
Quatrehomme G, I̊şcan MY (1998) Analysis of beveling in gunshot entrance wounds. Forensic Sci Int 93(1):45–60
Radford G, Taylor MC, Kieser J, Waddell JN, Walsh K, Schofield J, Das R, Chakravorty E (2016) Simulating backspatter of blood from cranial gunshot wounds using pig models. Int J Legal Med 130:985–994
Davidson PL, Taylor MC, Wilson SJ, Walsh KA, Kieser JA (2012) Physical components of soft-tissue ballistic wounding and their involvement in the generation of blood backspatter. J Forensic Sci 57(5):1339–1342
Humphrey C, Kumaratilake J (2016) Ballistics and anatomical modelling–a review. Leg Med 23:21–29
Thierauf A, Glardon M, Axmann S, Kneubuehl BP, Kromeier J, Pircher R, Pollak S, Große M, Perdekamp (2013) The varying size of exit wounds from center-fire rifles as a consequence of the temporary cavity. Int J Legal Med 127:931–936
Große Perdekamp M, Kneubuehl BP, Ishikawa T, Nadjem H, Kromeier J, Pollak S, Thierauf A (2010) Secondary skull fractures in head wounds inflicted by captive bolt guns: autopsy findings and experimental simulation. Int J Legal Med 124:605–612
Mahoney PF, Carr DJ, Delaney RJ, Gibb IE (2020) Shooting through windscreens: ballistic injury assessment using a surrogate head model—two case reports. Int J Legal Med 134(4):1409–1417
Miyazaki Y, Tachiya H, Anata K, Hojo A (2008) Measurement of pressure responses in a physical model of a human head with high shape fidelity based on CT/MRI data. Int J Mod Phys B 22(09n11):1718–1723
Vellema J, Scholtz HJ (2011) Forensic aspects of ballistic injury. Springer London, London, pp 91–121
Berryman HE, Smith OJ, Symes SA (1995) Diameter of cranial gunshot wounds as a function of bullet caliber. J Forensic Sci 40(5):751–754
Molina DK, Rulon JJ, Wallace EI (2012) The atypical entrance wound: differential diagnosis and discussion of an unusual cause. Am J Forensic Med Pathol 33(3):250–252
Karimi A, Razaghi R, Navidbakhsh M, Sera T, Kudo S (2016) Dynamic finite element simulation of the gunshot injury to the human forehead protected by polyvinyl alcohol sponge. J Mater Sci Mater Med 27:1–12
Nikolic S, Živkovic V, Babic D, Jukovic F (2012) Suicidal single gunshot injury to the head: differences in site of entrance wound and direction of the bullet path between right-and left-handed—an autopsy study. Am J Forensic Med Pathol 33(1):43–46
Karger B, Teige K, Brinkmann B (1997) Laceration of the thoracic aorta from a. 22 Lr bullet. Int J Legal Med 110:92–94
Henwood BJ, Oost TS, Fairgrieve SI (2019) Bullet caliber and type categorization from gunshot wounds in Sus scrofa (linnaeus) long bone. J Forensic Sci 64(4):1139–1144
Stuehmer C, Blum KS, Kokemueller H, Tavassol F, Bormann KH, Gellrich N-C, Rücker M (2009) Influence of different types of guns, projectiles, and propellants on patterns of injury to the viscerocranium. J Oral Maxillofac Surg 67(4):775–781
Will DD, Whiting TL (2019) Achieving humane outcomes in killing livestock by free bullet II: target selection. Can Vet J 60(10):1051
Sellier KG, Kneubuehl BP, Haag LC (1995) Wound ballistics and the scientific background, LWW
Wen Y, Xu C, Wang H, Chen A, Batra RC (2013) Impact of steel spheres on ballistic gelatin at moderate velocities. Int J Impact Eng 62:142–151
** Y, Haitao L, Cheng W, Wang X, Han R, Li R, Dong D (2019) The experimental and numerical investigation on the ballistic limit of BB-Gun pellet versus skin simulant. Forensic Sci Int 298:393–397
Al Khalil M, Frissane H, Taddei L, Meng S, Lebaal N, Demoly F, Bir C, Roth S (2019) SPH-based method to simulate penetrating impact mechanics into ballistic gelatin: toward an understanding of the perforation of human tissue. Extrem Mech Lett 29:100479
Awoukeng-Goumtcha A, Taddei L, Tostain F, Roth S (2014) Investigations of impact biomechanics for penetrating ballistic cases. Biomed Mater Eng 24(6):2331–2339
Gilson L, Rabet L, Imad A, Kakogiannis D, Coghe F (2016) Development of a numerical model for the ballistic penetration of Fackler gelatine by small calibre projectiles. Eur Phys J Special Top 225(2):375–384
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Akanae Chattrairat: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing—original draft, Writing— review & editing. Everson Kandare: Writing—review & editing, Supervision. Sontipee Aimmanee: Writing—review & editing, Investigation, Supervision. Phuong Tran: Writing—review & editing. Raj Das: Writing—review & editing, Resources, Supervision.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Ethical approval
Human Ethics Approval and Consent to Participate declarations: The MRI images voluntarily provided by individuals were approved by The University of Auckland Human Participants Ethics Committee as part of the LiFePaTH (Liggins Fetal, Perinatal and Maternal Translational Research for Lifelong Health) Group research programme.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
Supplementary Material 5
Appendix A: Numerical convergence of the SPH model
Appendix A: Numerical convergence of the SPH model
The numerical convergence of the SPH human cranial model was investigated by analysing the effect of particle size of 3, 2, 1, and 0.7 mm. It was found that when the particle size was larger than 2 mm, the projectile failed to perforate the human head. This behaviour occurred because a larger size and mass of particles require more kinetic energy to translate them. To achieve convergence, the particle size was refined, resulting in different characteristics of the backspatter. While the ejecting shape remained the same, there was a more significant amount of backspatter with smaller particle sizes, consistent with findings in [40]. Refinement of the particle size also led to changes in the skin ballooning height, cavity diameter, and entrance wound diameter, as presented in Table 9. The collapse time of the skin temporary cavity remained similar across different particle sizes. However, the forming time of the brain temporary cavity showed a delayed response associated with greater cranial injuries when using smaller particles in the simulation. Although further simulations may be needed to establish a conclusive convergence, the SPH numerical model provided a good approximation of post-ballistic impact behaviours.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chattrairat, A., Kandare, E., Aimmanee, S. et al. Understanding post-impact biomechanics of ballistic cranial injury by smoothed particle hydrodynamics numerical modelling. Comp. Part. Mech. (2024). https://doi.org/10.1007/s40571-024-00783-2
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40571-024-00783-2