
Abstract
The concept of an observatory for examining and monitoring trends for research in the social sciences and health arose from analogy with the facilities of astronomy and the realization that close and consistent observation was essential to understand interactions among determinants of health in a community. Their theoretical foundations are largely grounded in the “population health model,” an intellectual framework developed in 1974 and associated with a movement called “the new public health.” We developed an observatory for an affluent, unexceptional, suburban jurisdiction (“County 20”) in the province of Alberta, in western Canada, and used it to study and monitor both normative and emergent issues in environmental health. The observatory was conceived as a utility, or multi-purpose vehicle, for describing and responding to emerging community issues quickly and gathering data and qualitative findings as required. Case studies on issues of local importance allowed us to observe the dynamics of community response comprehensively, using quantitative and qualitative methods as appropriate. Valuable insights gleaned from the cases studied pertained to risk perception, the NIMBY syndrome, and reorganizing and auditing public health services. It did less well when the object of study was further removed from the community of interest, when there was no clear action item to be recommended, and when sponsors had expectations for certainty that could not be supported by available data sources. The observatory eventually was merged into a community health outreach program. The local observatory model is a practical, low-cost, and sustainable model for capturing generalizable and specifically local case study experience on a small scale but is limited in its effectiveness and by the scope of its coverage. It can be an initial step toward longitudinal and community monitoring studies on a larger scale. The observatory model can be used to elevate the level of case studies, impose rigor on analysis, and compile case studies for comparative and analytical studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
We developed an observatory for environmental health issues on a local level in 1985 and employed the technique for about a decade. During this relatively short period, we were able to make a number of important observations and assemble a research team that later conducted an important prospective study on a larger scale that is described elsewhere (Guidotti et al. 2000).
The initiative was originally called the “County 20 studies,” after the official municipal designation of the jurisdiction in the province of Alberta (Canada). Its operations were funded on project-by-project or informal basis from local sources. Its principal assets were access to individual investigators and staff already working on projects within the Occupational Health Program and the Department of Public Health Sciences generally and an informal and temporary network of collaborators and research assistants, assembled as the situation required.
The observatory was conceived as a utility, or multi-purpose vehicle, for responding to emerging community issues quickly and gathering data and qualitative findings as required. It was not a study in its own right nor supported by a theoretical framework, but rather a means of collecting information that might be useful in responding to the issue in real time, locking in reliable data, and reconstructing the case study from reliable data collected in a timely manner and from primary sources.
Background
The concept of an observatory for examining and monitoring trends in the social sciences arose from analogy with the facilities of astronomy and the realization that close and consistent observation was essential to understand dynamics and interactions in a community (Hackenberg 1967). The proponents of the idea also observed that events and interactions in a relatively confined community could be described in detail and that the data so derived could substitute in some respects for long-term or longitudinal studies, because “…the social sciences are data starved.” However, the primary justification for setting up “observatories” as laboratories for social science observation was to find “new theoretical breakthroughs” through intense study that could lead to the formulation of new hypotheses (Adam et al. 2015). Use of the observatory approach has since become widespread and no longer implies longitudinal data collection (Hemmings and Wilkinson 2003). Major institutions such as the World Bank (2016), UNESCO (2011), and the European University Institute (2021) have adopted the observatory model for operational purposes to guide programs in economic and social development, notably in monitoring supply and deployment of faculty at European universities. There is a network of observatories (the Social Observation Coordinating Network) funded by the National Science Foundation of the United States (Hofferth and Hubacek 2021). Crossing over from social to health trends was a logical progression; for example, the Economics Observatory at the University of Bristol (2020), supported by the Economic and Social Research Council of UK Research and Innovation, has addressed economic issues arising from the COVID-19 pandemic.
The idea of an observatory for health trends, closely monitoring trends in a defined population, appears to have arisen in France in 1974 and spread widely among health agencies on the local and regional level. The concept was adopted by several European countries and in the 1990s became a fixture in public health in the UK where it was used not only for information-gathering but to facilitate coordination among agencies and levels of government, following validation of a successful prototype in Liverpool in 1990 (Hemmings and Wilkinson 2003).
The term “observatory” with respect to health began trending in PubMed in 1990, signaling adoption of the term and concept by health professionals and embrace of the ideas of social epidemiology by the literature of mainstream medicine (Marmot 2005). As of 2003, a small literature had already accumulated using the operational definition of a program or facility that closely observed trends in a defined community with the objective of identifying modifiable social or material determinants of health, with the capacity to monitor and interpret them (Hemmings and Wilkinson 2003). Concerns have been raised that the term is overly broad and implies a strictly passive role. Others refute this perception and allow for intervention studies to be part of the agenda of observatories. They have been described by their leading proponents as having certain characteristics, among which are autonomy, a capacity to work on sensitive agendas, acceptance of intuitive “hunches,” small size, synthetic in their approach, heavily reliant on networks, and policy-oriented (Hemmings and Wilkinson 2003). All these essential characteristics applied to the observatory described here although they had not been formulated, nor was the term in common use at that time.
In general, observatories for population health have been developed without committing to a particular theoretical model. Tacitly, they appear to have avoided doing this in order to avoid bias, to stay eclectic in their methods, and to prevent interpolating a filter that would interfere with the identification of novel or unexpected trends. However, there is a theoretical grounding common to all modern population health research that informed this and other observatories: the “population health model.”
The population health model was developed and popularized by Health Canada in the 1970s as a way of defining the critical determinants of human health: social, physical (including environmental), heredity, and healthcare (Lalonde 1974). The interplay among social and material determinants of human health was a major concern of proponents of what was then called “the new public health” (the term is rarely used today), a school of thought emphasizing disparities in social determinants of health (Fig. 1). The population health model quickly went mainstream in the 1980s and remains the most influential model for understanding determinants of health and explaining health disparities. However, the population health model is based on society-level analysis, developed to inform governance of medical and public health policy. Translation of the macro-level model to a given community or situation requires further steps (Guidotti 2015). Observatories can be seen as a practical application of the population health model, monitoring how determinants of health play out in real life.

The public health model as interpreted by the Canadian Institute for Advanced Research
By 2016, the health observatory model was considered an essential institution in population health and the organizational model of choice for closely following trends in defined populations (Aspinall et al. 2016). Today, the concept of a social observatory or a health observatory is familiar and can be found at many research and academic institutions, particularly those monitoring easily harvested data such as vital statistics or social media trends. The recent experience with tracking disinformation on COVID-19 and vaccination hesitancy has proven the value of social observatories in health applications, suggesting that the method lends itself to interdisciplinary theory development as well as secular hypothesis testing. Examples include the European Union.Social observatory for disinformation and social media analysis. Available at: https:www.disinfobservatory.org. Accessed 20 January (2021). (2021) Social Observatory for Disinformation and Social Media Analysis, developed in 2018, and Indiana University (2020), both of which have uncovered evidence of deliberate spreading of misinformation on COVID-19.
However, as the concept gained acceptance, it has expanded from the original concept of a small effort monitoring health or social trends in a small area to include global monitoring efforts. The term now includes on-line data collection. The World Health Organization established in 2008 what became the Global Observatory for Health as a data linkage network, greatly increasing the scale and scope of the “observatory” concept and redefining it as global rather than local (Adam et al. 2015; Aspinall et al. 2016). Gradually, the concept of an observatory has crept toward big data analysis rather than small-scale intensive study. It was as if a small astronomical observatory on Earth (say, Griffith Park in Los Angeles) had suddenly morphed into the Hubble space telescope.
Even so, intensive study of a local community on a small scale still has many benefits. The original concept, here redefined as “community-level observatories,” is worth kee** for several reasons. Community-level observatories can:
-
Isolate and conceivably even quantify the main effects and interactions of the determinants of health by examining them on a small scale;
-
Collect historical and initial cross-sectional data that can be the basis for planning and executing longitudinal studies;
-
Serve as entry points into systematic population-based research;
-
Offer an opportunity to network with local leaders and institutions to establish working relationships for larger scale projects;
-
Study a limited area intensively and identify a set of relationships to allow examinations of relationships, attitudes, fortuitous events, resource allocation, motivation, and social and political uncertainties that cannot be captured by big data analysis;
-
Allow a combination of quantitative and qualitative studies to be undertaken, which advances theory development and explanatory power;
-
Identify novel events and trends in a community;
-
Provide an infrastructure with which to capture ephemeral or short-term developments that might otherwise be missed because of limited funding, time constraints on applications for funding, the inertia of the funding apparatus, and competing priorities; and
-
Allow the investigators to compile comparable events into a study set that can be used to compare commonalities and differences in experience, leading to more formal testable hypotheses and policy studies.
Community-level observatories are generally inexpensive to start but soon leverage themselves through elaboration, extension, supplemental contracts and grants for specific purposes, and revenue-generating activities (such as contract work for health departments). They do not depend on special characteristics of the community; they can be used to study norms of behavior in any population of interest, for example, the consumption and perception of risk-related or health information.
However, they are responsive to community events and observational, rather than interventional, community-level observatories are at a disadvantage in conducting theory-based research. On the other hand, their observations can be foundational to quasi-experimental outcome studies, support the design of structured studies, and be used to support individual hypothesis-driven studies.
The role of social observatories has been described by Soler and Castellanos 2015 in five dimensions, emphasizing documentation: purpose, targeting, topics, “problematique” (problem clusters), and methods. (In the original Spanish: finalidad, focalización, temas, problemáticas, y métodos.) In his opinion, observatories have as their primary purpose uncovering and diffusing reliable and actionable information, with the purpose to empower communities. They concentrate on particular defined topics but with the intention of putting them in a broader context, focusing on complicated issues, and making knowledge about the topic usable. The problematique describes how the constituent problems and issues interact and complicate one another, the study of which is a particular advantage of the observatory approach. Methods are appropriate to the problem, not intrinsic to the observatory, and may be quantitative, qualitative, or hybrid.
Methodology
At the time the observatory was created, the term was not in common use in the population health sciences. However, although not named as such, the observatory was designed to serve the same functions as those later postulated to be the essence of the observatory model (Hemmings 2003): autonomy (independence and separation from other functions of the academic department and the agenda of funding sources), a capacity to work on sensitive agendas, acceptance of intuitive “hunches,” small size, synthetic in their approach, heavy reliance on networks, and concern for public policy. It therefore qualifies as an “observatory” in the contemporary sense although it predated common use of the term.
Following the five-point analysis of Soler and Castellanos (2015), the observatory was designed for the purpose of capturing detailed information on and document topical local environmental issues that pertained to environmental conditions and health for the purpose of understanding them in context (the “problematique”), with an emphasis on complications that involved history, management, and policy, using the most appropriate qualitative or quantitative methods to the problem. It was not designed to generate longitudinal health data, as this would duplicate data resources of Alberta Health and be prohibitively expensive to collect on a regular basis without assured funding, but the possibility of accessing or conducting serial studies was considered for a future phase.
In practice, significant health issues came to the attention of investigators in various ways: by referral and request for expert consultation (for example, from the Edmonton Board of Health), media attention, targets of opportunity, because of their connection to other works of the academic unit in occupational or community health, or a priori interest (the environmental impact of golf course tourism). Initially there was no screening or selection procedure for issues selected but following a survey of environmental hazards in the community, this was considered for future development.
The idea of an organized capacity to examine emerging health issues on a community level separate from the mandate of the Occupational Health Program at the University of Alberta to pursue workplace health research came from two unrelated incidents (Guidotti 2012).
In the first early incident, a novel tobacco product (close cigarettes, or “kreteks”) was observed to be increasingly popular among adolescents and young adults in ways that might potentiate addiction to tobacco. This issue was “under the radar” of public health authorities but familiar to the investigator, who had encountered it before and had participated in early studies with the Centers for Disease Control. It also brought together issues of adolescent risk-taking behavior and inhalation toxicology, which had some commonality with the occupational health research agenda. A small grant was obtained to conduct local studies, successfully resulting in several publications, one of which continues to be cited today (Guidotti et al. 1989). This project featured the invaluable observations of a young research assistant who was part of the local youth community involved in the “punk” scene and who provided an insider’s view of the phenomenon. During critical funding negotiations with the Occupational Health Program’s main funding source at the time (Guidotti 2012), this relatively small project was criticized as a distraction that the investigators should not have pursued, regardless of its overall public health relevance.
The second early incident was a request from the Edmonton Board of Health to prepare a report on drinking water quality at a high level of generalization in response to a transient but publicized incident of contamination. The report was really a teaching exercise designed to inform decision-makers how water quality management worked. The report essentially repeated the content of an earlier teaching article (Guidotti 1984) but that was enough to satisfy the political requirement for a response. Again, the government agency took exception, without stating its reasons but presumably because environmental health was the domain of another department.
To the investigators, this underscored the need for a mechanism that would keep such side projects separate from the main research agenda of the program, in order to preserve autonomy and allow exploration of targets of opportunity.
Although these two experiences are not counted as projects of the observatory per se, they informed its creation. Later, in the late 1990s, the totality of the experience of the observatory proved invaluable in formulating an approach to comparative risk assessment for prioritizing emerging environmental health issues (Guidotti and Herz 2002).
Profile of the community
The community in question was called “County 20” out of deference to a local reeve (mayor equivalent) who requested that we use its administrative number and not its more familiar name in publications in order to avoid reputational injury. With the passage of time, anonymity is no longer required and the location can be identified as Strathcona County and its main population center, Sherwood Park.
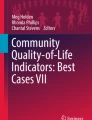
At the time of this history, which begins in 1987, the County had a population of about 56,000 dominated by a planned community of 34,000 that was its political, economic, and social center. It was settled in the 1950s primarily as residential community for workers in the petrochemical industry. The County covered a total area of 1172 km2, most of which was farmland, residential acreages (some of which were second homes), and open space. In the 1970s, it grew rapidly into a major suburb of Edmonton, Alberta, catering to relatively affluent families. In order to diversify its economic base, which was initially closely tied to jobs in Edmonton and a nearby petrochemical complex (third-largest in North America), the city and County developed an industrial park and attracted light industry to the area as well. Local housing prices, while lower than for comparable homes in Edmonton, were high relative to other nearby towns and rural areas and the housing stock was new and of high quality (Fig. 2).

A typical neighborhood in the principal community in County 20 circa 1990, as described in the text, showing the type of housing that showed a drop in sales price following the false announcement of an elevation in cancer rates (photograph courtesy of Strathcona County Museum and Archives, Sherwood Park, Alberta)
First case study
The original event that led to the establishment of the observatory was an incorrect report of an excess of cancer in a small area (roughly, a “county” containing a large residential community and a smaller industrial town) to the east of Edmonton, a major city in the province of Alberta, Canada. Residents of two nearby communities in northern Alberta, with a combined population of 52,000, became concerned about an apparently elevated rate of cancer among adults in their area. This perception came in part because a local clergyman had the impression that he was encountering a disproportionate number of cancer cases during his pastoral calls (Guidotti 1994).
In 1986, the provincial agency responsible for cancer surveillance conducted a preliminary study of cancer incidence in the area compared to the province as a whole. The findings were summarized in a draft document intended solely for internal use during the investigation. However, the report was leaked, apparently by one or more persons in a higher provincial government office. The findings were widely reported in the local, provincial, and eventually national media. Although the draft report itself was quoted correctly as written, at the time the agency was unaware that there was an error. It falsely reinforced the inaccurate findings which had been raised in meetings with the public. The premature release of the report did not allow the agency time for exploration of alternative explanations and to audit the unusual result. Many local residents and some health authorities openly speculated that there was a causal association with the concentration of refineries and petrochemical facilities in the area.
A subsequent review by an expert committee the following year and interviews with the personnel involved revealed that a mistake had been made in reading a confusing set of census tables. The cases from the industrial community had been included in the numerator but the population of the community had not been included in the denominator. It had been falsely assumed that the industrial community was part of the county in the table, but the community actually held separate political status as a township and its population was counted in another table entirely. There was no excess, only a miscalculation. Correction of this mistake brought the calculated rates into line with those for Alberta as a whole.
The findings were actually suspect from the beginning. Uniform elevations in cancer risk, regardless of tissue type, are not an expected result in a cancer cluster, in which one expects elevations in one or a small number of cancers related by cause. The absence of any deficits in cancer risk was also suspicious. Random variation would predict that even for elevations in a majority of outcomes there should be some findings that fall below expected by chance alone. The magnitude of the excess was also suspiciously large for a community elevation (on the order of 25%). The original study is now discredited.
Because the author served on a task force to determine the implications of the findings in the report, our academic unit was well aware of the error in advance of release to the media. We therefore quickly put into place a survey to determine attitudes of residents to a variety of health issues in order to determine if there was a spill-over effect from concern for cancer to other health-related behaviors. A survey of residents (100 each in the two and an adjacent comparison community) found significant (P < 0.05 or less) differences at the time in health-related behavior and beliefs suggesting increased perception of personal, family, and community risk and modest changes in personal behavior. We also requested sales information on standard two-bedroom median-priced houses from the local real estate boards. We found that real estate values in the larger community temporarily lost an average of 5% of total value (P < 0.01) compared to a similar, adjacent housing market. Shortly after the clarification, housing prices recovered completely. We concluded that perception of an elevated cancer risk may have a substantial negative effect on an affected community (Guidotti and Jacobs 1992).
We also retained a well-respected reporter for a local newspaper to study the responses of community leaders who were present and affected by the false allegation of increased cancer risk. She interviewed elected and appointed public officials in one affected community as well as non-official community leaders and realtors to determine their subjective impression regarding the effect of the incident on their communities and to rule out alternative explanations for the drop in housing prices. A few individuals suggested that real estate agents in surrounding communities had played up the reports of cancer risk in an effort to steer potential buyers away from the community and toward their listings in unaffected communities. Their collective perceptions attributed at least part of the impact to the disclosure that a high official in the community was afflicted by cancer. Most felt that there remained a great deal of latent concern in the community and at least some felt that a subsequent public issue reflected heightened sensitivity following the cancer scare (Guidotti 1994).
Our group produced three major publications and several conference abstracts from this initial work at a time when the academic program was just getting started. It grounded much of our subsequent work (Guidotti 2015).
Subsequent development of the observatory
The next issue up involved high-voltage transmission line planned for installation on a right of way cutting through the community. In this case, the observatory monitored the issue through the media and publicly available reports but refrained from conducting its own study, fortunately. The issue arose in 1988 with a proposal to expand power distribution within the area and peaked around 1992 together with issues concerning pricing of electricity (van Krieken 1984; Wilkins 1988; Pedersen 1992). (A much bigger and separate provincial issue involving high-voltage power lines carrying electricity for export was still 5 or 10 years in the future.) The local issue did not focus on health risks from electromagnetic field effects, perhaps because there were already two transmission lines in other parts of the community. The principal concern was land use and access to recreational areas used for cross-country skiing. A local consulting firm was contracted to do an analysis of impact on parcels for sale zoned for house and acreages (small landholdings usually used as a second rural residence or hobby farm) in the path of the towers. They found that not only were land values not much affected but that some buyers perceived proximity to the right of way to be a positive feature and so considered the properties undervalued and a good deal. The reason was that power transmission rights of way are meticulously maintained and guaranteed to be left open space in perpetuity (Serecon Valuation and Agricultural Consulting 2006). This makes frontage on them desirable to homeowners.
This was a sobering near-miss for the observatory. Had we done the study ourselves using the methodology that we had previously used successfully for the cancer scare, we would almost certainly have missed that important off-setting factor. Recognizing that we nearly made a mistake in interpretation of this issue confirmed our belief that to be effective in studying risk perception, an observatory cannot be passive, depending on reporting of events by others and collecting publicly available data, as we were doing at the time. We concluded that there must be active engagement with community residents who are immersed in conversation at the local level in order to interpret community response correctly.
The next large-scale activity of the observatory was to study the implications of a proposed landfill for the nearby city of Edmonton in 1990 to be built at an isolated and mostly vacant site (called “Aurum”) within city limits but across a river from the city itself and on a bluff. The site was not naturally suitable in terms of drainage (leachate in groundwater would predictably percolate and eventually reach surface water) and was therefore designed with many engineering and monitoring features. The siting was bitterly opposed by the government and residents of adjacent County 20, on grounds that the site was unsuitable on geological grounds for containment of leachate. Because our prior study of the response to these issues had given us insight into the dynamics of the community and because the opposition to the project seemed disproportionate to the likely impact, we were asked to assist County 20 in develo** their contest to planning approval. We did so and produced a report which, under the procedures at that time, was submitted by the County to the Edmonton Board of Health (Guidotti and Abercrombie 2008).
In 1990, the Edmonton Board of Health completed its evaluation and, to the surprise of almost everyone, rejected the application, making it impossible for the city to issue “planning approval.” The grounds for the rejection were both technical and procedural, in that the text of the report was found to be deficient in analysis on issues of health. The city withdrew the plan.
We decided to use Aurum as a case study of the “not in my backyard” (NIMBY) phenomenon. We funded an investigative journalist to interview 46 participants in a public hearing on the issue. She found, unexpectedly, that a major factor in the opposition to Aurum was an attitude on the part of County leaders of resentment toward the city of Edmonton for opposing the legal incorporation of the County in 1962 and also for a failed annexation attempt in 1980. Contemporary leaders in the city of Edmonton were unaware of this history and were surprised to learn that there was lingering resentment toward the city on the part of County 20 residents and leaders (Guidotti and Abercrombie 2008). We concluded that in this instance, and probably many others, the political history of the community played a major role in conditioning the response to “locally undesirable land use” (LULUs) and the NIMBY phenomenon (Guidotti 2015).
Not long afterward, another NIMBY landfill issue emerged in a central, rural area of the province under different circumstances. In this case, the local authority proceeded with a reasonable plan to build an engineered sanitary landfill to replace an unsecured landfill that was reaching capacity. However, costs escalated dramatically and construction defects compromised the integrity of the new facility. The end result was a bad outcome for a project that should have been an environmental improvement and a sobering validation of community concerns that initially seemed overstated. Ironically, the community (called by the pseudonym “Ghostpine”) was devastated a few years later by a tornado. This incident provided a valuable teaching example of the importance of humility in environmental planning (Guidotti 2015).
On the strength of the observatory activities and particularly Aurum, we developed an on-going relationship with the County’s leaders. In 1992, we were invited to conduct a review “to assist [County 20] in assessing the degree of risk to residents presented by the industrial, transportation, and agricultural environment, in such a way as to facilitate development of a strategic plan for minimization of risk within the constraints of economic development and personal choice.” This was intended to be in equal parts an audit function and a hazard assessment. During the course of this review, an unrelated survey by the respected firm Decima Research (Vancouver) was conducted on County residents and found that most residents considered the County to be a safe place to live but had concerns over traffic, air pollution, and increased traffic (Decima Research 1992).
The data that were available to our group were limited but of high quality and showed clearly that the County itself was not an area of high risk and compared very favorably to other local jurisdictions in health indicators. Reportable disease and mortality rates were comparable or lower than elsewhere in the province. No hazard appeared to be exceptional, unusual, or particularly severe compared to other similar jurisdictions. Traffic safety emerged as by far the most conspicuous environmental risk to life in terms of serious injury, not surprisingly. “Environmental” complaints to bylaw enforcement officers almost always involved nuisances instead of significant health hazards. (Bylaws are local ordinances, enforceable only in that community and subsidiary to provincial law.) Available data sources at the time, in the early 1990s, simply could not provide a detailed picture of risk at the local level (Guidotti et al. 1997).
Among the stakeholders with whom we communicated on the project was an advisory committee designated by the medical officer of health to receive the findings and make recommendations. There was a preponderance of engineers on the advisory committee, with no other health professionals. We reported our findings and proposed that the County follow up with a workshop on risk comparison to determine residents’ priorities in managing risk going forward and to design a County-level inventory to monitor trends (Guidotti 1994).
The reception of the study report was sharp and disappointing. The public and local decision leaders were satisfied but the advisory committee was not pleased. We had contracted to conduct a review of available public health data but the unexpressed and unrealistic expectation of the advisory committee was that new data would be forthcoming and that we would provide the County with a detailed map of environmental risk for County residents. It soon became apparent that the engineering community represented on the committee had assumed that abundant data was readily available but public health practitioners knew that it was not. (The days of large, on-line databases covering small jurisdictions lay in the future but the engineering-oriented advisory committee thought it had already arrived.) In 1992, there were simply no existing databases on which to base a fine-grained analysis of issues such as well-water quality, emissions from local refineries, or local release of toxic substances (although there was abundant information on transportation). By far the most detailed data available were on vehicular traffic and injury. In retrospect, it should have been a red flag that the offer was grossly underfunded. We had been offered Can$10,000 ($16,000 in 2020 dollars, without overhead) which we had accepted in the interests of develo** the observatory and gaining access to the data bases, which in the event turned out to be of little value.
Interestingly, however, the findings and conclusions of our much smaller study converged almost exactly with a similar study conducted by a team at The Johns Hopkins School of Hygiene and Public Health (1992) at about the same time, using the same methods, for Anne Arundel County in the State of Maryland.
The review of health department data did position our group to participate in another review of environmental health services in the province, conducted in 1993 by a team of epidemiologists in our department (Guidotti and Hrudey 1996; Saunders et al. 1996). We entered this project as skeptics and emerged with a more nuanced sense that although environmental health services probably did not require a complete reinvention, management toward measurable objectives was a worthy goal; indeed, this has now become mainstream thinking. While this was not a project of the observatory itself, our earlier work in County 20, including the disappointing risk identification project, prepared us through experience to contribute to the work.
In 1993, the observatory’s activities were folded into a new entity with a broader agenda. The Northern Alberta Centre for Work, Safety and Health was funded mostly by Alberta Labour as a vehicle to conduct a much larger study in northern Alberta on social marketing in the prevention of injury but it also had a mandate to conduct community outreach. Subsequently, the observatory no longer had an independent existence.
Dead ends
Not all of the planned initiatives of the observatory bore fruit.
In the early 1990s, the provinces of Alberta and British Columbia saw an opportunity for economic diversification in the development of recreational facilities as tourist destinations. There was a worldwide surge of interest in golf, particularly in countries that traditionally favored Alberta for recreational travel, such as Japan. In Japan, golf course development had significantly slowed because of public concern over environmental impact and public controversy over the appropriateness of committing large tracts of land to this land use in a densely populated country (Efron 1992). There was considerable commercial interest in making Alberta a golfing destination for Japanese enthusiasts on packaged vacations. We joined a proposal in 1992 to track potential environmental and health implications of the intensive turf management required, including the application of chemicals or bioaccumulation in animal and plant species and to compare outcomes with integrated pest management as a preferred approach. One aspect of the work was monitoring the response of community residents. The approach was necessarily qualitative because the populations were too small and too interconnected for quantitative results to be independently analyzed. Despite an initially favorable reception by the funding agencies involved, the final proposal was not accepted, because the site ultimately chosen by the province for the demonstration project was too far away from Edmonton.
Another unsuccessful initiative was a proposal to use an extensive database of death certificates, compiled to support a prospective occupational mortality study, to test the hypothesis that the relationship between underlying conditions and immediate cause of death was changing over time. The thinking was that this might illuminate determinants of health, some of which would reflect environmental factors. The proposal more closely approximated a traditional epidemiological study but was intended to probe community-level health risks. The proposal was never funded.
Discussion
The observatory did succeed in collecting fine-grained qualitative and small-group level quantitative information. The observatory concept worked best when it was narrowly focused and applied to risk perception studies. It did least well when it attempted to scale up activities and work outside its geographic area of focus.
The experienced and trusted journalist was an indispensable resource. Although we were initially concerned about objectivity, given her following in the community, she remained appropriately skeptical of claims of risk throughout and was a reliable observer of events in the County. Her access to people and local information sources was invaluable.
Specific lessons learned from the experience of the observatory included the following:
-
There must be active engagement with community residents who are immersed in conversation at the local level in order to interpret community impact and trends with confidence; even if initial interpretation is correct scientifically, one cannot be sure of its validity as a social construct until it is tested against perceptions.
-
The history of a community shapes perceptions of the present in the minds of those most concerned with the past and is often not shared; it can surprise those who come to an issue unawares.
-
Observatories need to be wary of assuming administrative functions that would otherwise be within their mission, such as audits or status reviews, as these can complicate relationships.
-
The perceptions of different professional communities may be quite biased to their expectations, for example, of the availability of data.
-
Gaining experience from observing various incidents and situations provides valuable experience in itself, apart from data capture and analysis.
-
Underfunded projects can be very destructive to a research unit because of their reputational risk.
-
The observatory model is a strategy to convert episodic research opportunities into clusters of observed events that can support hypothesis generation and policy studies.
The observatory was always funded on a shoestring and was never the sole or even the most important research activity of the academic unit or department. During the early 1990s, at least, individual projects were sufficient to fund the low level of on-going activity required to monitor trends in the community. Our subsequent experience with a much larger community-based study confirmed that this cost structure is not scalable and that at a certain point professional staffing resident in the community becomes essential. Today the cost of data gathering, aggregation, and analysis would be much less due to the internet and off-the-shelf analytics. Had the observatory not been functionally absorbed into the already-funded community outreach program, a formalized longitudinal study would undoubtedly have been proposed eventually, although with no assurance of success in attracting stable funding.
Conclusions
In retrospect, the observatory worked well to prepare the academic group for what was to come in terms of research opportunities in the local area. It also provided a useful community laboratory for observing and thinking about environmental health issues and risk in the community. The observatory was a viable starting point for community-based research in environmental health and had the great advantage of grounding data monitoring in qualitative observation.
The transition between the observatory model and a properly funded community outreach study highlighted the limitations of the local observatory but also the value of deep qualitative study of key events and issues. The observatory prepared investigators and trained staff to look more deeply at complicated social phenomena with respect to health and made the transition to a systematic approach easier.
The local observatory model is a practical, low-cost, and sustainable model for capturing generalizable and specifically local case study experience on a small scale but is limited in its effectiveness and by the scope of its coverage. It can be an initial step toward longitudinal and community monitoring studies on a larger scale.
It is often said that “the plural of anecdote is not data” but it is equally true that the multiplicity of thoughtful observation is experience.
References
Adam T, Røttingen JA, Kieny MP (2015) Informing the establishment of the WHO Global Observatory on Health Research and Development: a call for papers. Health Res Policy Syst 2015(13):9
Aspinall PJ, Jacobson B, Castillo-Salgado C (2016) Establishing and sustaining health observatories serving urbanized populations around the world: sco** study and survey. Euro J Public Health 26(4):681–686
Decima Research (1992). Report to the County of Strathcona on attitudes towards industrial development and health and safety issues. Vancouver BC, 5 October 1992.
Efron S (1992). Environment: critics take swing at Japan’s golf courses: they are scarring the land, fouling the water and encouraging corruption, critics claim. Los Angeles Times 7 July 1992. Available at: https://www.latimes.com/archives/la-xpm-1992-07-07-wr-1641-story.html
European Union. Social observatory for disinformation and social media analysis. Available at: https://www.disinfobservatory.org/. Accessed 20 January 2021.
European University Institute (2021). Academic careers observatory. Available at: https://www.eui.eu/ProgrammesAndFellowships/AcademicCareersObservatory. Accessed 20 January 2021.
Guidotti TL (1991) The cancer non-epidemic of County 20: case study of an epidemiologic mistake. Pub Health Rev 19:179–190
Guidotti TL (1994) Comparing environmental risks: a consultative approach to setting priorities at the community level. Pub Health Rev 22:321–337
Guidotti TL (2012) Beginnings: the Occupational Health Program at the University of Alberta, 1984–1999. Can Bull Med Hist 29(2):283–307
Guidotti TL (2015) Health and sustainability. Oxford University Press, New York
Guidotti TL, Abercrombie S (1994) Voices of leadership in a community under stress: personal observations by officials on an epidemiological mistake. J Pub Health Med 16:381–388
Guidotti TL, Abercrombie S (2008) Aurum: a case study in the politics of NIMBY. Waste Manag Res 26(6):582–588
Guidotti TL (1984) Conway JB (1984). Water Health Am Fam Physician 30(4):97–104
Guidotti TL, Ford L, Wheeler M (2000) The Fort McMurray Demonstration Project in Social Marketing: theory, design and evaluation. Am J Prev Med 18(2):163–169
Guidotti TL, Herz WC (2002) A process to reconcile priorities among agencies responsible for environmental health risks. Int J Risk Assessment Management 19(2/3/4):170–188
Guidotti TL, Jacobs P (1992) Implications of an epidemiologic mistake: a communities response to a perceived excess cancer risk. Am J Publ Health 83:233–239
Guidotti TL, Jhangri GS, Ford L (1997) Comparing environmental risks in a county in Alberta. Environ Health Rev (j Can Instit Publ Health Inspectors) 41:84–90
Guidotti TL, Hrudey SE (1996). Measurable objectives for local environmental health programs. Saunders DL, Wanke MI. J Envir Health 58(6):6–11.
Guidotti TL, Laing L, Prakash UBS (1989) Clove cigarettes: the basis for concern regarding health effects. West J Med 151:220–228
Hackenberg RA (1967) The social observatory: time series data for health and behavioral research. Soc Sci Med 1970(3):343–357
Hemmings J, Wilkinson JR (2003) What is a public health observatory? J Epidemiol Comm Health 57(5):324–326
Hofferth S, Hubacek K (2021). Social observation coordinating network. Available at: https://www.popcenter.umd.edu/research/selected_research/research_1371480705699. Accessed 20 January 2021.
Indiana University (2020). Observatory on social media. Available at: (https://venturebeat.com/2020/12/21/studies-show-bots-might-not-be-the-dominant-driver-of-covid-19-misinformation-on-social-media/. Accessed 20 January 2021.
[The] Johns Hopkins University Health Program Alliance. The public health needs and resources of Anne Arundel County. Section L. Environmental Health Profile. Baltimore, Johns Hopkins School Hyg Publ Health, 1 June 1992, pp. L-1 - L-19 and Appendix.
Lalonde M (1974). A new perspective on the health of Canadians. A working document. Ottawa, Government of Canada.
Marmot M (2005) The social environment and health. Clin Med 5(3):244–248
Pedersen R. It’s our turn to gain, Edmonton Power says. Edmonton Journal, 3 June 1992.
Saunders LD, Wanke MI, Pelton JM, Hrudey SH, Guidotti TL (1996) Redesigning local environmental health programs. J Envir Health 58(9):6–11
Serecon Valuation and Agricultural Consulting (2006). The impact of power transmission lines on rural residential property values. Edmonton, Alberta, Duncan & Craig, August 2006. Available at: https://open.alberta.ca/dataset/41e14d83-e58e-4e89-8a05-e8ba44240635/resource/00c1cd00-7a0a-4fa1-9da7-2f429f04365f/download/appendix-e-studies-of-impacts-on-land-value.pdf
Soler GEM, Castellanos JFMC (2015) A review of the social observatory concept: towards an understanding of its objectives, scope, methods, and purposes. Psicogente (revistas Científicas Universidad Simón Bolivar) 19(36):347–359 (In Spanish)
United Nations Economic and Social Council (2011). Concept Paper: UNESCO’s Global Observatory on Science, Technology and Innovation Policy Instruments GO SPIN. Paris, October 2011. Available at: http://www.unesco.org/new/fileadmin/MULTIMEDIA/HQ/SC/pdf/GO-SPIN_Concept.pdf
University of Bristol (2020). Economics observatory awarded funding boost to address pressing economic questions prompted by the COVID-19 pandemic. Available at: https://www.bristol.ac.uk/news/2020/december/economics-observatory.html. Accessed 20 January 2021.
Van Krieken C (1984). Strathcona council to oppose power lines on recreational land. Edmonton Journal, 12 December 1984, p. 12.
Wilkins B (1988). Power line rouses opposition. Edmonton Journal, 13 - 19 November 1988, p. 48.
World Bank (2016). The social observatory: a living lab for develo** a science of delivery. 28 January 2016. Available at: https://www.worldbank.org/en/news/feature/2016/01/28/the-social-observatory-a-living-lab-for-develo**-a-science-of-delivery. Accessed 20 January 2021.
Acknowledgements
Many professionals participated in the observatory, most without knowing it because it was unnamed at the time, consisting of a string of related projects managed by the Occupational Health Program until the Northern Alberta Centre for Work, Environment and Health was created. Lynda Ford, who became Managing Director of the Northern Alberta Centre for Work, Environment and Health, supported and participated in the work of the observatory throughout. The core team that investigated community reaction to the cancer excess included Merva Cottle, Phil Jacobs, and Sheila Abercrombie. Gian Jhangri provided biostatistical support. Ken Yoshida provided support in occupational hygiene and exposure assessment. Veronica Clough served as research assistant during this period. Casey van Teeling took the lead on the project involving golf courses. Steve Hrudey, Duncan Saunders, and Margaret Wanke led the work on objectives for environmental health, in which the observatory team took a supportive role. Lisa Zacharkiw assisted with the kretek study, which foreshadowed the methods of the observatory.
Funding
Much of the early work of the observatory was conducted without dedicated funding. The initial study on cancer rates was conducted by the Alberta Cancer Board but the advisory committee was not funded. The Aurum project and the review of environmental health risks were funded by contracts with the jurisdiction identified here as County 20. The Northern Alberta Centre for Work, Environment and Health, which took over the work in about 1993, was funded in part by an operating grant from what was then Alberta Labour, Occupational Health. The primary mission of the Northern Alberta Centre for Work, Environment and Health was to serve as a resource for occupational and community health in response to local needs and to conduct a 5-year project in social marketing for safety promotion, the Fort McMurray Demonstration Program in Social Marketing (Guidotti et al. 2000). This project has been extensively described elsewhere and was undertaken separately from the observatory function and other activities of the Occupational Health Program as a condition of funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Names of places and agencies are given as they were in 1992, and may have changed since.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Guidotti, T.L. The observatory: a model for studies in health, society, and the environment. J Environ Stud Sci 12, 827–837 (2022). https://doi.org/10.1007/s13412-022-00786-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13412-022-00786-6