
Abstract
MOGHE is defined as mild malformation of cortical development with oligodendroglial hyperplasia in epilepsy. Approximately half of the patients with histopathologically confirmed MOGHE carry a brain somatic variant in the SLC35A2 gene encoding a UDP-galactose transporter. Previous research showed that D-galactose supplementation results in clinical improvement in patients with a congenital disorder of glycosylation due to germline variants in SLC35A2. We aimed to evaluate the effects of D-galactose supplementation in patients with histopathologically confirmed MOGHE, with uncontrolled seizures or cognitive impairment and epileptiform activity at the EEG after epilepsy surgery (NCT04833322). Patients were orally supplemented with D-galactose for 6 months in doses up to 1.5 g/kg/day and monitored for seizure frequency including 24-h video-EEG recording, cognition and behavioral scores, i.e., WISC, BRIEF-2, SNAP-IV, and SCQ, and quality of life measures, before and 6 months after treatment. Global response was defined by > 50% improvement of seizure frequency and/or cognition and behavior (clinical global impression of “much improved” or better). Twelve patients (aged 5–28 years) were included from three different centers. Neurosurgical tissue samples were available in all patients and revealed a brain somatic variant in SLC35A2 in six patients (non-present in the blood). After 6 months of supplementation, D-galactose was well tolerated with just two patients presenting abdominal discomfort, solved after dose spacing or reduction. There was a 50% reduction or higher of seizure frequency in 3/6 patients, with an improvement at EEG in 2/5 patients. One patient became seizure-free. An improvement of cognitive/behavioral features encompassing impulsivity (mean SNAP-IV − 3.19 [− 0.84; − 5.6]), social communication (mean SCQ − 2.08 [− 0.63; − 4.90]), and executive function (BRIEF-2 inhibit − 5.2 [− 1.23; − 9.2]) was observed. Global responder rate was 9/12 (6/6 in SLC35A2-positive). Our results suggest that supplementation with D-galactose in patients with MOGHE is safe and well tolerated and, although the efficacy data warrant larger studies, it might build a rationale for precision medicine after epilepsy surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Malformation of cortical development (MCD) is the most frequent disease condition histopathologically observed in surgical specimens of children undergoing surgery for refractory focal epilepsy [1,2,3,4]. Recently, a new type of MCD, mild malformation of cortical development with oligodendroglial hyperplasia in epilepsy (MOGHE), was described in children and adults with refractory epilepsy, characterized by an increase in oligodendroglial cells and in addition to heterotopic neurons located in the white matter, among other features [5].
Since somatic variants of the mechanistic target of rapamycin (mTOR) were associated with focal cortical dysplasia (FCD) type 2, somatic mosaicism has been elucidated as a common cause of MCD [6,7,8]. Deep sequencing of brain specimens from patients with MOGHE has revealed a pathogenic variant in the SCL35A2 gene in approximately 45% of the patients [8,9,10,11,12]. The SLC35A2 gene encodes for the UDP-galactose transporter which is essential in protein and sphingolipid glycosylation taking place in the major Golgi apparatus and in the endoplasmic reticulum. Germline variants in SLC35A2 cause an X-linked congenital disorder of glycosylation (SLC35A2-CDG), a syndrome characterized by multiorgan involvement, including a neurodevelopmental disorder with seizures [13, 14].
A better understanding of the molecular mechanisms in developmental and epileptic encephalopathies (DEEs) has fostered the repurposing of existing drugs that target specific cellular pathways [15]. This paradigm of precision medicine has been recently applied to mTORopathy-related epilepsies. For example, in tuberous sclerosis complex (TSC), caused by dysregulation of the mTOR pathway, rapamycin and other mTOR inhibitors demonstrated a reduction greater than 50% of seizure frequency compared with 15% treated with placebo [16]. As a result, rapamycin has been approved as a repurposed drug for the treatment of focal refractory seizures in patients with TSC [17], suggesting also preliminary effectiveness in preclinical studies of other mTORopathies caused by brain mosaicism [18,19,20,21,22,23,24,25,26].
In the context of UDP-galactose transporter–related pathology, a small trial with oral supplementation of D-galactose demonstrated clinical and developmental improvements in patients with germline variants in SLC35A2 (SLC35A2-CDG). Half of the patients (2/4) achieved seizure freedom upon D-galactose supplementation [27]. Improvement in glycosylation [28] and clinical features such as alertness and interactivity [29] has also been observed in SLC35A2-CDG patients treated with D-galactose.
Resective surgery constitutes the first-choice treatment for drug-resistant focal epilepsy due to FCD and other MCDs. The overall rate of favorable epilepsy outcome ranges between 64 and 70% at 12 months after surgery [3, 30, 31]. However, a significant proportion of MCD patients are not rendered seizure-free after surgery. Factors that may influence the effectiveness of resective surgery include the presence of multilobar pathology and difficulty in identifying and delineating lesions in neuroimaging [32], as well as incomplete resection due to the involvement of eloquent areas. Additionally, developmental and cognitive problems are not always solved after surgical treatment, with cognitive function being reported as unchanged or worsened after surgery in up to 91% of patients [3]. Moreover, although surgery may improve cognitive outcomes in some patients, especially in those who presented a shorter duration of epilepsy and achieved seizure-free status access to epilepsy, surgery is typically delayed in most series [33, 34]. D-galactose is an easily accessible and well-tolerated treatment that allows the entry of galactose to the Golgi apparatus and endoplasmatic reticulum, thus improving the glycosylation process in UDP-galactose transporter–deficient cells. We hypothesized that treatment with D-galactose in histopathologically confirmed MOGHE patients may achieve improvements in epilepsy and neurodevelopmental outcomes. In this study, we present the data from the first trial employing D-galactose supplementation in MOGHE patients, and the obtained results may indicate that D-galactose supplementation could be used as an effective disease-modifying treatment specially tailored to MOGHE patients.
Methods
Patient Recruitment
This is a prospective multicenter single-arm study involving three European epilepsy centers: Hospital Ruber Internacional, HRI (Madrid, Spain); Kepler Universitätsklinikum, KU (Linz, Austria); and Schön Klinik Vogtareuth, SKV (Vogtareuth, Germany). Patients must meet the three inclusion criteria: (1) age between 2 and 30 years at the start of the study, (2) histopathological diagnosis of MOGHE diagnosis of the resected brain tissue, and (3) refractory epilepsy or cognitive impairment with ongoing epileptiform activity at the beginning of the study. Exclusion criteria were the presence of allergy to D-galactose, or other supplement components, and/or the presence of a germline variant in SLC35A2.
Intervention
Oral D-galactose was administered at a dose of up to 1.5 g/kg daily for 18 weeks. A progressive titration similar to the already published protocol for SLC35A2-CDG patients was followed to minimize gastrointestinal side effects: (a) weeks 0–6: 0.5 g/kg daily, (b) weeks 7–12: 1 g/kg daily, and (c) in weeks 13–18: 1.5 g/kg daily, following the already published schedule for SLC35A2-CDG patients [27]. Concomitant ASMs were not allowed to change during the first 6 months after initiation of D-galactose treatment. D-galactose was started at a minimum of 6 months after the epilepsy surgery and MOGHE histopathological diagnosis.
Study Protocol
For each patient, investigators were asked to provide pseudo-anonymized information on the following items: (a) general clinical and demographic characteristics: sex, age, early development, neurological examination, age at first seizure, presence of autism spectrum or attention-deficit/hyperactivity disorder (ADHD); (b) seizure characteristics: type of seizures at onset, type of seizures at any time, presence of status epilepticus at any time, and epilepsy syndrome; (c) description of baseline electroencephalographic information; (d) MRI pattern, according to the Hartlieb et al. classification of MOGHE [2]; and (e) treatment information: ASM received at any time, current ASM, age at surgery, type of resection, behavioral, cognitive, and epilepsy outcome of surgery according to the Engel classification [35].
At the start of the study and after the treatment, the following variables were recorded:
-
Seizure outcome: monthly frequency at baseline, and at 1, 3, and 6 months after the start of the treatment. Monthly seizure frequency was estimated as the number of seizures in the previous month divided by 30. Subjective changes in seizure duration and intensity reported by the patient and clinical global impression (CGI [36]) scale for epilepsy were also noted at 6 months.
-
EEG outcome (epileptiform activity): in the HRI cohort, a 24-h video-electroencephalographic recording was obtained before and after 6 months of treatment. For each patient, quantification of the epileptic activity per epoch was done, as well as the presence of bilateral synchrony and propagation of the activity.
-
Cognitive and behavioral assessment: for each patient, CGI of cognition and behavior at 6 months was registered. In the HRI cohort of patients, at baseline and after 6 months of treatment, a comprehensive neuropsychological battery was administered, which included the Wechsler Intelligence Scale for Children (WISC-IV [37], in patients from 6–17 years), the Wechsler Adult Intelligence Score (WAIS-IV, in patients older than 16 years), the Swanson, Behavior Rating Inventory Of Executive Function (BRIEF-2 [38], administered to the family and teachers), Conners’ Continuous Performance Test (CPT-II [39]), the Nolan and Pelham Teacher and Parent Rating Scale (SNAP-IV [40, 41], administered by caregivers and teachers), and Lifetime and Current Social Communication Questionnaire (L-SCQ and C-SCQ [42], administered by the caregivers). All ratings are expressed as percentiles, relative to a normative population, with increasing scoring in WISC and WAIS demonstrating an improvement and in BRIEF-2, CPT-II, SNAP-IV, and SCQ lower scores pointing to amelioration. BRIEF-2 indexes include the behavior regulation index (BRI), which refers to the ability to regulate and monitor behavior and impulses; the emotion regulation index (ERI) which refers to the ability to regulate emotional responses; cognitive regulation index (CRI) which references to the ability to regulate thinking and attention; and global executive composite (GEC), which is an overall summary score. To determine if changes in BRIEF were clinically meaningful, we relied on the reliable change index (RCI) for BRI, ERI, CRI, and GEC, using a 95% value for RCI, with thresholds at 9 for BRI and ERI and 8 for CRI and GEC. In this case, the differences were calculated for the evaluations of the family before and after treatment [38].
-
Quality of life: in the HRI cohort, questionnaires measuring the quality of life (Encuesta para la Calidad de Vida de niños con Epilepsia: CAVE [43] and Pediatric Quality of Life Inventory: PedsQL [44]) at baseline and 6 months were provided to the caregivers and patients.
Discontinuation and adverse events were registered at any time of the study, including the time when the adverse event was noted.
Outcomes
-
Seizure responder rate: proportion of patients with 50% or greater reduction in the seizure frequency at 6 months compared to baseline, in patients who had non-controlled seizures at the start of the trial
-
Global responder rate: proportion of patients with a significant reduction in seizure frequency (50% or higher compared to baseline) activity and/or CGI for behavior or cognition of 2 (“much improved”) or better
-
Changes in CGI for epilepsy, cognition, and behavior
-
Significant reduction in epileptiform activity: this is defined as a reduction of more than 50% of epileptiform activity or a decrease in the presence of bilateral synchrony or propagation when a 50% reduction was not achieved. The disappearance of polyspike or fast activity in the follow-up 24-h video-EEG was also a measure of EEG improvement.
-
Changes in neuropsychological and behavioral scales
Histopathological Diagnosis
Assessment of the histopathological specimens was performed by an expert neuropathologist (IB/RC). Digitally scanned slides were made accessible for microscopic evaluation providing hematoxylin and eosin staining of all tissue blocks, cresyl violet-luxol fast blue (CV-LFB) stainings, and/or immunohistochemistry for NeuN, MAP2, Olig2, and KI-67 in selected cases. The diagnosis of MOGHE was given if clusters of oligodendroglial cells were recognized at a density of more than 2000/mm2 at the grey-white matter junction and an excess of heterotopic neurons in the white matter > 20/mm2.
Detection of Somatic Variants
DNA was extracted from FFPE tissue and was subjected to targeted sequencing with a gene panel. The panel contains 21 genes associated with FCD/MCD and MOGHE. NGS libraries were prepared by use of Twist Bioscience custom panel (Twist Bioscience) and paired-end sequenced on an Illumina platform (NovaSeq 6000, Illumina, San Diego, California, USA) (read depth range 251–30, × 150 mean read depth). Reads were demultiplexed and aligned to GRCh37/hg19 human reference genome with BWA-MEM, and variants were called with the use of FreeBayes. Variants were filtered and analyzed by use of Golden Helix VarSeq 2.2.3 (Golden Helix Inc., Bozeman, Montana, USA). The Varseq filter parameters were as follows: (1) phred quality score (QUAL) > 10; (2) variant allele frequency (VAF) > 0.02; (3) with the sample read depth (DP) set to ≥ 10; and (4) finally, variants should not have been observed more than once in homozygous or hemizygous state; hence, the GnomAD Homo/Hemi filter was set to AC < 1.
All low-frequency variants were evaluated according to the ACMG guidelines (Richards et al., 2015, Genet Med 17(5):405–24). Included in this evaluation were database searches like Human Gene Mutation Database (HGMD), the Genome Aggregation Database (gnomAD, release 2.1.1), ClinVar, and dbSNP(155). Predictions on protein level were obtained from the dbNSFP functional predictions and Cores 3.0 database. All patients had a normal previous germline genetic testing (a gene panel or exome sequencing performed in blood or saliva samples).
Protocol Approvals and Patient Consents
Written informed consent for participation/publication in this study was obtained from all parents or legal guardians. Protocol and design of the study were reviewed by the ethics committee of HRI. The protocol was approved and published in clinicaltrials.gov: NCT04833322.
Statistical Analysis
Statistical analysis and graphical representation were performed in R Core Team [45] and RStudio [46]. Qualitative measures were expressed in fractions and percentages, whereas quantitative measures are shown as median and range, except for SNAP-IV, where the interquartile range is shown. Associations between two qualitative measures are studied with the chi-square test or the Fisher test when appropriate. Analysis of the change of the quantitative tests over time was performed with the generalized linear mixed models, adjusting by ID and evaluator as random effects when necessary and using time as a fixed effect. No interactions nor subgroup analyses were performed due to the low number of observations. Statistical associations are expressed in mean changes of the measure, 95% confidence interval, and p-value.
Results
Twelve patients (3 females, 5–16 years; 9 males, 9–28 years) were enrolled in the study. In 6/12 patients, a SLC35A2 brain-specific mosaic variant was detected (Table 1). Two of the variants were nonsense, one of them was an inframe deletion of one amino acid and two of them were missense variants, and the last variant was a non-coding variant in the 3′ UTR. The two nonsense variants appeared relatively early in the transcript and are therefore likely to lead to nonsense-mediated decay. The inframe deletion of one amino acid was previously seen in a patient with early-onset epilepsy and a congenital disorder of glycosylation [8, 20, 22]. Likewise, the p.(Gly282 = /Arg) amino acid substitution was observed in a patient with a congenital disorder of glycosylation [41]. The two remaining variants, the missense and the non-coding 3′-UTR variants, are not previously observed. Clinical and radiological baseline features of the patients are shown in Table 2. Median time from the first seizure and from resective surgery to the start of the trial was 141 months (range 55–186) and 30 months (range 6–120), respectively. Of note, 6 patients had ongoing seizures, and 6 were seizure-free before the start of the study but showed cognitive impairment and epileptiform activity at the baseline video-EEG monitoring.
Drug Administration
All patients received D-galactose, at a median dose of 1.15 g/kg per day (range 1.3–0.5 g/kg day) and a median total daily dose of 50 g (range 40–66 g). In 7/12 patients, galactose was administered once a day (four in the morning, three in the afternoon), in two patients twice daily, in one patient three times daily, and in two patients four times daily. Patients reached the maximum dose at a median of 12 weeks (range 4–16 weeks) and were followed at a median of 12 months (range 7–16 months).
Safety
None of the patients reported dietary changes related to the administration of the drug, but in 2/12, adverse events related to the administration appeared. In case #3, nausea was reported, which was resolved when medication intake was separated into different doses over the course of the day. In the other case (#12), skin rash, gastrointestinal discomfort, and diarrhea appeared at the daily dose of 66 g (1.32 g/kg) and improved after symptomatic treatment and a reduction to daily 45 g (0.9 g/kg). In regard to patient #6, adherence to treatment could not be guaranteed due to the refusal of the patient, and she discontinued the treatment because of lack of efficacy at 12 months.
Seizure Outcomes
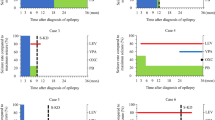
In 4/6 patients with seizures, a 50% seizure reduction was achieved at 1 month after the target dose, while no change was noted in 2/6. No increase in the seizure frequency was reported in the cohort. The 50% reduction was maintained at 6 months in all but one patient (3/6), who came back to her baseline seizure frequency after the initial response (seizure responder rate of 50%). Also, an improvement in seizure intensity and duration was noted in all the patients with reduced seizure frequency (3/3) at 6 months. One of the patients (patient #8) became seizure-free after the treatment (Fig. 1).

Relative seizure frequency after treatment in patients who had seizures before the start of the study
Continuous 24-h video-EEG was available before and after 6 months of treatment in 5/12 patients. In 2/5, there was a significant reduction in the epileptiform activity, while in 3/5, no change was noted in the EEG. Seizure reduction was associated with a decrease in epileptiform activity in 2/3 of patients.
Cognitive, Behavioral, and Quality of Life Outcomes
After treatment, CGI for cognition was reported as “much improvement” in 8/10 patients, while in 2 of them, this change was “minimal” or “none.” Regarding behavior after treatment, no change was reported in 6/11 patients, and just 5/11 noted a “minimal improvement” (considered as non-significant).
Average scoring in WISC, SNAP-IV, PEDS-QL, BRIEF-2 global executive composite, CPT-II, and SCQ for all the patients before and after treatment is shown in Table 3 and supplementary table 1. Individual changes in BRIEF-2 scores can be found in the supplementary material (Fig. 2).

Flowchart diagram of the outcomes. Main outcome measures are shown in the chart, and details about neuropsychological and EEG outcomes can be found in the main text. Epi refractory epileptic cohort, cog cognitively impaired with epileptic activity (seizure-free) cohort, SL
Global Responder Rate
Nine (9/12) patients showed a global response (either in seizure or cognitive/behavioral outcomes, Fig. 3). Notably, in 6/9 responder cases, a pathogenic variant in SLC35A2 was found; thus, the global responder rate was 6/6 in SLC35A2-positive cases, while it was 3/6 in the SLC35A2-negative group.

Changes in the EEG epileptiform activity in patient #8: A before D-galactose, with almost continuous focal activity over the right central-parietal area; B after 6 months of supplementation with D-galactose, with EEG almost normalized
Case Study
Patient #8 was a 29-year-old male, with normal neurodevelopment and university education, who had onset of drug-resistant focal epilepsy at the age of 15 years, despite treatment with more than 10 ASMs, including a clinical trial with padsevonil. Seizures were frequent (8–10 per month) and classified as focal impaired awareness, with postictal dysphasia. Video EEG and magnetoencephalography demonstrated epileptiform activity in the left central and parietal regions, and MRI showed a mild abnormality of the gyral architecture in the left parietal operculum and the posterior temporal region. A stereo EEG was performed over that region, including radiofrequency thermocoagulation obtaining a temporary improvement in seizure frequency and intensity. Due to the proximity to eloquent areas, a new intracranial EEG with a subdural grid was performed, with language map**. After that, a partial parietal resection, without resecting some of the areas related to the seizure-onset zone due to language involvement, was made at the age of 28 years. This confirmed the histopathological diagnosis of MOGHE in the resected tissue. Gene panel testing on saliva was negative; however, targeted sequencing of the resected brain tissue revealed a pathogenic variant [c.322C > T; p.(Gln108*)] in SLC35A2, with a variant allele frequency of 17%. The clinical picture of the patient was compatible with the drug-resistant focal epilepsy MOGHE phenotype, according to Barba et al. [3]. Six months after the surgery, the patient still had 4 seizures/month despite treatment with lamotrigine, lacosamide, clobazam, and oxcarbazepine. The patient was enrolled in this trial and was being assigned to a target daily dose of 50 g D-galactose (0.5 g/kg/day). In the first month after the treatment, the patient became seizure-free, with a video EEG showing a 90% reduction in the epileptiform activity (Fig. 3). The seizure freedom was maintained until the last follow-up (12 months after treatment initiation).
Discussion
In the present study, we demonstrated the feasibility, safety, and tolerability of D-galactose supplementation in a cohort of 12 patients with MOGHE, as well as preliminary evidence of the efficacy of the treatment. In our cohort, we found a maintained 50% or higher seizure reduction in half of the patients. Global responder rate, defined as the proportion of patients with significant response in either seizure or cognitive/behavioral outcomes, was 9 out of 12.
Overall, the treatment was safe and well tolerated, but 2/12 patients experienced mild gastrointestinal discomfort, which was solved after dose adjustment and spacing. One patient discontinued the treatment before the 6-month follow-up because of a lack of efficacy and difficulties in adherence. Despite that our cohort is small, interestingly, the responder proportion was higher in SLC35A2-positive patients (6/6) compared to those without an SLC35A2 variant (3/6). Of note, half of the patients were seizure-controlled at the beginning of the trial, showing that D-galactose might be effective for cognitive/behavioral outcomes even in patients who remain seizure-free after epilepsy surgery.
Although the samples in both studies are small, our findings are in line with the results of D-galactose supplementation in SLC35A2-CDG, where there was seizure improvement (2/4), and significant improvement in the cognitive profile [27]. Even though our patients already underwent epilepsy surgery, our study found that D-galactose treatment can improve epilepsy and cognitive outcomes. Some explanations for that are the presence of MRI-undetected multilobar involvement [32] or surgical remnants, which is common in patients with MOGHE [3]. We hypothesize that D-galactose supplementation can improve the glycosylation in the remaining cells after surgery, ameliorating their functionality.
Regarding non-responder patients, it is remarkable that all of them were SLC35A2-negative. However, SLC35A2 subgroup analysis should be taken with caution. Although in our series, the frequency of SLC35A2 positivity in MOGHE patients (6/12) is similar to other series reporting around 45% of somatic pathogenic SLC35A2 variants in MOGHE brain samples [9], the lesser efficacy in SLC35A2 negative patients cannot be completely attributed to this finding. Variants in other genes of the N-glycosylation pathway or the lack of sensitivity of the sequencing techniques can also explain the SLC35A2 negativity. Thus, we cannot ascertain whether D-galactose is more effective in SLC35A2-positive patients. Furthermore, specific types of SLC35A2 variants may have different responses to D-galactose, which was not explored due to the low sample size of our study. However, due to the absence of biochemical determinations in our study, we cannot confirm whether galactose actually reaches the brain parenchyma of the affected patients, who indeed have a defective Golgi transporter. Additional studies involving pre-surgery D-galactose administration and the determination of galactose levels and glycosylation in the affected tissue would be necessary. These biochemical and metabolic assessments would provide crucial information on galactose availability and metabolism in the brains of patients with MOGHE, enabling a stronger understanding of its therapeutic effects. Future investigations incorporating these determinations can help validate the preliminary findings and establish a more robust scientific foundation for D-galactose use in patients with MOGHE.
In addition, the response might be worse in patients with severe phenotypes of developmental and epileptic encephalopathies and longer epilepsy duration. In our cohort, the best responder (case study, patient #8), who became completely seizure-free after D-galactose supplementation, had a “late-onset” form of MOGHE. He had an onset of intractable focal epilepsy at the age of 15 years but no learning difficulties or cognitive impairment. Larger samples are warranted to further elucidate this finding.
One of the main limitations of our study is its unblinded, non-placebo-controlled character and improvement being scored by the treating physicians. Future studies should include a double-blind randomized placebo-controlled design to increase the evidence and obtain more granular data. Since this is a relatively difficult-to-diagnose and rare condition, a double-blind, cross-over control study design could be the most affordable approach. Another limitation is the low number of patients, the lack of complete neuropsychological evaluation in centers other than HRI, and the short follow-up period, which might have underpowered the possibility of statistical analysis. Although the 6-month follow-up could be considered a limitation, the assessment tools [37,38,39,40,41,42] are parent-reported scales and do not show learning bias.
To date, this is the first pilot study of D-galactose in a cohort of histologically diagnosed MOGHE patients after surgery. Although these results warrant larger and controlled studies, they also suggest a window of opportunity to improve cognitive and seizure outcomes after surgery with D-galactose supplementation in patients with MOGHE, and provide preliminary evidence of the efficacy of precision medicine in this subgroup of patients.
Data Availability
De-identified data will be shared on request from any qualified investigator.
References
Hauptman JS, Mathern GW. Surgical treatment of epilepsy associated with cortical dysplasia: 2012 update. Epilepsia. 2012;53(Suppl 4):98–104. https://doi.org/10.1111/j.1528-1167.2012.03619.x.
Hartlieb T, et al. Age-related MR characteristics in mild malformation of cortical development with oligodendroglial hyperplasia and epilepsy (MOGHE). Epilepsy Behav 2019;91:68–74. https://doi.org/10.1016/j.yebeh.2018.07.009.
Barba C, et al. Clinical features, neuropathology, and surgical outcome in patients with refractory epilepsy and brain somatic variants in the SLC35A2 gene. Neurology. 2023 Jan 31;100(5):e528–42. https://doi.org/10.1212/wnl.0000000000201471.
Gaballa A, et al. Clinical characteristics and postoperative seizure outcome in patients with mild malformation of cortical development and oligodendroglial hyperplasia. Epilepsia. 2021;62(12):2920–31. https://doi.org/10.1111/EPI.17084.
Schurr J, et al. Mild malformation of cortical development with oligodendroglial hyperplasia in frontal lobe epilepsy: a new clinico‐pathological entity. Brain Pathol. 2017 Jan;27(1):26–35. https://doi.org/10.1111/bpa.12347.
D’Gama AM, et al. Somatic mutations activating the mTOR pathway in dorsal telencephalic progenitors cause a continuum of cortical dysplasias. Cell Rep. 2017;21(13):3754–66. https://doi.org/10.1016/j.celrep.2017.11.106.
Blumcke I, Budday S, Poduri A, Lal D, Kobow K, Baulac S. Neocortical development and epilepsy: insights from focal cortical dysplasia and brain tumours. Lancet Neurol. 2021;20(11):943–55. https://doi.org/10.1016/S1474-4422(21)00265-9.
Baldassari S, et al. Dissecting the genetic basis of focal cortical dysplasia: a large cohort study. Acta Neuropathol. 2019;138(6):885–900. https://doi.org/10.1007/S00401-019-02061-5.
Bonduelle T, et al. Frequent SLC35A2 brain mosaicism in mild malformation of cortical development with oligodendroglial hyperplasia in epilepsy (MOGHE). Acta Neuropathol Commun. 2021 Dec;9(1):1–3. https://doi.org/10.1186/s40478-020-01085-3.
Winawer MR, et al. Somatic SLC35A2 variants in the brain are associated with intractable neocortical epilepsy. Annal Neurol. 2018 Jun;83(6):1133–46. https://doi.org/10.1002/ana.25243.
Sim NS, et al. Precise detection of low-level somatic mutation in resected epilepsy brain tissue. Acta Neuropathol. 2019;138(6):901–12. https://doi.org/10.1007/S00401-019-02052-6.
Sim NS, et al. Brain somatic mutations in SLC35A2 cause intractable epilepsy with aberrant N-glycosylation. Neurol Genet. 2018;4(6):294. https://doi.org/10.1212/NXG.0000000000000294.
Vals MA, et al. Clinical, neuroradiological, and biochemical features of SLC35A2‐CDG patients. J Inherit Metab Dis. 2019 May;42(3):553–64. https://doi.org/10.1002/jimd.12055.
Ng BG, et al. SLC35A2-CDG: Functional characterization, expanded molecular, clinical, and biochemical phenotypes of 30 unreported individuals. Hum Mutat. 2019;40(7):908–25. https://doi.org/10.1002/HUMU.23731.
Beltrán-Corbellini Á, et al. Epilepsy genetics and precision medicine in adults: a new landscape for developmental and epileptic encephalopathies. Front Neurol. 2022;13. https://doi.org/10.3389/FNEUR.2022.777115.
French JA, et al. Adjunctive everolimus therapy for treatment-resistant focal-onset seizures associated with tuberous sclerosis (EXIST-3): a phase 3, randomised, double-blind, placebo-controlled study. The Lancet. 2016 Oct 29;388(10056):2153–63. https://doi.org/10.1016/S0140-6736(16)31419-2.
D’Gama AM, Poduri A. ‘Precision therapy for epilepsy related to brain malformations.’, Neurotherapeutics. 2021;18(3):1548–1563. https://doi.org/10.1007/s13311-021-01122-6.
Lim JS, et al. ‘Brain somatic mutations in MTOR cause focal cortical dysplasia type II leading to intractable epilepsy.’ Nat Med. 2015;21(4):395–400. https://doi.org/10.1038/nm.3824.
Hsieh LS, et al. Convulsive seizures from experimental focal cortical dysplasia occur independently of cell misplacement. Nat Commun. 2016;7:11753. https://doi.org/10.1038/ncomms11753.
Ljungberg MC, Sunnen CN, Lugo JN, Anderson AE, D’Arcangelo G. ‘Rapamycin suppresses seizures and neuronal hypertrophy in a mouse model of cortical dysplasia. Dis Model Mech. 2009;2(7–8):389–398. https://doi.org/10.1242/dmm.002386.
Nguyen LH, et al. mTOR inhibition suppresses established epilepsy in a mouse model of cortical dysplasia. Epilepsia. 2015;56(4):636–646. https://doi.org/10.1111/epi.12946.
Zhou J, et al. Pharmacological inhibition of mTORC1 suppresses anatomical, cellular, and behavioral abnormalities in neural-specific Pten knock-out mice. J Neurosci. 2019;29(6):1773–1783. https://doi.org/10.1523/JNEUROSCI.5685-08.2009.
Leitner DF, et al. Pilot study evaluating everolimus molecular mechanisms in tuberous sclerosis complex and focal cortical dysplasia. Plos one. 2022 May 19;17(5):e0268597. https://doi.org/10.1371/journal.pone.0268597.
Kato M, et al. Sirolimus for epileptic seizures associated with focal cortical dysplasia type II. A Clin Transl Neurol. 2022 Feb;9(2):181–92. https://doi.org/10.1002/acn3.51505.
Xu Q, et al. mTOR inhibitors as a new therapeutic strategy in treatment resistant epilepsy in hemimegalencephaly: a case report. J Child Neurol. 2019 Mar;34(3):132–8. https://doi.org/10.1177/0883073818813238.
Marsan E, et al. Depdc5 knockout rat: a novel model of mTORopathy. Neurobiol Dis. 2016;89:180–9. https://doi.org/10.1016/J.NBD.2016.02.010.
Witters P, et al. Clinical and biochemical improvement with galactose supplementation in SLC35A2-CDG. Genetics in Medicine. 2020 Jun 1;22(6):1102–7. https://doi.org/10.1038/s41436-020-0767-8.
Dörre K, et al. A new case of UDP-galactose transporter deficiency (SLC35A2-CDG): molecular basis, clinical phenotype, and therapeutic approach. J Inherit Metab Dis. 2015 Sep;38:931–40. https://doi.org/10.1007/s10545-015-9828-6.
Demos M, et al. Diagnostic yield and treatment impact of targeted exome sequencing in early-onset epilepsy. Front Neurol. 2019 May 21;10:434. https://doi.org/10.3389/fneur.2019.00434.
Willard A, Antonic-Baker A, Chen Z, O'Brien TJ, Kwan P, Perucca P. Seizure Outcome After Surgery for MRI-Diagnosed Focal Cortical Dysplasia: A Systematic Review and Meta-analysis. Neurology. 2022 Jan 18;98(3):e236–48. https://doi.org/10.1212/WNL.0000000000013066.
Lamberink HJ, et al. Seizure outcome and use of antiepileptic drugs after epilepsy surgery according to histopathological diagnosis: a retrospective multicentre cohort study. Lancet Neurol. 2020;19(9):748–57. https://doi.org/10.1016/S1474-4422(20)30220-9.
Xu S, et al. Multifocal mild malformation of cortical development with oligodendroglial hyperplasia (MOGHE) associated with SLC35A2 brain mosaicism. Clinical Neurophysiology: Official Journal of the International Federation of Clinical Neurophysiology. 2022 Nov 7;145:22–5. https://doi.org/10.1016/J.CLINPH.2022.11.001.
Freitag H, Tuxhorn I. Cognitive function in preschool children after epilepsy surgery: rationale for early intervention. Epilepsia. 2005 Apr;46(4):561–7. https://doi.org/10.1111/j.0013-9580.2005.03504.x.
Ladino LD, et al. Barriers impeding access to epilepsy surgery: a review of the literature. Revista de Neurologia. 2017 Sep 1;65(6):268–79.
Engel Jr JV. Outcome with respect to epileptic seizures. Surgical Treatment of the Epilepsies. 1993:609–22.
Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont) 2007;4(7):28–37
Grizzle R. Wechsler intelligence scale for children, fourth edition. in Encyclopedia of child behavior and development, S. Goldstein and J. A. Naglieri, Eds. Boston, MA: Springer US. 2011:1553–1555. https://doi.org/10.1007/978-0-387-79061-9_3066.
Gioia GA, Isquith PK, Guy SC. Behavior rating inventory of executive function. PAR Inc., 2015
Homack S, Riccio CA. Conners continuous performance test (2nd ed.; CCPT-II). J Atten Disord. 2006;9(3):556–558. https://doi.org/10.1177/1087054705283578.
Swanson JM, et al. Clinical relevance of the primary findings of the MTA: success rates based on severity of ADHD and ODD symptoms at the end of treatment. J Am Acad Child Adolesc Psychiatry. 2001;40(2):168–179. https://doi.org/10.1097/00004583-200102000-00011.
Swanson JM, et al. Categorical and dimensional definitions and evaluations of symptoms of ADHD: history of the SNAP and the SWAN rating scales. Int J Educ Psychol Assess. 2022;10(1):5. Accessed: Dec. 05, 2022. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4618695/
Snow A. Social communication questionnaire. In Encyclopedia of autism spectrum disorders, F. R. Volkmar, Ed. New York, NY: Springer New York. 2013:2893–2895. https://doi.org/10.1007/978-1-4419-1698-3_1651.
Casas-Fernández C. Experience with health quality of life questionnaire for the epileptic child (CAVE). Rev Neurol. 1997;25(139):415–421.
Varni JW, Seid M, Kurtin PS, PedsQL 4.0: reliability and validity of the pediatric quality of life inventory version 4.0 generic core scales in healthy and patient populations. Med Care. 2001;39(8):800–812. https://doi.org/10.1097/00005650-200108000-00006.
R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria, 2021.
RStudio Team. RStudio: integrated development environment for R. RStudio, Inc., Boston, MA, 2022.
Hino-Fukuyo N, et al. Genomic analysis identifies candidate pathogenic variants in 9 of 18 patients with unexplained West syndrome. Hum Genet. 2015;134(6):649–58. https://doi.org/10.1007/S00439-015-1553-6.
Funding
IB’s work was partially funded by the German Research Council (DFG Bl 421/4–1, DFG Bl 421/5–1).
Author information
Authors and Affiliations
Contributions
AAS and AGN conceived the original idea of the study. AAS, AGN, GG, IGM, RT, EH, BC, ABC, DMH, AB, TH, and MB recruited and evaluated the patients. RC, KK, and IB performed the histopathological diagnosis. SB, SB, RM, CDF, and IP carried out the genetics. IP performed the neuropsychological evaluation. AAS and AVC wrote the original manuscript. AVC performed the statistical analysis and created the plots. AAS, AVC, SB, IB, RM, and AGN revised the manuscript.
Corresponding author
Ethics declarations
Ethical Publication
We confirm that all the authors have read the journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Patient Consent
Written informed consent for participation/publication in this study was obtained from all parents or legal guardians.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

{kind=link}
Cite this article
Aledo-Serrano, Á., Valls-Carbó, A., Fenger, C.D. et al. D-galactose Supplementation for the Treatment of Mild Malformation of Cortical Development with Oligodendroglial Hyperplasia in Epilepsy (MOGHE): A Pilot Trial of Precision Medicine After Epilepsy Surgery. Neurotherapeutics 20, 1294–1304 (2023). https://doi.org/10.1007/s13311-023-01395-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13311-023-01395-z