
Abstract
Reductions in premature mortality are widely attributed to economic, educational, and medical factors. This study contributes to our understanding of the influence of political factors in preventing early death and gender inequalities in health outcomes. We analyze data from life tables of the World Health Organization, 2000–2015, to estimate the annual, sex-specific standard deviation of the age-at-death distribution across 162 countries. We apply dynamic panel model analyses to assess the association between political liberalization and inequalities in premature mortality. Our findings show reduced inequalities in premature mortality in liberal democracies, with men benefiting disproportionately. We theorize that liberal democracy may motivate governments to respond to citizens’ desires for policies that improve health and reduce risks. As democratic liberalization increases, premature mortality falls for men, which may be accounted for in part by reduced male mortality from injuries. Reductions in premature mortality for women appear to stem primarily from improvements in maternal mortality across regime types. Our findings support the idea that democratization may provide public health benefits, especially for male citizens.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Global health outcomes have significantly improved in recent decades, resulting in reduced premature mortality rates. Global child mortality, for example, has dropped by 60 percent since 1990 (World Health Organization 2022). Adult life expectancy has also improved globally for both men and women. Maternal mortality associated with pregnancy-related risks fell markedly, resulting in increased overall female life expectancy (World Bank et al. 2023). Yet around the world there remain enormous gaps both within and across countries in health outcomes such as premature mortality (Rajaratnam et al. 2010; Kuhn 2010; Rodriguez et al. 2015).
Improvements in premature mortality—deaths occurring before an individual’s expected number of life-years—are widely attributed to economic, educational, technological, and medical factors (McKeown and Record 1962; Caldwell 1986; Wilmoth 2007). Our analysis contributes to a relatively small yet growing literature bringing insights from comparative politics into research in public health. We argue that democratic liberalization reduces inequalities in premature mortality of adults, particularly male adults. Key democratic processes such as political representation and accountability may enable individuals to elect leadership and engage in collective action to affect policy action that may put them at lower risk of premature death in adulthood. In particular, we suggest that sex-specific causes of premature death, such as fatal injuries and accidents, may improve with democratic liberalization.
Recent scholarship has questioned the long-standing view that democracies are more likely to enable healthy and longer lives (Shandra et al. 2004; Burroway 2016). A wide literature shows beneficial effects of democracy on health, but several studies show no effect (Ross 2006; Mejia 2022). Much of what we know about the political factors influencing mortality comes from studies of infant and child mortality, life expectancy at birth, or maternal welfare (Rodriguez et al. 2022). For example, out of the 201 studies on democracy and population health reviewed by McGuire (2020), only four studies specifically explore adult mortality outcomes. Existing studies predominantly employ measures capturing the premature mortality of infants and young children, or central-tendency measures like the life expectancy at birth. We examine a different indicator, variation in premature mortality in adults, to consider alternative ways that regime type may matter for health outcomes over the course of life.
We use the standard deviation of the age-at-death distribution (S20) to measure variation in premature mortality of the adult population, for both men and women. An increasing standard deviation of age at death signals more deaths at younger adult ages, indicating increased inequality in lifespan. A decreasing standard deviation signals more deaths at older ages and less lifespan inequality, with a higher fraction of the population dying at older ages. Premature death is not evenly distributed across populations within and across nations (Rodriguez et al. 2014). Those with more economic, social, and political resources are better able to avoid risky circumstances such as dangerous occupations, poor infrastructure, exposure to pollutants, stress, unhealthy diets, and unhealthy behaviors that increase their risk of death (Geronimus et al. 2019). As these individuals show high rates of survival, they are also able to influence democratic processes for longer periods of their life (Rodriguez 2018). By exploring premature mortality in young adults and the middle aged, we can infer policy responsiveness to the most economically productive and politically active portion of nations’ populations. We ask whether premature mortality differs across levels of liberal democracy and, if so, whether these differences manifest differently for men and women.
We find that as nations increase their level of liberal democracy, they manifest a lower standard deviation in the age at death, even after accounting for levels of economic development, overall levels of mortality, and a battery of controls for endogenous processes. Liberal democracies appear to reduce lifespan inequalities primarily by lowering premature mortality in men (Mackenbach et al. 2013; Espelt et al. 2008; Wejnert 2008). Women do not show large, statistically significant differences in their age-at-death variation across regime types, even if the effect of democracy on variation in mortality is negative for women (i.e., it decreases the standard deviation of age at death), on average. We consider whether these differences by sex point toward possible mechanisms whereby regime type impacts inequalities in premature mortality. Democracies may be particularly likely to improve regulatory policies to reduce injuries, from occupational safety, road injury, and accidents, which disproportionately affect men (Bollyky et al. 2019; Scholz 1991; Kruk et al. 2018, Winslow 2005). In contrast, women’s health inequalities are generally reduced more as a function of the expansion of health care services and preventive care. Liberal democracy may enable collective action or electoral processes to reduce premature mortality via policies that result in lower incidence of injury, beyond larger gains in healthcare, which benefit both men and women but particularly men.
Our research contributes to the understanding of potential mechanisms whereby democratic processes may improve living standards, beyond levels of economic development. We also consider if electoral mechanisms and the legal exercise of collective action may provide channels to improve health and safety for the broad population. Our emphasis on risk and safety regulations also distinguishes our work from public health research focused primarily on healthcare systems. Possible implications of our study include that health gains and losses driven by democratization may come particularly in the form of differential exposure to physical and other risks.
By combining insights from comparative politics, public health, and social epidemiology, we contribute to research in comparative global health. The use of the standard deviation of age at death is novel to comparative politics. In international epidemiological studies it has been shown to capture health inequalities in a broad, consistent, and coherent cross-national framework (van Raalte et al. 2011; Edwards and Tuljapurkar 2005). Our focus on differential effects of regime type on health inequalities by sex is also novel to comparative politics, to our knowledge. Our study also fits within the public health tradition, asking whether features of democracy affect health equities with an interdisciplinary approach focused on potential causal mechanisms beyond medical determinants of health that may inform policies to increase health equity (Porta 2014).
We are also careful to address the methodological concerns of studying health inequalities in countries of very different levels of economic development and governmental structure. Estimating the impact of regime type on health outcomes is fundamentally challenged with concerns of endogeneity driven by the underlying relationship between economic development and democracy on the one hand, and economic development and health outcomes on the other. Health outcomes improve as countries get richer (Pritchett and Summers 1996; Weil 2014) and countries get richer as their populations get healthier (Bloom et al. 2004; Well 2007). Moreover, countries are more likely to be democracies when they are richer (Przeworski et al. 2000), and democratic factors have been shown to have indirect effects on economic output (Doucouliagos and Ulubaşoğlu 2008). Similarly, health outcomes including premature mortality have been shown to be a cause and effect of political processes (Rodriguez et al. 2015). We address these issues of endogeneity in our conceptual approach, examining outcome differences between the sexes to identify possible mechanisms of regime effects. We also place endogeneity at the forefront of our empirical approach with system generalized method of moments (SGMM) estimators.
Liberal Democracy and Health Outcomes
The literature in political science and epidemiology holds that democratic regimes are positively associated with improved health outcomes (overall levels and inequalities). Democratic regimes are found to be more active in producing health policy, delivering public health interventions, and institutionalizing health care systems. Among the espoused benefits of democracy are accelerated improvements in non-communicable diseases and injuries (Bollyky et al. 2019). Democracies also appear to reduce health inequalities across key factors such as gender and socioeconomic indicators (Bambra 2013).
Research arguing democracy improves public health emphasizes the role of electoral mechanisms, which may incentivize politicians to provide broader healthcare goods and services than in autocracies (Lake and Baum 2001; Huber and Stephens 2012; Wang et al. 2019; McGuire 2010). For example, Wigley and Akkoyunlu-Wigley (2017) argue that democratic leaders have greater motivation than autocratic leaders to reduce child mortality due to the electoral and economic benefits associated with improved infant health. Reeves and Mackenbach (2019) show that political participation is also strongly associated with lower health inequalities. Grépin and Dionne (2013) demonstrate that universal healthcare coverage is a visible policy issue generating high electoral dividends. Shandra et al. (2010) argue that democracy is a pre-condition for the effectiveness of international health and women’s organizations’ efforts to reduce infant mortality. Pieters et al. (2016) found that a democratic transition results in a decline in under-five mortality, with the effect increasing over time. If we think democracies are responsive to large groups, health is an evident policy area in which governments could improve life standards and its provision should substantially reduce health inequalities across the population (Mackenbach et al.2013).
Liberal democracies generally outperform autocracies in healthcare outcomes, with the benefits tending to accrue in high-income countries (Besley and Kudamatsu 2006). High-income liberal democracies have higher levels of redistribution, specifically in areas of healthcare and key social determinants of health such as education. A key argument is that, when people vote, they tend to vote for policies that help them as individuals, via human capital, rather than other types of capital that may also boost economic growth (Lake and Baum 2001). Moreover, elections provide incentives to extend human capital to the less fortunate to capture votes (Baum and Lake 2003; Stasavage 2005; Gerring et al. 2012). Kavanaugh (2016) argues that deliberation within liberal democracies also makes it more likely that citizens view health care as a human right and responsibility of the government. As a result, liberal democracies may enjoy more effective healthcare systems and lower health inequalities than non-democratic regimes at similar levels of economic development (Kuhn 2010; Ghobarahet al. 2004; Muntaner et al. 2011).
A related mechanism whereby democracy may matter for population health is through greater collective action opportunities (Bermeo and Yashar 2016). Political parties and civil society organizations are important stakeholders for improving human development. They serve as an informational pathway, imparting the needs of local communities, and putting pressure on politicians to improve health policies. Bernhard et al. (2019) emphasize the importance of collective action, arguing that political parties and social movements play a vital deterrent role to check political actors who might consider deviating from democratic agreements.
Collective action and direct participatory processes can lead to improved social welfare and health outcomes. Strong rule of law and constitutionally guaranteed civil rights and liberties are important for understanding the health effects of democratic engagement and functioning of democracy (Wigley and Akkoyunlu-Wigley 2011; Cheibub et al. 2020). Greer et al. (2017) show how in the early 1990s, civil society in newly democratic Poland pressured the government to adopt significantly improved standards of obstetric care and childbirth procedures. The success of Polish women was facilitated by a free and independent media. In Brazil, community organizations and social advocates pressed the judicial and legislative systems to achieve universal coverage for AIDS testing and treatment (Rich 2019). Research in India shows significant direct health benefits to the poor, especially for women, through local public participation institutions called gram sabhas and gram panchayat (Gibson 2012; Hamal et al. 2018).
Democratic processes of public engagement may encourage policy feedback that allows voters to influence healthcare policies. Citing examples from Thailand, Chile, and Costa Rica, McGuire (2010) shows reduced mortality (via improved regulations) and improved healthcare services that resulted from constituent pressure on government. The WHO found similar dynamics in the Philippines, Central America, and South Africa (World Health Organization 2007).
The need for an engaged civil society is emphasized during major health crises (Acharya et al. 2020). Epidemics and pandemics bring public health issues to the national level and mobilize citizens to demand an effective government response. Community groups and other civil society organizations have been important stakeholders in governmental responses to HIV/AIDS in Africa and Latin America (Björkman and Svensson 2009; Wamai 2014). Boone and Batsell (2001) suggest that political liberalization contributed to the effectiveness of policies responding to HIV/AIDS. Senegal and Uganda saw grassroots activism and awareness campaigns build broad legitimacy for AIDS prevention.
Yet research on regime type and health outcomes is not unified. Evidence of the link between democracy and child health is mixed, with some studies finding negative associations between health and democracy (for a review, see Mejia 2022). Some research finds that factors like economic development, improved sanitation, and educational attainment are more important as determinants of child health outcomes than regime type (Shandra et al. 2004; Burroway 2016). Dionne (2011) shows that time horizons, whether in democratic or autocratic regimes, explained government responses to AIDS in Africa.
The effects of democracy on health, if any, may also be indirect. Shandra et al. (2004) find no direct effects from democracy on infant mortality in develo** countries, but their results suggest that democracy might have a moderating effect, in which international dependency might negatively affect infant mortality at lower levels of democracy than at higher levels. Similarly, Noble (2019) finds no direct impact of democracy on infant mortality, but instead identifies a mediation effect: democracy increases public health spending, which is positively associated to socio-health resources, which in turn reduces infant mortality.
Health Inequalities by Sex and Regime Type
Our research contributes to the study of regime type on health outcomes as evidenced by gender disparities. Mackenbach et al. (2013) show that in Europe all-cause mortality among men decreases as democracies mature, but the democratization effect does not appear to reduce mortality among women. Similarly, Wejnert (2008) shows that women in develo** countries did not enjoy improved maternal health, labor force participation, and educational opportunities from democratic advancement between 1970 and 2000. Espelt et al. (2008) find that health inequalities in democracies are particularly prevalent for women.
Causes of death vary by sex and levels of economic development. Women are more likely than men to die of communicable diseases, and due to the sex-specific mortality risks associated with pregnancy, birth, and post-partum conditions. The World Bank estimates that about 50% of women around the world who die between ages 15 and 34 do so from communicable diseases (World Bank et al. 2016). Women in this age range are also vulnerable to chronic diseases, such as diabetes, cancer, and cardiovascular illness, as well as domestic violence, with the latter greatly underreported (Krantz 2002; Raymond et al. 2005). In contrast, about half of men who die prematurely (between ages 15–34) succumb to injuries from accidents, injuries, interpersonal violence, and self-harm (World Bank et al. 2016). These sex differences suggest how liberal democratic governance may possibly reduce premature mortality among men in particular, by advancing public health policies to regulate hazardous workplaces, improve road infrastructure, and reduce the overall risk of injury.
Democracy may foster social and institutional conditions conducive for collective action to seek public health protections. High-quality healthcare can ensue from political and legal accountability through laws and regulations, transparency, and greater political activism demanding improved working and living conditions. Workplace safety regulation is one of the areas in which we should see governments’ role in impacting mortality, particularly for men in the labor force who are disproportionately likely to die of injuries. Cross-national data on occupational mortality shows that its rate in non-democracies is about 30 percent higher than in democracies (ILO 2003). Democratic liberalization may also improve health outcomes and health inequalities if safety conditions are improved for a large percentage of the working population, especially as men are most likely to be engaged in the primary and secondary economic sectors in which injuries are particularly likely. Democracies also feel pressure to reduce environmental harm, including those that contribute to cancers and other non-communicable diseases (Winslow 2005).
As democratic liberalization increases, demands tend to rise for safer work and living conditions and a higher quality of life (Inglehart and Welzel 2005; Dorman 1986). For example, Bollyky et al. (2019) show that democracies attenuate the conditions that lead to injury. They estimate that democratic experience is associated with an 18-percent reduction in transportation injuries. Kruk et al. (2018) show that road injury deaths are also more likely to be averted by higher quality care offered in democracies when accidents do occur.
In industrialized nations, women live longer than men (Nathanson 1975; Read and Gorman 2010). Women’s health improves with economic development, and as healthcare services and sanitation reduce maternal mortality in particular, women live longer, reducing variation in premature death amongst women. Goldin and Lleras-Muney (2019) show a sharp reduction in infectious diseases in the early twentieth century contributed to improved female longevity in the United States and Europe. Despite living longer and faring better than men on the leading causes of death, women also experience more illness and comorbidity (communicable and non-communicable), especially at younger ages (Singh-Manoux et al. 2008). Factors impacting female mortality are primarily related to biological, behavioral, and socioeconomic factors (Mackenbach et al. 2008; Read and Gorman 2010; Freeman et al. 2020). Caldwell (1986) credits improvements in female empowerment and education for reduced female mortality and better health policies in poor nations. These may not be so readily improved in early stages of democratic development or may not differ drastically from those in less democratic societies. Overall, existing research suggests that political mechanisms may improve health outcomes disproportionately for men relative to women.
The Standard Deviation of Age at death
Our analysis employs the standard deviation of the age-at-death distribution conditional on survival to age 20 (S20). This measure captures inequalities in premature death among adults, and is useful for assessing and describing heterogeneity of a population’s wellbeing (Sasson 2016). In our study, S20 is a measure of the dispersion of proportions of individuals dying at different ages around the central tendency of the human lifespan in a given year and country. Accordingly, S20 captures the uncertainty of the length of life for adult populations exposed to country-specific characteristics, including political and economic ones. A larger value of S20 implies greater heterogeneity of the underlying factors that determine human longevity.
Our S20 indicator is calculated from the full distribution of period age-specific mortality rates above the age of 19. This is the age span in which most political activity, both electoral and nonelectoral, and mortality manifest. Given the left-skewed nature of the age-at-death distribution, with higher fractions of the population dying at older ages, S20 is particularly sensitive to deaths occurring before the central tendency of the age at death. Much of the inequality in mortality is due to early, preventable deaths and not due to mortality at older ages. These longevity benefits are parallel to the benefits to life expectancy at birth from reducing infant mortality.
Figure 1 provides an example of the age-at-death distribution for men in Iran. As the age-at-death distribution is compressed from 2000 to 2015, so is its standard deviation. The S20 decreases from 15.2 years to 12.4 years, with life expectancy at birth increasing from 69.1 years in 2000 to 75.8 years in 2015. In Iran, we observe that the decrease in S20 during the 15-year period is mostly due to averting premature deaths among adults, with an increased proportion of individuals in 2015 dying after the age where the two distributions intersect.

Age-at-death Distribution, Males, Iran, 2000 and 2015
conditional on survival to age 20.
As critical factors for survival become similar across adults, reduction in standard deviation of age at death should ensue. Reduction in S20 reflects the convergence of mortality scenarios that homogenize in populations, including political, economic, and social sources of variation in longevity. Low levels of variability in the age of death are particularly evident in economically advanced industrial nations, which are mostly democracies. These countries have high life expectancy at birth, relative to develo** nations, and are potentially approaching the biological limit of the human lifespan (Fries 1980; Olshansky et al. 1990; Wilmoth 2007; Vallin and Meslé 2010). Less developed nations, however, are likely to experience larger gains in life expectancy at birth, considering that a larger proportion of their population is still far away from the life expectancies experienced in advanced industrial democracies. While the age-at-death distribution remains relatively stable in advanced industrialized nations and middle income nations in the last decades, S20 is shrinking in the less developed world.
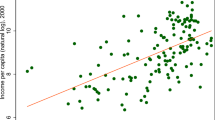
This situation is illustrated in Fig. 2. The S20 shrinks as countries become richer. This is particularly the case for women, for whom economic development appears to mitigate health risks for premature death, especially maternal conditions (Roser and Ritchie 2013; Wang 2014). The S20 falls for men as well as development increases, but to a lesser extent than for women. As the level of economic development increases, the sex difference in S20 also increases, with lower premature mortality among women relative to men.

Standard Deviation of Age-at-death and GDP per Capita by Sex. Note: All countries for all years (2000–2015) included
Another implication of these observations on mortality variation is that typical central tendency indicators of population well-being and longevity, such as life expectancy at birth, may remain relatively stable over long periods of time. In contrast, the S20 measure is more sensitive to variation arising from underlying mortality mechanisms within and across nations. Mortality inequality is primarily due to differences in the age at death among adults in wealthier countries (Tuljapurkar 2010). Central tendency measures of longevity may remain static in spite of increasing heterogeneity in death among middle-age and older adults, thus masking variation in underlying processes. Edwards and Tuljapurkar (2005) hold mortality displayed in life-tables should not only be characterized by the mean, or other measures of central tendency, but equally important by measures of the variability in the distribution of mortality rates. S20 therefore allows us to map variation—not linked to any particular age—that could not be otherwise captured by purely chronological age indicators of the lifespan (Kannisto 2000; Sasson 2016).
Data
Standard Deviation of Age-at-death
We collected annual abridged life tables for 162 countries over the 2000–2015 period from the World Health Organization’s Global Health Observatory. Our dataset includes nearly all countries across the full range of economic development. We use as our dependent variables the standard deviation of age at death for ages 20 and older (S20), separately for females and males, calculated with the fraction of people dying within a 5-year age group (from a standardized population of 100,000 individuals) in a given year. For illustration, see Table 1 in the Online Appendix showing Iran’s life-tables for 2000 and 2015.
The standard deviation measurement is regularly used in demographic and public health research. Demographers Wilmoth and Horiuchi (1999) state the standard deviation of age at death is one of the few measures of the variability in life tables that is easy to interpret, because it is expressed in years of age units.
To help visualize our dependent variable, Fig. 3 displays the distribution of S20 by terciles of countries’ levels of democratization for males and females for the first and last year of the period of analysis. Although males across all terciles have a higher median S20 than females, females have larger variation. The changes in female S20 from 2000 to 2015 in Botswana, South Africa, Namibia, and Tanzania (the outliers noted in the 2000 top tercile) exemplify the faster reduction of inequality in females’ age at death experienced by countries in the top tercile.

Standard Deviation of Age-at-death by Terciles of Liberal Component Index
Inter-quartile ranges remain relatively stable for males and females across terciles of democratization, with a small increase for top-tercile females in 2015 as outlier nations in 2000 were incorporated to the overall distribution by 2015. Slight differences are detected in the upper and lower whiskers, with a notable contraction for males and females in the bottom tercile. Overall, distributions of S20 shifted downwards from 2000 to 2015.
Independent Variables
Our independent variable of interest is the Varieties of Democracy Project’s (V-Dem) liberal component index (Coppedge et al. 2023). The V-Dem dataset has also been used in public health research to study the health effects of political regimes (Bollyky et al. 2019). The liberal component index gauges the democratic quality of a political regime by how much the government is constrained from taking unilateral actions against individuals and institutions. It emphasizes the rule of law and protection of individual and minority rights, especially free assembly and free press, as well as constitutional limits on executive power.
The liberal component index is an aggregate measure of the following indices: 1) equality before the law and individual liberties; 2) judicial constraints on the executive; and 3) legislative constraints on the executive (Coppedge et al. 2023). The first component of the index focuses on transparent and impartial laws and administration, and access to justice and freedom. The second component measures the judiciary’s ability to act independently and the executive’s compliance with court rulings. The third component measures the legislature’s ability to investigate, question, and overrule the executive.Footnote 1 The index ranges from 0 to 1, with 0 indicating the total absence and 1 indicating the total achievement of liberal democratic principles. It should be noted that the meaningfulness of elections, electoral participation of citizens in the political process, and political responsiveness of the elected officials are beyond the scope of the liberal component index. Nonetheless, these factors are likely to be highly correlated with the liberal components index.
For our study period, the liberal component index has an average of 0.62, with Eritrea showing the lowest score at 0.01 and Norway the highest at 0.98. Figure 4 depicts patterns of S20 over time for a selection of countries at each tercile of the liberal components index, by sex. Across all terciles of the liberal components index distribution, we see overall reductions in S20, with notable recent exceptions of countries in the Americas (e.g., Brazil, Mexico, United States). Perhaps the main pattern in Fig. 4 is the increasingly lower S20 for males and females as we move from the bottom to the upper tercile of the liberal component index distribution, with overall S20 values markedly lower at the upper tercile.

Standard Deviation of Age at Death, by Sex and Regime Type
In addition to the liberal component index, we use a measure of electoral participation to capture the extent of political engagement. The variable is the total percentage of voters who cast a vote in an election (Vanhanen 2019). All other control variables come from the Quality of Government (QoG) dataset, compiled from multiple original sources (Teorell et al. 2021). We include the level of economic development, proxied by GDP per capita in 2010 US dollars from the World Development Indicators (WDI) (World Bank n.d.), and life expectancy at birth by sex (World Health Organization 2015). As discussed above, improvements in health outcomes are strongly associated with increased economic development and regime type.
Life expectancy is a crucial factor to include in our analysis, given that longer life expectancy is associated with lower premature mortality, higher economic development, and regime type. Life expectancy at birth and the standard deviation of age at death are both dimensions of mortality, and life expectancy is a standard control in epidemiological studies of S20 to control for aspects related to the central tendency of longevity (Wilmoth and Horiuchi 1999; Tuljapurkar 2010; Vaupel et al. 2011).
We also include standard sociodemographic controls for health outcomes in cross-national studies: unemployment rate measured as the percentage of unemployed individuals in the labor force) (ILO 2020); the percentage of rural population (World Bank n.d.), and number of years of educational attainment for individuals between 35 and 44 years of age (IHME 2015). An additional control included in our models is a one-year lagged version of the dependent variable, which should capture variation not explained by other control variables, and which offers a highly conservative estimate of the impact of our independent variables of interest.
Table 1 reports summary statistics for our analytic sample. Although the average S20 for females is one year less than for males (Male = 15.2 vs. Female = 14.1), its range is larger (as low as 9.4 in Kuwait and as high as 21.1 in South Africa) relative to a range of 11.2–19.4 years for males. In most countries S20 is lower for women than men, but in some atypical cases in Sub-Saharan Africa, such as Lesotho and Gabon, S20 is higher for women than men. This likely reflects persistently high maternal mortality and health outcomes associated with poverty as a main cause of high variability of women’s age at death.
We also find a wide range of variation across our control variables. Given the inclusion of dictatorships in the analytic sample, the electoral participation variable ranges from 0 to 70. Although average participation increased by almost six percentage points from 2000 to 2015 (from 33.5% to 39%), the variance of this measure remained high (SD2000 \(\approx\) 19 and SD2015 \(\approx\) 17), reflecting wide differences between regime types. The overall average unemployment rate for females is larger than it is for males (8.97 and 7.17, respectively). Both distributions—for males and females—are skewed to the right with a set of countries showing particularly high levels of unemployment, mostly in Eastern Europe and Africa. Similarly, overall average educational attainment is one school-year higher for young adult males (~ 9 years) than for females (~ 8 years), with the latter exhibiting higher variation (SDmales = 4.18 vs. SDfemales = 3.24). Logged GDP per capita illustrates the significant income inequality across nations, with a lowest value of 5.27 (or about $195 U.S. dollars per capita in a year) to a maximum value of 11.63 (or about $112,500 U.S. dollars per capita in a year). Lastly, life expectancy in our sample shows that females (71.5 years) tend to live longer than men (66.8 years), on average, with great inequalities, ranging between 33.2 and 81.2 years for men, and a 40 to 87 years for women, in our study period.
Methods
A central challenge of research using political variables to predict public health outcomes is the potential endogeneity of the analyzed variables. Notably, democracy has long been argued to be a function of level of development, and health outcomes themselves may in turn impact levels of development and democracy. As people have better health outcomes, they can contribute to the economy more productively and for a longer period of their life, thus improving the economy. As health improves, people have more time, accessibility, and resources to engage in politics, thus improving democratic processes as well. Accordingly, an analysis such as ours requires consideration of endogenous processes within our econometric framework.
Our estimation strategy is based on the system generalized method of moments (SGMM) estimator for dynamic models of panel data developed by Arellano and Bover (1995) and Blundell and Bond (1998). The properties of the SGMM estimator fit the purpose of our study as it addresses data limitations and supports our underlying assumptions. First, our panel structure has a large number of panels (n = 162) relative to its number of periods (T = 16). SGMM is appropriate for this panel structure. Second, as a first approximation and to simplify our interpretation of parameter estimates, we can assume that the underlying associations specified in our models follow a linear function. Our parameters, therefore, can be interpreted as changes in our dependent variable with respect to a given explanatory variable independent of the value of the explanatory variable, and our parameters can also be assumed not to be a function of other parameters. We tested, yet did not find, non-linearity among variables and parameters in our models.
Third, the SGMM estimator allows our dependent variable—the standard deviation of the age-at-death distribution conditional on survival to age 20—to manifest inertia in time and behave as a country-specific slow-moving series. The SGMM is particularly appropriate for such panel dynamics. Fourth, the SGMM estimator accounts for the fact that the variables on the right side of our econometric equation (democratic liberalization and socio-economic controls) are not strictly exogenous, exhibiting inertia in time and contemporaneous correlation in their errors. This feature helps us manage endogeneity specifically. Fifth, these errors can also be assumed heteroskedastic and autocorrelated within countries, but not across them (for which we included time fixed-effects in our model specifications, removing global time-related shocks from the errors). And finally, the SGMM estimator also accounts for unobserved heterogeneity across countries.
The econometric specification of our main model is of the form:
where \({{\sigma }_{20},}_{it}\) is our dependent variable—i.e., the standard deviation of age-at-death for ages 20–85 + for country i in time t. The first term \({{\sigma }_{20},}_{i(t-1)}\) is a 1-year lagged version of our dependent variable. \({L}_{it}\) stands for the democratic liberalization component index, for country i in time t. The expression \(\sum_{j=1}^{n}{\delta }_{j}{X}_{it}\) is a vector of n endogenous covariates \({X}_{it}\) (in our case, the gender-specific unemployment rate, share of the rural population, logged GDP per capita, gender-specific educational attainment in middle ages 35–44 years, voter turnout, and gender-specific life expectancy) for country i in time t, each covariate with its respective coefficient \({\delta }_{j}\). The term T is a vector of time fixed effects, and \({\varepsilon }_{it}\) is the error term—assumed to be independent for each country i for all t. We include the complete econometric specification of our system of equations with detailed descriptions of our SGMM instruments in the Online Appendix, Sect. 2, as well as tests of the underlying assumptions behind and appropriateness of our models in Sect. 3.
Results
The SGMM parameter estimates for six models are included in Table 2. Models 1 and 4 report the estimated effect of the liberal component index, without the inclusion of controls, on male and female S20, respectively; models 3 and 6 include all controls. Results for models with only controls (i.e., excluding the liberal component index) are included in models 2 and 5.
Our main result is that liberal democracy shows different levels of association with premature mortality by sex. The liberal component index is negative and statistically significantly related to inequality in premature mortality for males. This is not the case for females, which is still negative, yet half the size of the estimate for males and not precisely estimated.
The effect size is also substantive for men. A one-unit increase in the liberal component index (e.g., going from a country with total absence of, to one with total achievement of liberal democratic components) is associated with a decrease in male S20 of 1.25 years (p < 0.01), on average. The size of this annual estimate is meaningful, especially when considering that the total reduction of the mean male S20 in our 162-country sample between 2000 and 2015 is 0.61 years (Table 1). Correspondingly, these 0.61 years are achieved by an increase in the liberal component index of 0.49 units. For instance, should a country undergo a democratic transition, such as going from the level of Nicaragua (= 0.43) to that of Uruguay (= 0.92), or from Myanmar (= 0.15) to Thailand (= 0.62), we would expect a decrease in premature mortality of 0.61 years—or, the equivalent to the decrease in premature mortality in a 15-year period. This effect is robust to model specification (including additional controls), estimation strategy, and the use of different GMM estimators, and alternative calculations of the dependent variables. See Online Appendix Sect. 4.
We also consider whether economic development helps to explain reductions in premature mortality. The coefficient for logged GDP per capita is significant in the model for men without the liberal component index (Model 2); yet, once the liberal component index is included, the size of the economic effect is almost halved and it loses statistical significance (Model 3). Unlike the scenario for males, the liberal component index does not affect the coefficient size of logged GDP per capita for women, which is much smaller than for males and not statistically significant (models 5 and 6). This suggests that, if economic development has mitigating effects on female lifespan variation, then characteristics unique to liberal democratic regimes do not account for these effects, and vice versa.
The electoral participation measure does not have a statistically significant effect on premature mortality for either men or women when the liberal component index is included in the model. The sign of this coefficient, nonetheless, goes from positive \((\widehat{\delta }=.0004)\) to negative \((\widehat{\delta }=-.005)\) when the liberal index is excluded from the model for males, then showing a statistically significant negative effect on S20 (Model 2). This result may reflect a crucial importance of liberalization, including constraints on the executive and civil liberties, in reducing premature mortality of adult men, beyond the legal ability to vote. The coefficient of the electoral participation variable for females are small and do not reach statistical significance. This suggests that neither electoral nor liberal democratic mechanisms tested in our analyses appear to improve inequalities in premature mortality for women at the same level as they do for men. In our Online Appendix Table A8 we also include results with an indicator of civil society participation as alternative independent variable capturing a possible mechanism of liberal democratic processes. Our results are consistent with the civil society participation variable substituted in our models.
Not surprisingly, we find that a higher life expectancy is associated with a decrease in S20. This relationship is particularly strong for females. As their life expectancy at birth improves, so does their premature mortality. These annual estimates are also large, especially considering the slow movement of the average age-at-death, variation in the age-at-death distribution, and life expectancy in populations, and that these figures apply to the total population of 162 countries.
The estimates for the autoregressive terms show that, compared to the male S20, the variability in female age at death tends to remain relatively stable over time. Given the strictness of our model focusing on endogenous processes and including lag dependent variables on the right side of Eq. 1, we do not observe strong relationships between our controls and the dependent variables in most models. Estimates for all other sociodemographic controls either do not reach statistical significance or are substantively trivial.
Models with Causes of Death
We also test whether increased democracy reduces premature mortality for men (and women) via the potential mechanism of improved safety and reduced risk, and whether increased democracy might reduce premature mortality for women (and men) via communicable and nutritional diseases, and maternal mortality. We collected data on estimated causes of death, by gender, from the Institute for Health Metrics and Evaluation (2015). Table 3 includes parameter estimates of our base models (Models 3 and 6 in Table 2) including three relevant causes of death: fatal injuries (expected to affect men disproportionately), communicable and nutritional diseases (expected to afflict both men and women), and maternal mortality (affecting only women). For each model, we include the sex-specific death rate according to each cause.
Model 1 in Table 3 shows support for the idea that higher deaths from injuries (from all causes of injury) are associated with higher S20 in men. The coefficient of the liberal component indicator remains significant in this model, but the coefficient size decreases, possibly indicating that some of the variation in premature mortality originally explained by the liberal component index could be attributed to the mortality rate due to injuries in men—with lower injury mortality rates in liberal democracies. In contrast, we do not see a significant impact of communicable disease rates on men’s inequalities in premature death in Model 2. These findings are consistent with the idea that liberal democracy may improve health inequalities for men via improvements in safety that reduce risk.
We observe a reduction in the size of the coefficient of the liberal democratization indicator once female injury death rates are included in the model, suggesting the possibility that some of the association originally detected between S20 and liberal democratization may be partially mediated by injury death rates (Model 3). Similar to men, lower injury mortality rates.
for women are observed in liberal democracies. Both coefficients for women, nevertheless, remain non-statistically significant. In contrast, we observe an increase in the size of the liberal democratization coefficient once communicable disease death rates are included in the model (Model 4). Although both coefficients remain non-statistically significant, this finding suggests that the association between female’s premature mortality and liberal democratization may be partially mediated by higher communicable disease death rates for women in liberal democracies than in non-liberal ones.
As expected, we find that women’s S20 is highly related to maternal mortality (Model 5). We also find that, once the maternal mortality rate is included in the model, its coefficient is large and statistically significant while the coefficient for liberal democratization collapses toward zero (Model 5). This finding suggests that, even though the coefficient for liberal democratization was not precisely estimated, maternal mortality mediates nearly the totality of its impact. The negative (although statistically insignificant) association between premature mortality of females and liberal democratization in the reference models appears to be explained by differences in maternal mortality rates between liberal and non-liberal democracies—with liberal democracies producing lower maternal mortality rates than non-liberal ones. Our estimates are consistent with the idea that improvements in life expectancy and the standard deviation of age at death for women come in great part from reductions in maternal mortality for young and young-adult women of child-bearing age.
Discussion and Conclusion
Our results provide empirical support for the proposition that democratic liberalization improves premature mortality. We find a robust, large, and statistically significant association between the degree of liberal democracy and the contraction of inequalities in premature mortality across nations. The effect, although favorable in both instances, is only precisely estimated for males and not for females. Our findings are empirically reliable and causally informative as we account for endogenous processes related to health outcomes, democracy, economic development, electoral participation, and life expectancy, among others. Our findings suggest that liberal democratization may generate a feedback-loop of political advantages: as nations experience lower premature mortality, their citizens have more opportunities to participate in politics and increase their community involvement, which in turn produce a more informed and active citizenry—all fundamental conditions for healthy and stable democracies. We also discuss several possible mechanisms that may help to explain the reduction in adult male’s premature mortality associated with liberal democracy, including less exposure to occupational and unintentional injuries or road accidents in comparison to less liberal regimes. As nations move up the ladder in democratic principles, they tend to invest more in the sectors that improve occupational safety and decrease accidents and injuries. These types of policies disproportionately reduce premature death inequalities among men.
We also find evidence, although weaker, suggesting that inequalities in female premature mortality may be improved by liberal democratization. Even though our liberalization index coefficients are not precisely estimated, we do find evidence suggesting that its association with premature mortality among females is mediated through the improvement of maternal conditions. The stability of the models, the strength of the associations, and the precision of estimates favor the greater benefits that males can achieve from the advancement of democratic principles, as opposed to females. These results emphasize the paradox that democratic principles, while likely enhancing the quality of life for citizens, may not necessarily address gender equality.
Our research may be particularly relevant to public health as we are experiencing a period of democratic backsliding around the world and a recent decline in life expectancy in the United States (Bermeo 2016; Mechkova et al. 2017; Waldner and Lust 2018). If democracy encourages politicians to improve health and safety, or if it provides opportunities for citizens to engage in collective action to improve health outcomes, we may see stagnation in global gains in gender health equality and in the reduction of premature mortality among men. Son and Bellinger (2022) find empirical evidence of the high cost of authoritarianism to public health. They show that a rise in authoritarianism reduces healthcare spending, increases infant mortality, and decreases female life expectancy. The authors posit that weakening of liberal democratic components of democracy, such as freedom of expression, association, clean elections, and undermining of legislature by the executive are all associated with adverse health outcomes. While global trends in health outcomes have been showing success for several decades, this progress may not continue at the same pace as many nations limit political freedoms. At the same time, paradoxically, gender inequalities in premature death may decrease, not because of the stagnation of health improvements for females due to the deterioration of health improvements for males.
Our research findings have implications regarding the potential for greater liberalization to influence health policies even in non-democracies. Though citizens of non-democracies may have limited agency to challenge the state directly, it may be possible to influence autocratic decision makers through informal networks and the pressures of media. Access to information related to health issues could be expanded by strengthening grassroots advocacy and independence of media. Additionally, people in non-democracies may be able to work directly with key constituencies that comprise a base of support for the regime and influence policy changes that will improve public health. These efforts may be particularly efficacious to improve outcomes if influential social groups can stress to autocratic governments potential improvements in economic productivity among working age people, and how reductions in premature mortality may help the economy.
Research into political processes within authoritarian regimes shows ostensibly democratic institutions, such as political parties and elections, however stage-managed they might be by autocratic rulers, are important structures to garner support from key constituencies and offer democratic validity for authoritarian control (Gandhi 2008). Most autocratic nations have some “popular” institutions, including voting for legislatures or local government officials. Such political opportunities may be beneficial for citizens in non-democracies to demand improvements in health through adoption of laws and regulations and allocation of resources to minimize risks of premature death from childbearing, occupational hazards, and poorly maintained infrastructure.
Our study has also implications for international multilateral organizations and non-profits focused on public health. These groups may improve public health outcomes by explicitly recognizing the association between democracy, including the role of civil society and social movement pressures, and health outcomes. Our research suggests it is not only the affluence and material resources of democracies that positively affect people’s health, but the degree of citizen involvement and input into decision-making. Institutional oversight over the executive, rule of law, and civil liberties and rights may be key for health improvements. The political empowerment of citizens likely needs to come from within the society and its political values, but these organizations can provide opportunities for education and resources to push for improvements for both men and women.
Our research findings also put into focus the importance for these organizations to adopt strategies for equal access to vaccinations and medication to tackle communicable diseases, especially among young and middle-aged adults. Financial aid and loans could also include programming to improve regulations related to workplace hazards and more aggressive improvements in sanitation, hygiene, and infrastructure.
Our research considers variation in premature adult mortality across the globe and provides supporting evidence that political liberalization may be one of the possible means toward effective action for global health. The most pressing needs for mitigation are in places with very high adult premature mortality; for one critical example, certain Sub-Saharan African nations known for high prevalence of HIV and maternal mortality. Latin America is also an important region to examine as variation in premature mortality has increased due to interpersonal violence, road injuries, and ischemic heart diseases as the leading causes (Wang et al. 2016). The Americas is also the region of the world in which levels and inequality in premature mortality are growing worse, including the United States (Bound et al. 2015; Geronimus et al. 2019). El Salvador is a case in point, with extremely high inequalities in male lifespans. The trends in the Americas suggest that for middle- and high-income countries, addressing causes of preventable death may be critical.
There are several limitations of this study. First, our analysis includes a large sample of 162 countries, representing a wide range of variation in economic and government systems across the globe. Yet, our results may not be generalizable to especially small and poor nations, which were excluded from our study due to lack of data availability. Second, our liberal component index is a crude, overall estimate that attempts to capture as much variation as possible about factors that previous research linked to processes of liberal democracy. Although our chosen index is well-established in the literature, and available for a large sample of countries, the process that generates the variable as well as each of its underlying components may induce non-essential variation and measurement error in the overall index indicator. As such, our findings should be interpreted in the context of summary indexes of liberal democracy and not in the context of specific characteristics of regimes. Future research should examine the specific mechanisms whereby democracies reduce premature mortality, and on how to make those favorable effects spill over to females. We have theorized certain mechanisms, especially risk reductions in the workplace, on the road, and due to violent conflict, that could be tested with more detail in subsequent studies.
The implications of our research for global health are such that achieving equity in global outcomes via international cooperation and aid is more likely if the sources of these inequities lie in economics, medical technological advancement and knowledge, or education. Global health inequalities driven by politics are likely to only be addressed by social and political development at the national and local levels, which may be improved by increased liberalization.
Data Availability
The dataset and replication files for this study can be found on the Harvard Dataverse: https://dataverse.harvard.edu/dataset.xhtml?persistentId=doi:10.7910/DVN/UQMFEN&faces-redirect=true.
Notes
Empirical tests show that measures of electoral aspects of democracy operationalized in more fined-grained levels and aggregated in a multiplicative manner are more likely to show an impact on mortality outcomes, such as the infant mortality rate (Gerring et al. 2021). V-Dem's liberal component index is additively aggregated as an average of the aforementioned components, which can make a statistically significant association less likely.
References
Arnab, Acharya, Gerring John, and Aaron Reeves. 2020. Is health politically irrelevant? Experimental evidence during a global pandemic. BMJ Global Health 5:10.
Arellano, Manuel, and Olympia Bover. 1995. Another look at the instrumental variable estimation of error-components models. Journal of Econometrics 68 (1): 29–51.
Bambra, Clare. 2013. In defense of (social) democracy: On health inequalities and the welfare state. Journal of Epidemiological Community Health 67 (9): 713–714.
Baum, Matthew, and David Lake. 2003. The political economy of growth: Democracy and human capital. American Journal of Political Science 47 (2): 333–347.
Bermeo, Nancy. 2016. On democratic backsliding. Journal of Democracy 27 (1): 5–19.
Bermeo, Nancy, and Deborah J. Yashar, eds. 2016. Parties, movements, and democracy in the develo** world. Cambridge University Press.
Bernhard, Michael, Allen Hicken, Christopher Reenock, and Staffan I Lindberg. 2019. Parties, civil society, and the deterrence of democratic defection. Studies in Comparative International Development 55(1):1–26.
Besley, Timothy, and Masayuki Kudamatsu. 2006. Health and democracy. American Economic Review 96 (2): 313–318.
Björkman, Martina, and Jakob Svensson. 2009. Power to the People. The Quarterly Journal of Economics 124 (2): 735–769.
Bloom, David, David Canning, and Jaypee Sevilla. 2004. The effect of health on economic growth. World Development 32 (1): 1–13.
Blundell, Richard, and Stephen Bond. 1998. Initial conditions and moment restrictions in dynamic panel data models. Journal of Econometrics 87 (1): 115–143.
Bollyky, Thomas, Tara Templin, Matthew Cohen, Diana Schoder, Joseph Dieleman, and Simon Wigley. 2019. The relationships between democratic experience, adult health, and cause-specific mortality in 170 countries between 1980 and 2016: An observational analysis. Lancet 393 (10181): 1628–1640.
Boone, Catherine, and Jake Batsell. 2001. Politics and AIDS in Africa. Africa Today 48 (2): 3–33.
Bound, John, Arline T. Geronimus, Javier M. Rodriguez, and Timothy A. Waidmann. 2015. Measuring recent apparent declines in longevity: The role of increasing educational attainment. Health Affairs 34 (12): 2167–2173.
Burroway, Rebekah. 2016. Democracy and child health in develo** countries. International Journal of Comparative Sociology 57(5): 338–64.
Caldwell, John C. 1986. Routes to low mortality in poor countries. Population and development review :171–220.
Cheibub, José Antonio, Ji Yeon Jean Hong, and Adam Przeworski. 2020. Rights and deaths: Government reactions to the pandemic. SSRN 3645410.
Coppedge, Michael, et al. 2023. V-Dem Dataset v13. Varieties of democracy (V-Dem) Project.
Dionne, Kim Yi. 2011. The role of executive time horizons in state response to AIDS in Africa. Comparative Political Studies 44 (1): 55–77.
Doucouliagos, Hristos, and Mehmet Ali Ulubaşoğlu. 2008. Democracy and economic growth: a meta‐analysis. American Journal of Political Science 52(1):61–83.
Dorman, Peter. 1986. Markets and mortality. Cambridge University Press.
Edwards, Ryan, and Shripad Tuljapurkar. 2005. Inequality in life spans and a new perspective on mortality convergence across industrialized countries. Population and Development Review 31 (4): 645–674.
Espelt, Albert, Carme Borrell, Maica Rodriguez-Sanz, Carles Muntaner, M. Isabel Pasarin, Joan Benach, Maartje Schaap, Anton Kunst, and Vicente Navarro. 2008. Inequalities in health by social class dimensions in European countries of different political traditions. International Journal of Epidemiology 37(5):1095–1105.
Freeman, Toby, Hailay Abrha Gesesew, Clare Bambra, Elsa Regina Justo Giugliani, Jennie Popay, David Sanders, James Macinko, Connie Musolino, and Fran Baum. 2020. Why do some countries do better or worse in life expectancy relative to income? An analysis of Brazil, Ethiopia, and the United States of America. International Journal for Equity in Health 19(1):1–19.
Fries, J.F. 1980. Aging, natural death, and the compression of morbidity. New England Journal of Medicine 303 (3): 130–135.
Geronimus, Arline, John Bound, Timothy Waidmann, Javier Rodriguez, and Brenden Timpe. 2019. Weathering, drugs, and whack-a-mole. Journal of Health and Social Behavior 60 (2): 222–239.
Gerring, John, Strom C. Thacker, and Rodrigo Alfaro. 2012. Democracy and human development. Journal of Politics 74 (1): 1–17.
Gerring, John, Carl Henrik Knutsen, Matthew Maguire, Svend-Erik Skaaning, Jan Teorell and Michael Coppedge. 2021. Democracy and human development: issues of conceptualization and measurement. Democratization 28(2):308–332.
Gandhi, Jennifer. 2008. Political Institutions under Dictatorship. Cambridge: Cambridge University Press.
Ghobarah, Hazem Adam, Paul Huth, and Bruce Russett. 2004. Comparative public health: The political economy of human misery and well-being. International Studies Quarterly 48(1):73–94.
Gibson, Christopher. 2012. Making redistributive direct democracy matter: Development and women’s participation in the Gram Sabhas of Kerala, India. American Sociological Review 77 (3): 409–434.
Goldin, Claudia, and Adriana Lleras-Muney. 2019. XX> XY?: The changing female advantage in life expectancy. Journal of Health Economics 67: 102224.
Greer, Scott L., Matthias Wismar, Gabriele Pastorino, and Monika Kosinska. 2017. Civil Society And health: Contributions and potential. Health Policy Series, 48. World Health Organization.
Grépin, Karen, and Kim Yi Dionne. 2013. Democratization and universal health coverage: A case comparison of Ghana, Kenya, and Senegal. Global Health Governance 6(2).
Hamal, Mukesh, Tjard de Cock Buning, Vincent De Brouwere, Azucena Bardají, and Marjolein Dieleman. 2018. How does social accountability contribute to better maternal health outcomes? A qualitative study on perceived changes with government and civil society actors in Gujarat, India. BMC Health Services Research 18:1–15.
Huber, Evelyne, and John D. Stephens. 2012. Democracy and the left: Social policy and inequality in Latin America. University of Chicago Pres.
Inglehart, Ronald, and Christian Welzel. 2005. Modernization, cultural change and democracy. Cambridge University Press.
Institute for Health Metrics and Evaluation. (2015). Global educational attainment 1970–2015.
International Labour Organization. (2003). World Statistic.
International Labour Organization. (2020). ILOSTAT database.
Kannisto, Vaino. 2000. Measuring the compression of mortality. Demographic Research 3.
Kavanaugh, Matthew M. 2016. The right to health: Institutional effects of constitutional provisions on health outcomes. Studies in Comparative International Development 51 (3): 328–364.
Krantz, Gunilla. 2002. Violence against women: A global public health issue! Journal of Epidemiology & Community Health 56 (4): 242–243.
Kruk, Margaret, Anna Gage, Catherine Arsenault, Keely Jordan, Hannah Leslie, Sanam Roder-DeWan, and Olusoji Adeyi. 2018. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. The Lancet Global Health 6 (11): e1196–e1252.
Kuhn, Randall. 2010. Routes to low mortality in poor countries revisited. Population and Development Review 36 (4): 655–692.
Lake, David, and Matthew Baum. 2001. The invisible hand of democracy: Political control and the provision of public services. Comparative Political Studies 34 (6): 587–621.
Mackenbach, Johan, Irina Stirbu, Albert-Jan. Roskam, Maartje Schaap, Gwenn Menvielle, Mall Leinsalu, and Anton Kunst. 2008. Socioeconomic inequalities in health in 22 European countries. New England Journal of Medicine 358 (23): 2468–2481.
Mackenbach, Johan, Hu. Yannan, and Caspar Looman. 2013. Democratization and life expectancy in Europe, 1960–2008. Social Science & Medicine 93: 166–175.
McGuire, James. 2010. Wealth, health, and democracy in East Asia and Latin America. Cambridge University Press.
McGuire, James. 2020. Democracy and population health. Cambridge University Press.
McKeown, Thomas, and R. Graham Record. 1962. Reasons for the decline of mortality in England and Wales during the nineteenth century. Population studies 16(2):94–122.
Mejia, Steven. 2022. Democracy and health in develo** countries: New cross-national evidence, 1990–2016. Sociological Perspectives 65(5):981–1000
Mechkova, Valeriya, Anna Lührmann, and Staffan I. Lindberg. 2017. How much democratic backsliding? Journal of Democracy 28 (4): 162–169.
Muntaner, Carles, Carme Borrell, Edwin Ng, Haejoo Chung, Albert Espelt, Maica Rodriguez-Sanz, Joan Benach, and Patricia O’Campo. 2011. Politics, welfare regimes, and population health: Controversies and evidence. Sociology of Health & Illness 33 (6): 946–964.
Nathanson, Constance. 1975. Illness and the feminine role: a theoretical review. Social Science & Medicine 1967 9(2):57–62.
Noble, Mark. 2019. Democracy and Infant Mortality in Less-Developed Nations: Dismantling Differences in Direct and Indirect Effects Modeling. Sociological Perspectives 62 (3): 282–307.
Olshansky, S. Jay, Bruce A. Carnes, and Christine Cassel. 1990. In search of Methuselah: estimating the upper limits to human longevity. Science 250(4981):634–640.
Pieters, Hannah, Daniele Curzi, Alessandro Olper, and Johan Swinnen. 2016. Effect of democratic reforms on child mortality: A synthetic control analysis. The Lancet Global Health 4 (9): e627–e632.
Porta, Miquel, ed. 2014. A dictionary of epidemiology. Oxford university press.
Przeworski, Adam, R. Michael Alvarez, Jose Antonio Cheibub, and Fernando Papaterra Limongi Neto. 2000. Democracy and development: Political institutions and well-being in the world, 1950–1990. Cambridge University Press.
Pritchett, Lant, and Lawrence Summers. 1996. Wealthier Is Healthier. Journal of Human Resources 31 (4): 841–868.
Rajaratnam, Julie Knoll, Jake R. Marcus, Alison Levin-Rector, Andrew N. Chalupka, Haidong Wang, Laura Dwyer, Megan Costa, Alan D. Lopez, and Christopher JL Murray. 2010. Worldwide mortality in men and women aged 15–59 years from 1970 to 2010: a systematic analysis. The Lancet 375(9727):1704–1720.
Raymond, Susan U., Henry M. Greenberg, and Stephen R. Leeder. 2005. Beyond reproduction: Women’s health in today’s develo** world. International Journal of Epidemiology 34 (5): 1144–1148.
Read, Jen'nan Ghazal, and Bridget Gorman. 2010. Gender and health inequality. Annual review of sociology 36:371–386.
Reeves, Aaron, and Johan Mackenbach. 2019. Can inequalities in political participation explain health inequalities? Social Science & Medicine 234: 112371.
Rich, Jessica. 2019. State-Sponsored Activism: Bureaucrats and Social Movements in Democratic Brazil. Cambridge University Press.
Rodriguez, Javier. 2018. Health disparities, politics, and the maintenance of the status quo: A new theory of inequality. Social Science & Medicine 200: 36–43.
Rodriguez, Javier, John Bound, and Arline Geronimus. 2014. US infant mortality and the President’s party. International Journal of Epidemiology 43 (3): 818–826.
Rodriguez, Javier, Arline T. Geronimus, John Bound, and Danny Dorling. 2015. Black lives matter: Differential mortality and the racial composition of the US electorate, 1970–2004. Social Science & Medicine 136: 193–199.
Rodríguez, Javier, Byengseon Bae, Arline Geronimus, and John Bound. 2022. The Political Realignment of Health: How Partisan Power Shaped Infant Health in the United States, 1915–2017. Journal of Health Politics, Policy and Law 47 (2): 201–224.
Roser, Max and Hannah Ritchie. 2013. Maternal Mortality. Published online at OurWorldInData.org. Accessed Aug 2022.
Ross, Michael. 2006. Is democracy good for the poor? American Journal of Political Science 50 (4): 860–874.
Sasson, Isaac. 2016. Trends in life expectancy and lifespan variation by educational attainment: United States, 1990–2010. Demography 53 (2): 269–293.
Scholz, John. 1991. Cooperative regulatory enforcement and the politics of administrative effectiveness. American Political Science Review 85 (1): 115–136.
Shandra, John, Jenna Nobles, Bruce London, and John Williamson. 2004. Dependency, democracy, and infant mortality: A quantitative, cross-national analysis of less developed countries. Social Science & Medicine 59 (2): 321–333.
Shandra, John, Carrie Shandra, and Bruce London. 2010. Do non-governmental organizations impact health? A cross-national analysis of infant mortality. International Journal of Comparative Sociology 51 (1–2): 137–164.
Singh-Manoux, Archana, Alice Guéguen, Jane Ferrie, Martin Shipley, Pekka Martikainen, Sébastien. Bonenfant, Marcel Goldberg, and Michael Marmot. 2008. Gender differences in the association between morbidity and mortality among middle-aged men and women. American Journal of Public Health 98 (12): 2251–2257.
Son, Byunghwan, and Nisha Bellinger. 2022. The Health Cost of Autocratization. Journal of Development Studies 58 (5): 873–890.
Stasavage, David. 2005. Democracy and education spending in Africa. American Journal of Political Science 49 (2): 343–358.
Tuljapurkar, Shripad. 2010. The final inequality: Variance in age at death. NBER Chapters. In Demography and the Economy, 209–221.
Teorell, Jan, Aksel Sundström, Sören Holmberg, Bo Rothstein, Natalia Alvarado Pachon and Cem Mert Dalli. 2021. Quality of government standard dataset v2021.
Vallin, Jacques, and France Meslé. 2010. Will life expectancy increase indefinitely by three months every year? Population Societies 473 (11): 1–4.
Vanhanen, Tatu. 2019. Measures of democracy 1810–2018 . Version 8.0.
van Raalte, Alyson, Anton Kunst, Patrick Deboosere, Mall Leinsalu, Olle Lundberg, Pekka Martikainen, Bjørn Heine Strand, Barbara Artnik, Bogdan Wojtyniak, and Johan P. Mackenbach. 2011. More variation in lifespan in lower educated groups: evidence from 10 European countries. International journal of epidemiology 40(6):1703–1714.
Vaupel, James W., Zhen Zhang, and Alyson A. van Raalte. 2011. Life expectancy and disparity: an international comparison of life table data. BMJ Open 1(1):e000128.
Waldner, David, and Ellen Lust. 2018. Unwelcome change: Coming to terms with democratic backsliding. Annual Review of Political Science 21 (1): 93–113.
Wamai, Richard. 2014. Civil society’s response to the HIV/AIDS crisis in Africa. In The handbook of civil society in Africa, 361–398.
Wang, Guang-zhen. 2014. The impact of social and economic indicators on maternal and child health. Social Indicators Research 116: 935–957.
Wang, Yi.-ting, Valeriya Mechkova, and Frida Andersson. 2019. Does democracy enhance health? New empirical evidence 1900–2012. Political Research Quarterly 72 (3): 554–569.
Wang, Haidong, Mohsen Naghavi, Christine Allen, Ryan M. Barber, Zulfiqar A. Bhutta, Austin Carter, Daniel C. Casey et al. 2016. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet 388(10053):1459–1544.
Weil, David. 2014. Health and Economic Growth. Handbook of Economic Growth. 2: 623–682.
Wejnert, Barbara. 2008. Effects of global democracy on women’s reproductive health: 1970–2005, Cross-world analysis. Marriage & Family Review 44 (2–3): 154–172.
Well, David. 2007. Accounting for the effect of health on economic growth. Quarterly Journal of Economics 122 (3): 1265–1306.
Wigley, Simon, and Arzu Akkoyunlu-Wigley. 2011. The impact of regime type on health: Does redistribution explain everything? World Politics 63 (4): 647–677.
Wigley, Simon, and Arzu Akkoyunlu-Wigley. 2017. The impact of democracy and media freedom on under-5 mortality, 1961–2011. Social Science & Medicine 190: 237–246.
Wilmoth, John R. 2007. Human longevity in historical perspective. In Physiological Basis of Aging and Geriatrics, edited by Paola S. Timiras, 4th ed. New York: Informa.
Wilmoth, John, and Shiro Horiuchi. 1999. Rectangularization revisited: Variability of age at death within human populations. Demography 36 (4): 475–495.
Winslow, Margrethe. 2005. Is democracy good for the environment? Journal of Environmental Planning and Management 48 (5): 771–783.
World Bank. n.d. World development indicators. Washington: World Bank.
World Bank. Wolde, Dereje K., and Tariq Khokhar. 2016. How do causes of death vary between men and women? World Bank Blogs.
World Bank. Suzuki, Emi, Kouame, Charles and Mills, Samuel. 2023. Progress in reducing maternal mortality has stagnated and we are not on track to achieve the SDG target: New UN Report. The World Bank Blogs.
World Health Organization. 2015. Global Health Observatory Data.
World Health Organization. 2022. Child Mortality (under 5 Years). https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-child-under-5-mortality-in-2020. Accessed Aug 2022.
World Health Organization Commission on Social Determinants of Health. 2007. Civil Society Report.
Funding
Open access funding provided by SCELC, Statewide California Electronic Library Consortium
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Salazar, A.O., Rodríguez, J., Salayeva, R. et al. Does Democracy Matter for Lifespan Inequalities? Regime Type and Premature Mortality by Sex. St Comp Int Dev 58, 511–537 (2023). https://doi.org/10.1007/s12116-023-09407-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12116-023-09407-x