
Abstract
Introduction
Fibroblast growth factor receptor (FGFR)-4/FGF19 pathway dysregulation is implicated in hepatobiliary and other solid tumors. INCB062079, an oral, selective, FGFR4 inhibitor, inhibits growth in FGF19/FGFR4-driven liver cancer models.
Methods
This was a two-part, phase I study (NCT03144661) in previously treated patients with advanced solid tumors. The primary objective was to determine safety, tolerability, and maximum tolerated dose (MTD), while secondary objectives included pharmacokinetics, pharmacodynamics (plasma FGF19; bile acid salts/7α-hydroxy-4-cholesten-3-one [C4] levels), and preliminary efficacy. In Part 1, patients received INCB062079 starting at 10 mg once daily, with 3 + 3 dose escalation. Part 2 (dose expansion) was not conducted because of study termination.
Results
Twenty-three patients were treated (hepatobiliary, n = 11; ovarian, n = 9; other, n = 3). Among six patients receiving 15 mg twice daily, two patients had dose-limiting toxicities (DLTs; grade 3 diarrhea, grade 3 transaminitis). Both had high pretreatment C4 concentrations, prompting a protocol amendment requiring pretreatment C4 concentrations < 40.9 ng/mL and concomitant prophylactic bile acid sequestrant treatment. No additional DLTs were reported at 10 and 15 mg twice daily; higher doses were not assessed. The most common toxicity was diarrhea (60.9%). INCB062079 exposure was dose-proportional; FGF19 and bile acid/C4 concentrations increased with exposure. One partial response was achieved (15 mg twice daily; ovarian cancer; FGF/FGFR status unknown; duration of response, 7.5 months); two patients had stable disease.
Conclusions
With C4 cut-off and prophylactic bile acid sequestrant implementation, INCB062079 demonstrated a manageable safety profile and evidence of target inhibition. In view of the rarity of FGF19/FGFR4 alterations and slow patient accrual, the study was terminated before establishing an MTD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In this phase I study of INCB062079 for previously treated advanced solid tumors, INCB062079 demonstrated a manageable safety profile, generally dose-proportional pharmacokinetics, and pharmacodynamics consistent with target inhibition. |
Because of slow patient accrual, the study was terminated before a maximum tolerated dose of INCB062079 could be identified, and clinical development was terminated. |
Nevertheless, the results validate INCB062079 as a clinical grade fibroblast growth factor receptor-4 inhibitor and support future research into the relevance of the FGF19/FGFR4 signaling axis as a therapeutic target in solid tumors. |
1 Introduction
Fibroblast growth factor (FGF)-19 is an endocrine factor produced by the ileum in response to postprandial luminal bile salts [1,2,3]. In the liver, FGF19 binds to FGF receptor (FGFR)-4, and the co-receptor βklotho, thereby regulating both bile salt formation and hepatocyte proliferation [3,4,5]. Under physiologic conditions, FGF19 and its receptors are thought to play a critical role in protecting against cholestatic liver injury [1].
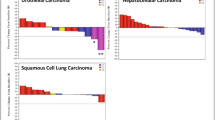
Emerging evidence indicates that dysregulation of the FGF19/FGFR4 signaling axis contributes to oncogenesis in hepatocellular carcinoma (HCC) and several other solid tumors [6,7,8]. In clinical HCC samples, FGF19 is genomically amplified in the context of an 11q13 amplicon in approximately 5% of tumors [4a, b). One of the two patients achieving stable disease had advanced HCC and unknown FGF19 status, and had progressed on sorafenib before study enrollment. This patient, who received INCB062079 10 mg once daily, achieved stable disease without progression for 31.3 months. The other patient achieving stable disease had intrahepatic cholangiocarcinoma with no reported FGF19 status and had been previously treated with surgery, radiation, and five lines of systemic therapy. This patient received INCB062079 10 mg twice daily and achieved stable disease without progression for 4.9 months.

a Waterfall plot of best percentage change in the sum of target lesions for individual patients receiving INCB062079 (efficacy-evaluable population). Data were from investigator review per standard RECIST v1.1 and modified RECIST for hepatocellular carcinoma, and response was unconfirmed. b Duration of treatment and response assessments among individual patients receiving INCB062079. aThis patient had cholangiocarcinoma and FGF3, FGF4, and FGF19 amplifications. bThis patient had esophageal cancer and FGF3, FGF4, FGF10, and FGF19 amplifications, and an FGFR4 p.S551F mutation. cThis patient had ovarian cancer. dPatients were enrolled after a protocol amendment requiring all newly enrolled patients to have a C4 concentration < 40.9 ng/mL and to take a prophylactic bile acid sequestrant for the prevention of diarrhea while receiving INCB062079 treatment. BID twice daily, C4 7α-hydroxy-4-cholesten-3-one, GE gastroesophageal, NE not evaluable, PD progressive disease, PR partial response, QD once daily, RECIST Response Evaluation Criteria in Solid Tumors, SD stable disease
4 Discussion
Dysregulation of FGF19/FGFR4/βklotho-mediated signal transduction through the MAPK, PI3K/AKT/mTOR, JAK-STAT, NFκB, and Wnt/β-catenin pathways can result in uncontrolled cellular growth in preclinical models of HCC [6, 8, 28]. Whereas this oncogenic mechanism is highly relevant to hepatobiliary cancers, dysregulation of the FGF19/FGFR4/βklotho signaling axis has also been observed in other solid tumors [6,7,8]. We therefore evaluated INCB062079, a potent, oral, irreversible inhibitor of FGFR4, in patients with solid tumors, including hepatobiliary cancers, in the context of a first-in-human clinical trial. Manageable on-target gastrointestinal toxicity was observed in most patients at the initial dosages. However, dose escalation beyond 15 mg twice daily was not possible because two of six patients experienced gastrointestinal/hepatobiliary DLTs. The protocol was subsequently amended to include eligibility criteria that mitigated this toxicity by requiring the prophylactic use of bile acid sequestrants and a pretreatment serum C4 concentration cut-off < 40.9 ng/mL. This amendment resulted in an apparent blunting of toxicity allowing successful dose escalation. Importantly, the generally dose-proportional PK of INCB062079 was associated with an expected increase in plasma C4 and FGF19 concentrations, consistent with target inhibition of FGFR4 in vivo. A partial response was observed at the highest dose levels tested (15 mg twice daily), indicating a signal of antitumor activity. Despite these findings, because of the rarity of FGF19/FGFR4 alterations and the slow accrual of patients who satisfied the eligibility criteria, the study was terminated before the MTD could be identified, and the clinical development of INCB062079 was terminated.
Increasing postprandial luminal bile salt concentrations result in exocrine farnesoid X receptor (FXR)-induced production of FGF19 by enterocytes, which serves to activate FGFR4/βklotho-mediated signaling in hepatocytes and cholangiocytes [27, 29]. Under normal physiologic conditions, FGF19/FGFR4/βklotho signal activation suppresses bile acid biosynthesis in hepatocytes by downregulating the CYP7A1 gene [3, 4, 8] via SHP/liver receptor homolog-1 (LRH-1)-dependent [30, 31] and JNK-dependent [4] feedback mechanisms. Consistent with this, FGFR4 inhibition was associated with increased CYP7A1 RNA expression and bile salt excretion in cynomolgus monkeys [21]. Furthermore, in murine models, knocking out FGFR4 or βklotho leads to elevated bile acid excretion and an increased bile acid pool [5, 32]. Moreover, βklotho–/– mice have been shown to display phenotypic characteristics suggestive of early-stage liver damage, including increased liver size, increased ALT and AST levels, increased proinflammatory cytokine expression, and fibrogenesis [33]. It was further demonstrated that these characteristics were associated with a large increase in microbiota-derived deoxycholic acid [33]. Given the potential toxicity of excessive bile salt accumulation [33], the expected on-target gastrointestinal and hepatobiliary toxicity of selective FGFR4 inhibitors must be scrutinized and mitigated to ensure an adequate therapeutic index of this drug class. The observed safety profile of INCB062079 was consistent with its proposed mechanism of action, with manageable any-grade diarrhea (60.9%), nausea (47.8%), vomiting (26.1%), and AST and ALT increases (17.4 and 13.0%, respectively). Such on-target effects were also observed in 106 patients with advanced HCC receiving the selective FGFR4 inhibitor fisogatinib in a recent phase I study [7], which reported treatment-related adverse events of diarrhea (any-grade 74%; grade 3 or higher, 8%), nausea (42%; 2%), and vomiting (35%; 4%). Treatment-related grade 3 or higher ALT and AST increase adverse events were also observed in 11% and 15%, respectively, of patients treated with fisogatinib [7]. Because this class of drug has greatest applicability in hepatobiliary cancers, the potential liability of on-target FGFR4 toxicity and need for mitigation efforts are of clear importance.
Without mitigation efforts, the INCB062079 dose could not be escalated without intolerable dose-limiting gastrointestinal toxicity in patients, indicative of a narrow therapeutic index. For this reason, efforts were made to select patients with low baseline plasma C4 expression and prophylactically treat with bile acid sequestrants. Preclinical toxicology data indicate that bile acid sequestration is a novel method to prevent FGFR4-induced hepatic and gastrointestinal toxicity [34, 35]. Although the patient sample sizes in the present study are too small to draw conclusions, diarrhea was reported by a smaller percentage of patients who received concurrent prophylactic treatment with a bile acid sequestrant (Cohorts 4 and 5), compared with patients who did not receive such treatment. Bile acid sequestrant treatment may therefore have merit as a clinical strategy to blunt gastrointestinal toxicity associated with FGFR4 inhibition and should be explored in future studies.
Importantly, INCB062079 exhibited linear exposure relative to dose and did not accumulate with repeat dosing. The addition of bile acid sequestrant did not appear to interfere with absorption or reduce INCB062079 exposure. PK/PD modeling did indicate a statistically significant increase in bile salt and C4 concentrations with increasing INCB062079 exposure and a two- to four-fold increase in FGF19 concentrations with repeat dosing. These findings suggest that INCB062079 inhibits its proposed target, further supporting INCB062079 as a clinical grade FGFR4 inhibitor. FGF19/FGFR4/βklotho pathway inhibition by INCB062079 in tumor tissues could not be confirmed because paired pretreatment and on-treatment biopsies were not obtained in this study (per protocol).
Determination of antitumor activity was not a primary objective of this phase I study and could not be satisfactorily assessed given that higher INCB062079 doses were not tested. Interestingly, a partial response was seen in a patient with ovarian cancer with unknown FGF19/FGFR status. In addition, long-term stable disease was observed in a patient with HCC treated with INCB062079 (31.3 months). This observation is in kee** with previous findings with fisogatinib, where eight patients with HCC achieved either partial or complete responses lasting over 6 months [7]. Taken together, these observations are hypothesis-generating and support further investigation of the efficacy and safety of selective FGFR4 inhibitors in patients with advanced HCC and other solid tumors. No correlation was established between potential biomarkers and clinical efficacy; the two patients with known FGF19 amplifications did not respond to study treatment. Other selective FGFR4 inhibitors currently in phase I/II clinical trials for HCC or other advanced solid tumors as monotherapy or in combination with other anticancer agents include roblitinib (FGF401) [22] (NCT02325739), EVER4010001 (NCT04699643), ABSK-011 [36] (NCT04906434), and H3B-6527 [37] (NCT02834780). Together, these studies will help clarify the merit of selective FGFR4 inhibitor treatments in patients with solid tumors.
Limitations of the study include a lack of pretreatment data on the types of FGF19/FGFR4 alterations, including fusions or other rearrangements, mutations, amplifications, as well as FGF19 protein overexpression. In addition, FGFR4/FGF19 genomic testing data were missing in 52.2% of patients in the dose-escalation cohort; however, this reflects the design of Part 1, which enrolled patients regardless of FGFR4/FGF19 alteration status. Expansion cohorts had been planned for these analyses to explore the predictive and prognostic significance of FGF19 and FGFR4 alterations on patient outcome. Importantly, inclusion of other histology/tumor types led to hypothesis-generating clinical observations that would have been explored in the planned expansion cohorts. For example, the only partial responder in the present study had heavily pretreated ovarian cancer. Recent retrospective and translational analyses indicate that FGFR4 overexpression is associated with a worse outcome in advanced ovarian cancer, and that blockade of ligand-dependent FGFR4 activation is deleterious to ovarian cancer cell growth in vitro and in vivo [13]. Finally, although only a minority of patients had C4 concentrations exceeding the C4 concentration cut-off initiated with the protocol amendment, this additional eligibility criterion served to slow accrual and thus further narrowed a pool of patients with an already infrequent FGF19/FGFR4 variant. Indeed, the C4 threshold was established based on a limited sample size using an assay not certified by the Clinical Laboratory Improvement Amendments (CLIA) while the study was ongoing, without statistical power for robust analysis. In retrospect, C4 levels should be embedded as an integrated biomarker of toxicity. Nevertheless, the data presented herein help to credential INCB062079 as a bona fide clinical grade inhibitor of FGFR4, provide useful information for future drug development of agents blocking FGFR4, and support continued investigation to determine the relevance of the FGF19/FGFR4 axis as a target in solid tumors.
References
Luo J, Ko B, Elliott M, Zhou M, Lindhout DA, Phung V, et al. A nontumorigenic variant of FGF19 treats cholestatic liver diseases. Sci Transl Med. 2014;6:247ra100. https://doi.org/10.1126/scitranslmed.3009098.
Inagaki T, Choi M, Moschetta A, Peng L, Cummins CL, McDonald JG, et al. Fibroblast growth factor 15 functions as an enterohepatic signal to regulate bile acid homeostasis. Cell Metab. 2005;2:217–25. https://doi.org/10.1016/j.cmet.2005.09.001.
Lundasen T, Galman C, Angelin B, Rudling M. Circulating intestinal fibroblast growth factor 19 has a pronounced diurnal variation and modulates hepatic bile acid synthesis in man. J Intern Med. 2006;260:530–6. https://doi.org/10.1111/j.1365-2796.2006.01731.x.
Holt JA, Luo G, Billin AN, Bisi J, McNeill YY, Kozarsky KF, et al. Definition of a novel growth factor-dependent signal cascade for the suppression of bile acid biosynthesis. Genes Dev. 2003;17:1581–91. https://doi.org/10.1101/gad.1083503.
Ito S, Fujimori T, Furuya A, Satoh J, Nabeshima Y, Nabeshima Y. Impaired negative feedback suppression of bile acid synthesis in mice lacking βKlotho. J Clin Invest. 2005;115:2202–8. https://doi.org/10.1172/JCI23076.
Prieto-Dominguez N, Shull AY, Teng Y. Making way for suppressing the FGF19/FGFR4 axis in cancer. Future Med Chem. 2018;10:2457–70. https://doi.org/10.4155/fmc-2018-0099.
Kim RD, Sarker D, Meyer T, Yau T, Macarulla T, Park JW, et al. First-in-human phase I study of fisogatinib (BLU-554) validates aberrant FGF19 signaling as a driver event in hepatocellular carcinoma. Cancer Discov. 2019;9:1696–707. https://doi.org/10.1158/2159-8290.CD-19-0555.
Levine KM, Ding K, Chen L, Oesterreich S. FGFR4: a promising therapeutic target for breast cancer and other solid tumors. Pharmacol Ther. 2020;214: 107590. https://doi.org/10.1016/j.pharmthera.2020.107590.
Wang K, Lim HY, Shi S, Lee J, Deng S, **e T, et al. Genomic landscape of copy number aberrations enables the identification of oncogenic drivers in hepatocellular carcinoma. Hepatology. 2013;58:706–17. https://doi.org/10.1002/hep.26402.
Schulze K, Imbeaud S, Letouze E, Alexandrov LB, Calderaro J, Rebouissou S, et al. Exome sequencing of hepatocellular carcinomas identifies new mutational signatures and potential therapeutic targets. Nat Genet. 2015;47:505–11. https://doi.org/10.1038/ng.3252.
Shi S, Li X, You B, Shan Y, Cao X, You Y. High expression of FGFR4 enhances tumor growth and metastasis in nasopharyngeal carcinoma. J Cancer. 2015;6:1245–54. https://doi.org/10.7150/jca.12825.
Gao L, Lang L, Zhao X, Shay C, Shull AY, Teng Y. FGF19 amplification reveals an oncogenic dependency upon autocrine FGF19/FGFR4 signaling in head and neck squamous cell carcinoma. Oncogene. 2019;38:2394–404. https://doi.org/10.1038/s41388-018-0591-7.
Zaid TM, Yeung TL, Thompson MS, Leung CS, Harding T, Co NN, et al. Identification of FGFR4 as a potential therapeutic target for advanced-stage, high-grade serous ovarian cancer. Clin Cancer Res. 2013;19:809–20. https://doi.org/10.1158/1078-0432.CCR-12-2736.
Xu YF, Yang XQ, Lu XF, Guo S, Liu Y, Iqbal M, et al. Fibroblast growth factor receptor 4 promotes progression and correlates to poor prognosis in cholangiocarcinoma. Biochem Biophys Res Commun. 2014;446:54–60. https://doi.org/10.1016/j.bbrc.2014.02.050.
Khan J, Wei JS, Ringner M, Saal LH, Ladanyi M, Westermann F, et al. Classification and diagnostic prediction of cancers using gene expression profiling and artificial neural networks. Nat Med. 2001;7:673–9. https://doi.org/10.1038/89044.
Hagel M, Miduturu C, Sheets M, Rubin N, Weng W, Stransky N, et al. First selective small molecule inhibitor of FGFR4 for the treatment of hepatocellular carcinomas with an activated FGFR4 signaling pathway. Cancer Discov. 2015;5:424–37. https://doi.org/10.1158/2159-8290.CD-14-1029.
Joshi JJ, Coffey H, Corcoran E, Tsai J, Huang CL, Ichikawa K, et al. H3B–6527 is a potent and selective inhibitor of FGFR4 in FGF19-driven hepatocellular carcinoma. Cancer Res. 2017;77:6999–7013. https://doi.org/10.1158/0008-5472.CAN-17-1865.
Sawey ET, Chanrion M, Cai C, Wu G, Zhang J, Zender L, et al. Identification of a therapeutic strategy targeting amplified FGF19 in liver cancer by oncogenomic screening. Cancer Cell. 2011;19:347–58. https://doi.org/10.1016/j.ccr.2011.01.040.
French DM, Lin BC, Wang M, Adams C, Shek T, Hotzel K, et al. Targeting FGFR4 inhibits hepatocellular carcinoma in preclinical mouse models. PLoS ONE. 2012;7: e36713. https://doi.org/10.1371/journal.pone.0036713.
Liu PCC, Lu L, Bowman K, Stubbs MC, Wu L, DiMatteo D, et al. Selective inhibition of FGFR4 by INCB062079 is efficacious in models of FGF19- and FGFR4-dependent cancers [abstract]. Cancer Res. 2017;77:2100. https://doi.org/10.1158/1538-7445.Am2017-2100.
Ruggeri B, Stubbs M, Yang Y-O, Juvekar A, Lu L, Condon S, et al. The novel FGFR4-selective inhibitor INCB062079 is efficacious in models of hepatocellular carcinoma harboring FGF19 amplification [abstract]. Cancer Res. 2017;77:1234. https://doi.org/10.1158/1538-7445.Am2017-1234.
Weiss A, Adler F, Buhles A, Stamm C, Fairhurst RA, Kiffe M, et al. FGF401, a first-in-class highly selective and potent FGFR4 inhibitor for the treatment of FGF19-driven hepatocellular cancer. Mol Cancer Ther. 2019;18:2194–206. https://doi.org/10.1158/1535-7163.MCT-18-1291.
US Food and Drug Administration. Estimating the maximum safe starting dose in initial clinical trials for therapeutics in adult healthy volunteers. Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/estimating-maximum-safe-starting-dose-initial-clinical-trials-therapeutics-adult-healthy-volunteers. Accessed 29 Oct 2021.
Scaldaferri F, Pizzoferrato M, Ponziani FR, Gasbarrini G, Gasbarrini A. Use and indications of cholestyramine and bile acid sequestrants. Intern Emerg Med. 2013;8:205–10. https://doi.org/10.1007/s11739-011-0653-0.
Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30:52–60. https://doi.org/10.1055/s-0030-1247132.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–47. https://doi.org/10.1016/j.ejca.2008.10.026.
Jung D, York JP, Wang L, Yang C, Zhang A, Francis HL, et al. FXR-induced secretion of FGF15/19 inhibits CYP27 expression in cholangiocytes through p38 kinase pathway. Pflugers Arch. 2014;466:1011–9. https://doi.org/10.1007/s00424-013-1364-3.
Chen Z, Jiang L, Liang L, Koral K, Zhang Q, Zhao L, et al. The role of fibroblast growth factor 19 in hepatocellular carcinoma. Am J Pathol. 2021;191:1180–92. https://doi.org/10.1016/j.ajpath.2021.04.014.
Kliewer SA, Mangelsdorf DJ. Bile acids as hormones: the FXR-FGF15/19 pathway. Dig Dis. 2015;33:327–31. https://doi.org/10.1159/000371670.
Goodwin B, Jones SA, Price RR, Watson MA, McKee DD, Moore LB, et al. A regulatory cascade of the nuclear receptors FXR, SHP-1, and LRH-1 represses bile acid biosynthesis. Mol Cell. 2000;6:517–26. https://doi.org/10.1016/s1097-2765(00)00051-4.
Lu TT, Makishima M, Repa JJ, Schoonjans K, Kerr TA, Auwerx J, et al. Molecular basis for feedback regulation of bile acid synthesis by nuclear receptors. Mol Cell. 2000;6:507–15. https://doi.org/10.1016/s1097-2765(00)00050-2.
Yu C, Wang F, Kan M, ** C, Jones RB, Weinstein M, et al. Elevated cholesterol metabolism and bile acid synthesis in mice lacking membrane tyrosine kinase receptor FGFR4. J Biol Chem. 2000;275:15482–9. https://doi.org/10.1074/jbc.275.20.15482.
Somm E, Henry H, Bruce SJ, Bonnet N, Montandon SA, Niederländer NJ, et al. β-Klotho deficiency shifts the gut-liver bile acid axis and induces hepatic alterations in mice. Am J Physiol Endocrinol Metab. 2018;315:E833–47. https://doi.org/10.1152/ajpendo.00182.2018.
Bartz R, Fukuchi K, Ohtsuka T, Lange T, Gruner K, Watanabe I, et al. Preclinical development of U3–1784, a novel FGFR4 antibody against cancer, and avoidance of its on-target toxicity. Mol Cancer Ther. 2019;18:1832–43. https://doi.org/10.1158/1535-7163.MCT-18-0048.
Schadt HS, Wolf A, Mahl JA, Wuersch K, Couttet P, Schwald M, et al. Bile acid sequestration by cholestyramine mitigates FGFR4 inhibition-induced ALT elevation. Toxicol Sci. 2018;163:265–78. https://doi.org/10.1093/toxsci/kfy031.
Chen Z. Discovery and characterization of a novel FGFR4 Inhibitor for the treatment of hepatocellular carcinoma [abstract]. Cancer Res. 2018;78:LB-272. https://doi.org/10.1158/1538-7445.Am2018-lb-272.
Macarulla T, Moreno V, Chen LT, Sawyer MB, Goyal L, Muñoz Martín AJ, et al. Phase I study of H3B–6527 in hepatocellular carcinoma (HCC) or intrahepatic cholangiocarcinoma (ICC). J Clin Oncol. 2021;39:4090. https://doi.org/10.1200/JCO.2021.39.15_suppl.4090.
Acknowledgements
The authors thank the patients and families, investigators, and site personnel who participated in this study. This study was sponsored by Incyte Corporation (Wilmington, DE, USA). Medical writing assistance was provided by Simon J. Slater, PhD, CMPP, of Envision Pharma Group (Philadelphia, PA, USA), and funded by Incyte Corporation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This research was funded by Incyte Corporation and, in part, through the NIH/NCI Cancer Center Support Grant P30 CA008748 (JJH).
Conflict of interest
James J. Harding: Consulting or advisory role for Adaptimmune, Bristol Myers Squibb, CytomX, Eisai, Eli Lilly & Company, Exelixis, Imvax, Merck, Zymeworks; and research funding from Boehringer Ingelheim (Inst), Bristol Myers Squibb (Inst), Calithera Biosciences (Inst), Debiopharm (Inst), Eli Lilly & Company (Inst), Incyte Corporation (Inst), Novartis (Inst), Pfizer (Inst), Polaris Group (Inst), Yiviva (Inst), and Zymeworks (Inst). Christiane Jungels: Travel, accommodations, and expenses from Ipsen, PharmaMar. Jean-Pascal Machiels: Consulting or advisory role for ALX Oncology, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, CUE Biopharma, Debiopharm, Incyte Corporation, Innate Pharma, Janssen, Merck Serono, Merck Sharp & Dohme, Nanobiotix, Novartis, Pfizer, Roche; research funding from Bayer, Janssen, Novartis, Sanofi; and travel, accommodations, and expenses from Amgen, Bristol Myers Squibb, Merck Sharp & Dohme, and Pfizer. David C. Smith: Research funding from Agensys (Inst), Atterocor (Inst), Bayer (Inst), Boston Biomedical (Inst), Bristol Myers Squibb/Medarex (Inst), Celgene (Inst), Eli Lilly & Company (Inst), ESSA (Inst), Exelixis (Inst), Genentech (Inst), ImClone Systems (Inst), Incyte Corporation (Inst), MedImmune (Inst), Medivation/Astellas Pharma (Inst), Millennium Pharmaceuticals (Inst), Novartis (Inst), OncoGenex (Inst), OncoMed Pharmaceuticals (Inst), Regeneron (Inst), SeaGen (Inst), Takeda (Inst), Tekmira Pharmaceuticals (Inst), and Teva Pharmaceuticals (Inst). Chris Walker, Tao Ji, Pin Jiang: Former employees of Incyte Corporation. Ekaterine Asatiani, **n Li: Employment by, and stock ownership in, Incyte Corporation. Eric Van Cutsem: Consulting or advisory role for Array BioPharma, AstraZeneca, Bayer, Biocartis, Bristol Myers Squibb, Celgene, Daiichi Sankyo, Eli Lilly & Company, GlaxoSmithKline, Halozyme, Incyte Corporation, Merck KGaA, Merck Sharp & Dohme, Novartis, Pierre Fabre, Roche, Servier, Sirtex Medical, and Taiho Pharmaceutical Co., Ltd; and research funding from Amgen (Inst), Bayer (Inst), Boehringer Ingelheim (Inst), Bristol Myers Squibb (Inst), Celgene (Inst), Eli Lilly & Company (Inst), Ipsen (Inst), Merck (Inst), Merck KGaA (Inst), Novartis (Inst), Roche (Inst), and Servier (Inst). Ghassan K. Abou-Alfa: Research grants from Arcus, AstraZeneca, BioNtech, Bristol Myers Squibb, Celgene, Flatiron Health, Genentech/Roche, Genoscience Pharma, Incyte Corporation, Polaris Group, Puma Biotechnology, QED Therapeutics, Silenseed, Yiviva; and consultancy with Adicet Bio, Alnylam Pharmaceuticals, AstraZeneca, Autem Therapeutics, BeiGene, Berry Genomics, Boehringer Ingelheim, Celgene, Cend Therapeutics, CytomX, Eisai, Eli Lilly & Company, Exelixis, Flatiron Health, Genentech/Roche, Genoscience Pharma, Helios Pharmaceuticals, Helsinn Group, Incyte Corporation, Ipsen, Merck, Nerviano Medical Sciences, NewBridge Pharmaceuticals, Novartis, QED Therapeutics, Redhill, Rafael Pharmaceuticals, Servier, Silenseed, Sobi, Vector Pharma, and Yiviva.
Availability of data and material
Incyte Corporation (Wilmington, DE, USA) is committed to data sharing that advances science and medicine while protecting patient privacy. Qualified external scientific researchers may request anonymized datasets owned by Incyte for the purpose of conducting legitimate scientific research. Researchers may request anonymized datasets from any interventional study (except phase I studies) for which the product and indication have been approved on or after 1 January 2020 in at least one major market (e.g., United States, European Union, Japan). Data will be available for request after the primary publication or 2 years after the study has ended. Information on Incyte’s clinical trial data sharing policy and instructions for submitting clinical trial data requests are available at: https://www.incyte.com/Portals/0/Assets/Compliance%20and%20Transparency/clinical-trial-data-sharing.pdf?ver=2020-05-21-132838-960.
Ethics approval
The study, registered under ClinicalTrials.gov (NCT03144661), was performed in accordance with the International Conference for Harmonization Good Clinical Practice guidelines, the Declaration of Helsinki, and applicable local regulations with approval from institutional review boards. The study protocol was reviewed and approved by the respective institutional review boards of the participating institutions (Online Supplementary Table 1).
Consent to participate
Written informed consent was obtained for all patients before performing study-related procedures.
Consent for publication
Not applicable.
Code availability
Not applicable.
Author contributions
All authors were responsible for data collection, data integrity and analyses, and data interpretation, and reviewed and edited the manuscript. The corresponding author wrote the initial draft manuscript, had full access to all study data, and had final responsibility for the decision to submit for publication.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Harding, J.J., Jungels, C., Machiels, JP. et al. First-in-Human Study of INCB062079, a Fibroblast Growth Factor Receptor 4 Inhibitor, in Patients with Advanced Solid Tumors. Targ Oncol 18, 181–193 (2023). https://doi.org/10.1007/s11523-023-00948-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11523-023-00948-8