
Abstract
Fulminant myocarditis (FM) may lead to cardiogenic shock requiring veno-arterial extracorporeal membrane oxygenation (VA-ECMO). Results of effectiveness studies of VA-ECMO have been contradictory. We evaluated the aggregate short-term mortality after VA-ECMO and predictive factors in patients with FM. We systematically searched in electronic databases (February 2022) to identify studies evaluating short-term mortality (defined as mortality at 30 days or in-hospital) after VA-ECMO support for FM. We included studies with 5 or more patients published after 2009. We assessed the quality of the evidence using the QUIPS and GRADE tools. Mortality was pooled using random effect models. We performed meta-regression to explore heterogeneity based on a priori defined factors. We included 54 observational studies encompassing 2388 FM patients supported with VA-ECMO. Median age was 41 years (25th to 75th percentile 37–47), and 50% were female. The pooled short-term mortality was 35% (95% CI 29–40%, I2 = 69%; moderate certainty). By meta-regression, studies with younger populations showed lower mortality. Female sex, receiving a biopsy, cardiac arrest, left ventricular unloading, and earlier recruitment time frame, did not explain heterogeneity. These results remained consistent regardless of continent and the risk of bias category. In individual studies, low pH value, high lactate, absence of functional cardiac recovery on ECMO, increased burden of malignant arrhythmia, high peak coronary markers, and IVIG use were identified as independent predictors of mortality. When conventional therapies have failed, especially in younger patients, cardiopulmonary support with VA-ECMO should be considered in the treatment of severe FM.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fulminant myocarditis (FM) is a clinical manifestation of cardiac inflammation with rapid onset and severe hemodynamic compromise [1]. FM most often occurs after a viral infection [2], and it may progress rapidly to refractory cardiogenic shock (CS) and death. In refractory CS, early initiation of mechanical circulatory support (MCS) is a critical therapeutic option to rescue these patients [3,4,5]. Recent evidence [6] indicates that there is a rising trend in the utilization of MCS strategies such as veno-arterial extracorporeal membrane oxygenation (VA-ECMO), and the percutaneous ventricular assist devices (VAD) Impella and TandemHeart, whereas the usage of the intra-aortic balloon pump has declined. The success of MCS depends on adequate timing of initiation, pre-existing patient comorbidities, and severity of peripheral organ hypoperfusion. In recent years, VA-ECMO is often used as first-line MCS because it can be introduced quickly [1, 3, 7]. Other advantages of VA-ECMO include biventricular support, which is often needed in FM patients, and respiratory support through the use of an oxygenator to the circuit in patients with concomitant respiratory failure.
FM is often a reversible process, and VA-ECMO can be used as a bridge to recovery or less commonly heart transplantation (HTx) or durable VAD. Due to the significant cost and risks associated with VA-ECMO, such as failure or rupture of any part of the VA-ECMO circuit, as well as bleeding, thromboembolic, neurologic, vascular, and infectious complications [8], timely decision-making, refined patient selection, and the availability of an experienced team may favorably impact outcomes in patients supported with VA-ECMO. The conflicting results from previous published data with respect to short-term outcomes in FM patients on VA-ECMO is most likely a result of small sample size [3,4,5, 9,10,11] or single-center cohorts [3, 5, 11]. Thus, conducting a meta-analysis on aggregate study data may offer some benefit over individual study reports. Therefore, we sought to evaluate short-term mortality after VA-ECMO in patients with FM in a systematic review and meta-analysis.
Materials and methods
This study was conducted in accordance with the PRISMA statement for reporting on meta-analysis evaluating prognosis or diagnosis [12]. As this study is a systematic review and meta-analysis including aggregate data from studies already published, ethics approval was not required.
Data sources and searches
A comprehensive search strategy was developed for the two core concepts, myocarditis and ECMO. The initial search strategy was developed for Ovid Medline by using a combination of database-specific subject headings and text words. The search strategy was then customized for each database. Searches were executed on July 9, 2020, and repeated on February 10, 2022, in the following databases: Ovid MEDLINE, Ovid EMBASE, Cochrane CENTRAL (Ovid), and Cochrane Database of Systematic Reviews (Ovid). Limits were applied for humans, adults (≥ 18 years), and years 2009 to present. See Supplementary Appendix A for search strategies. Additional search methods included screening references of included studies.
Study selection
We included observational studies or post hoc analysis of randomized controlled trials on adult (≥ 18 years) patients with myocarditis, evaluating short-term mortality after VA-ECMO implantation, as well as any predictor associated with short-term mortality with univariable or multivariable analysis. Short-term mortality included 30-day mortality, death during index hospitalization, or death on ECMO. In the case of two studies reporting on the same cohort, we included studies with the larger population or both studies only if they reported on different predictors. There were no restrictions on language or publication status. We included abstracts if they provided sufficient information to characterize the population and short-term mortality. We restricted inclusion to studies with ≥ 5 patients published in 2009 or after, to represent more contemporary VA-ECMO strategies and patient management. Studies were excluded if they did not include patients who died within the first 24 h from their analysis, due to the risk of patient selection bias.
Using a study eligibility form (Supplementary Appendix B), independent reviewers selected citations by screening titles and abstracts in duplicate. Reviewers, independently and in duplicate, also screened the full texts of any citations deemed eligible during the title and abstract screening phase. In cases of disagreement, consensus was reached through discussion or participation of a third reviewer if deemed necessary.
Data abstraction
We abstracted data from eligible studies related to study and population characteristics (Supplementary Table S1 and Supplementary Table S2), as well as the number of deaths at different time points and follow up times allowing multiple mortality outcomes to be abstracted from one paper (Supplementary Table S2). In addition, we abstracted data on any predictor of mortality including their definition, effect estimate, and confidence interval. In studies reporting results from univariable and multivariable analyses, we abstracted the effect of a predictor reported in both univariable and multivariable regression models.
Risk of bias assessment
We performed risk of bias assessment for each included study using the Quality in Prognosis Studies (QUIPS) tool [13]. Given that the focus of our review was overall prognosis, we only appraised risk of bias based on methods of patient selection (consecutive or random patient selection), study attrition (complete follow-up), and outcome measurement. For each domain, we judged risk of bias as low, moderate, or high. If all domains were at low risk of bias, we judged the overall risk of bias to be low. If two or more domains were at high risk of bias, we judged the overall risk of bias to be high. For all other combinations, we judged the overall risk of bias to be moderate.
Certainty in the evidence
The Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) approach [14], assessing confidence in estimates across studies, was used to appraise our confidence in the pooled estimates from the gathered evidence. We assessed risk of bias at the outcome level considering risk of bias at the study level along with inconsistency, imprecision, indirectness, and reporting bias. We formally assessed publication bias with funnel plots at different stages in the analysis. We summarized confidence in estimates as high, moderate, low, or very low.
Data synthesis and statistical analysis
Study and population characteristics were summarized and reported using proportions (percentage) for categorical variables and median and 25th and 75th percentiles for continuous variables. To assess for overall risk of mortality, we pooled short-term mortality of the studies using an inverse variance method in a random-effects model reporting an overall pooled estimate with its respective 95% confidence interval (CI).
To evaluate for any potential regional variation in mortality, we grouped studies by continent and used meta-regression to evaluate differences in survival estimates across regions adjusted for the population mean age. Furthermore, to explore heterogeneity in mortality estimates across studies, we used univariable meta-regression evaluating the effect of average population age, proportion of females, patients with cardiac arrest, patients who received a biopsy or left ventricular (LV) unloading, as well as temporal variation based on first year of the recruitment time frame.
As all 7 predictors in multivariate models were reported only in 1 study or were defined differently according to study, the effect estimates could not be pooled together, and therefore were not meta-analyzed.
We used the same statistical plan described above to meta-analyze the overall risk of VAD or HTx after VA-ECMO implant, as well as ECMO complications, and explore heterogeneity using meta-regression. The results were provided as overall pooled estimates with their respective 95% CIs.
A two-sided p-value of 0.05 or lower was considered statistically significant. Stata 15.1’s metaprop and Review Manager 5 provided the statistical platform for the conduct of our meta-analysis.
Results
Study selection and patient characteristics
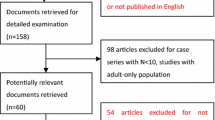
After screening 8070 citations, 54 studies (37 full text articles and 17 abstracts) comprising 2388 FM patients on VA-ECMO were included (Fig. 1; see Supplementary Appendix C for the 54 study references). Of these, all reported on short-term mortality, and only 3 studies reported on factors associated with mortality.

Study selection flow
Overall study demographics and clinical characteristics of FM patients treated with VA-ECMO are summarized in Table 1. The median sample size was 12 (25th to 75th percentile 7–27) patients, 43 (80%) of the studies were from single centers, and 40 (85%) of the studies were from Europe and Asia. The FM patient population had a median age of 41 (37–47) years, an equal distribution of sex, and a low burden of comorbidities (5 studies). Although a biopsy was taken to verify the diagnosis of FM in 12 studies (n = 243), only 9 studies (n = 133) explicitly included biopsy positivity, and the majority of these biopsy positive cases were categorized as lymphocytic myocarditis (65%). Cardiac arrest was observed in 465 (32%) patients (14 studies), and one-third of these occurred out of hospital. In 6 studies (n = 298), 56 (19%) patients received steroids. Co-management with LV unloading was seen in 314 (66%) patients (14 studies) whereof an intra-aortic balloon pump was most commonly used (n = 295 (60%), 14 studies). The median ECMO duration was 7.3 days (6.0–9.4 days; n = 465, 22 studies), and at discharge, the median ejection fraction was 49% (48–58%; n = 137, 5 studies).
Risk of bias of individual studies
All studies were retrospective cohort studies. For short-term mortality at 30 days or during index hospitalization, the risk of bias across studies was considered low in 18 (36%), moderate in 24 (48%), and high in 8 (16%; Supplementary Table S3a). Full text was available for 37 (69%) of studies. The main reason for downgrading risk of bias was related to study attrition (incomplete follow-up, 28 studies) and patient selection (non-consecutive sampling, 13 studies). Similar tendencies were seen for the short-term mortality death on ECMO (Supplementary Table S3b).
Short-term mortality
All studies reported on short-term mortality: 50 studies reported on either 30-day mortality (n = 142, 13 studies) or death during index hospitalization (n = 2328, 47 studies), and 36 studies reported on death on ECMO (n = 945). The overall pooled short-term mortality at 30 days or during index hospitalization was 35% (95% CI 29–40%; Fig. 2), and there was no difference in the pooled effect estimate based on sub-group analysis according to risk of bias (p = 0.14) and continent (p = 0.79; data not shown). By meta-regression, older age (p = 0.023) was associated with higher mortality, explaining 28% of the variation in results across studies (Supplementary Fig. S1). Other factors, such as the proportion of female patients, the proportion of those who received a biopsy, cardiac arrest, LV unloading, and earlier recruitment time frame did not explain heterogeneity across studies. The quality of the evidence on short-term mortality at 30 days or during index hospitalization was deemed moderate due to unexplained residual heterogeneity (Supplementary Fig. S2 and Supplementary Table S4). Similar tendencies were seen for the overall pooled effect estimate for death on ECMO; however, none of the aforementioned factors explained heterogeneity across studies (Supplementary Fig. S3, Supplementary Fig. S4, and Supplementary Fig. S2 and Supplementary Table S4, respectively).

Meta-analysis of pooled short-term mortality (30-day mortality or death during index hospitalization) among fulminant myocarditis patients treated with veno-arterial extracorporeal membrane oxygenation in multivariate studies
Factors associated with short-term mortality
A total of 7 predictors of short-term mortality were evaluated in univariate and multivariate analyses (n = 180, 3 studies; Table 2), and they were all independently associated with higher mortality. Whereas high lactate was reported in 2 studies, the other predictors were only reported in 1 study.
VAD or HTx after VA-ECMO implant
Twenty-four (44%) studies, including a total of 651 patients, reported on probability of receiving a VAD or HTx after VA-ECMO. The overall pooled effect estimate for VAD implantation was 2.2% (95% CI 0.1–5.9%). Risk of bias across studies, continent, age, female sex, receiving a biopsy, cardiac arrest, LV unloading, or earlier recruitment time frame (Supplementary Fig. S5) did not explain variation in results across studies. The pooled probability of HTx was 3.7% (95% CI 0.5–8.8%). Studies with lower proportion of LV unloading showed higher probability of HTx after VA-ECMO (p = 0.004). Other factors explored were not associated with differences in mortality across studies (Supplementary Fig. S6).
ECMO complications and complications from FM
Only 8 (15%) of the 54 studies reported on complications and with the most common being blood transfusions (55%, 95% CI 0–100%, reported in 2 studies) or bleeding (40%, 95% CI 23–59%, 6 studies), dialysis (35%, 95% CI 12–62%, 6 studies), infections (35%, 95% CI 16–56%, 8 studies), and third-degree atrioventricular block (30%, 95% CI 0–78%, 3 studies; Supplementary Fig. S7).
Discussion
In this systematic review and meta-analysis, consisting of 54 studies including a total of 2388 FM patients on VA-ECMO, we showed that the pooled estimate of short-term mortality in FM patients on VA-ECMO was 35% (95% CI 29–40%). Older age was the only factor associated with higher short-term mortality, explaining 28% of the variation in results across studies. The probability of receiving a VAD or HTx after VA-ECMO implant was low, and the probability of receiving a HTx was even lower in patients who received LV unloading during VA-ECMO support. These results remained consistent regardless of continent and the risk of bias category. The most frequent major complications included blood transfusions/bleeding, as well as acute kidney injury requiring dialysis, and infections.
Relation to previous work
Pooled analyses
To date, there are no large clinical trials evaluating outcomes in FM patients supported with VA-ECMO. In this context, the performance of pooled analyses ascertains outcomes and the effect of prognostic factors more precisely. A previously conducted meta-analysis by Chen et al. [15] reported a pooled estimate of in-hospital mortality of 33% (95% CI 26–41%) in 170 FM patients requiring VA-ECMO across 6 studies, which is comparable to our pooled estimate of short-term mortality (35%; 95% CI 29–40%). However, some differences are worth mentioning. Whereas Chen et al. [15] only included full-text studies in English and with 10 or more FM patients published between 2000 and 2012, we had broader inclusion criteria (both full-text studies and abstracts in any language with 5 or more FM patients published in 2009–2022). In addition, Chen et al. [15] only included in-hospital mortality, whereas we included 30-day mortality, death during index hospitalization, and death on VA-ECMO. Based on our expanded inclusion criteria, we included a total of 54 studies, of which 50 were published after 2012. As a result of the larger number of patients with FM on VA-ECMO included in the present study, we were able to report a more precise pooled estimate of short-term mortality with narrower confidence intervals. We were also able to explore heterogeneity and showed that older age increased short-term mortality. Furthermore, as we only included studies published after 2009, our results represent more contemporary VA-ECMO strategies and patient management.
The favorable results of VA-ECMO in FM patients are noticeably highlighted when the usage of VA-ECMO is compared across different etiologies. In a recent large systematic review and meta-analysis of 29,289 CS patients supported with VA-ECMO, Alba et al. [16], in a more restrictive analysis, showed a low pooled estimate of short-term mortality of FM patients of 40% (95% CI 33–46%) compared to other etiologies such as post-myocardial infarction (60%; 95% CI 57–64%), and heart failure (53%; 95% CI 46–59%). The association of lower mortality in FM patients supported with VA-ECMO could be partly explained by the nature of the disease, in which the probability of myocardial recovery is high if the hemodynamic status can be maintained. In contrast, cardiac recovery is less likely in other etiologies based on the presence of irreversible myocardial injury [17, 18].
Impact of risk factors on short-term mortality
Our finding of favorable results of VA-ECMO in FM patients who are younger is consistent with the ECMO literature [17, 19,20,21]. For instance, in one study of 135 FM patients who received VA-ECMO, the mean age of survivors was lower (51.9 ± 17.6 years) than non-survivors (62.1 ± 15.4 years) [19]. Evidence indicates that the poor prognosis in the elderly is probably due to comorbidities with advanced age [20]. In contrast to previous work [21], we did not find a benefit of VA-ECMO initiation in those without cardiac arrest. In addition, our finding that sex did not influence short-term mortality of FM patients on VA-ECMO is in accordance with some but not all of the ECMO literature [22, 23]. The fact that these studies are confined to small cohorts or single centers might contribute to the conflicting results.
Short-term mortality risk is of the utmost importance when deciding on the utility of treatment, particularly when considering a very resource intensive and costly intervention such as VA-ECMO [24]. This underlines the importance of identifying predictors that determine which patient groups have the highest chance of survival. This systematic review found that only 3 small mostly single-center studies (including 180 of the 2388 FM patients) reported on predictors. Moreover, these 3 studies reported on different predictors associated with short-term mortality and with only a very small overlap among the studies, making it difficult to pool together the effect estimates of the predictors and use these to guide clinical decisions. In addition, other factors impacting short-term mortality during VA-ECMO support (i.e., comorbidities, peak lactate level, liver injury, respiratory status, or renal function) were poorly reported (see Supplementary Table S2). Differences in these factors could perhaps explain variation in short-term mortality across studies. Consequently, it is of utmost importance to identify predictors which may aid clinicians in timely decision-making for VA-ECMO initiation in FM.
Complications
The complication rates in the present study were rather high. However, each complication was only reported in 2 to 8 studies, and consequently the variability of each complication was very high among studies. For instance, blood transfusions were reported in only 2 studies with a range of 0 to 100%, and bleeding was reported in 6 studies with a range of 23 to 59%. In addition, it is worth noting that several of the complications were not necessarily complications related to VA-ECMO but rather to the underlying disease of FM.
Coronavirus disease 2019
Myocarditis due to coronavirus disease 2019 (COVID-19) is a severe complication of the disease. Studies evaluating outcomes and management of patients with COVID-19 myocarditis are scarce. In addition, due to the respiratory compromise of COVID-19 patients, some patients received primarily ECMO for respiratory failure associated with subsequent multi-organ failure [25]. In an international cohort study of the Extracorporeal LIFE Support Organization (ELSO) registry, 1035 patients with COVID-19 received ECMO support (including both VA and venous-venous) at 213 hospitals in 36 countries. Of these, only 22 (2%) had myocarditis. However, separate mortality rates for the myocarditis patients were not reported [26]. Most of the evidence on mortality rates in FM patients with COVID-19 who receive VA-ECMO treatment comes from case reports [27,28,29]. Zeng et al. [27] reported the first case of COVID-19-induced FM in a 63-year-old male requiring VA-ECMO as a successful bridge to recovery. Since then, others have reported similar success of VA-ECMO as a bridge to recovery in COVID-19-induced FM in both sexes [28, 29]. Whether the pooled mortality estimate reported in this meta-analysis could be extrapolated to COVID-19 FM patients remains uncertain as COVID-19 infection presents with particular characteristics including respiratory failure and pro-thrombotic risk among others.
Implications for clinical practice and future research
The pooled results of this meta-analysis indicate that VA-ECMO should be considered in FM patients with cardiac failure who have failed conventional therapies, especially in younger patients. However, although a meta-analysis on aggregate study data may offer additional information over individual study reports, there is still a high variation in the results across studies with insufficient exploration of the different sources of heterogeneity. Thus, future research should focus on the performance of individual patient data meta-analysis, registry, or multicenter large prospective cohort studies, which offer improved quality of data and more robust analyses than meta-analysis on aggregate study data ensuing more reliable results. In addition, it is worth noting that the present study does not inform us of whether or not patients with FM should receive VA-ECMO, it only tells us what to expect if we choose this modality. Many patients with FM can be managed with inotropes alone and thereby avoid ECMO related complications. This notion is supported by clinical experience, as well as by previous work where not all FM patients were treated with ECMO, and they still had a good prognosis [30, 31]. However, due to ethical constraints, research studies comparing outcomes in FM patients treated with and without VA-ECMO are at risk of reporting biased worse outcomes in patients supported with VA-ECMO due to patient selection bias. Future research should focus on identifying characteristics of patients supported with VA-ECMO who would benefit more or less.
Strengths and limitations
A major strength of the present systematic review and meta-analysis is that we adapted broad inclusion criteria and included all cohort studies published after 2009 evaluating short-term mortality on VA-ECMO in FM patients. We defined explicit study eligibility criteria and assessed eligibility in duplicate. We followed the same approach to assess the quality of the individual studies eligible for inclusion (risk of bias) and for the data extraction. A final strength of our review is the use of the GRADE approach to rate our certainty in the pooled estimates. Some limitations should also be considered. First, all of the data collected was observational and retrospective in nature. Second, we pooled different definitions of short-term mortality together (i.e., mortality on ECMO, mortality at 30 days, mortality during index hospitalization) due to the limited studies and varied definitions in the literature available. This could have introduced some heterogeneity. However, Alba et al. [16] showed that in a sub-analysis of their meta-analysis of 58 studies, where each study reported on both 30-day mortality and death during index hospitalization, and where the two endpoints were compared, there was no significant difference in the risk estimates. Third, the management of VA-ECMO encompasses a multidisciplinary approach and has changed over time, leading to improved outcomes. To capture this change and report on contemporary patient outcomes, we arbitrarily limited the search to studies published after 2009. However, this strategy does not entirely address this issue, potentially leading to overestimation of mortality. Fourth, factors impacting short-term mortality during VA-ECMO support were poorly reported, and only included a small proportion of the total population of 2388 FM patients, making it difficult to explore whether these factors could perhaps explain variation in short-term mortality across studies. Fifth, we included studies with 5 or more FM patients, and therefore center volume and experience may also influence outcomes such that higher-volume centers report on lower mortality than low-volume centers [32]. The total number of cases performed at each center was not reported. Sixth, the verification of FM by histological findings was not carried out in all studies, and the indications for the initiation of VA-ECMO were not uniform among studies.
Conclusion
With moderate certainty, the short-term mortality in patients with rapidly progressive FM was 35%, with lower mortality in younger patients. When conventional therapies have failed, cardiopulmonary support with VA-ECMO should be considered, especially in the treatment of younger patients with severe FM. There is a need for more prospective studies exploring the utility of VA-ECMO in severe FM, as well as factors related to short-term mortality as careful patient selection may further enhance outcomes.
Availability of data and materials
The dataset generated during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- ELSO:
-
Extracorporeal LIFE Support Organization
- FM:
-
Fulminant myocarditis
- GRADE:
-
Grades of Recommendation, Assessment, Development, and Evaluation
- HTx:
-
Heart transplantation
- LV:
-
Left ventricular
- LVAD:
-
Left ventricular assist device
- MCS:
-
Mechanical circulatory support
References
Caforio AL, Pankuweit S, Arbustini E et al (2013) Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 34(33):2636–48, 48a-48d. https://doi.org/10.1093/eurheartj/eht210
Tschope C, Cooper LT, Torre-Amione G, Van Linthout S (2019) Management of myocarditis-related cardiomyopathy in adults. Circ Res 124(11):1568–1583. https://doi.org/10.1161/CIRCRESAHA.118.313578
Asaumi Y, Yasuda S, Morii I et al (2005) Favourable clinical outcome in patients with cardiogenic shock due to fulminant myocarditis supported by percutaneous extracorporeal membrane oxygenation. Eur Heart J 26(20):2185–2192. https://doi.org/10.1093/eurheartj/ehi411
Acker M (2001) Mechanical circulatory support for patients with acute-fulminant myocarditis. Ann Thorac Surg 71:S73–S76. https://doi.org/10.1016/S0003-4975(00)02628-X
Maejima Y, Yasu T, Kubo N et al (2004) Long-term prognosis of fulminant myocarditis rescued by percutaneous cardiopulmonary support device. Circ J 68:829–833. https://doi.org/10.1253/circj.68.829
Pahuja M, Adegbala O, Mishra T et al (2019) Trends in the incidence of in-hospital mortality, cardiogenic shock, and utilization of mechanical circulatory support devices in myocarditis (Analysis of National Inpatient Sample Data, 2005–2014). J Card Fail 25(6):457–467. https://doi.org/10.1016/j.cardfail.2019.04.012
Pozzi M, Banfi C, Grinberg D et al (2016) Veno-arterial extracorporeal membrane oxygenation for cardiogenic shock due to myocarditis in adult patients. J Thorac Dis 8(7):E495–502. https://doi.org/10.21037/jtd.2016.06.26
Lo Coco V, Lorusso R, Raffa GM et al (2018) Clinical complications during veno-arterial extracorporeal membrane oxigenation in post-cardiotomy and non post-cardiotomy shock: still the Achilles heel. J Thorac Dis 10(12):6993–7004. https://doi.org/10.21037/jtd.2018.11.103
Chen J, Spanier T, Gonzalez J et al (1999) Improved survival in patients with acute myocarditis using external pulsatile mechanical ventricular assistance. J Heart Lung Transplant 18:351–357. https://doi.org/10.1016/S1053-2498(98)00054-0
Hsu KH, Chi NH, Yu HY et al (2011) Extracorporeal membranous oxygenation support for acute fulminant myocarditis: analysis of a single center’s experience. Eur J Cardiothorac Surg 40(3):682–688. https://doi.org/10.1016/j.ejcts.2010.12.050
Aoyama N, Izumi T, Hiramori K et al (2002) National survey of fulminant myocarditis in japan therapeutic guidelines and long-term prognosis of using percutaneous cardiopulmonary support for fulminant myocarditis (Special Report From a Scientific Committee). Circ J 66:133–144. https://doi.org/10.1253/circj.66.133
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 8(5):336–341. https://doi.org/10.1016/j.ijsu.2010.02.007
Hayden J, van der Windt D, Cartwright J, Cote P, Bombardier C (2013) Assessing bias in studies of prognostic factors. Ann Intern Med 158:280–286. https://doi.org/10.7326/0003-4819-158-4-201302190-00009
Iorio A, Spencer FA, Falavigna M et al (2015) Use of GRADE for assessment of evidence about prognosis: rating confidence in estimates of event rates in broad categories of patients. BMJ 350:h870. https://doi.org/10.1136/bmj.h870
Cheng R, Hachamovitch R, Kittleson M et al (2014) Clinical outcomes in fulminant myocarditis requiring extracorporeal membrane oxygenation: a weighted meta-analysis of 170 patients. J Card Fail 20(6):400–406. https://doi.org/10.1016/j.cardfail.2014.03.005
Alba AC, Foroutan F, Buchan TA et al (2021) Mortality in patients with cardiogenic shock supported with VA ECMO: a systematic review and meta-analysis evaluating the impact of etiology on 29,289 patients. J Heart Lung Transplant 40(4):260–268. https://doi.org/10.1016/j.healun.2021.01.009
Chen Y, Yu H, Huang S et al (2008) Extracorporeal membrane oxygenation support can extend the duration of cardiopulmonary resuscitation. Crit Care Med 36(9):2529–2535. https://doi.org/10.1097/CCM.0b013e318183f491
Bermudez CA, Rocha RV, Toyoda Y et al (2011) Extracorporeal membrane oxygenation for advanced refractory shock in acute and chronic cardiomyopathy. Ann Thorac Surg 92(6):2125–2131. https://doi.org/10.1016/j.athoracsur.2011.07.029
Lee W, Kim Y, Choi H et al (2017) Advanced age as a predictor of survival and weaning in venoarterial extracorporeal oxygenation: a retrospective observational study. Biomed Res Int 2017:3505784. https://doi.org/10.1155/2017/3505784
Lee SN, Jo MS, Yoo KD (2017) Impact of age on extracorporeal membrane oxygenation survival of patients with cardiac failure. Clin Interv Aging 12:1347–1353. https://doi.org/10.2147/CIA.S142994
Chung SY, Sheu JJ, Lin YJ et al (2012) Outcome of patients with profound cardiogenic shock after cardiopulmonary resuscitation and prompt extracorporeal membrane oxygenation support. A single-center observational study Circ J 76(6):1385–1392. https://doi.org/10.1253/circj.CJ-11-1015
Wang A, Nemeth S, Kurlansky P et al (2020) Sex differences in patients with cardiogenic shock requiring extracorporeal membrane oxygenation. J Thorac Cardiovasc Surg S0022–5223(20):33397–33403. https://doi.org/10.1016/j.jtcvs.2020.12.044
Gill G, Patel JK, Casali D et al (2021) Outcomes of venoarterial extracorporeal membrane oxygenation for cardiac arrest in adult patients in the United States. J Am Heart Assoc 10(20):e021406. https://doi.org/10.1161/JAHA.121.021406
Abrams DC, Prager K, Blinderman CD, Burkart KM, Brodie D (2014) Ethical dilemmas encountered with the use of extracorporeal membrane oxygenation in adults. Chest 145(4):876–882. https://doi.org/10.1378/chest.13-1138
Cinar T, Hayiroglu MI, Cicek V, Uzun M, Orhan AL (2020) COVID-19 and acute myocarditis: current literature review and diagnostic challenges. Rev Assoc Med Bras (1992) 66Suppl 2(Suppl 2):48–54. https://doi.org/10.1590/1806-9282.66.S2.48
Barbaro RP, MacLaren G, Boonstra PS et al (2020) Extracorporeal membrane oxygenation support in COVID-19: an international cohort study of the Extracorporeal Life Support Organization registry. The Lancet 396(10257):1071–1078. https://doi.org/10.1016/S0140-6736(20)32008-0
Zeng JH, Liu YX, Yuan J et al (2020) First case of COVID-19 complicated with fulminant myocarditis: a case report and insights. Infection 48(5):773–777. https://doi.org/10.1007/s15010-020-01424-5
Veronese G, Cipriani M, Bottiroli M et al (2020) Fulminant myocarditis triggered by OC43 subtype coronavirus: a disease deserving evidence-based care bundles. J Cardiovasc Med (Hagerstown) 21(7):529–531. https://doi.org/10.2459/JCM.0000000000000989
Ishikura H, Maruyama J, Hoshino K et al (2021) Coronavirus disease (COVID-19) associated delayed-onset fulminant myocarditis in patient with a history of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. J Infect Chemother 27(12):1760–1764. https://doi.org/10.1016/j.jiac.2021.08.007
Ammirati E, Cipriani M, Lilliu M et al (2017) Survival and left ventricular function changes in fulminant versus nonfulminant acute myocarditis. Circulation 136(6):529–545. https://doi.org/10.1161/CIRCULATIONAHA.117.026386
McCarthy R, Boehmer J, Hruban R et al (2000) Long-term outcome of fulminant myocarditis as compared with acute (nonfulminant) myocarditis. N Engl J Med 342:690–695. https://doi.org/10.1056/NEJM200003093421003
Barbaro RP, Odetola FO, Kidwell KM et al (2015) Association of hospital-level volume of extracorporeal membrane oxygenation cases and mortality. Analysis of the extracorporeal life support organization registry. Am J Respir Crit Care Med 191(8):894–901. https://doi.org/10.1164/rccm.201409-1634OC
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and the design of the work. Drs. Julie KK Vishram-Nielsen, Farid Foroutan, and Ana Carolina Alba contributed to the analyses and interpretation of data. Drs. Julie KK Vishram-Nielsen and Ana Carolina Alba drafted the manuscript. All authors revised the manuscript critically for important intellectual content. All gave final approval of the manuscript submitted and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethical approval
Not applicable.
Competing interests
Dr. Finn Gustafsson reports receiving personal fees from Abbott, Novartis, Boehringer-Ingelheim, Pfizer, Bayer, Astra-Zeneca, Pharmacosmos, Alnylam, and Ionis, all outside of the submitted work. EF reports personal fees from ALung Technologies, Aerogen, Baxter, GE Healthcare, Inspira, and Vasomune outside the submitted work. Drs. Julie KK Vishram-Nielsen, Farid Foroutan, Saima Rizwan, Heather J Ross, Eddy Fan, Vivek Rao, Filio Billia, and Ana Carolina Alba, as well as Serena S Peck, Julia Bodack, and Ani Orchanian-Cheff, have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Vishram-Nielsen, J.K.K., Foroutan, F., Rizwan, S. et al. Patients with fulminant myocarditis supported with veno-arterial extracorporeal membrane oxygenation: a systematic review and meta-analysis of short-term mortality and impact of risk factors. Heart Fail Rev 28, 347–357 (2023). https://doi.org/10.1007/s10741-022-10277-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-022-10277-z