
Abstract
Hospitalization for breast surgery is a distressing experience for women. This study investigated the impact of music therapy (MT), an integrative approach that is characterized by the establishment of a therapeutic relationship between patients and a certified music therapist, through different musical interventions targeted to the specific needs of the patients. The impact of two different MT experiences was compared on anxiety and distressing emotions.
Methods
One hundred fifty-one patients during hospitalization for breast surgery were randomly assigned to two music therapy treatment arms: individual/receptive (MTri) vs. group/active-receptive integrated (MTiGrp). Stress, depression, anger, and need for help were measured with the emotion thermometers (ET) and State Trait Anxiety Inventory Y-1 form (STAY-Y1). Data were collected before and after the MT intervention.
Results
Both types of MT interventions were effective in reducing all the variables: stress, depression, anger, and anxiety (T Student p‹0.01). Patients’ perception of help received was correlated with a significant reduction in anxiety and distressing emotions during hospitalization for breast surgery.
Conclusion
Considerations regarding the implementation of MT interventions in clinical practice are discussed. In individual receptive MT, there was a significant decrease in anxiety levels, whereas in the integrated MT group, there was a higher perception of help received and use of inter-individual resources.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
During diagnosis and treatment of breast cancer, women can be exposed to intense anxiety and stress, related to uncertainty, type of treatment, and life-threatening situations. The anxiety can affect both the surgical experience and the experience of pain [1, 2]. Women are subjected to significant psychological distress [3,4,5,6]; and high-state anxiety, distress, and emotional suppression can be modified if women share their experience of illness in a supportive health care environment [7,8,9,10]. Music therapy has been recommended for anxiety/stress reduction and for depression/mood disorders in women with breast cancer [11, 12]. In oncological settings, music therapy (MT) contributes [13, 14] to counteract symptom management [15] and significantly improves health of adult cancer patients in various treatment phases [16]. MT is characterized by the establishment of a therapeutic relationship between the patient (or group of patients) and a certified music therapist, who offers musical interventions targeted to the specific needs of the patient [14, 17, 18] through receptive or active approaches [19, 20]. In order to manage pre- and post-operative anxiety in a safe, effective, and time-efficient way, music therapy with both live and recorded music can be included as integrative treatment surgical procedures [21,22,23]. In MT groups with hospitalized cancer adults, its effectiveness on significantly improved mood, anxiety, and sense of cohesion has been shown [24, 25]. Group MT in hospital settings also has a psychosocial value as it brings patients out of isolation, creating strong social and emotional bonds and generating a feeling of well-being [26]. Patients with breast cancer undergoing a single group session of MT, highlight a reduction of negative emotions during oncological treatments after single group session of MT and emotional expression [27]. Further research is now needed to identify the optimal approach to reduce preoperative anxiety in breast cancer undergoing breast surgery, studying the effects, timing, and best setting (individual or group) of complementary music therapy approaches [28, 29].
Aim
This study was conducted during the 2 years preceding the Covid-19 pandemic in an oncology ward of a hospital in southern Italy. Aim was to evaluate the impact of a single MT session on anxiety, distress, anger, depression, and help-seeking in cancer patients hospitalized for breast surgery. Two MT approaches were compared: an individual receptive and an interactive group. It also highlighted social variables (such as age, educational qualification, and occupational status) of the patients who can benefit the most from music therapy [16].
Patients and study design
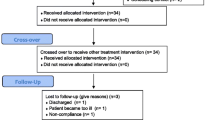
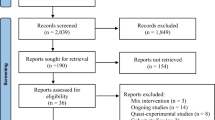
Patients enrolled were female inpatients with breast cancer admitted to the hospital for breast surgery, age 25–70 years old, a good understanding of the Italian language, informed consent to participate, ECOG 0–1, and absence of mental illness or auditory/visual deficits. Exclusion criteria were assumption of opioids, psychotropic drugs, or inability to express informed consent. One hundred ninety-five patients were eligible to participate and were informed, 44 were excluded because not able to move from bedside (N = 30), or declined to participate (N = 14). The remaining 151 patients were enrolled and divided into two experimental arms (flow chart Fig. 2 in Appendix). Informed consent was obtained from all individual participants included in the study. The design was single-center, experimental, and randomized, with two experimental arms comparing two different music therapy approaches. Using a randomized selection criterion, the two arms were defined: ARM1/MTri, in which 48 individual sessions of receptive MT were conducted, and ARM2/MTiGrp, which involved 25 integrated group music therapy sessions with an average of four patients each.
Material and method
A psycho oncologist administered test before (T0) and 1 h after (T1) the treatment. Sociodemographics and clinical data (as described in Table 4) were collected from the clinical chart. The first tool used was emotion thermometer (ET) Italian Version [30] that measures emotions through five analogic visual scales of four domains (stress, anxiety, depression, and anger) as well as the perceived effectiveness of the intervention received through the variable “need for help.” The second tool was State Trait Anxiety Inventory (STAI), used only in its form Y-1 to measure the state anxiety through 20 items are rated on a 4-point scale [31].
Description of music therapy interventions
The MT interventions were led by a senior certified board clinical music therapist (Mtc). In ARM1—receptive music therapy (MTri), each 60-min session followed phases. The Mtc offered the patient a brief experience of listening to three pre-recorded pieces of music inviting her to choose one of them and then conducting a relaxation on the chosen music listening. The pre-recorded music for the session was selected by Mtc on the basis of her music therapy and clinical experience from her specialized training in BMGIM (Bonny Method of Guided Imagery and Music). Referring to the literature [32], the choice was been oriented towards pieces with supporting characteristics. The identified had no features of harmonic complexity and contained no unexpected surprise effects. The chosen pieces had a form and dynamics of musical elements without sudden changes, with good predictability, melodic recursiveness in a major mode, and a basic ostinato on which two instruments intervened at a time, together evoking a sense of reliability. The selection was made so that listening could be easy, light, and caressing. Mtc decided to offer patients the opportunity to be able to make an individual choice among three pieces having these characteristics, so as to still give a chance for preference at that time, the day before mastectomy surgery. Afterwards, the Mtc improvised for the patient on a range of different musical instruments. To conclude, the MTC progressively guided the patient to regain contact with environment without the presence of music. At the end of the session, the MTC invited the patient to give a verbal feedback on the experience. The procedure is summarized in Appendix Fig. 3.
In ARM2—integrated group music therapy (MTiGrp), the psycho-oncologist co-lead the Mtc the group experience, which lasted 90 min. In the MTiGrp, patients were offered several integrated active-receptive music therapy experiences. The setting was set up in a dedicated room of Breast Surgery Unit equipped with musical instruments and chairs positioned in a circle. Each session was structured in two parts: the first part focused on the choice of an instrument and the possibility of playing it freely following the state of mind (Fig. 1) and the group musical improvisation that gradually formed. The second part consisted of visualization experiences through images and music, choral singing, and concluding verbal and reflective discussion. The procedure is summarized in Appendix Fig. 4.

A woman in MTiGrp plays her sound exploration with the chosen musical instrument, the pentatonic chitara
Statistical analysis
The scores were summarized in terms of median and interquartile range (i.e., the interval between the first and third quartiles of the empirical distribution). The distribution of scores for different arms or parameters was compared using a non-parametric Kruskall-Wallis Mann–Whitney test [32], whereas for comparison of only two groups, we used Mann–Whitney U test [33]. The scores measured before and after the treatment were compared using paired T test [34]. A result was considered statistically significant when the p value was less than 0.05. MATLAB R2021a (MathWorks, Inc., Natick, MA, USA) software was used for the statistical analysis.
Results
One hundred three women participated in the MTiGrp intervention with mean age of 55.6 years old (range 27–87), whereas 48 women participated in MTri with mean age of 54.8 years old (range 26–71), with the sociodemographic characteristics listed in Appendix Table 8. We have calculated the difference between the pre- and post-treatment scores of the STAI-Y1 and the emotion thermometers (Term) measured both MTiGrp (Table 1) and MTri treatment (Table2) Pre-and post-treatment scores differed in a statistically significant way (p value T Student for paired data < 0.01) in both the complementary MTiGrp treatment and the MTri treatment: both interventions showed positive effects in reducing anxiety and emotional parameters. “The Help” parameter, number five, was excluded from this phase of analysis, as the difference between the value (from 1 to 10) “Effectiveness of Help Received”/post and the value (from 1 to 10) “Need for Help”/pre cannot be used as a measure of efficacy.
For each treatment arm, baseline differences of the variables under study (anxiety and emotional parameters) were also evaluated in relation to the sociodemographic characteristics of the sample, such as age, educational qualification, and profession. With regard to the MTiGrp group, there were no significant differences between the distributions of the sociodemographic categories of patients for any of the pre-treatment STAI scores and parameters of emotion thermometers (Term) considered (p value Kruskall-Wallis test, < 0.01) (Table 3).
The same consideration can be extended to the MTri ARM1 (Table 4). There were no significant associations between the variables under study and the sociodemographic and clinical characteristics considered (p value Krushall-Wallis test < 0.01).
Both MT intervention modalities offer significant reductions in anxiety levels and emotion thermometers. The current study aimed at evaluating of any sociodemographic subgroups, for each intervention arm, could benefit more from music therapy treatments. There were no significant differences between the distributions of the sociodemographic categories of patients for any of the pre-treatment STAI scores and parameters of emotion thermometers (Term) considered (p value Kruskall-Wallis test, < 0.01).
With regard to MTiGrp group, Table 5 shows that there is no significant difference between the distributions of the sociodemographic categories of patients for each of the five individual characteristics analyzed (p value Kruskall-Wallis test < 0.01). It follows that the sample studied did not show any significant association between the difference in pre- and post-treatment scores for either the STAI parameter, the emotion thermometers, or the demographic and clinical characteristics taken into consideration. The same study was carried out on patients in the MTri group, to see whether this type of group music therapy session could be more beneficial for a sociodemographic subgroup than the individual sessions.
With regard to MTri ARM1 group, there are significant differences in distribution of patient categories only for the exception of depression and anxiety in relation to age and educational qualification (p value non-parametric Kruskall-Wallis test < 0.05): after MTri, older women showed a greater reduction in depression and women with a higher level of education showed greater reduction in anxiety (Table 6). Although both individual and group music therapy showed significant reductions in anxiety and emotional parameters, the present study aimed at understanding whether one of these was more effective than the other.
Although the distribution of difference in pre- and post-treatment scores in the two arms showed a greater reduction in anxiety in MTRi (p value Mann–Whitney test < 0.01) (Table 7), it was significantly effective in both (Tables 2 and 3). In order to understand which of the two experiences is more effective in terms of the subjective perception of help received, the emotion thermometer “Help-Post; Efficacy of the help received” was compared in the two ARMs MTGrp and MTRi: 7.81 (SD 3.05) in MTGrp vs. 8.64 (SD 2.07) in MTRi, with Student’s t test. The results did not reveal significant differences between the two arms (p value T test > 0.05).
Discussion
The results show that in the perioperative phase both MT interventions offered a significant reduction in the state anxiety and improvement in emotion thermometers of stress, depression, anxiety, and anger. Although equally effective in reducing state anxiety, the individual intervention leads to a more pronounced reduction in levels of state anxiety. No differences in the perception of received help were found between the two interventions. In this study, we were well aware of the limitation of the absence of a control group; within the number of participants eligible for the study, we prioritized the comparison of the two different music therapy approaches in order to better understand their specific usefulness and declination with such a clinical population.
Efficacy of the two interventions in reducing anxiety and negative emotions
The results confirm previous literature: MT in the perioperative phase, which can be effective in reducing anxiety, shows highly potential benefits in adult cancer patients addressed with supplementary treatment undergoing mastectomy [35,36,37]. Beneficial effects are also shown in states of depression and distress [38]. The current study also addresses the theme of anger, an aspect which has been less explored in literature to date, and attests to its reduction in both treatments.
Individual intervention leads to a more pronounced reduction in anxiety levels
In the individual approach, patients have had the possibility to choose one piece for their session from a set of three pieces preselected by the MTC. Even if this music could not represent the patient most preferred one, making choices and exercising preferences for patients with cancer, who are subjected to medical-surgical procedures during hospitalization as “passive” subjects, can have a positive impact on anxiety [39]. Furthermore, the individual sessions also allowed the music therapist to tailor the interventions even more to patients’ individual needs [40]. This was achieved by listening and attuning more deeply on the individual timing, breathing, and level of energy of the patient and share a space of intimacy trough music.
The perception of the help received in the two interventions is substantially the same
Despite the existence of different modulating factors, the effectiveness of the interventions in the two music therapy approaches can be considered similar. While choice of the musical piece, individual, and individualized attention of the music therapist, are central in individual treatment; in group intervention, the “co-therapeutic” factors highlighted are sharing a traumatic experience with other people, mentalizing, and cognitively processing the traumatic experience [41].
In fact, after the MTiGrp session, the psycho–oncologist conduced a moment of verbal reflection on the emotions evoked by the music [42] that aimed at facilitating the externalization and sharing of patients’ emotional experiences rather than achieving relaxation.
The group intervention was therefore focused on the expression of emotions and on the exploration of personal experiences and their affective resonance in the group of the musical improvisation.
Clinical observations
The data collected show that both approaches can be effective even though they focus on different aspects: greater emphasis on intra-psychic elements for the receptive modality, and increased interpersonal and expressive dynamics for the active modality. Observation of the overlap** effects in terms of anxiety and emotional parameters can guide the clinician in suggesting one intervention rather than the other. Firstly, a high level of patient anxiety, would point more towards the individual approach, both to satisfy the need for greater emotional containment and to avoid a potential negative conditioning of the emotional climate within the group context.
Secondly, the conditions dictated by the Covid 19 pandemic, may make it inappropriate to create situations of physical proximity between hospitalized and potentially fragile patients, thus making a receptive approach of individual music therapy more appropriate. Furthermore, it is necessary to bear in mind the complex logistics of hospital wards, exacerbated by the current pandemic. It is not always possible to find a separate room for group music therapy for example, and thus for practical reasons, the individual setting may sometimes be the only feasible choice. In spite of all these considerations, however, the group setting may allow reducing anxiety and regulating emotional parameters in the perioperative phase, for a larger number of patients and with less expenditure of time and professional resources.
Study limitations
This study has some limitations of which we are aware that were due to ethical considerations and decisions.
Primally, we did not perform a follow-up after patient discharge observing the endurance of positive effects achieved. In fact, a structured follow-up would have been too demanding and stressful for patients.
Another limitation is the absence of a valuation of the emotional condition of women who refused to participate in the study. Some patients refused to participate in the group or to receive individual music therapy because they were frightened or depressed, so we chose not to subject these patients to psychological testing in order not to further burden their emotional condition. Conditions permitting, in future studies, these elements could be included for greater reliability of results.
Finally, as mentioned above, we did not structure a control group with standard care for ethical and organizational reasons. Since the aim of the study was to evaluate the impact of a single session and specifically the possible greater appropriateness of one approach over the other, we preferred to offer all eligible patients the opportunity to benefit from such an experience by joining the study. We did not want to deprive any patient of a potentially supportive experience, especially because some control group patients could have been in the same room with a patient of the experimental arm. This could generate feelings of frustration, which we did not consider useful and ethical. For future studies, we will try to refine organizational measures that may also make it possible to implement a control group without an ethical impact on patients.
Conclusions
Since mastectomy psychologically affects women in a complex and multidimensional way, patients hospitalized for breast surgery may experience emotional distress caused by the surgical experience. The present study indicates that even a single music therapy session during hospitalization can be varied according to certain psychological variables. In individual receptive MT, there was a significant decrease in anxiety levels, whereas in the integrated MT group, there was a higher perception of help received and use of inter-individual resources. This study offers suggestions to implement active and receptive interventions with supportive purposes in the perioperative phase of breast surgery. All of these clinical interventions are oriented towards a humanization of medicine from the point of view of the global care of hospitalized patients.
Data availability
The data presented in this study are not publicly available and must be requested directly from the authors.
Abbreviations
- S.T.A.I. Y-1:
-
State Trait Anxiety Inventory Y-1;
- E.T.:
-
Emotion thermometers
- MT:
-
Music therapy
- Mtc:
-
Senior certified clinic music therapist
- Mtri:
-
Individual receptive music therapy
- MTiGrp:
-
Integrated group music therapy
References
Poleshuck EL, Katz J, Andrus CH, Hogan LA, Jung BF, Kulick DI, Dworkin RH (2006) Risk factors for chronic pain following breast cancer surgery: a prospective study. J Pain 7(9):626–634. https://doi.org/10.1016/j.jpain.2006.02.007
Lim CC, Devi MK, Ang E (2011) Anxiety in women with breast cancer undergoing treatment: a systematic review. Int J Evid Based Healthc 9(3):215–235
Montgomery M, McCrone SH (2010) Psychological distress associated with the diagnostic phase for suspected breast cancer: systematic review. J Adv Nurs 66(11):2372–2390. https://doi.org/10.1111/j.1365-2648.2010.05439.x
Ludwigson A, Huynh V, Bronsert M, Sloan K, Murphy C, Christian N, Tevis SE (2020) A screening tool identifies high distress in newly diagnosed breast cancer patients. Surgery 168(5):935–941. https://doi.org/10.1016/j.surg.2020.04.051
Chirico A, Lucidi F, Mallia L, D’Aiuto M, Merluzzi TV (2015) Indicators of distress in newly diagnosed breast cancer patients. PeerJ 3:e1107. https://doi.org/10.7717/peerj.1107
Mark M (2003) Patient anxiety and modern elective surgery: a literature review. J Clin Nur 12(6):806-815.9. https://doi.org/10.1046/j.1365-2702.2003.00812.x
Katsohiraki M, Poulopoulou S, Fyrfiris N, Koutelekos I, Tsiotinou P, Adam O, Vasilopoulou E, Kapritsou M (2020) Evaluating preoperative anxiety levels in patients undergoing breast cancer surgery. Asia Pac J Oncol Nurs 7(4):361–364. https://doi.org/10.4103/apjon.apjon_31_20
Boinon D, Sultan S, Charles C, Stulz A, Guillemeau C, Delaloge S, Dauchy S (2014) Changes in psychological adjustment over the course of treatment for breast cancer the predictive role of social sharing and social support. Psycho-oncology 23(3):291–298. https://doi.org/10.1002/pon.3420
Nakatani Y, Iwamitsu Y, Kuranami M, Okazaki S, Yamamoto K, Watanabe M, Miyaoka H (2003) Predictors of psychological distress in breast cancer patients after surgery. Kitasato Med J 43:49–56. https://doi.org/10.1016/j.anr.2017.10.003
Iwamitsu Y, Shimoda K, Abe H, Tani T, Okawa M, Buck R (2005) The relation between negative emotional suppression and emotional distress in breast cancer diagnosis and treatment. Health Commun 18(3):201–215. https://doi.org/10.1207/s15327027hc1803_1
Greenlee H, DuPont-Reyes MJ, Balneaves LG, Carlson LE, Cohen MR, Deng G, Johnson JA, Mumber M, Seely D, Zick SM, Boyce LM, Tripathy D (2017) Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin 67(3):194–232. https://doi.org/10.3322/caac.21397
Kievisiene J, Jautakyte R, Rauckiene-Michaelsson A, Fatkulina N, Agostinis-Sobrinho C (2020) The effect of art therapy and music therapy on breast cancer patients: what we know and what we need to find out—a systematic review. Evid Based Complement Alternat Med. https://doi.org/10.1155/2020/7390321
Bradt J, Dileo C, Magill L, Teague A (2016) Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst Rev 8.https://doi.org/10.1002/14651858.CD006911.pub3
Magill L (2006) Role of music therapy in integrative oncology. J Soc Integr Oncol 4(2):79–81. https://doi.org/10.2310/7200.2006.009
Bradt J, Potvin N, Kesslick A, Shim M, Radl D, Schriver E, Gracely EJ, Komarnicky-Kocher LT (2015) The impact of music therapy versus music medicine on psychological outcomes and pain in cancer patients: a mixed methods study. Support Care Cancer 23(5):1261–1271. https://doi.org/10.1007/s00520-014-2478-7
Köhler F, Martin ZS, Hertrampf RS, Gäbel C, Kessler J, Ditzen B, Warth M (2020) Music therapy in the psychosocial treatment of adult cancer patients: a systematic review and meta-analysis. Front Psychol 11:651. https://doi.org/10.3389/fpsyg.2020.00651
Trondalen G, Bonde L O (2012) Music therapy: models and interventions. In Music, Health, and Wellbeing; MacDonald, R., Kreutz, G., Mitchell, L., Eds.; Oxford University Press: Oxford, UK, 40–61
Bonde LO, Wigram T (2002) A comprehensive guide to music therapy: theory, clinical practice, research and training. Jessica Kingsley Publishers, London, UK, pp 32–34
Vinayak S, Dehkhoda F, Vinayak R (2017) The effect of music therapy on sleep quality of cancer patients undergoing chemotherapy or radiotherapy: a randomized control trial. J Soc Sc (COES&RJ-JSS) 6(4):734–743. https://doi.org/10.25255/jss.2017.6.4.734.743
Lynch KA, Emard N, Liou KT, Popkin K, Borten M, Nwodim O, Atkinson TM, Mao JJ (2021) Patient perspectives on active vs. passive music therapy for cancer in the inpatient setting: a qualitative analysis. J Pain Symptom Manage 62(1):58–65. https://doi.org/10.1016/j.jpainsymman.2020.11.014
Palmer JB, Lane D, Mayo D, Schluchter M, Leeming R (2015) Effects of music therapy on anesthesia requirements and anxiety in women undergoing ambulatory breast surgery for cancer diagnosis and treatment: a randomized controlled trial. J Clin Oncol 33(28):3162–3168. https://doi.org/10.1200/JCO.2014.59.6049
Giordano F, Zanchi B, De Leonardis F, Rutigliano C, Esposito F, Brienza N, Santoro N (2020) The influence of music therapy on preoperative anxiety in pediatric oncology patients undergoing invasive procedures. The Arts in Psychotherapy 68:101649. https://doi.org/10.1016/j.aip.2020.101649
Li XM, Zhou KN, Yan H, Wang DL, Zhang YP (2012) Effects of music therapy on anxiety of patients with breast cancer after radical mastectomy: a randomized clinical trial. J Adv Nurs 68(5):1145–1155. https://doi.org/10.1111/j.1365-2648.2011.05824.x
Chaput-McGovern J, Silverman MJ (2012) Effects of music therapy with patients on a post-surgical oncology unit: a pilot study determining maintenance of immediate gains. Arts Psychother 39(5):417–422. https://doi.org/10.1016/j.aip.2012.06.008
Waldon EG (2001) The effects of group music therapy on mood states and cohesiveness in adult oncology patients. J Music Ther 38(3):212–238. https://doi.org/10.1093/jmt/38.3.212
Stanczyk MM (2011) Music therapy in supportive cancer care. Rep Pract Oncol Radiother 16(5):170–172. https://doi.org/10.1016/j.rpor.2011.04.005
Romito F, Lagattolla F, Costanzo C, Giotta F, Mattioli V (2013) Music therapy and emotional expression during chemotherapy. How do breast cancer patients feel? Eur J Int Med 5(5):438–442. https://doi.org/10.1016/j.eujim.2013.04.001
Evans H, Brown EL, Groom J (2019) Preoperative relaxation techniques for breast cancer patients undergoing breast-altering surgery a systematic review. Iris J of Nur & Car. 1 (3). https://doi.org/10.33552/IJNC.2019.01.000512
Gramaglia C, Gambaro E, Vecchi C, Licandro D, Raina G, Pisani C, Burgio V, Farruggio S, Rolla R, Deantonio L, Grossini E, Krengli M, Zeppegno P (2019) Outcomes of music therapy interventions in cancer patients—a review of the literature. Crit Rev Oncol Hematol 138:241–254. https://doi.org/10.1016/j.critrevonc.2019.04.004
Emotion Thermometers Tool © A rapid modular screening tool for detection and monitoring of emotional disorders in clinical practice. Available online: http://www.psycho-oncology.info/ET_italian.pdf (accessed on 23 February 2022).
Spielberger CD, Gorsuch RL, Lushene RE, Vagg PR, Jacobs GA (1983) Manual for the State-Trait Anxiety Inventory (Form Y1–Y2). Consulting Psychologists Press, Palo Alto, CA
Värja M, Bonde LO (2014) Music as co-therapist: towards a taxonomy of music in therapeutic music and imagery work. Music and Medicine 6(2):16–27
Corder GW, Foreman DJ (2011) Nonparametric Statistics for Non-Statisticians: a step-by-step approach. Wiley, New York, NY
Mann HB, Whitney DR (1947) On a test of whether one of two random variables is stochastically larger than the other. Ann Math Statist 18(1):50–60. https://doi.org/10.1214/aoms/1177730491
David HA, Gunnink JL (1997) The paired t test under artificial pairing. Am Stat 51(1):9–12. https://doi.org/10.2307/2684684
Lopez G, Christie AJ, Powers-James C, Bae MS, Dibaj SS, Gomez T, Williams JL, Bruera E (2019) The effects of inpatient music therapy on self-reported symptoms at an academic cancer center: a preliminary report. Support Care Cancer 27(11):4207–4212. https://doi.org/10.1007/s00520-019-04713-4
Palmer JB, Lane D, Mayo D (2017) Surgical music therapy: the significance and implementation of music therapy in the operating arena. Music Ther Perspect 35(1):30–35. https://doi.org/10.1093/mtp/miv036
Boyde C, Linden U, Boehm K, Ostermann T (2012) The use of music therapy during the treatment of cancer patients: a collection of evidence. Global Advances in Health and Medicine 1(5):24–29. https://doi.org/10.7453/gahmj.2012.1.5.009
Bradt J, Dileo C, Myers-Coffman K, Biondo J (2021). Music interventions for improving psychological and physical outcomes in people with cancer. Cochrane Database Syst Rev, 10. https://doi.org/10.1002/14651858.CD006911.pub4
Yates GJ, Silverman MJ (2015) Immediate effects of single-session music therapy on affective state in patients on a post-surgical oncology unit: a randomized effectiveness study. Arts Psychother 44:57–61. https://doi.org/10.1016/j.aip.2014.11.002
Bradt J, Dileo C, Shim M (2013). Music interventions for preoperative anxiety. Cochrane Database Syst Rev 6. https://doi.org/10.1002/14651858.CD006908.pub2
Nolan P (2005) Verbal processing within the music therapy relationship. Music Ther Perspect 23(1):18–28. https://doi.org/10.1093/mtp/23.1.18
Zeppegno P, Krengli M, Ferrante D, Bagnati M, Burgio V, Farruggio S, Rolla R, Gramaglia C, Grossini E (2021) Psychotherapy with music intervention improves anxiety, depression and the redox status in breast cancer patients undergoing radiotherapy: a randomized controlled clinical trial. Cancers 13(8):1752. https://doi.org/10.3390/cancers13081752
Acknowledgements
Special thanks to Timothy Trevor-Briscoe for revision of the text in English. The authors would also like to thank the medical and nurse team of the Breast Surgery for departmental collaboration; the General Director and the Scientific Director for their support and encouragement in both MT research and clinical music therapy activities with adult cancer patients in I.R.C.C.S. Istituto Tumori “Giovanni Paolo II” of Bari, Italy.
Author information
Authors and Affiliations
Contributions
Conceptualization, methodology, investigation: Fulvia Lagattolla, Francesca Romito; data curation: Francesca Caporale Erika Rieti; formal analysis and software: Annarita Fanizzi, Raffaella Massafra; presentation: Barbara Zanchi, Vito Lorusso, Sergio Diotaiuti, Annarita Fanizzi, Raffaella Massafra; writing—original draft preparation: Fulvia Lagattolla, Francesca Romito. Writing—review and editing: Barbara Zanchi, Silvia Costanzo, Claudia Cormio; principal investigator: Claudia Cormio. Supervision: Silvia Costanzo, Sergio Diotaiuti, Barbara Zanchi, Vito Lorusso, Pietro Milella. All authors read and approval the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the guidelines of the Declaration of Helsinki. It was submitted and approved by the Scientific Board and Ethic committee of IRCCS Istituto Tumori “Giovanni Paolo II” of Bari, Italy. The study took place within a wider 3-year research project in psycho-oncology: “Abbraccio di Luce: terapie complementari e supporto psicologico per i pazienti oncologici” with protocol number 575/2016. Principal Investigator Claudia Cormio. Informed consent was obtained from all subjects involved in the study.
Consent for publication
Institutional consent obtained.
Competing interests
The authors declare no competing interests.
Disclaimer
The authors affiliated to the IRCCS Istituto Tumori “Giovanni Paolo II”, Bari, are responsible for the views expressed in this article, which do not necessarily represent the Institute.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.



Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lagattolla, F., Zanchi, B., Pietro, M. et al. Receptive music therapy versus group music therapy with breast cancer patients hospitalized for surgery. Support Care Cancer 31, 162 (2023). https://doi.org/10.1007/s00520-023-07624-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00520-023-07624-7