
Abstract
Background
Role of Long non-coding RNAs in cancer research in the recent years have been highlighted with evidence to their involvement in cancer disease pathogenesis and progression. One of these emerging long non-coding RNAs is differentiation antagonizing non-protein coding RNA (DANCR). DANCR distinct expression in different cancers and implication in tumor signaling pathways made it a promising therapeutic target for cancer.
The purpose of this study was to evaluate DANCR expression in de novo acute myeloid leukemia (AML) patients and to assess DANCR expression in relation to cytogenetics and French American British (FAB) AML classification as well as correlate DANCR expression with patients’ response to treatment.
The present study included 60 newly diagnosed AML patients and 30 healthy subjects as controls. Relative DANCR expression was done using real time qPCR method.
Results
DANCR was significantly downregulated in AML patients compared to controls (p = 0.038). In addition, DANCR showed significantly lower expression in M4 and M5 compared to M0, M1, and M2 groups (p < 0.001). Furthermore, DANCR expression was significantly downregulated in cytogenetically normal AML patients compared to the controls (p = 0.011).
Conclusion
Significant downregulation of DANCR in AML suggests a potential tumor suppressor role and variable expression of DANCR among AML subtypes suggests that DANCR action may be different among AML subtypes. Also, M1 subtype patients with higher DANCR expression were less refractory to treatment and therefore less resistant to cytarabine.
Similar content being viewed by others


Background
Acute Myeloid leukemia (AML) is the most common form of all leukemias affecting adults, making about 25% of all leukemia types with an incidence rate of 4 per 100,000 and with a high mortality rate being the sixth highest cancer related death in male population in the United States [1]. AML is characterized by uncontrolled proliferation of cells and arrest of differentiation of myeloid progenitors in different stages [2]. AML is commonly classified using two staging systems, the French-American-British (FAB) classification which classifies AML into subtypes from M0 to M7 depending on the cell morphology and the type of cell that AML arises from [3] and the more recent WHO classification which included the variable cytogenetic abnormalities that occur in AML [4].
AML is a disease of complex pathogenesis, and is known for its genetic heterogeneity, where there is more than one mutation found in the majority of the patients [5]. Around half of the patients have chromosomal abnormalities, and the other half is cytogenetically normal AML (CN-AML), with or without somatic mutations in nucleophosmin (NPM1), or FMS-like tyrosine kinase 3 internal tandem duplication (FLT3-ITD) which are in-frame duplications of variable size, ranging from three to more than one thousand nucleotides or mutations in CEBPA [6, 7].
Identification of these genetic mutations in AML focused on protein-coding genes to understand complex molecular pathogenesis of the disease. Despite aggressive treatment regimen, response to treatment is still unsatisfactory and long-term survival is still low [8], thus identifying potential molecular therapeutic targets has become essential to improve disease prognosis.
High throughput technologies highlighted the various roles played by non-coding RNAs (ncRNAs), which are transcribed from the human genome, but are not encoded into proteins. ncRNAs that exceed 200 nucleotides in length are Long non-coding RNAs (lncRNAs) [9]. Though they are not encoded into proteins, they are involved in various cellular functions such as regulating the expression of different genes involved in cell cycle, proliferation, differentiation, stem cell differentiation, apoptosis, invasion, migration and autophagy [10]. Subsequent studies suggested that several lncRNAs are deregulated in cancers and may play an oncogenic role through cancer development [11, 12].
Among these lncRNAs is differentiation antagonizing non-protein coding RNA (DANCR), which is 855 bases in length [23]. Follow-up of patients was done after standard induction therapy with 7 plus 3 regimen (7 days of cytarabine plus doxorubicin on days 1 to 3) to track response to treatment. Patients who had less than 5% of bone marrow (BM) blasts as well as showed recovery of peripheral blood counts without circulating blasts were considered complete remission. Partial remission was defined as less than 25% of blast cells in the BM and BM is functioning normally. Patients who were unresponsive to treatment were considered refractory.
RNA isolation and cDNA synthesis
Isolation of total RNA from fresh blood samples collected on ethylenediamine tetraacetic acid (EDTA) tubes was performed by Qiagen® miRNeasy Mini Kit. (Cat. No. 217004) according to kit protocol. The purity and quantity of RNA was done by Nanodrop Spectrophotometer. After RNA extraction, RNA was reverse transcribed to complementary DNA (cDNA) using High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems, USA) in accordance with the kit’s instructions. The reaction was programmed as follows; 10 min at 25 °C, 120 min at 37 °C, 5 min at 85 °C. Resultant cDNA was stored for further usage in RT-qPCR at − 20 °C.
Real-time quantitative PCR
RT-qPCR was performed on Rotor Gene Q PCR system (QIAGEN, Germany). Maxima SYBR Green qPCR Master Mix (2X) kit was used (Thermo Scientific, Cat. No. K0251), and for an endogenous control, Glyceraldehyde 3-phosphate dehydrogenase (GADPH) was employed.
Specific primers used for DANCR and GADPH were;
-
DANCR forward primer: 5’-AGCTGCCTCAGTTCTTAGCG-3’
-
DANCR reverse primer: 5’-CATGGTGATGTGCAAAGCGG'-3
-
GADPH forward primer: 5’-GAAGGTGAAGGTCGGAGTCAAC-3’
-
GADPH reverse primer: 5’-CAGAGTTAAAAGCAGCCCTGGT -3’.
The following were pipetted into each reaction tube; 10 μl Maxima SYBR Green qPCR Master Mix (2X), 1 μl forward Primer (50 pmol), 1 μl reverse primer (50 pmol), 6.5 μl nuclease free water, 1.5 μl cDNA (~ 75 ng/reaction) and no ROX. Each sample was carried out in duplicates. In each run, a no template control was done. RT-qPCR was programmed for an initial activation cycle of 50 °C for 2 min then 95 °C for 10 min; followed by 40 cycles of denaturation at 95 °C for 15 s, annealing at 55 °C for DANCR and GAPDH for 30 s and extension at 72 °C for 30 s.
For PCR products, a melting curve was done to ensure specificity and identity. The relative quantification approach (RQ = 2–ΔΔCT) was used to determine the fold change between a sample and a normal control for DANCR [24]. Results were analyzed using Rotor-Gene Q Software 2.3.4.3.
Statistical analysis of the data
Data was analyzed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp). Numbers and percentages were used to illustrate categorical data. To compare between AML patients and healthy controls, the chi-square (χ2) was used. For continuous data, they were tested for normality by the Kolmogorov- Smirnov test. Range (minimum and maximum), mean, standard deviation and median were used to express quantitative data. For comparing normally distributed quantitative data between two groups, Student t-test was used. On the other hand, for comparing not normally distributed quantitative data between two groups, Mann Whitney test was used. For correlation between two markers that are not normally distributed, Spearman coefficient was used. To analyze whether DANCR expression was associated with AML FAB subtypes or cytogenetics or prognosis, AML patients were divided into two groups based on the median value into low and high DANCR expression and the relationship was analyzed by χ2 test. Receiver operating characteristic (ROC) curve was used to determine the diagnostic performance of DANCR, with an area under the curve (AUC) more than 50% gives acceptable performance and AUC about 100% is the best performance for the test. Significance of the acquired results was assessed at the 5% level, and a p value ≤ 0.05 was considered statistically significant.
Results
Demographic characteristics of the studied groups were shown in Table 1. In the current study, there were no statistically significant differences regarding gender and age distribution (p = 0.058, p = 0.309 respectively). Complete blood count of the two studied groups is shown in Table 1. BM blasts at diagnosis ranged from 28 to 97% with a median of 78%.
FLT3-ITD mutation was absent in 59 (98.3%) patients, while NPM1 mutation was absent in 56 (93.3%) patients. 28 patients were CN-AML, 13 patients were cytogenetically abnormal of variable chromosomal abnormalities and in 19 patients no metaphase chromosomes were acquired, and thus excluded from risk stratification. Response to treatment was variable, 12 patients showed complete remission, 3 patients showed partial remission. 19 patients were refractory to treatment, while 19 patients died. 7 patients were lost during follow-up (Table 2). By assessing DANCR expression, we found that DANCR expression in AML patients ranged from 0.07 to 6.09 and was significantly lower in AML patients with a median of 0.64 than in the control group which ranged from 0.2 to 5.68 with a median of 1.02 (p = 0.038) (Table 1).
Correlation between lncRNA DANCR expression and patients’ age, gender, FAB subtypes, cytogenetics and response to treatment
AML patients were divided into two groups based on the median value (0.64) into low DANCR expression group [n = 30] and high DANCR expression group [n = 30] (Table 3). DANCR expression was significantly associated with FAB subtypes (p ≤ 0.05). However, there was no significant relationship between DANCR expression with other features as age, gender, cytogenetics or response to treatment.
Since the majority of AML M1 subtype patients showed high DANCR expression, further analysis of M1 subtype with high DANCR [n = 16], was done to compare their response to treatment with the remaining AML patients with low DANCR [n = 30]. AML patients of M1 subtype with high DANCR (above 0.64) were significantly less refractory to treatment and thus less resistant to cytarabine, whereas AML patients of different subtypes with low DANCR expression (below 0.64) were more refractory to treatment and therefore resistant to cytarabine (Table 4).
Comparison between FAB subtypes M0, M1 and M2, with M4 and M5 AML patients and healthy controls in relation to DANCR expression
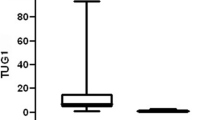
To investigate the relation between FAB subtypes and DANCR expression, we further grouped AML patients into immature M0, M1 and M2 subtypes into one group and a second group with the more differentiated M4 and M5 subtypes. Relative expression of DANCR was significantly lower in M4 and M5 subtypes [n = 34] compared to M0, M1 and M2 subtypes [n = 26] (p < 0.001), as well as compared to the control group [n = 30] (p < 0.001). M4 and M5 group had a median value of 0.53 and expression was ranging from 0.07 to 3.17, while M0, M1 and M2 group had a median value of 1.19 and levels were ranging from 0.11 to 6.09. However, there was no significant difference between AML patients of M0, M1 and M2 subtypes and controls (p = 0.808) (Fig. 1).

DANCR expression in different FAB subtypes and healthy controls
Comparison between cytogenetically normal AML patients and healthy control group in relation to DANCR expression
DANCR expression in CN-AML patients included in our study [n = 28] was compared to controls [n = 30], and DANCR expression was significantly lower in CN-AML patients with a median of 0.58 and expression ranging from 0.11 to 1.98 (p = 0.011).
Comparison between AML patients with abnormal cytogenetics and healthy control group in relation to DANCR expression
DANCR expression in AML patients with abnormal cytogenetics [n = 13] was compared to controls [n = 30], and there was no significant difference between the two groups, where AML patients with abnormal cytogenetics had a median of 0.75 and expression ranging from 0.12 to 6.09 (p = 0.397).
Comparison between intermediate risk AML patients and high-risk patients in relation to DANCR expression
DANCR expression in intermediate risk patients [n = 33] was compared to high-risk patients [n = 7], and there was no significant difference in DANCR expression. (p = 0.337).
Correlation between DANCR expression in AML patients with BM blasts at diagnosis and WBCs count
There was no significant correlation between DANCR expression and percentage of BM blasts at time of diagnosis (rs = -0.084, p = 0.523), as well as WBCs count of AML patients (rs = -0.091, p = 0.489).
Diagnostic value of DANCR in AML patients
ROC curve and AUC were used to investigate DANCR as a potential marker of AML on data from all subjects. The ROC curve showed separation between AML patients [n = 60] and healthy individuals [n = 30] with an AUC of 0.635 at the cut off value of ≤ 0.917, sensitivity was 71.67% and specificity was 63.33% (95% CI: 0.512 – 0.757, p = 0.038) (Fig. 2a). ROC curve also showed strong separation between AML patients of M4 and M5 subtypes [n = 34] and healthy controls [n = 30] with AUC of 0.758 at the cut off value of ≤ 0.917; the sensitivity was 94.12% and specificity was 63.33% (95% CI: 0.634 – 0.883, p < 0.001) (Fig. 2b). In addition, ROC curve was used to discriminate AML patients of M 0, M1 and M2 subtypes [n = 26] from AML patients of M4 and M5 subtypes [n = 34] and showed separation between both groups at the cut off value of ≤ 0.886 with an AUC of 0.764; sensitivity was 91.18% and specificity was 61.54% (95% CI: 0.632 – 0.897, p < 0.001) (Fig. 2c). ROC curve was also applied to discriminate between CN-AML patients [n = 28] and healthy controls [n = 30] and showed a separation with AUC of 0.707 at the cut off value of ≤ 0.917; sensitivity was 85.71% and specificity was 63.33% (95% CI: 0.570 – 0.843, p = 0.007) (Fig. 2d).

ROC curve for diagnostic value of DANCR for; a differentiating AML patients [n = 60] from healthy controls [n = 30], b for differentiating M4 and M5 subtypes [n = 34] from heathy controls [n = 30], c for differentiating M4 and M5 subtypes [n = 34] from M0, M1 and M2 subtypes [n = 26] and d for differentiating CN-AML patients from healthy controls
Discussion
In the current study, we assessed the expression of lncRNA DANCR in AML patients as well as healthy volunteers, where DANCR expression varied among patients with a significantly lower median than that of the control group. In previous studies regarding DANCR in AML, Bill et al. found that DANCR expression was upregulated in adult CN-AML patients when compared to controls and demonstrated that DANCR may have a role in regulation of leukemic stem cells through the regulation of WNT pathway by using animal models with AML expressing both MII partial tandem duplication/FLT3-ITD [25]. However, in this study DANCR expression was significantly downregulated in CN-AML patients. We might speculate the difference may be due to the absence of FLT3-ITD mutation in the majority of the patients (98.3%) included in the current study. Another reason may be due to differences in AML subtypes included in each study as in this study DANCR showed significant difference in expression among different AML subtypes.
Patients were further classified according to FAB criteria [3] into two groups and DANCR expression in M0, M1 and M2 subtypes was compared to M4 and M5 subtypes (no M6 patients were tested in the present study) and to the control group. DANCR was found to be significantly downregulated in M4 and M5 subtypes compared to M0, M1 and M2 subtypes and compared to the control group. However, there was a non-significant increment in DANCR expression in M0, M1 and M2 subtypes compared to the controls.
By further analyzing 16 patients in M1 subtype with higher level of DANCR and comparing them to other AML subtypes with lower DANCR expression regarding response to treatment, M1 subtype with higher DANCR expression showed less chemoresistance to cytarabine. However, Zhang et al., showed that treating cultured AML cell lines and primary AML cell lines isolated from newly diagnosed pediatric patients with cytarabine was associated with dose dependent elevation in DANCR expression, where DANCR overexpression was associated with cytarabine resistance, while its knockdown diminishes cytarabine resistance [26]. Thus, DANCR relation to cytarabine resistance may be different in adult AML.
A study by Zhang et al., on papillary thyroid cancer, showed that DANCR was downregulated in cancerous tissue compared with adjacent cancer-free healthy tissue [22]. It was suggested that DANCR may act as a tumor suppressor rather than an oncogenic lncRNA. An explanation might be provided by a study in breast cancer by Li et al., which demonstrated that DANCR acts as a tumor suppressor by controlling the epithelial mesenchymal transition (EMT) pathway and cancer metastasis through attaching to enhancer of zeste homolog 2 (EZH2) and promoting its subsequent phosphorylation and degradation [21]. A study in osteoblasts by Zhu et al., found that DANCR interaction with EZH2, decreased the expression of runt-related transcription factor 2 gene (Runx2) [27], where Runx2 was found to be upregulated in AML [28].
Although many studies showed that DANCR acts as an oncogene that is overly expressed in cancers and promotes tumor invasion [29], DANCR was downregulated in papillary thyroid cancer [22] and multiple myeloma [30] and renal cell carcinoma [31]. Moreover, DANCR induction in-vitro was proved to inhibit tumor invasion and metastasis in cancers as multiple myeloma [30] breast cancer [32] and non-small cell lung cancer [33]. Thus, DANCR may hold a therapeutic potential where increasing DANCR expression in human cancers may prevent tumor progression and invasion.
Furthermore, in our study, the diagnostic value of DANCR was tested and multivariable logistic analysis indicated that DANCR could discriminate AML patients from the control group with a sensitivity of 71.67%. This sensitivity increased to 94.12% when DANCR was used to discriminate between M4 and M5 subtypes of AML from the control group.
To the best of our knowledge, this is the first study to evaluate DANCR expression in different AML FAB subtypes, a classification that is surpassed by WHO classification. However, varying expression of lncRNA DANCR among different FAB subtypes might highlight the role played by the predominate leukemic cells in each subtype in AML pathogenesis.
In conclusion, DANCR expression was downregulated in patients which might suggest that DANCR has a tumor suppressor function in AML. DANCR was also significantly downregulated in M4 and M5 subtypes compared to M0, M1 and M2 subtypes; and AML M1 patients who showed higher DANCR expression were less resistant to cytarabine. However, there was no relation found between DANCR expression and age, sex, WBCs, and BM blasts count. Further research is recommended on AML patients with FLT3-ITD mutations as well as NPM1 mutations to further elucidate the role of DANCR in the presence of these mutations. Research is also recommended to further verify DANCR relation to EZH2 and Runx2, which are highly implicated in AML but were not correlated with DANCR in AML patients.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AML:
-
Acute myeloid leukemia
- AUC:
-
Area under curve
- BM:
-
Bone marrow
- cDNA:
-
Complementary deoxyribonucleic acid
- CI:
-
Confidence interval
- CN-AML:
-
Cytogenetically normal acute myeloid leukemia
- DANCR:
-
Differentiation antagonizing non-protein coding RNA
- EDTA:
-
Ethylenediamine tetraacetic acid
- ELN:
-
European Leukemia Net
- EMT:
-
Epithelial Mesenchymal transition
- EZH2:
-
Enhancer of zeste homolog 2
- FAB:
-
French American British
- FLT3-ITD:
-
FMS-like tyrosine kinase 3 internal tandem duplication
- GADPH:
-
Glyceraldehyde 3-phosphate dehydrogenase
- lncRNA:
-
Long non-coding ribonucleic acid
- ncRNA:
-
Non-coding ribonucleic acid
- NPM1:
-
Nucleophosmin
- ROC:
-
Receiver operating characteristic
- RT-qPCR:
-
Real time quantitative polymerase chain reaction
- Runx2:
-
Runt related transcription factor 2
- rs :
-
Spearman coefficient
- WBC:
-
White blood cell
References
Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM (2019) Epidemiology of acute myeloid leukemia: recent progress and enduring challenges. Blood Rev 36:70–87
Miraki-Moud F, Anjos-Afonso F, Hodby KA et al (2013) Acute myeloid leukemia does not deplete normal hematopoietic stem cells but induces cytopenias by impeding their differentiation. Proc Natl Acad Sci 110(33):13576–13581
Bennett JM, Catovsky D, Daniel MT et al (1976) Proposals for the classification of the acute leukaemias. French-American-British (FAB) co-operative group. Br J Haematol 33(4):451–8
Khoury JD, Solary E, Abla O, et al (2022) The 5th edition of the World Health Organization classification of haematolymphoid tumours: myeloid and histiocytic/dendritic neoplasms. Leukemia 36(7):1703–19
Romer-Seibert JS, Meyer SE (2021) Genetic heterogeneity and clonal evolution in acute myeloid leukemia. Curr Opin Hematol 28(1):64
Ley TJ, Miller C, Ding L et al (2013) Genomic and epigenomic landscapes of adult de novo acute myeloid leukemia. N Engl J Med 368(22):2059–2074
Konstandin NP, Pastore F, Herold T et al (2018) Genetic heterogeneity of cytogenetically normal AML with mutations of CEBPA. Blood Adv 2(20):2724–2731
Liu H (2021) Emerging agents and regimens for AML. J Hematol Oncol 14(1):49
Ponting CP, Oliver PL, Reik W (2009) Evolution and functions of long noncoding RNAs. Cell 136(4):629–641
Chi Y, Wang D, Wang J, Yu W, Yang J (2019) Long non-coding RNA in the pathogenesis of cancers. Cells 8(9):1015
Nandwani A, Rathore S, Datta M (2021) LncRNAs in cancer: regulatory and therapeutic implications. Cancer Lett 501:162–171
Taniue K, Akimitsu N (2021) The functions and unique features of LncRNAs in cancer development and tumorigenesis. Int J Mol Sci 22(2):632
Pan L, **ao X, Zhao Y et al (2020) The functional roles of long noncoding RNA DANCR in human cancers. J Cancer 11(23):6970
Mao Z, Li H, Du B, et al. (2017) LncRNA DANCR promotes migration and invasion through suppression of lncRNA-LET in gastric cancer cells. Biosci Rep 37(6):1–10
Yu JE, Ju JA, Musacchio N, Mathias TJ, Vitolo MI (2020) Long noncoding RNA DANCR activates Wnt/β-catenin signaling through MiR-216a inhibition in non-small cell lung cancer. Biomolecules 10(12):1646
Li J, Zhou L (2018) Overexpression of lncRNA DANCR positively affects progression of glioma via activating Wnt/β-catenin signaling. Biomed Pharmacother 102:602–607
Liu Y, Zhang M, Liang L, Li J, Chen Y-X (2015) Over-expression of lncRNA DANCR is associated with advanced tumor progression and poor prognosis in patients with colorectal cancer. Int J Clin Exp Pathol 8(9):11480
Sx Y, Wang J, Yang F et al (2016) Long noncoding RNA DANCR increases stemness features of hepatocellular carcinoma by derepression of CTNNB1. Hepatology 63(2):499–511
Tian W, Lei N, Guo R, Yuan Z, Chang L (2020) Long non-coding RNA DANCR promotes cervical cancer growth via activation of the Wnt/β-catenin signaling pathway. Cancer Cell Int 20(1):1–12
Thin KZ, Liu X, Feng X, Raveendran S, Tu JC (2018) LncRNA-DANCR: a valuable cancer related long non-coding RNA for human cancers. Pathol Res Pract 214(6):801–805
Li Z, Hou P, Fan D et al (2017) The degradation of EZH2 mediated by lncRNA ANCR attenuated the invasion and metastasis of breast cancer. Cell Death Differ 24(1):59–71
Zhang K, Lv J, Peng X, et al (2019) Down-regulation of DANCR acts as a potential biomarker for papillary thyroid cancer diagnosis. Biosci Rep 39(4):1–8
Döhner H, Estey E, Grimwade D et al (2017) Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 129(4):424–447
Livak KJ, Schmittgen TD (2001) Analysis of relative gene expression data using real-time quantitative PCR and the 2− ΔΔCT method. Methods 25(4):402–408
Bill M, Papaioannou D, Karunasiri M et al (2019) Expression and functional relevance of long non-coding RNAs in acute myeloid leukemia stem cells. Leukemia 33(9):2169–2182
Zhang H, Liu L, Chen L, Liu H, Ren S, Tao Y (2021) Long noncoding RNA DANCR confers cytarabine resistance in acute myeloid leukemia by activating autophagy via the miR-874-3P/ATG16L1 axis. Mol Oncol 15(4):1203–1216
Zhu L, Xu P-C (2013) Downregulated LncRNA-ANCR promotes osteoblast differentiation by targeting EZH2 and regulating Runx2 expression. Biochem Biophys Res Commun 432(4):612–617
Sun C-C, Li S-J, Chen Z-L, Li G, Zhang Q, Li D-J (2019) Expression and prognosis analyses of runt-related transcription factor family in human leukemia. Mol Ther Oncolytics 12:103–111
Wang M, Gu J, Zhang X, Yang J, Zhang X, Fang X (2021) Long Non-coding RNA DANCR in Cancer: Roles, Mechanisms, and Implications. Front Cell Dev Biol 9:1–18
Wu L, **a L, Jiang H et al (2021) Long non-coding RNA DANCR represses the viability, migration and invasion of multiple myeloma cells by sponging miR-135b-5p to target KLF9. Mol Med Rep 24(3):1–12
** L, Fu H, Quan J et al (2017) Overexpression of long non-coding RNA differentiation antagonizing non-protein coding RNA inhibits the proliferation, migration and invasion and promotes apoptosis of renal cell carcinoma. Mol Med Rep 16(4):4463–4468
Li Z, Dong M, Fan D et al (2017) LncRNA ANCR down-regulation promotes TGF-β-induced EMT and metastasis in breast cancer. Oncotarget 8(40):67329–67343
Wang S, Lan F, **a Y (2018) lncRA ANCR inhibits non-small cell lung cancer cell migration and invasion by inactivating TGF-β pathway. Med Sci Monit 24:6002–6009
Funding
No funding was received by the authors for conducting this study.
Author information
Authors and Affiliations
Contributions
All authors contributed equally to the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted using human blood samples and approved by the Ethics Review Board of the Alexandria University, Faculty of Medicine in January 2021 under number 0201437.
Informed consent was obtained from each subject included in this study upon sample withdrawal.
Consent for publication
Available consent for publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rasheed, N.M., Nounou, H.A., Eltabakh, S.M. et al. Assessing the expression of differentiation antagonizing non-protein coding RNA (DANCR) in newly diagnosed Egyptian acute myeloid leukemia patients. Egypt J Intern Med 35, 66 (2023). https://doi.org/10.1186/s43162-023-00251-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-023-00251-y