
Abstract
Background
The results of recent systematic reviews have concluded that most exercise types are more effective than minimal treatment for improving outcomes in the management of non-specific chronic low back pain. However, exercise prescriptions are criticised for being prescribed without a clear rationale and with a high level of uncertainty. The preferred mode of exercise in this population is not outlined in clinical guidelines. The objective of this review is to describe the indications and dosimetry for the most common exercise interventions prescribed.
Methods
Literature was sourced from searches of MEDLINE, CINAHL, SPORTDiscus, and PEDro databases until October 2021 using descriptors related to pain, exercise, and prescription, totaling 33 articles that fulfilled the inclusion and exclusion criteria. The first author independently selected studies and extracted data on study characteristics of interest. Any doubts were resolved through discussion with the other reviewers.
Results
The results of the review showed that a baseline assessment comprising the patient’s pain, thoughts, beliefs, and behaviours concerning physical activity or exercises may be undertaken, and specific exercises may be prescribed based on the indication to reduce pain, allay fear, or re-educate neuromotor control.
Conclusion
Based on the heterogeneity in the understanding, administration, and progression of exercises and the sub-optimal or poor reporting of exercise prescriptions or dosages and outcomes reported, we conclude that it may not be possible to synthesise any evidence to inform precision exercise prescription for CLBP. Future studies should be of higher quality for the development of effective exercise programmes.
Similar content being viewed by others


Introduction
Numerous studies acknowledge that chronic low back pain (CLBP) has a complex nature, with many biological, social, and psychological elements influencing the problem, and should not be viewed as a homogeneous condition [1]. Healthcare professionals classify patients with low back pain (LBP) into specific spinal pathology, radicular syndromes, or non-specific LBP using diagnostic triage [2]. Develo** fundamental general rehabilitation therapy approaches that would apply to all or even most LBP subgroups is impossible due to this heterogeneity. Researchers have categorised biological pain mechanisms into nociceptive, nociplastic, and neuropathic [3], and they have expanded research to include psychological and movement system dysfunction [4]. Researchers classify more than 90–95% of the population as suffering from non-specific LBP, when there is no evidence of tissue pathology [5]. Researchers roughly equate the label non-specific LBP to ‘nociplastic pain’ [6].
Current treatment guidelines recommend that individuals suffering from CLBP avoid bed rest and fear of movement and return to normal activity. The clinical and research communities agree that addressing cognitive, emotional, psychological, behavioural, physical, and social factors is necessary in managing CLBP [7]. Systematic reviews and meta-analyses consistently show that engaging in exercise can reduce pain and improve functional outcomes among people with CLBP compared to receiving no treatment, standard care, or other conservative therapies in the short term [8,9,10]. Furthermore, studies have shown that exercises influence all the different types of pain mechanisms [11, 12].
In broad terms, exercises involve performing a series of specific movements at a set intensity and duration with the goal of promoting physical health [13]. Neuromuscular, psychological, neurophysiological, cardiometabolic, and tissue healing mechanisms attribute the positive effects of exercises [14]. Clinicians attempted to evaluate the individual effects of different types of exercise interventions, such as aerobic, strengthening, directional, aquatic, Pilates, yoga, core stabilisation, and motor control exercises, on improving outcomes in people with CLBP. Their modes of operation fundamentally differ. Physiology principles are used to devise some exercises (e.g., aerobic), while concepts (e.g., directional) form the basis of others. The results show mixed effectiveness, and studies have not found an ideal exercise programme for patients with CLBP [15]. A systematic review of systematic reviews found that different exercise types have varying effects on pain and disability in CLBP, and there is no significant difference between them [16]. A combination of approaches is suggested by a few articles [17], while other studies propose considering individuals’ personal needs, preferences, and capabilities when selecting the appropriate form of exercise [18]. The Canadian guidelines emphasise incorporating low-intensity exercises [19], while the French and German guidelines advocate continuing regular physical activities [20, 21]. On the other hand, the American College of Occupational and Environmental Medicine and the North American Spine Society consistently and emphatically endorse including aerobic exercise [22, 23]. Another literature review attempted to provide insights about exercise prescription [24], but it did not specifically customise the exercise prescription for people with CLBP.
Many experts widely consider exercise therapy as the first-line care for managing CLBP. However, the active ingredient of exercise programmes is still largely unknown [25]. Clinicians might use international guidelines and the findings of systematic reviews and meta-analyses to assist them in selecting interventions. However, when converting the evidence into recommendations for clinical practise, they only consider the effectiveness of the interventions. Facilitating replications of exercises requires a complete exercise prescription in all aspects. Yet, healthcare professionals are prescribing exercises for people with CLBP without a clear rationale and with a high level of uncertainty. Furthermore, many critics have widely criticised the recommendation of general exercises, which mostly consist of a combination of muscular strength, flexibility, and aerobic fitness, instead of targeted therapies [26]. Furthermore, despite many people calling for activity assessment and exercise prescription to be considered standard parts of the disease treatment and prevention paradigm [27], the clinical guidelines for CLBP do not give concrete directions regarding exercise prescription. To choose the best exercises or determine the dosages and methods for prescribing them to people with CLBP, we need to consolidate and synthesise the findings of earlier studies on exercise therapy due to these restrictions and issues. The overarching goal of this review is to offer a framework for clinicians to use when prescribing exercise to people with CLBP while taking into account the unique characteristics and challenges present in this population.
Methods
The objective of the review is to systematically categorise, elucidate, examine, and assess all accessible data pertaining to the indications and prescription of diverse exercises across various types of studies. Given the diverse clinical components encompassed by patient/population, intervention, comparison, and outcomes (PICO), the incorporation of both randomised controlled trials and non-randomised studies, as well as the inclusion of studies examining continuous and binary outcome measures, a narrative review was deemed an appropriate approach to address this research inquiry. In the context of this study, exercise therapy is regarded as an intervention that can be implemented by physiotherapists and other healthcare professionals and is operationally defined as a structured regimen of physical exercises specifically designed and prescribed to achieve specific therapeutic objectives.
Search strategy
An electronic search of MEDLINE, CINAHL, SPORTDiscus, and PEDro databases was conducted for research published during any time period until October 2021 using Medical Subject Headings (MeSH) for ‘pain’ AND ‘exercise’ AND ‘prescriptions’. The ‘OR’ search terms used for MeSH keywords are presented in Table 1 and were combined with ‘AND’ and searched in ‘All Fields’. The same method was extended to other databases. The search strategies employed for PubMed and PEDro databases are presented in Additional file 1. We also conducted manual searches on the reference lists of primary articles found from initial searches and previously published systematic reviews identified on the Cochrane Database of Systematic Reviews (search terms: chronic back pain exercise; limits: none).
The abstracts and titles obtained from the search technique were examined by two authors (SG and ARK) in a separate and unbiased manner. Both authors then used the predetermined inclusion and exclusion criteria to all the abstracts. The complete text of the paper was acquired in cases where the abstract appeared to meet the specified requirements or when the eligibility of the study was uncertain. The two authors individually collated and examined all full-text publications based on the established criteria for inclusion. The authors resolved any issues through the process of the discussion and arrived at a consensus. In the event of persistent differences, a third author was consulted.
Selection procedure
To be considered for the review, studies should have been published in English in a peer-reviewed journal. The other criteria followed the PICO framework, Population: adults ≥ 18 years old with CLBP of minimum more than a 3-month duration; Interventions: selected interventions satisfying the definition of exercise therapy as described above; Comparators: not applicable; Outcomes: any one of the below: pain, strength, endurance, fear avoidance; Study design: any; Length of follow-up: any. Studies were excluded if the population group comprised participants with symptomatic LBP such as conditions associated with pregnancy, infection, tumour, osteoporosis, fracture, structural deformity (e.g., scoliosis), inflammatory disorder, or cauda equina syndrome. Studies that included participants before or after surgery were also disqualified. Similarly, grey literature and articles published as conference abstracts, letters to the editor, and non-peer works were not considered. The exercises should have been categorised as spinal stability, motor control, Pilates, McKenzie therapy, general strengthening, aerobic stretching, or quota-based exercises. These exercises were chosen based on the popularity of these exercises in the authors’ place of practice. The articles should not have evaluated mixed interventions, i.e., combinations of aerobics and strengthening, aerobics, and flexibility, or interventions apart from specified exercises, e.g., psychological or non-physiotherapy-specific interventions. Studies were only taken into consideration for the final review if they met all the inclusion and exclusion criteria, including mentioning the indication or prescription of exercises, rather than just looking at the effectiveness of the various exercise types taken into consideration in this review in people with CLBP.
Data extraction
One of the authors who performed the screening (SG) independently conducted the data extraction. Data were extracted onto a standardised form. The following data were extracted from the studies: (1) study population; (2) characteristics of the interventions: theoretical rationale (indication or prescription for exercises, schedule, type, frequency, intensity, and duration). In addition, we also extracted post-treatment follow-up points and the outcome measures used to evaluate the interventions, as well as whether clinical or statistical significance was noted. When there were discrepancies, a consensus was reached within the research group.
Results
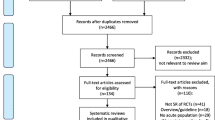
There were 1165 results from searches. 121 full-text evaluations were completed following the screening of abstracts and titles. Based on the inclusion and exclusion criteria, we were able to focus on 67 studies, of which 33 met our criteria for selection. The PRISMA flowchart is shown in Fig. 1.

PRISMA flow diagram of the search process for studies examining the indications and dosimetry for the most common exercise interventions prescribed in patients with CLBP
Study indings
The study findings may be broadly classified into two major headings:
-
Objectives of exercises and need for assessment
-
Common exercises prescribed
Objectives of exercise and need for assessment
Out of the 33 publications included in the analysis, one study examined the utilisation of goal-setting strategies that were centred on achieving functional outcomes by pacing up activity levels; this may help to indirectly reduce pain. This is important, as failure to reduce pain with exercises can lead to disability [28]. Another study focused on exploring the thoughts, beliefs, and behaviours components of patients in order to address the intricate process of prescribing exercise for CLBP [29]. As patients’ who exhibit positive yellow flags are candidates at risk of progression to chronic disability, graded exposure and supervision may be required to identify the limits of activities and exercises that can be safely initiated without increasing symptoms. Several studies have documented exercise prescription strategies that are guided by the categorisation of pain. A region-specific exercise may be chosen when the pain is driven by nociceptors, and patients with nociplastic and neuropathic pain may be prescribed generalised exercises such as aerobics [30,31,32].
Common exercise prescribed
Exercise encompassed strengthening exercises (n = 5), fear avoidance/quota based exercises (n = 3), direction-specific exercises (n = 4), core stability (n = 5), motor control exercises (n = 2), pilates (n = 4), and others (n = 5). As the theoretical rationale behind the prescription of these exercises, including the dosages, has not been addressed completely by these studies, and the heterogeneous principles underlying these exercises, it was not possible to synthesise the findings of the review. Therefore, the results are presented individually.
Strengthening exercises
Typically, the exercises aimed at enhancing strength mostly focus on the extensor muscles situated in the thoracic, lumbar, and posterior hip areas, commonly referred to as ‘posterior chain resistance training’ [32]. Individuals who do not have any cardiovascular or orthopaedic contraindications to resistance exercises and possess the ability to independently manage their own well-being are recommended to engage in strengthening exercises [33]. When advised, it is recommended to do these exercises with a complete range of motion and at a higher level of intensity [34]. It is recommended to perform eight to 12 repetition maximum (RM) each set once or twice per week. It was observed that there were no significant differences in repeating the exercises once or three times per week [35]. Individuals who have been diagnosed with spinal anomalies or structural deformities, as well as those with disc protrusions or herniations, are generally deemed unsuitable candidates for engaging in posterior chain exercises [36].
Fear avoidance/quota-based exercises
The use of graded or quota-based workouts is recommended in situations where the primary goal is to discourage sickness behaviours and aid in the process of fear desensitisation [37]. The implementation of exercises targeting activities that pose challenges for the patient is commenced with low-intensity levels, gradually advanced over time to enhance the patient’s capacity to engage in those activities, and are integrated into individuals’ regular routines and activities. The participants are required to completely fulfil the predetermined daily quotas of exercises [38], and the symptoms experienced by the participants do not impose any restrictions on the activities that can be undertaken. Positive reinforcement has been found to decrease the anxiety that is linked to movement and activities [39].
Direction-specific exercises (McKenzie)
Patients who demonstrate the centralization phenomenon of back pain are commonly recommended McKenzie exercises. Centralization is the process by which distal referred pain is gradually eliminated, with the pain eventually becoming localised at the midline of the body. In the McKenzie Method exercises, patients’ are classified into posture, dysfunction, and derangement sub-types, and sustained postures or repeated movements, along with an educational component and postural training [40, 41], are prescribed based on the patient’s responses to a clinical examination of posture and range of motion of the spine. The exercises are progressed either based on the concept of ‘progression of forces’ or the use of ‘alternative forces’ and the choice of self-overpressure, manual mobilisation, or ‘patient movement in a greater range of motion with extra pressure applied by the therapist’ [42]. Though there is no consensus regarding the optimal number of sessions for the McKenzie method, 3 sets of 10 repetitions that could be performed on the same day or at different times of day depending on the patient’s availability are recommended [43].
Core stability exercises
The prescription of core stability exercises is based on the concept that CLBP occurs because of the decrease in spinal stability due to delayed or decreased activation of the lumbar multifidi and transversus abdominus [44, 45]. Core muscle strengthening is intended to increase spinal stability and neuromuscular control around the lumbopelvic region [46] by training the localised stabiliser muscles. Variables that were found to accurately predict the candidates who are more likely to improve with lumbar stabilisation exercises are (1) age less than 40 years, (2) average straight leg raise of 91° or greater, (3) the presence of aberrant lumbar movement, and (4) a positive prone instability test [47]. For optimal success, evidence recommends 20–30 min per session, three to five times a week [48].
Motor control exercises
Motor control exercises use the principles of segmentation and simplification to train control and coordination of the spine and pelvis based on the movement and muscle activation patterns of the superficial and deep trunk muscles [49, 50]. The patient is assumed to have learned proper activation if they are able to maintain contractions of the muscles for 10 repetitions of 10 s while maintaining optimal posture and normal respiration [51]. Feedback is provided when required. The exercises are progressed by incorporating these contractions in functional static and dynamic activities [50] based on patient’s fatigue, pain thresholds, or observed movement control.
Pilates
In this method, isometric contraction of the transversus abdominis, perineal, gluteal, and multifidus muscles is performed without any postural compensation while maintaining diaphragmatic breathing. On average, 10 repetitions of 15 to 20 exercises are performed per session, and the exercises are performed at 3 difficult levels: basic, intermediate, and advanced, according to individual needs [51] and pain. For optimal outcomes, interventions have to be performed for 30–60 min at least twice per week [52]. A Delphi study has indicated that persons with CLBP with maladaptive movement patterns, a lack of body awareness, fear avoidance behaviour, weak lumbar stabilisers, and poor breathing patterns are ideal candidates for Pilates [53]. Another study indicated individuals with a total trunk flexion range of motion (ROM) of 70° or less, a duration of 6 months or less, symptoms not radiating to the leg, a body mass index of 25 kg/m2 or more, and a hip rotation ROM of 25° or more would benefit better from Pilates-based exercise [54].
Others
As chronic pain may result in facilitation (increased) muscle tension [55], interventions that induce relaxation, such as stretching, may be considered in the presence of muscle spasms or motor facilitation. End-range loading exercises may be prescribed for patients with radicular low back pain whose symptoms extend below the buttocks and who exhibit centralization and peripheralization of symptoms on repeated movement testing [56]. When patients have been assessed to receive general exercises, a choice can be provided to select the type of aerobic exercises they would enjoy to ensure exercise adherence (walking, stationary cycling, or swimming). Patients may be asked to work at moderate exercise intensity for optimal benefits. For example, trials have shown that exercises lasting 20–30 min twice or three times a week may be adequate to induce exercise-induced analgesia in patients with chronic pain [57].
Promoting physical activity as an intervention for people with CLBP looks vague at this point in time, as the relationship between physical activity and the risk of CLBP is unclear. While some studies relate too little or too much physical activity as a risk factor for CLBP [58], other works reveal no association between physical activity and a sedentary lifestyle with CLBP [59].
Discussion
Many reviews and clinical practice guidelines have recommended exercise programmes to reduce pain and disability [60]. An exercise prescription is a physical activity plan created in a systematic and individualised way according to the FITT-VP (frequency, intensity, time, type, volume, and progression) principle. We could not find many studies that prescribed exercise to people with CLBP in accordance with the aforementioned criteria. Instead of determining whether individuals were appropriate for the selected exercises, many of the studies we analysed randomly assigned participants to one of the studied interventions. The fact that many of the trials have studied the effects of integrated flexibility, strength, and aerobic training may limit drawing firm conclusions from the results. Additionally, very few trials have compared exercise programmes at different dosages.
Baseline assessments form the basis of traditional exercise prescriptions. Critics argue that these assessments do not measure true physical performance and are influenced by the patient’s psychological status [61]. Studies have not reported any association between muscle endurance and pain or disability [47], postural control and the persistence of chronic LBP symptoms [62], or pain and deconditioning [63]. Therefore, it is unclear whether exercises should target improvement in strength-loaded or mobility-unloaded positions.
The overall findings of this review do not allow for the synthesis of any evidence regarding precision prescription. Studies have found that exercises reduce pain and disability in people with CLBP without changing physiological measures such as strength, endurance, or flexibility [64]. Prescribing active exercise therapies as an effective treatment for CLBP may be done due to their potential for improving pain, physical function, muscle strength, and mental health, as there is limited evidence to support the prescription of one type of exercise over another based on indications. For example, previous studies have shown that exercise programmes that target strength and movement are equally effective [65]. While studies have conducted abundant literature on the efficacy of strength training [10, 66], they have found mixed support for aerobic exercises [67]. A systematic analysis of 43 clinical trials concluded that interventions involving muscle strengthening showed significantly greater efficacy in promoting functional improvements compared to other active approaches [68]. A network meta-analysis concluded that Pilates, stabilisation/motor control, resistance training, and aerobic exercise training are the most effective treatments based on low-quality evidence for the outcomes of interest [10]. Another network meta-analysis [69] concluded that Pilates, McKenzie therapy, and functional restoration were more effective than other types of exercise treatment in reducing pain and functional limitations. However, the authors recommended encouraging people with CLBP to perform the exercises they enjoy.
The Guide to Physical Therapist Practice acknowledges that categorising patients according to clusters of signs and symptoms is the major objective of the diagnostic procedure [70]. Clinicians believed that classifying patients with CLBP into homogeneous subgroups would help them to receive individualised treatment [47] and avoid the problems that arise from providing the same treatments to a group of patients with different needs. However, it is worth noting that clinicians were able to classify individuals with low back pain in fewer than 10% of cases [71], and a systematic review concluded that treatment-based subgroup analyses have low credibility [72].
Patient recruitment has been found to influence the results of exercise as a confounding factor. Studies have found that people who actively seek treatment for LBP better represent the population with LBP compared to when patients are recruited from the community [32]. Moreover, clinicians face a challenge in determining the precise number of sessions due to the observed trend of an increase in the treatment effect size with each additional exercise session [73]. Contrary to popular belief, studies have shown that higher dosages of exercises do not necessarily lead to better outcomes in musculoskeletal rehabilitation [66, 74].
Recent studies have confirmed that exercise interventions are designed to temporarily aggravate patients’ pain and symptoms, as no relationship between pain and tissue damage has been identified [75, 76]. Studies speculate that these treatments redefine the meaning of pain [77] and reduce the overall sensitivity of the central nervous system [76, 77]. Another systematic review suggested no relation between pain modulation and exercises, despite touting exercise-induced endogenous analgesia effects and activation of spinal inhibitory mechanisms as reasons for pain reduction [78, 79]. On the other hand, Van Oosterwijck et al. [80] reported dysfunction of endogenous analgesia in patients with musculoskeletal pain and recommended that patients exercise non-painful body parts [81]. When prescribing ‘exercises in pain,’ the clinician must provide an appropriate recovery period [82].
The review’s main limitation is that it only searched for selected exercises. We have another limitation in that this narrative review allowed us to highlight the state of the literature for the selected objectives, and we did not statistically weigh the included studies. However, we hope clinicians will gain an understanding of the different exercises discussed through the results of this study. The review showed a lack of large, high-quality randomised trials. The majority of the published studies were shown to have a high risk of bias [83], with suboptimal or poor reporting of exercise prescriptions or dosages [84]. A study seeking to determine the primary therapeutic objectives of exercise for CLBP concluded that exercise interventions should explicitly outline their treatment goals, which may include enhancing functionality, improving quality of life, alleviating pain, addressing patient-specific objectives, mitigating fear associated with movement [85]. Studies should further prioritise investigating the mediating effects of exercises that align with the proposed mechanisms of their action and assessing their cost-effectiveness. This will help gain a more comprehensive understanding of the underlying reasons for the efficacy of exercise in CLBP. Emerging evidence suggests that structures in the lower back can cause structural and functional alterations in the cerebral cortex, leading to CLBP [86]. Researchers may consider the neuroplastic behaviour of the nervous system in future studies and develop exercise recommendations based on cortical responses while administering exercises [87].
Conclusion
From the results of the review, it may be safely assumed that more research is required for the development of effective exercise programmes. As exercise prescriptions have the power to either build up or destroy the patient’s demonization about the relationship between pain and activity, exercise prescriptions may be carefully constructed to ensure patient adherence. If the clinicians are not confident regarding the type and dosage of exercise prescription, the approach may be based on patient preference, and patients may be permitted to self-select their dosages or may be encouraged to work at lower intensities.
Availability of data and materials
Not applicable.
Abbreviations
- CLBP:
-
Chronic low back pain
- LBP:
-
Low back pain
- PICO:
-
Patient/population, intervention, comparison and outcomes
- MeSH:
-
Medical Subject Headings
- FITT-VP:
-
Frequency, Intensity, Time, Type, Volume, and Progression
References
Abenhaim L, Rossignol M, Gobeille D, Bonvalot Y, Fines P, Scott S. The prognostic consequences in the making of the initial medical diagnosis of work-related back injuries. Spine. 1995;20:791–5.
Aina A, May S, Clare H. The centralization phenomenon of spinal symptoms–a systematic review. Man Ther. 2004;9(3):134–43. https://doi.org/10.1016/j.math.2004.03.004. (PMID: 15245707).
Alsufiany MB, Lohman EB, Daher NS, Gang GR, Shallan AI, Jaber HM. Non-specific chronic low back pain and physical activity: a comparison of postural control and hip muscle isometric strength: a cross-sectional study. Medicine (Baltimore). 2020;99(5): e18544.
American College of Sports Medicine. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41(3):687–708. https://doi.org/10.1249/MSS.0b013e3181915670. PMID: 19204579.
American Physical Therapy Association. Guide to physical therapist practice, second edition. Phys Ther. 2001;81:9–746.
Anema JR, Steenstra IA, Bongers PM, de Vet HC, Knol DL, Loisel P, van Mechelen W. Multidisciplinary rehabilitation for subacute low back pain: graded activity or workplace intervention or both? A randomized controlled trial. Spine (Phila Pa 1976). 2007;32(3):291–8; discussion 299–300. https://doi.org/10.1097/01.brs.0000253604.90039.ad. PMID: 17268258.
Bailly F, Trouvin AP, Bercier S, Dadoun S, Deneuville JP, Faguer R, Fassier JB, Koleck ML, Lassalle L, Le Vraux T, Brigitte L, Petitprez K, Ramond-Roquin A, Renard JO, Roren A, Rozenberg S, Sebire C, Vuides G, Rannou FO, Audrey P. Clinical guidelines and care pathway for management of low back pain with or without radicular pain. Joint Bone Spine. 2021;88(6):105227. https://doi.org/10.1016/j.jbspin.2021.105227. Epub 2021 May 26. PMID: 34051387.
Bardin LD, King P, Maher CG. Diagnostic triage for low back pain: a practical approach for primary care. Med J Aust. 2017;206(6):268–73. https://doi.org/10.5694/mja16.00828. (PMID: 28359011).
Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica: summary of NICE guidance. BMJ. 2017;6(356): i6748. https://doi.org/10.1136/bmj.i6748.Erratum.In:BMJ.2021Jul14;374:n1627. (PMID: 28062522).
Brennan GP, Fritz JM, Hunter SJ, Thackeray A, Delitto A, Erhard RE. Identifying subgroups of patients with acute/subacute ‘nonspecific’ low back pain: results of a randomized clinical trial. Spine (Phila Pa 1976). 2006;31(6):623–31. https://doi.org/10.1097/01.brs.0000202807.72292.a8. PMID: 16540864.
Brito RG, Rasmussen LA, Sluka KA. Regular physical activity prevents development of chronic muscle pain through modulation of supraspinal opioid and serotonergic mechanisms. Pain Rep. 2017;2: e618.
Bronfort G, Haas M, Evans R, Kawchuk G, Dagenais S. Evidence-informed management of chronic low back pain with spinal manipulation and mobilization. Spine J. 2008;8(1):213–25. https://doi.org/10.1016/j.spinee.2007.10.023. PMID: 18164469.
Cashin AG, Booth J, McAuley JH, Jones MD, Hübscher M, Traeger AC, Fried K, Moseley GL. Making exercise count: considerations for the role of exercise in back pain treatment. Musculoskeletal Care. 2021. https://doi.org/10.1002/msc.1597. Epub ahead of print. PMID: 34676659.
Cashin AG, Lee H, Bagg MK, O’Hagan E, Traeger AC, Kamper SJ, Folly T, Jones MD, Booth J, McAuley JH. A systematic review highlights the need to improve the quality and applicability of trials of physical therapy interventions for low back pain. J Clin Epidemiol. 2020;126:106–15. https://doi.org/10.1016/j.jclinepi.2020.06.025. (Epub 2020 Jun 27 PMID: 32603685).
Chen SM, Liu MF, Cook J, Bass S, Lo SK. Sedentary lifestyle as a risk factor for low back pain: a systematic review. Int Arch Occup Environ Health. 2009;82(7):797–806. https://doi.org/10.1007/s00420-009-0410-0. (Epub 2009 Mar 20 PMID: 19301029).
Chimenti RL, Frey-Law LA, Sluka KA. A mechanism-based approach to physical therapist management of pain. Phys Ther. 2018;98(5):302–14. https://doi.org/10.1093/ptj/pzy030. (PMID:29669091;PMCID:PMC6256939).
College of Family Physicians of Canada. Evidence-informed primary care management of low back pain: towards optimized pratice. In Clinical Practice Guideline. College of Family Physicians of Canada. Mississauga: 2015.
Colloca L, Benedetti F. Nocebo hyperalgesia: how anxiety is turned into pain. Curr Opin Anaesthesiol. 2007;20(5):435–9. https://doi.org/10.1097/ACO.0b013e3282b972fb. (PMID: 17873596).
Costa LO, Maher CG, Latimer J, Hodges PW, Herbert RD, Refshauge KM, McAuley JH, Jennings MD. Motor control exercise for chronic low back pain: a randomized placebo-controlled trial. Phys Ther. 2009;89(12):1275–86. https://doi.org/10.2522/ptj.20090218. (Epub 2009 Nov 5 PMID: 19892856).
De Ridder EM, Van Oosterwijck JO, Vleeming A, Vanderstraeten GG, Danneels LA. Posterior muscle chain activity during various extension exercises: an observational study. BMC Musculoskelet Disord. 2013;14(204):1–11.
Del Pozo-Cruz B, Gusi N, Del Pozo-Cruz J, Adsuar JC, Hernandez-Mocholí M, Parraca JA. Clinical effects of a nine-month web-based intervention in subacute non-specific low back pain patients: a randomized controlled trial. Clin Rehabil. 2013;27:28–39.
Delitto A, George SZ, Van Dillen L, Whitman JM, Sowa G, Shekelle P, Denninger TR, Godges JJ. Orthopaedic section of the american physical therapy association. Low back pain. J Orthop Sports Phys Ther. 2012;42(4):A1–57. https://doi.org/10.2519/jospt.2012.42.4.A1. Epub 2012 Mar 30. PMID: 22466247; PMCID: PMC4893951.
Donzelli S, Di Domenica E, Cova AM, Galletti R, Giunta N. Two different techniques in the rehabilitation treatment of low back pain: a randomized controlled trial. Eura Medicophys. 2006;42(3):205–10 (PMID: 17039216).
Ferreira ML, Smeets RJ, Kamper SJ, Ferreira PH, Machado LA. Can we explain heterogeneity among randomized clinical trials of exercise for chronic back pain? A meta-regression analysis of randomized controlled trials. Phys Ther. 2010;90:1383–403.
Ferreira PH, Ferreira ML, Maher CG, Refshauge K, Herbert RD, Hodges PW. Changes in recruitment of transversus abdominis correlate with disability in people with chronic low back pain. Br J Sports Med. 2010;44(16):1166–72. https://doi.org/10.1136/bjsm.2009.061515. (Epub 2009 May 26 PMID: 19474006).
Friedrich M, Gittler G, Halberstadt Y, Cermak T, Heiller I. Combined exercise and motivation program: effect on the compliance and level of disability of patients with chronic low back pain: a randomized controlled trial. Arch Phys Med Rehabil. 1998;79:475–87.
Fuentes CJP, Armijo-Olivo S, Magee DJ, Gross DP. Effects of exercise therapy on endogenous pain-relieving peptides in musculoskeletal pain: a systematic review. Clin J Pain. 2011;27(4):365–74. https://doi.org/10.1097/AJP.0b013e31820d99c8. (PMID: 21430521).
Ganesh S, Kaur P, Meena S. Systematic reviews evaluating the effectiveness of motor control exercises in patients with non-specific low back pain do not consider its principles - a review. J Bodyw Mov Ther. 2020. https://doi.org/10.1016/j.jbmt.2020.08.010. In Press, Journal Pre-proof.
Grooten WJA, Boström C, Dedering Å, Halvorsen M, Kuster RP, Nilsson-Wikmar L, Olsson CB, Rovner G, Tseli E, Rasmussen-Barr E. Summarizing the effects of different exercise types in chronic low back pain - a systematic review of systematic reviews. BMC Musculoskelet Disord. 2022;23(1):801. https://doi.org/10.1186/s12891-022-05722-x. Published 2022 Aug 22.
Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev. 2021; Issue 9. Art. No.: CD009790. https://doi.org/10.1002/14651858.CD009790.pub2.
Hayden JA, Ellis J, Ogilvie R, Stewart SA, Bagg MK, Stanojevic S, Yamato TP, Saragiotto BT. Some types of exercise are more effective than others in people with chronic low back pain: a network meta-analysis. J Physiother. 2021;67(4):252–62. https://doi.org/10.1016/j.jphys.2021.09.004. (Epub 2021 Sep 16 PMID: 34538747).
Hayden JA, van Tulder MW, Malmivaara AV, Koes BW. Meta-analysis: exercise therapy for nonspecific low back pain. Ann Intern Med. 2005;142:765–75.
Hayden JA, van Tulder MW, Tomlinson G. Systematic review: strategies for using exercise therapy to improve outcomes in chronic low back pain. Ann Intern Med. 2005;142(9):776–85. https://doi.org/10.7326/0003-4819-142-9-200505030-00014. (PMID: 15867410).
Hayden JA, vanTulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non-specific low back pain. Cochrane Database Syst Rev. 2005;3:1–68.
Hegmann KT, Travis R, Andersson GBJ, Belcourt RM, Carragee EJ, Donelson R, Eskay-Auerbach M, Galper J, Goertz M, Haldeman S, Hooper PD, Lessenger JE, Mayer T, Mueller KL, Murphy DR, Tellin WG, Thiese MS, Weiss MS, Harris JS. Non-invasive and minimally invasive management of low back disorders. J Occup Environ Med. 2020;62(3):e111–38. https://doi.org/10.1097/JOM.0000000000001812. (PMID: 31977923).
Henchoz Y, Kai-Lik SA. Exercise and nonspecific low back pain: a literature review. Joint Bone Spine. 2008;75(5):533–9.
Heneweer H, Vanhees L, Picavet HS. Physical activity and low back pain: a U-shaped relation? Pain. 2009;143(1–2):21–5. https://doi.org/10.1016/j.pain.2008.12.033. (Epub 2009 Feb 12 PMID: 19217208).
Heymans MW, van Tulder MW, Esmail R, Bombardier C, Koes BW. Back schools for non-specific low-back pain. Cochrane Database Syst Rev. 2004;(4):CD000261. https://doi.org/10.1002/14651858.CD000261.pub2. PMID: 15494995.
Hicks GE, Fritz JM, Delitto A, McGill SM. Preliminary development of a clinical prediction rule for determining which patients with low back pain will respond to a stabilization exercise program. Arch Phys Med Rehabil. 2005;86(9):1753–62. https://doi.org/10.1016/j.apmr.2005.03.033. (PMID: 16181938).
Hides J, Stanton W, Mendis MD, Sexton M. The relationship of transversus abdominis and lumbar multifidus clinical muscle tests in patients with chronic low back pain. Man Ther. 2011;16(6):573–7. https://doi.org/10.1016/j.math.2011.05.007. (Epub 2011 Jun 8 PMID: 21641268).
Hodges PW, Ferreira PH, Ferreira M. Lumbar spine: treatment of instability and disorders of movement control. In: Magee DJ, Zachazewski JE, Quillen WS, eds. Pathology and Intervention in Musculoskeletal Rehabilitation. Amsterdam: Elsevier Science BV; 2007:389-425.
HuxelBliven KC, Anderson BE. Core stability training for injury prevention. Sports Health. 2013;5(6):514–22. https://doi.org/10.1177/1941738113481200.PMID:24427426;PMCID:PMC3806175.
International Association for the Study of Pain. Task force on taxonomy. IASP terminology updated from “Part III: pain terms, a current list with definitions and notes on usage” (pp 209–214), Classification of Chronic Pain, 2nd Edition. Seattle: IASP, 2017. p. IASP.
Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo RW, Guzman J, van Tulder MW. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ. 2015;18(350): h444. https://doi.org/10.1136/bmj.h444.PMID:25694111;PMCID:PMC4353283.
Karlsson M, Bergenheim A, Larsson MEH, Nordeman L, van Tulder M, Bernhardsson S. Effects of exercise therapy in patients with acute low back pain: a systematic review of systematic reviews. Syst Rev. 2020;9(1):182. https://doi.org/10.1186/s13643-020-01412-8.PMID:32795336;PMCID:PMC7427286.
Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. Low back pain. Lancet. 2021;398(10294):78–92. https://doi.org/10.1016/S0140-6736(21)00733-9. (Epub 2021 Jun 8 PMID: 34115979).
Kreiner DS, Matz P, Bono CM, Cho CH, Easa JE, Ghiselli G, Ghogawala Z, Reitman CA, Resnick DK, Watters WC 3rd, Annaswamy TM, Baisden J, Bartynski WS, Bess S, Brewer RP, Cassidy RC, Cheng DS, Christie SD, Chutkan NB, Cohen BA, Dagenais S, Enix DE, Dougherty P, Golish SR, Gulur P, Hwang SW, Kilincer C, King JA, Lipson AC, Lisi AJ, Meagher RJ, O'Toole JE, Park P, Pekmezci M, Perry DR, Prasad R, Provenzano DA, Radcliff KE, Rahmathulla G, Reinsel TE, Rich RL Jr, Robbins DS, Rosolowski KA, Sembrano JN, Sharma AK, Stout AA, Taleghani CK, Tauzell RA, Trammell T, Vorobeychik Y, Yahiro AM. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of low back pain. Spine J. 2020;20(7):998–1024. https://doi.org/10.1016/j.spinee.2020.04.006. Epub 2020 Apr 22. Erratum in: Spine J. 2021 Feb 24;: PMID: 32333996.
Lima LV, Abner TSS, Sluka KA. Does exercise increase or decrease pain? Central mechanisms underlying these two phenomena. J Physiol. 2017;595(13):4141–4150. https://doi.org/10.1113/JP273355. Epub 2017 May 26. PMID: 28369946; PMCID: PMC5491894.
Littlewood C, Malliaras P, Bateman M, Stace R, May S, Walters S. The central nervous system–an additional consideration in ‘rotator cuff tendinopathy’ and a potential basis for understanding response to loaded therapeutic exercise. Man Ther. 2013;18(6):468–72. https://doi.org/10.1016/j.math.2013.07.005. (Epub 2013 Aug 6 PMID: 23932100).
Littlewood C, Malliaras P, Chance-Larsen K. Therapeutic exercise for rotator cuff tendinopathy: a systematic review of contextual factors and prescription parameters. Int J Rehabil Res. 2015;38:95–106. https://doi.org/10.1097/MRR.0000000000000113.
Luchtmann M, Firsching R. Central plasticity resulting from chronic low back pain in degenerative disorders of the spine. Neural Regen Res. 2015;10(8):1234–6.
Machado L, van Tulder MW, Lin C-WC, Clare H, Hayden JA. The McKenzie method for chronic non-specific low-back pain. Cochrane Database Syst Rev. 2012; Issue 3. Art. No.: CD009712. https://doi.org/10.1002/14651858.CD009712.
Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH. The effectiveness of the McKenzie method in addition to first-line care for acute low back pain: a randomized controlled trial. BMC Med. 2010;26(8):10. https://doi.org/10.1186/1741-7015-8-10.PMID:20102596;PMCID:PMC2842230.
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–47. https://doi.org/10.1016/S0140-6736(16)30970-9. (Epub 2016 Oct 11 PMID: 27745712).
Mayer JM, Haldeman S, Tricco AC, Dagenais S. Management of chronic low back pain in active individuals. Curr Sports Med Rep. 2010;9(1):60–6. https://doi.org/10.1249/JSR.0b013e3181caa9b6. PMID: 20071924.
McKenzie R, May S. The lumbar spine mechanical diagnosis and therapy. Vol 2. 2nd ed. Waikanae: Spinal Publications; 2003. p553–642.
Moseley GL. Reconceptualising pain according to modern pain science. Phys Ther Rev. 2007;12:169–78. https://doi.org/10.1179/108331907X223010.
Mueller J, Niederer D. Dose-response-relationship of stabilisation exercises in patients with chronic non-specific low back pain: a systematic review with meta-regression. Sci Rep. 2020;10(1):16921. https://doi.org/10.1038/s41598-020-73954-9. (PMID:33037280;PMCID:PMC7547082).
Nijs J, Kosek E, Van Oosterwijck J, Meeus M. Dysfunctional endogenous analgesia during exercise in patients with chronic pain: to exercise or not to exercise? Pain Physician. 2012;15(3 Suppl):ES205–13. PMID: 22786458.
Nijs J, Roussel N, Paul van Wilgen C, Köke A, Smeets R. Thinking beyond muscles and joints: therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Man Ther. 2013;18(2):96–102. https://doi.org/10.1016/j.math.2012.11.001. Epub 2012 Dec 28. PMID: 23273516.
Osteras H, Paulsberg F, Olsen SE, Osteras B, Torstensen TA. Effects of medical exercise therapy in patients with hip osteoarthritis: a randomized controlled trial with six months follow-up. A pilot study. J Bodyw Mov Ther. 2017;21(2):284–9. https://doi.org/10.1016/j.jbmt.2016.06.016. Epub 2017/05/24.
O’Sullivan P, Waller R, Wright A, Gardner J, Johnston R, Payne C, Shannon A, Ware B, Smith A. Sensory characteristics of chronic non-specific low back pain: a subgroup investigation. Man Ther. 2014;19(4):311–8. https://doi.org/10.1016/j.math.2014.03.006. (Epub 2014 Mar 25 PMID: 24731602).
Owen PJ, Miller CT, Mundell NL, Verswijveren SJJM, Tagliaferri SD, Brisby H, Bowe SJ, Belavy DL. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br J Sports Med. 2020;54(21):1279–87.
Pangarkar SS, Kang DG, Sandbrink F, Bevevino A, Tillisch K, Konitzer L, Sall J. VA/DoD clinical practice guideline: diagnosis and treatment of low back pain. J Gen Intern Med. 2019;34(11):2620–2629. https://doi.org/10.1007/s11606-019-05086-4. Epub 2019 Sep 16. PMID: 31529375; PMCID: PMC6848394.
Philips C. The modification of tension headache pain using EMG biofeedback. Behav Res Ther. 1977;15:119–29.
Rabey M, Beales D, Slater H, O’Sullivan P. Multidimensional pain profiles in four cases of chronic non-specific axial low back pain: an examination of the limitations of contemporary classification systems. Man Ther. 2015;20:138–47.
Ray CA, Carter JR. Central modulation of exercise-induced muscle pain in humans. J Physiol. 2007;585:287–94. https://doi.org/10.1113/jphysiol.2007.140509.
Refshauge K, Gass E, editors. Musculoskeletal physiotherapy clinical science and evidence-based practice. 2nd ed. Oxford: Butterworth-Heinemann; 2004.
Sallis RE. Exercise is medicine and physicians need to prescribe it! Br J Sports Med. 2009;43(1):3–4.
Saragiotto BT, Maher CG, Moseley AM, Yamato TP, Koes BW, Sun X, Hancock MJ. A systematic review reveals that the credibility of subgroup claims in low back pain trials was low. J Clin Epidemiol. 2016;79:3–9.
Searle A, Spink M, Ho A, Chuter V. Exercise interventions for the treatment of chronic low back pain: a systematic review and meta-analysis of randomised controlled trials. Clin Rehabil. 2015;29:1155–67. https://doi.org/10.1177/0269215515570379.
Slade SC, Dionne CE, Underwood M, Buchbinder R. Consensus on Exercise Reporting Template (CERT): explanation and elaboration statement. Br J Sports Med. 2016;50(23):1428–37. https://doi.org/10.1136/bjsports-2016-096651. (Epub 2016 Oct 5 PMID: 27707738).
Smart KM, Blake C, Staines A, Doody C. The discriminative validity of “nociceptive”, “peripheral neuropathic”, and “central sensitization” as mechanisms based classifications of musculoskeletal pain. Clin J Pain LWW. 2011;27:655–63.
Smeets RJ, Vlaeyen JW, Hidding A, Kester AD, van der Heijden GJ, van Geel AC, Knottnerus JA. Active rehabilitation for chronic low back pain: cognitive-behavioral, physical, or both? First direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet Disord. 2006;20(7):5. https://doi.org/10.1186/1471-2474-7-5. (PMID:16426449;PMCID:PMC1382224).
Steiger F, Wirth B, de Bruin ED, Mannion AF. Is a positive clinical outcome after exercise therapy for chronic non-specific low back pain contingent upon a corresponding improvement in the targeted aspect(s) of performance? A systematic review Eur Spine J. 2012;21(4):575–98.
Stilwell P, Harman K. Contemporary biopsychosocial exercise prescription for chronic low back pain: questioning core stability programs and considering context. J Can Chiropr Assoc. 2017;61(1):6–17.
Stolze LR, Allison SC, Childs JD. Derivation of a preliminary clinical prediction rule for identifying a subgroup of patients with low back pain likely to benefit from Pilates-based exercise. J Orthop Sports Phys Ther. 2012;42:425–36.
Tataryn N, Simas V, Catterall T, Furness J, Keogh JWL. Posterior-chain resistance training compared to general exercise and walking programmes for the treatment of chronic low back pain in the general population: a systematic review and meta-analysis. Sports Med Open. 2021;7(1):17. https://doi.org/10.1186/s40798-021-00306-w. (PMID:33683497;PMCID:PMC7940464).
van Middelkoop M, Rubinstein SM, Kuijpers T, Verhagen AP, Ostelo R, Koes BW, van Tulder MW. A systematic review on the effectiveness of physical and rehabilitation interventions for chronic non-specific low back pain. Eur Spine J. 2011;20(1):19–39. https://doi.org/10.1007/s00586-010-1518-3.
Van Oosterwijck J, Nijs J, Meeus M, Van Loo M, Paul L. Lack of endogenous pain inhibition during exercise in people with chronic whiplash associated disorders: an experimental study. J Pain. 2012;13(3):242–54. https://doi.org/10.1016/j.jpain.2011.11.006. (Epub 2012 Jan 24 PMID: 22277322).
van Wambeke P, Desomer A, Jonckheer P, Depreitere B. The Belgian national guideline on low back pain and radicular pain: key roles for rehabilitation, assessment of rehabilitation potential and the PRM specialist. Eur J Phys Rehabil Med. 2020;56(2):220–7. https://doi.org/10.23736/S1973-9087.19.05983-5. (Epub 2019 Sep 23 PMID: 31556510).
Wand BM, Chiffelle LA, O'Connell NE, McAuley JH, Desouza LH. Self-reported assessment of disability and performance-based assessment of disability are influenced by different patient characteristics in acute low back pain. Eur Spine J. 2010;19(4):633–40. https://doi.org/10.1007/s00586-009-1180-9. Epub 2009 Oct 23. PMID: 19851791; PMCID: PMC2899836.
Wells C, Kolt GS, Marshall P, Bialocerkowski A. Indications, benefits, and risks of Pilates exercise for people with chronic low back pain: a Delphi survey of Pilates-trained physical therapists. Phys Ther. 2014;94(6):806–17. https://doi.org/10.2522/ptj.20130568. (Epub 2014 Apr 3 PMID: 24700138).
Wells C, Kolt GS, Marshall P, Bialocerkowski A. The definition and application of Pilates exercise to treat people with chronic low back pain: a Delphi survey of Australian physical therapists. Phys Ther. 2014;94(6):792–805. https://doi.org/10.2522/ptj.20130030. (Epub 2013 Oct 31 PMID: 24179139).
Wittink H, Hoskins Michel T, Sukiennik A, Gascon C, Rogers W. The association of pain with aerobic fitness in patients with chronic low back pain. Arch Phys Med Rehabil. 2002;83:1467–71.
Wood L, Bishop A, Lewis M, et al. Treatment targets of exercise for persistent non-specific low back pain: a consensus study. Physiotherapy. 2021;112:78–86. https://doi.org/10.1016/j.physio.2021.03.005.
Wun A, Kollias P, Jeong H, Rizzo R, Cashin A, Bagg M, McAuley J, Jones M. Why is exercise prescribed for people with chronic low back pain? A review of the mechanisms of benefit proposed by clinical trialists. Musculoskelet Sci Pract. 2020;51: 102307.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization: SG. Methodology: SG and ARK. Formal analysis and investigation: SG, ARK, and AK. Writing: SG. Writing—review and editing: All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ganesh, G.S., Khan, A.R., Das, S. et al. Prescription of therapeutic exercise for chronic low back pain management: a narrative review. Bull Fac Phys Ther 28, 47 (2023). https://doi.org/10.1186/s43161-023-00156-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43161-023-00156-5