
Abstract
Background
Cholestatic pruritus and fatigue are debilitating conditions associated with primary biliary cholangitis (PBC) and can significantly impact patients’ quality of life. Pruritus in PBC often worsens at night and patients frequently report sleep disturbance, which contributes to cognitive symptoms and fatigue. Linerixibat is an ileal bile acid transporter inhibitor in clinical development for the treatment of pruritus associated with PBC and was recently assessed versus placebo in the Phase 2b GLIMMER trial. This post-hoc analysis assesses the relationship between pruritus severity and sleep disturbance in participants of GLIMMER regardless of treatment group.
Methods
GLIMMER (NCT02966834), a multicenter, double-blind, randomized, placebo-controlled trial, recruited 147 patients with PBC and moderate-to-severe pruritus. Following 4 weeks single-blind placebo, patients (randomized 3:1) received linerixibat or placebo for 12 weeks (to Week 16). Participants graded their itch (twice daily) and its interference with sleep (once daily) in an electronic diary using a 0–10 numerical rating scale (NRS). Weekly and monthly itch scores were calculated as the mean of the worst daily itch score over the respective time period. At study visits, participants completed the 5-D itch scale and the PBC-40 quality of life questionnaire, both of which contain an item specific to itch-related sleep disturbance. The impact of pruritus on sleep was assessed post hoc through correlations between the changes in NRS, 5-D itch, and PBC-40.
Results
Strong correlations were found between change from baseline in weekly itch and sleep NRS scores (r = 0.88 [95% confidence interval (CI): 0.83; 0.91]) at the end of treatment (Week 16), as well as in monthly itch and sleep NRS scores (r = 0.84 [95% CI: 0.80; 0.87]). Patients with improved weekly pruritus score severity category demonstrated reduced perceived sleep interference on average. Itch responders (≥2-point improvement in weekly itch score from baseline) displayed larger improvements in weekly sleep NRS score, 5-D itch, and PBC-40 sleep items, than itch non-responders (<2-point improvement).
Conclusions
A strong correlation exists between changes in pruritus severity and sleep interference in patients with PBC; pruritus reduction could generate concomitant improvement in sleep.
Plain English summary
Patients with primary biliary cholangitis (PBC) often experience debilitating itching, which can be worse at night. In the GLIMMER study of linerixibat, patients with PBC and itch also had sleep interference. When the severity of itching was reduced, there was a corresponding improvement in sleep. Reduction in itch is likely to have a beneficial impact on quality of life in patients with PBC.
Similar content being viewed by others
Background
Primary biliary cholangitis (PBC) is a rare, chronic, autoimmune, cholestatic liver disease that can lead to end-stage liver disease and necessitate liver transplantation [1]. Cholestatic pruritus (referred to by patients as itch) is commonly seen in PBC [2], affecting up to 81% of patients at some point during their disease course [2,3,4,5]. It can impair daily activities, adversely impact quality of life, contribute to fatigue, and lead to depression and, in extreme cases, suicidal ideation [5,6,7,8]. Patients with PBC who experience pruritus report worse fatigue scores than those who do not report pruritus [9, 10].
Pruritus in PBC tends to increase throughout the day and is often worse at night [11, 12]. When assessed at five timepoints (from wake time to sleep time), patients with PBC (n = 74) showed an increase in perceived pruritus over the course of a day, with the peak reported at bedtime [12].
In a study of patient perspectives by the PBCers organization, 65% of respondents with PBC and pruritus (n = 164) reported that their pruritus was worse at night [11]. One of the most prominent effects of pruritus is sleep disturbance, with 74% of patients in the same study reporting that pruritus interferes with their sleep [11]. Up to 20% of patients with PBC in the UK-PBC cohort reported that pruritus frequently or always affected their sleep [2]. In addition, patients with PBC who have higher pruritus scores have longer sleep latency, earlier wake times and increased daytime somnolence [12, 13], which in turn correlates with fatigue [13].
In a series of qualitative interviews with 20 patients with PBC and at least moderate pruritus, the symptoms reported by patients as having most impact fell into the subdomains ‘changes in daily performance’, ‘emotional functioning’, and ‘sleep difficulties caused by itching or other symptoms’ [14]. Thus, it is clear, sleep disturbance has a negative impact on the daily lives of patients with PBC.
An effective treatment for cholestatic pruritus in PBC may influence patient wellbeing by improving quality of life, which is affected by both pruritus and its impact on sleep. Current treatments for PBC, such as the first-line US Food and Drug Administration (FDA)-approved ursodeoxycholic acid (UDCA), have not been shown to improve either pruritus or sleep [15, 16]. Obeticholic acid, a conditionally approved adjunctive therapy to UDCA or monotherapy for those unable to tolerate UDCA for the treatment of PBC, has been associated with a greater incidence of severe pruritus in clinical studies than placebo, a reaction listed as a warning and precaution within the US and EU prescribing information [17,18,19]. Guideline-recommended anti-pruritic strategies for PBC include the bile acid-binding resin cholestyramine and off-label therapies including rifampicin, naltrexone, and sertraline [20]. Off-label fibrates have also been used to manage cholestatic itch [1). Similar findings were found for impact of pruritus on sleep measured by 5-D itch sleep item score and PBC-40 item 8 (“Itching disturbed my sleep”) (Table 1).
Relationship between pruritus and sleep
To evaluate the relationship between pruritus and sleep, this post-hoc analysis was conducted utilizing the GLIMMER study data to assess whether improvements in pruritus correlated with improvements in sleep. At Week 16, a strong correlation was observed between change from baseline in weekly sleep score and change from baseline in weekly itch score (r = 0.88 [95% CI: 0.83; 0.91]) (Fig. 1). Similar correlations were observed between change from baseline in monthly sleep score and monthly itch score (Fig. S1). Post-hoc analysis using the Bland–Altman statistical method showed a correlation between change from baseline in monthly itch score and change from baseline in monthly sleep score (Months 1–3) (r = 0.84 [95% CI: 0.80; 0.87]) (Fig. 2), indicating that the worsening of pruritus may contribute to increased sleep interference, and that the improvement of pruritus may contribute to decreased sleep interference.

Correlation between change from baseline in weekly sleep and itch scores at Week 16. n = 135 patients. Pearson product-moment correlation was used. BID twice daily, CI confidence interval, QD once daily

Correlation of CFB in monthly sleep and itch scores at Week 16. N = 147 patients (intent-to-treat population). Bland–Altman repeated measures correlation. Each colored dot and corresponding line is associated with an individual patient. CFB change from baseline, CI confidence interval
Relationship between improvement in pruritus and sleep
The relationship between improvement in pruritus and improvement in sleep was examined post-hoc by assessing whether reported improvements in pruritus severity categories (i.e., mild, moderate, severe) were associated with reduced sleep interference due to pruritus. Patients who experienced improvements in weekly itch score severity category from baseline at Week 16 also demonstrated improved weekly sleep score at Week 16 (Fig. 3). The extent of improvement in pruritus over the course of the study also seemed to have an impact, as patients who improved by two or more pruritus severity categories from baseline (i.e., severe to mild; moderate to none) reported greater improvements in sleep interference scores at Week 16 compared with those who only improved by one category.

Reduction in sleep interference by pruritus severity improvements from baseline at Week 16. n = 135 patients. Improvement by two severity categories corresponds to change in pruritus from severe to mild or moderate to none
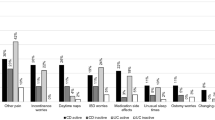
To further characterize the relationship between improvements in pruritus and sleep, weekly sleep score was assessed post-hoc in patients with improvements in pruritus (i.e., itch responders). Patients were considered itch responders if they exhibited weekly itch score improvement of ≥2 points from baseline at Week 16. Patients who demonstrated itch response experienced greater improvements in weekly sleep score, in the sleep items from the 5-D itch scale and in the PBC-40 sleep measure, compared with itch non-responders (Fig. 4). Exploring different thresholds to define itch responders, improvements from baseline of ≥3 or ≥4 points showed consistent and greater improvements in weekly sleep score, as well as in the sleep items from 5-D itch and PBC-40 measures, compared with itch non-responders (Fig. S2). Similar findings were observed with monthly sleep score (Fig. S3).

Itch responders analysis: CFB in weekly sleep score (n = 135), 5-D itch (n = 134), and PBC-40 itch domain sleep item (n = 134). A weekly sleep score; B 5-D itch scale impact of itch on sleep (disability domain sleep item) and C PBC-40 itch domain sleep item 8, impact of itch on sleep. A patient was considered an itch responder if they had a weekly itch score improvement from baseline of at least 2 points on the itch NRS at Week 16. Changes from baseline in continuous endpoints by itch responder groups are presented as box plots with mean (diamond), median, interquartile range, minimum, maximum, and outliers plotted. CFB change from baseline, PBC-40 quality of life measure for primary biliary cholangitis, 5-D 5-dimension
Discussion
Pruritus and fatigue are two of the most common and debilitating conditions impacting patients with PBC. To reduce the negative impact of these conditions on patients and their quality of life, it is essential to understand the relationship between pruritus and sleep and to determine whether improvements in pruritus have the potential to result in improved sleep. Although several studies have investigated the association between pruritus and sleep [11, 12, 39,40,41,42], this relationship has not previously been well characterized in patients with PBC. This post-hoc analysis of GLIMMER was the first and largest trial to extensively explore the directional relationship between pruritus and sleep in PBC in the entire population, regardless of treatment, using robust methodology [34]. The findings from this analysis demonstrate that there is a clear correlation between pruritus severity and the impact of pruritus on sleep interference in patients with PBC. Sleep interference was worse in patients with moderate or severe pruritus compared with those with mild pruritus, with a strong correlation between changes from baseline in weekly itch score and weekly sleep score at Week 16. Patients who reported an improvement in pruritus severity category from baseline to Week 16 exhibited improvements in sleep as measured by weekly sleep score. Further, mean improvement in weekly sleep score was greater in those with more substantial improvements in pruritus. Itch responders on average showed improved sleep compared with itch non-responders, which was confirmed by multiple different measures (weekly sleep score, reduced 5-D itch impact on sleep scores, and decreased PBC-40 sleep disturbance scores) across a range of itch response thresholds. Indeed, the reduction in pruritus-related sleep interference in patients with a ≥ 2-category improvement in pruritus was more than twice that in those with a 1-category improvement. Thus, improvement in pruritus is likely to lead to a concomitant reduction in sleep interference in patients with PBC.
In GLIMMER, daily sleep scores improved in all groups, including placebo, and there was a high concordance between improvements in itch and sleep scores [34]. The high placebo response is not unusual in pruritus studies [28, 43, 44], as well as studies that rely on subjective patient-reported outcomes [45]. GLIMMER was a dose-ranging study; changes in sleep score over the treatment period were more notable for the BID dose groups, concordant with significant improvements in pruritus. As such, this analysis was performed to further explore the relationship between pruritus severity and sleep-interference due to pruritus in patients with PBC, regardless of treatment group. The Phase 3 GLISTEN trial will further examine the effect of an optimized dose of linerixibat (40 mg BID) on sleep interference due to pruritus.
This post-hoc analysis of the GLIMMER study builds on results from a Phase 2a randomized, double-blind trial of 22 patients with PBC and pruritus, which demonstrated a significant improvement in pruritus and sleep NRS with 2 weeks of linerixibat treatment compared with placebo [24]. Two small open-label studies have shown improvements in pruritus-related sleep disturbance in patients with PBC; however, neither included a placebo comparator. The first was a Phase 2b study where 4 out of 10 patients treated with odevixibat reported improvements in pruritus as assessed by the PBC-40 itch domain and no longer experienced sleep disturbance due to pruritus [29]. The second was a Phase 2 open-label study of seladelpar in 101 patients with PBC where improvements in pruritus-related sleep disturbance, measured using the PBC-40 sleep item, were reported after 1 year [46]. Two earlier studies did include a placebo arm, including an analysis on the efficacy of sertraline in patients with cholestatic pruritus [47]. Fifty-seven percent of patients had PBC, and while sleep disturbance due to pruritus was reduced with open-label sertraline, improvements were similar in the sertraline and placebo arm when patients received double-blind treatment. The second study assessed the antipruritic effect of naltrexone in 16 patients with PBC or primary sclerosing cholangitis. Patients treated with naltrexone experienced reduced daytime and nighttime pruritus which correlated with reduced sleep disturbance [48]. While it is unclear whether improvements were associated with the specific study drug or a placebo effect, a commonality in each of these studies was that the improvement in pruritus resulted in an improvement in sleep in patients with chronic liver disease.
Despite the differences in study design and the variety of measures used to assess pruritus and sleep, there is arguably a suggestion in the published literature of an association between pruritus and sleep interference in PBC, as seen in other conditions [39, 40]. Although this post-hoc analysis demonstrates the potential clinical utility of PRO measures of sleep, the patient-reported nature of these measures may lead to a level of self-report bias. Other methods, such as actigraphy technology, monitor rest/activity cycles during sleep, may allow for an objective daily measure of sleep and sleep disturbance. Actigraphy was initially utilized in the GLIMMER trial as an optional component of the study but was discontinued due to negative patient feedback on the wearable device. The continued advancement in tools that can accurately and objectively assess sleep may provide more effective and practical means of measuring sleep in future studies [49]. Additionally, these analyses used simple correlations to assess the strength of the relationship between itch and sleep. These relationships could be further explored using modeling to adjust for covariates.
Lastly, one limitation of the current post-hoc analysis was the use of a single-item NRS for assessing sleep in GLIMMER, as it only evaluated sleep interference and was not able to differentiate which aspects of sleep were affected, such as quantity, quality, and effects on daily activities. In addition, since the protocol permitted patients with itch NRS ≥ 3 at baseline (Week 4) to be randomized, approximately 25% of the population with mild pruritus entered the treatment period [34]. Thus, the ability to fully detect an impact on pruritus, and any corresponding improvement in sleep in such patients, may have been limited. However, inclusion of patients with a wider range of pruritus is expected to have minimized the confounding effect of pruritus severity.
Conclusions
In conclusion, this post-hoc analysis of GLIMMER demonstrates a strong correlation between pruritus and sleep in patients with PBC, with the presence of worse pruritus correlating with worse sleep. Furthermore, reduction in PBC pruritus led to improved sleep, with greater improvements in pruritus associated with greater improvements in sleep. This is likely to have a beneficial impact on quality of life in patients with PBC. Future larger studies, such as the ongoing Phase 3 GLISTEN trial, will aim to better understand the effect of linerixibat on pruritus and sleep.
Data availability
Anonymized individual participant data and study documents can be requested for further research from https://www.gsk-studyregister.com/en/.
Abbreviations
- 5-D:
-
5-dimension
- ALP:
-
Alkaline phosphatase
- BID:
-
Twice daily
- CI:
-
Confidence interval
- eDiary:
-
Electronic diary
- FDA:
-
Food and Drug Administration
- IBAT:
-
Ileal bile acid transporter
- ITT:
-
Intent-to-treat
- NRS:
-
Numerical rating scale
- PBC:
-
Primary biliary cholangitis
- QD:
-
Once daily
- UDCA:
-
Ursodeoxycholic acid
References
Lleo A, Wang GQ, Gershwin ME, Hirschfield GM (2020) Primary biliary cholangitis. Lancet 396(10266):1915–1926. https://doi.org/10.1016/s0140-6736(20)31607-x
Hegade VS, Mells GF, Fisher H, Kendrick S, DiBello J, Gilchrist K, Alexander GJ, Hirschfield GM, Sandford RN, Jones DEJ, UK-PBC Consortium (2019) Pruritus is common and undertreated in patients with primary biliary cholangitis in the United Kingdom. Clin Gastroenterol Hepatol 17(7):1379–1387. https://doi.org/10.1016/j.cgh.2018.12.007
Oeda S, Takahashi H, Yoshida H, Ogawa Y, Imajo K, Yoneda M, Koshiyama Y, Ono M, Hyogo H, Kawaguchi T, Fujii H, Nishino K, Sumida Y, Tanaka S, Kawanaka M, Torimura T, Saibara T, Kawaguchi A, Nakajima A, Eguchi Y, (JSG-NAFLD) JSGoNFLD (2018) Prevalence of pruritus in patients with chronic liver disease: a multicenter study. Hepatol Res 48(3):E252–E262. https://doi.org/10.1111/hepr.12978
Talwalkar JA, Souto E, Jorgensen RA, Lindor KD (2003) Natural history of pruritus in primary biliary cirrhosis. Clin Gastroenterol Hepatol 1(4):297–302. https://doi.org/10.1016/S1542-3565(03)00134-4
Mayo MJ, Carey E, Smith HT, Mospan AR, McLaughlin M, Thompson A, Morris HL, Sandefur R, Kim WR, Bowlus C, Investigators T-P, Levy C (2023) Impact of pruritus on quality of life and current treatment patterns in patients with primary biliary cholangitis. Dig Dis Sci 68(3):995–1005. https://doi.org/10.1007/s10620-022-07581-x
Hirschfield GM, Dyson JK, Alexander GJM, Chapman MH, Collier J, Hübscher S, Patanwala I, Pereira SP, Thain C, Thorburn D, Tiniakos D, Walmsley M, Webster G, Jones DEJ (2018) The British society of gastroenterology/UK-PBC primary biliary cholangitis treatment and management guidelines. Gut 67(9):1568–1594. https://doi.org/10.1136/gutjnl-2017-315259
Tajiri K, Shimizu Y (2017) Recent advances in the management of pruritus in chronic liver diseases. World J Gastroenterol 23(19):3418–3426. https://doi.org/10.3748/wjg.v23.i19.3418
Younossi ZM, Bernstein D, Shiffman ML, Kwo P, Kim WR, Kowdley KV, Jacobson IM (2019) Diagnosis and management of primary biliary cholangitis. Am J Gastroenterol 114(1):48–63. https://doi.org/10.1038/s41395-018-0390-3
Al-Harthy N, Kumagi T, Coltescu C, Hirschfield GM (2010) The specificity of fatigue in primary biliary cirrhosis: evaluation of a large clinic practice. Hepatology 52(2):562–570. https://doi.org/10.1002/hep.23683
Hegade VS, Bolier R, Oude ERPJ, Beuers U, Kendrick S, Jones DEJ (2016) A systematic approach to the management of cholestatic pruritus in primary biliary cirrhosis. Frontline Gastroenterol 7(3):158–166. https://doi.org/10.1136/flgastro-2015-100618
Rishe E, Azarm A, Bergasa NV (2008) Itch in primary biliary cirrhosis: a patients’ perspective. Acta Derm Venereol 88(1):34–37. https://doi.org/10.2340/00015555-0350
Montagnese S, Nsemi LM, Cazzagon N, Facchini S, Costa L, Bergasa NV, Amodio P, Floreani A (2013) Sleep-wake profiles in patients with primary biliary cirrhosis. Liver Int 33(2):203–209. https://doi.org/10.1111/liv.12026
Newton JL, Gibson GJ, Tomlinson M, Wilton K, Jones D (2006) Fatigue in primary biliary cirrhosis is associated with excessive daytime somnolence. Hepatology 44(1):91–98. https://doi.org/10.1002/hep.21230
Martin ML, Stassek L, Blum SI, Joshi AV, Jones D (2019) Development and adaptation of patient-reported outcome measures for patients who experience itch associated with primary biliary cholangitis. J Patient Rep Outcomes 3(1):2. https://doi.org/10.1186/s41687-018-0090-1
Düll MM, Kremer AE (2020) Newer approaches to the management of pruritus in cholestatic liver disease. Curr Hepatol Rep 19(2):86–95. https://doi.org/10.1007/s11901-020-00517-x
Rudic JS, Poropat G, Krstic MN, Bjelakovic G, Gluud C (2012) Ursodeoxycholic acid for primary biliary cirrhosis. Cochrane Database Syst Rev 12(12):Cd000551. https://doi.org/10.1002/14651858.CD000551.pub3
Pate J, Gutierrez JA, Frenette CT, Goel A, Kumar S, Manch RA, Mena EA, Pockros PJ, Satapathy SK, Yimam KK, Gish RG (2019) Practical strategies for pruritus management in the obeticholic acid-treated patient with PBC: proceedings from the 2018 expert panel. BMJ Open Gastroenterol 6(1):e000256. https://doi.org/10.1136/bmjgast-2018-000256
Nevens F, Andreone P, Mazzella G, Strasser SI, Bowlus C, Invernizzi P, Drenth JPH, Pockros PJ, Regula J, Beuers U, Trauner M, Jones DE, Floreani A, Hohenester S, Luketic V, Shiffman M, van EKJ, Vargas V, Vincent C, Hirschfield GM, Shah H, Hansen B, Lindor KD, Marschall HU, Kowdley KV, Hooshmand-Rad R, Marmon T, Sheeron S, Pencek R, MacConell L, Pruzanski M, Shapiro D (2016) A placebo-controlled trial of obeticholic acid in primary biliary cholangitis. N Engl J Med 375(7):631–643. https://doi.org/10.1056/NEJMoa1509840
Intercept PI (2016) Occaliva (obeticholic acid) prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/207999s000lbl.pdf. Accessed Feb 2022
Lindor KD, Bowlus CL, Boyer J, Levy C, Mayo M (2019) Primary biliary cholangitis: 2018 practice guidance from the American association for the study of liver diseases. Hepatology 69(1):394–419. https://doi.org/10.1002/hep.30145
Shen N, Pan J, Miao H, Zhang H, **ng L, Yu X (2021) Fibrates for the treatment of pruritus in primary biliary cholangitis: a systematic review and meta-analysis. Ann Palliat Med 10(7):7697–7705. https://doi.org/10.21037/apm-21-1304
Kriegermeier A, Green R (2020) Pediatric cholestatic liver disease: review of bile acid metabolism and discussion of current and emerging therapies. Front Med Lausanne 7:149. https://doi.org/10.3389/fmed.2020.00149
European Association for the Study of the Liver (2009) EASL clinical practice guidelines: management of cholestatic liver diseases. J Hepatol 51(2):237–267. https://doi.org/10.1016/j.jhep.2009.04.009
Hegade VS, Kendrick SF, Dobbins RL, Miller SR, Thompson D, Richards D, Storey J, Dukes GE, Corrigan M, ERPJ O, Beuers U, Hirschfield GM, Jones DE (2017) Effect of ileal bile acid transporter inhibitor GSK2330672 on pruritus in primary biliary cholangitis: a double-blind, randomised, placebo-controlled, crossover, phase 2a study. Lancet 389(10074):1114–1123. https://doi.org/10.1016/s0140-6736(17)30319-7
Al-Dury S, Marschall HU (2018) Ileal bile acid transporter inhibition for the treatment of chronic constipation, cholestatic pruritus, and NASH. Front Pharmacol 9:931. https://doi.org/10.3389/fphar.2018.00931
Mirum Pharmaceuticals (2022) Livmarli (malarixibat) summary of product characteristics. Accessed Feb 2022 https://www.ema.europa.eu/documents/product-information/livmarli-epar-product-information_en.pdf
Mirum Pharmaceuticals (2021) Livmarli (malaraxibat) prescribing information. Accessed Feb 2022 https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/214662s000lbl.pdf
Mayo MJ, Pockros PJ, Jones D, Bowlus CL, Levy C, Patanwala I, Bacon B, Luketic V, Vuppalanchi R, Medendorp S, Dorenbaum A, Kennedy C, Novak P, Gu J, Apostol G, Hirschfield GM (2019) A randomized, controlled, phase 2 study of maralixibat in the treatment of itching associated with primary biliary cholangitis. Hepatol Commun 3(3):365–381. https://doi.org/10.1002/hep4.1305
Al-Dury S, Wahlström A, Wahlin S, Langedijk J, Elferink RO, Ståhlman M, Marschall HU (2018) Pilot study with IBAT inhibitor A4250 for the treatment of cholestatic pruritus in primary biliary cholangitis. Sci Rep 8(1):6658. https://doi.org/10.1038/s41598-018-25214-0
Baumann U, Sturm E, Lacaille F, Gonzalès E, Arnell H, Fischler B, Jørgensen MH, Thompson RJ, Mattsson JP, Ekelund M, Lindström E, Gillberg PG, Torfgård K, Soni PN (2021) Effects of odevixibat on pruritus and bile acids in children with cholestatic liver disease: phase 2 study. Clin Res Hepatol Gastroenterol 45(5):101751. https://doi.org/10.1016/j.clinre.2021.101751
Albireo Pharma (2021) Bylvay (odevixibat) summary of product characteristics. https://www.ema.europa.eu/en/documents/product-information/bylvay-epar-product-information_en.pdf. Accessed Aug 2022
Thompson RJ, Calvo PL, Hardikar W, Horn P, Lainka E, Mack CL, Ni Q, Kjems L (2022) Long-term treatment with odevixibat improves multiple sleep parameters in patients with progressive familial intrahepatic cholestasis: a pooled responder analysis from the phase 3 PEDFIC studies. Gastroenterology 162(7):S–1297. https://doi.org/10.1016/S0016-5085(22)63794-6
Thompson RJ, D’Antiga L, Gonzales E, Karpen SL, Kjems L, Loomes K, Mack CL, Ni Q, Verkade HJ, Horn P (2022) Odevixibat therapy improves clinically meaningful endpoints in children with progressive familial intrahepatic cholestasis: data from the PEDFIC 1 and PEDFIC 2 trials. Gastroenterology 162(7):S–1296. https://doi.org/10.1016/S0016-5085(22)63792-2
Levy C, Kendrick S, Bowlus CL, Tanaka A, Jones D, Kremer AE, Mayo MJ, Haque N, von Maltzahn R, Allinder M, Swift B, McLaughlin MM, Hirschfield GM, Group GS (2023) GLIMMER: a Randomized Phase 2b Dose-Ranging Trial of Linerixibat in Primary Biliary Cholangitis Patients With Pruritus. Clin Gastroenterol Hepatol 21(7):1902–1912 e1913. https://doi.org/10.1016/j.cgh.2022.10.032
Lai JW, Chen HC, Chou CY, Yen HR, Li TC, Sun MF, Chang HH, Huang CC, Tsai FJ, Tschen J, Chang CT (2017) Transformation of 5-D itch scale and numerical rating scale in chronic hemodialysis patients. BMC Nephrol 18(1):56. https://doi.org/10.1186/s12882-017-0475-z
Elman S, Hynan LS, Gabriel V, Mayo MJ (2010) The 5-D itch scale: a new measure of pruritus. Br J Dermatol 162(3):587–593. https://doi.org/10.1111/j.1365-2133.2009.09586.x
Jacoby A, Rannard A, Buck D, Bhala N, Newton JL, James OF, Jones DE (2005) Development, validation, and evaluation of the PBC-40, a disease specific health related quality of life measure for primary biliary cirrhosis. Gut 54(11):1622–1629. https://doi.org/10.1136/gut.2005.065862
Bonett DG, Wright TA (2000) Sample size requirements for estimating pearson, kendall and spearman correlations. Psychometrika 65(1):23–28. https://doi.org/10.1007/BF02294183
Bawany F, Northcott CA, Beck LA, Pigeon WR (2021) Sleep disturbances and atopic dermatitis: relationships, methods for assessment, and therapies. J Allergy Clin Immunol Pract 9(4):1488–1500. https://doi.org/10.1016/j.jaip.2020.12.007
Kaaz K, Szepietowski JC, Ł M (2019) Influence of itch and pain on sleep quality in atopic dermatitis and psoriasis. Acta Derm Venereol 99(2):175–180. https://doi.org/10.2340/00015555-3065
Lee J, Suh H, Jung H, Park M, Ahn J (2021) Association between chronic pruritus, depression, and insomnia: a cross-sectional study. JAAD Int 3:54–60. https://doi.org/10.1016/j.jdin.2021.02.004
Kaaz K, Szepietowski JC, Ł M (2018) Influence of itch and pain on sleep quality in patients with hidradenitis suppurativa. Acta Derm Venereol 98(8):757–761. https://doi.org/10.2340/00015555-2967
Bartels DJ, van Laarhoven AI, van de Kerkhof PC, Evers AW (2016) Placebo and nocebo effects on itch: effects, mechanisms, and predictors. Eur J Pain 20(1):8–13. https://doi.org/10.1002/ejp.750
Gonzales E, Hardikar W, Stormon M, Baker A, Hierro L, Gliwicz D, Lacaille F, Lachaux A, Sturm E, Setchell KDR, Kennedy C, Dorenbaum A, Steinmetz J, Desai NK, Wardle AJ, Garner W, Vig P, Jaecklin T, Sokal EM, Jacquemin E (2021) Efficacy and safety of maralixibat treatment in patients with Alagille syndrome and cholestatic pruritus (ICONIC): a randomised phase 2 study. Lancet 398(10311):1581–1592. https://doi.org/10.1016/S0140-6736(21)01256-3
Evans K, Colloca L, Pecina M, Katz N (2021) What can be done to control the placebo response in clinical trials? A narrative review. Contemp Clin Trials 107:106503. https://doi.org/10.1016/j.cct.2021.106503
Kremer AE, Mayo MJ, Hirschfield G, Levy C, Bowlus CL, Jones DE, Steinberg A, McWherter CA, Choi YJ (2021) Seladelpar improved measures of pruritus, sleep, and fatigue and decreased serum bile acids in patients with primary biliary cholangitis. Liver Int 42(1):112–123. https://doi.org/10.1111/liv.15039
Mayo MJ, Handem I, Saldana S, Jacobe H, Getachew Y, Rush AJ (2007) Sertraline as a first-line treatment for cholestatic pruritus. Hepatology 45(3):666–674. https://doi.org/10.1002/hep.21553
Wolfhagen FH, Sternieri E, Hop WC, Vitale G, Bertolotti M, Van BHR (1997) Oral naltrexone treatment for cholestatic pruritus: a double-blind, placebo-controlled study. Gastroenterology 113(4):1264–1269. https://doi.org/10.1053/gast.1997.v113.pm9322521
De Zambotti M, Cellini N, Goldstone A, Colrain IM, Baker FC (2019) Wearable sleep technology in clinical and research settings. Med Sci Sports Exerc 51(7):1538–1557. https://doi.org/10.1249/MSS.0000000000001947
Acknowledgements
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors. The authors take full responsibility for the scope, direction, and content of the manuscript and have approved the submitted manuscript. The authors received no compensation related to the development of the manuscript. Medical writing assistance, in the form of draft preparation, collation and incorporation of authors’ comments, and preparation of figures and tables, was provided by Terrance Ku, MSc, of Complete HealthVizion, funded by GSK. Additional medical writing assistance, in the form of editing, collation and incorporation of author’s comments at later drafts, and submission support was provided by Gemma Corr, DPhil, of Fishawack Indicia Ltd, UK, part of Avalere Health and was funded by GSK.
Funding
This study was funded by GSK, study number 201000. GSK was involved in the study design and the collection, analysis, and interpretation of the data.
Author information
Authors and Affiliations
Contributions
M.J.M., C.L. and D.J. were involved in the conception and design of the study and data acquisition. All authors were involved in data analysis and interpretation. All authors contributed to the development of the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed in accordance with the Declaration of Helsinki, International Conference on Technical Requirements for Registration of Pharmaceuticals for Human Use Good Clinical Practice, and applicable country-specific requirements. The study protocol, any amendments, informed consent, and other information that required pre-approval were reviewed and approved by a national, regional, or investigational center ethics committee or institutional review board. Written informed consent was obtained from all patients before participation.
Consent for publication
Not applicable.
Clinical trial registration
clinicaltrials.gov, NCT02966834. Registered 15 November 2016.
Competing interests
RVM is an employee of GSK and holds GSK shares. MJM has received research support from CymaBay, GSK, Intercept, Mallinckrodt, Salix, and TARGET RWE; and has consulted for CymaBay, GSK, Mallinckrodt, Mirum, and TARGET RWE. HTS is an employee of GSK and holds GSK shares. AT was an employee of GSK at the time of the study and holds GSK shares. SD is an employee of GSK. ARdS is an employee of GSK and holds GSK shares. EL is an employee of GSK and holds GSK shares. CL is an ABIM committee member and an associate editor of Hepatology; has consulted for Calliditas, CymaBay, DISC Medicine, Gilead, GSK, Intercept, Mirum, Pliant, Target RWE, and Ipsen; has participated on advisory boards for Bausch, Cymabay, GSK, Ipsen, Intercept and Pliant; and has received research grants from Cara Therapeutics, CymaBay, Disc Medicine, Escient, Genfit, Calliditas, Gilead, GSK, HighTide, Intercept, Mirum, Pliant, Target RWE, Ipsen and Zydus. MMM is an employee of GSK and holds GSK shares. DJ has received grant funding or fees from Abbott, Falk, GSK, Intercept, Novartis, and Pfizer.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
April Thompson: Affiliated with GSK during the conduct of the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
von Maltzahn, R., Mayo, M., Smith, H. et al. Relationship between pruritus and sleep in participants with primary biliary cholangitis in the Phase 2b GLIMMER trial. J Patient Rep Outcomes 8, 60 (2024). https://doi.org/10.1186/s41687-024-00722-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41687-024-00722-y